
Abstract
Background
To assess the diagnostic performance of 64-section computed tomography angiography (CTA) for detection of cerebral aneurysms by comparison with the new gold standard three-dimensional (3D) digital subtraction angiography (DSA).
Material and Methods
A total of 128 patients who underwent both 64-section CTA and 3D DSA for suspected intracranial aneurysms were included. The location, size, and shape of the aneurysm were assessed and compared with 3D DSA results. The sensitivity, specificity, positive and negative predictive values of 64-section CTA were calculated by using 3D DSA as reference standard.
Results
According to the reference standard, a total of 145 aneurysms were detected at 3D DSA in 118 patients. Of these 145 aneurysms, 64-section CTA detected 139 aneurysms in 118 patients. The sensitivity of CTA for detection of aneurysm was 95.8% on a per-aneurysm basis. All missed aneurysms were non-causative very small aneurysms in patients harboring multiple aneurysms. On a per-patient basis, the sensitivity, specificity, positive and negative predictive values were 100%.
Conclusion
Compared with the new gold standard 3D DSA, 64-section CTA offers high sensitivity and specificity for detection of intracranial aneurysms. It could be readily used as a screening imaging method for detection of intracranial aneurysms.
Introduction
Rupture of a cerebral aneurysm is the most common cause of subarachnoid hemorrhage. Patients with ruptured cerebral aneurysm should be evaluated and treated on an emergency basis to prevent subsequent medical and neurological complications. Digital subtraction angiography (DSA) has long been considered the gold standard in detection of intracranial aneurysms (1). However, the technique is invasive, time-consuming, and carries a potential risk of permanent neurological complications (2). In recent years, non-invasive imaging techniques have increasingly been used for the evaluation of intracranial aneurysms. Computed tomography angiography (CTA) is a fast, non-invasive imaging method that has been widely used in the diagnostic work-up of patients with subarachnoid hemorrhage. In previous studies, it is reported that the diagnostic performance of CTA is approaching that of DSA for detection and treatment planning of aneurysms (3–5).
In previous studies, several authors compared the diagnostic accuracy of CTA with conventional DSA (3–7). However, DSA false-negative small aneurysms were consistently reported during surgery of ruptured intracranial aneurysms (8,9). The incidence of very small occult cerebral aneurysms may be even higher than that reported in surgical series because surgery only allows partial exposure of the cerebral vessels. In recent years, three-dimensional (3D) DSA has been widely used in clinical practice for detection of small intracranial aneurysms. It is well established that 3D DSA may depict more aneurysm than conventional DSA (10). Few studies compared the diagnostic accuracy of 64-section CTA with 3D DSA for detection of intracranial aneurysms. The purpose of our study was to compare the diagnostic performance of 64-section multidetector CTA with 3D DSA for detection of intracranial aneurysms.
Material and Methods
A total of 128 patients who underwent 3D DSA for suspected intracranial aneurysms were included in our study. Patients were referred for 64-section CTA and 3D DSA based on signs and symptoms suggestive of intracranial aneurysms. Patients were included in the final analysis if they had undergone both 64-section CTA and 3D DSA for suspected intracranial aneurysms. Patients were excluded from the study if they had prior history of endovascular coiling or surgical clipping of intracranial aneurysms. A total of 128 patients (71 men, 57 women; mean age, 49 years; age range, 41–69 years) who underwent both 64-section CTA and 3D DSA for suspected intracranial aneurysms were included. Institutional review board approval and informed consent were obtained.
CTA protocol
All CTA examination was performed with a 64-section multidetector CT scanner (Lightspeed, GE Healthcare, Milwaukee. WI, USA). Patients were placed in the supine position and patients’ heads were immobilized during the scan to prevent motion artifacts. A total of 80 mL contrast material was intravenously injected through an 18- or 22-gauge needle via antecubital vein by using a power injector at a rate of 4.5 mL/s. The scan delay was determined by using a bolus tracking technique. The CTA acquisition parameters were as follows: section thickness, 0.625 mm; 120 kV; 300 mA. Images were transferred to a workstation (Advantage for Windows, GE Healthcare) for postprocessing. The raw image data were reformatted as maximum intensity projection (MIP) and volume-rendering (VR) images on a workstation for image analysis.
3D DSA protocol
DSA was performed by selective injection of 18 mL contrast material in the internal carotid and vertebral arteries. A standard projection format, including anteroposterior, lateral, and oblique views was obtained and images were transferred to the picture archiving and communication systems (PACS). Rotational angiography was performed by using a biplanar C arm. Rotational angiography was performed with a 200° arc rotational run around the patients’ head during intra-arterial injection of contrast material. The raw data were transferred to a dedicated workstation for postprocessing. 3D VR reconstructions were made with a matrix size of 1024 pixels. The reconstructed 3D VR images were sent to a PACS for further review.
Image interpretation
All 3D DSA results were evaluated by a group of interventional neurologists who performed the exam. All CTA results were judged by two independent readers who were blinded to the results of 3D DSA. In interpretation of CTA and 3D DSA images, the readers had to examine the following anatomic locations for aneurysms: the internal carotid artery (ICA), A1 and A2 segments of anterior cerebral artery (ACA), M1 and M2 segments of middle cerebral artery (MCA), P1 and P2 segments of posterior cerebral artery (PCA) and the vertebrobasilar artery. When an aneurysm was considered present, the authors have to evaluate the location, size, and shape of an aneurysm, as well as its relationship with the parent artery and branching arteries. All aneurysms were assessed based on the source images as well as the MIP and VR images.
Statistical analysis
The 3D rotational angiography results were used as the reference standard to assess the diagnostic performance of 64-section multidetector CTA. Sensitivity, specificity, positive predictive value, and negative predictive value of 64-section CTA for aneurysm detection were calculated on a per-aneurysm and per-patient basis.
Results
All patients have successfully completed both CTA and 3D DSA examinations. There were no technical failures or procedure-related neurological complications. All the angiograms were diagnostic. In 118 of 128 patients, a total of 145 aneurysms were detected on 3D DSA. No aneurysm was detected in 10 patients. A single aneurysm was detected in 101 patients. Seventeen patients had multiple aneurysms: 10 patients had two aneurysms, five patients had three aneurysms, one patient had four aneurysms, and one patient had five aneurysms. The aneurysms were located at the anterior communicating artery (n = 37, 25.5%), the posterior communicating artery (n = 36, 24.8%), the internal carotid artery (n = 48, 33.1%), the middle cerebral artery (n = 22, 15.1%), and the basilar artery (n = 2, 1.3%). The average maximal sac diameter was 5.1 mm (range, 2.1–15.8 mm). The average neck size was 4.3 mm (range, 1.2–12.1 mm). Of the 145 aneurysms, 43 (29.6%) were <3 mm, 63 (43.5%) were 3–5 mm, 32 (22.1%) were 5–10 mm, seven (4.8%) were >10 mm in maximal diameter.
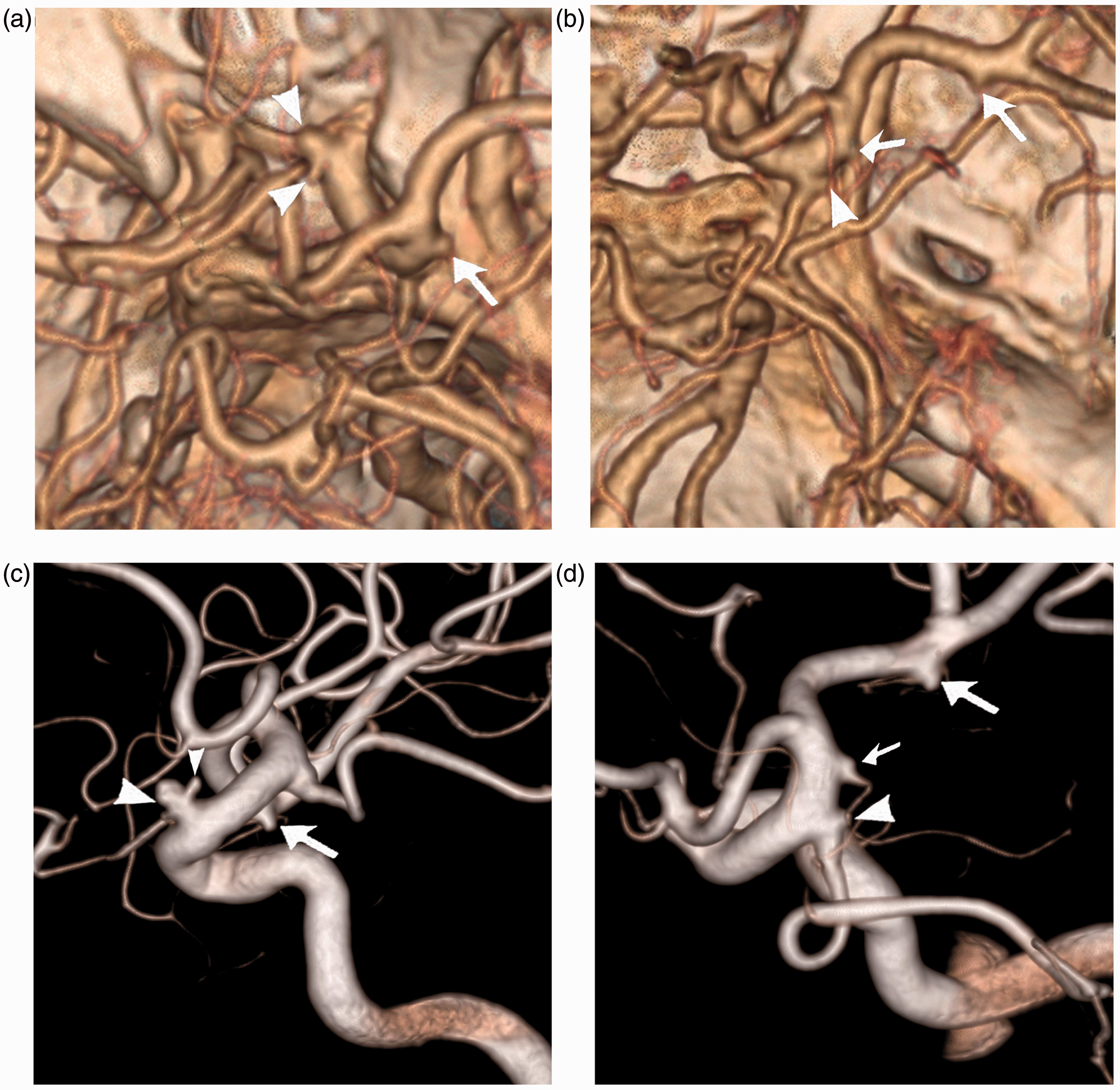
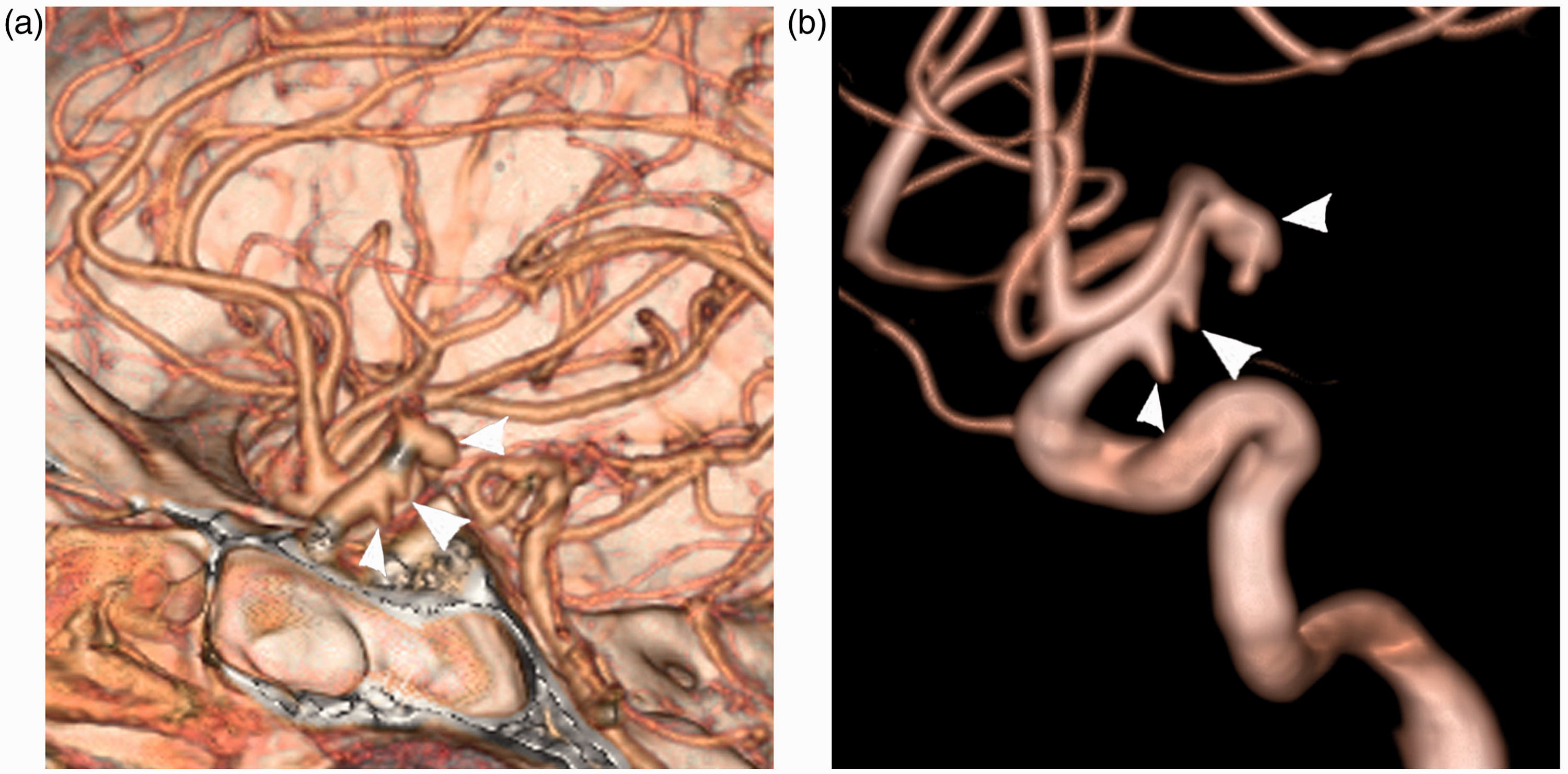
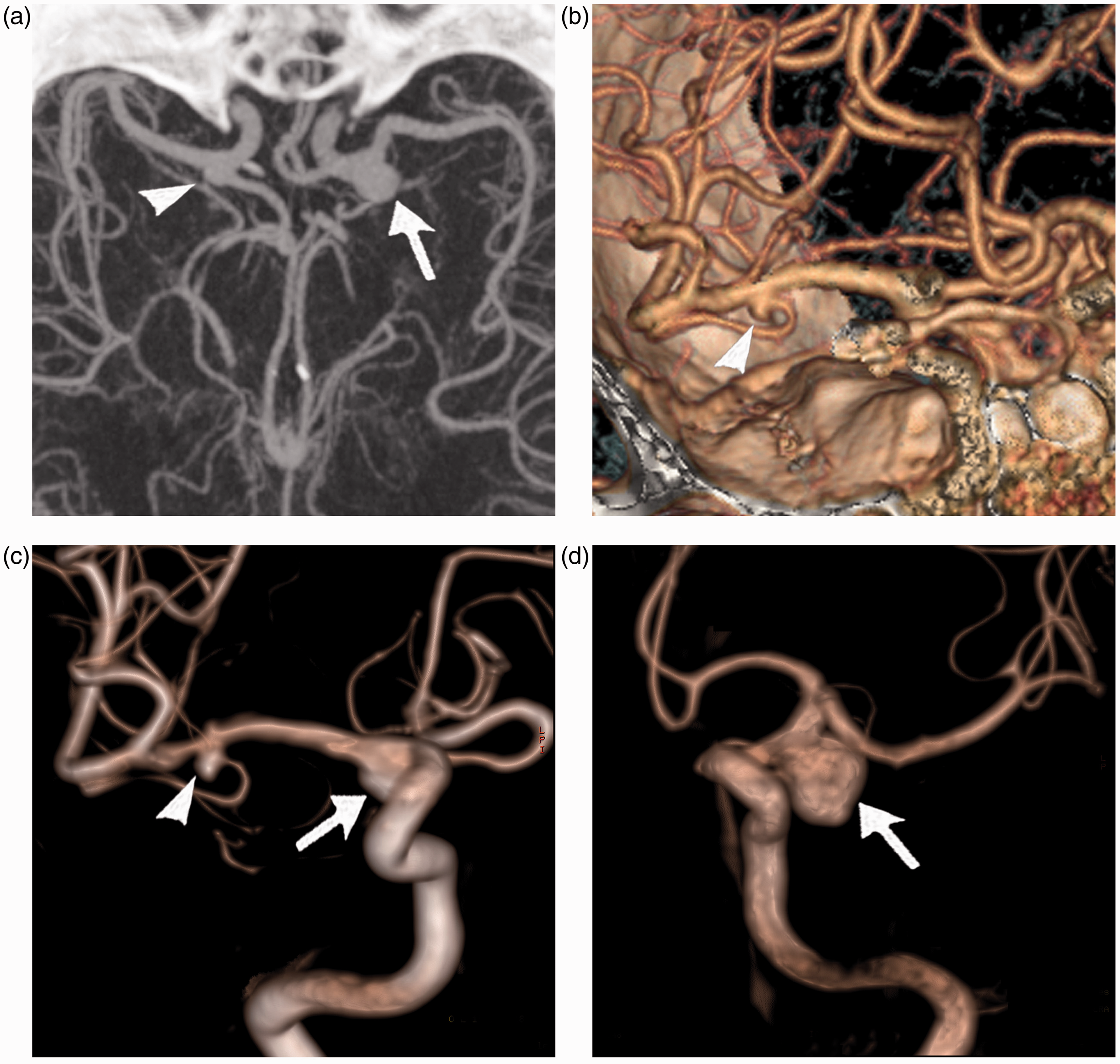
A total of 139 aneurysms were identified at CTA in 128 patients. In our case series, all CTA missed aneurysms were small occult non-causative aneurysms in patients with multiple aneurysms. There were no CTA false-positive cases. In a patient with four aneurysms, CTA successfully depicted three aneurysms but failed to reveal a very small unruptured occult aneurysm located at the internal carotid artery (Fig. 1). In another patient with four aneurysms, both readers missed a very small occult posterior communicating artery aneurysm (Fig. 2). However, subsequent analysis of CTA data revealed that the aneurysm was present on CT angiograms and could be retrospectively identified by both readers. In most cases with multiple aneurysms, CTA was equal to 3D DSA for detection of intracranial aneurysms (Fig. 3). The lobulation of the aneurysm could be clearly depicted in all cases by manipulating the 3D CTA images (Fig. 4). The 3D CTA images also allow accurate delineation of the aneurysm and its branching arteries. The sensitivity, specificity, positive and negative predictive values of CTA for detection of intracranial aneurysms were calculated according to aneurysm size (Table 1). The per-aneurysm and per-patient diagnostic performance of 64-section CTA were also calculated (Table 2). On a per-patient basis, the sensitivity, specificity, positive and negative predictive values of CTA for detecting intracranial aneurysms were 100%, 100%, 100%, and 100%, respectively. On a per-aneurysm basis, the sensitivity, specificity, positive and negative predictive values of CTA for detecting intracranial aneurysms were 95%, 100%, 100%, and 80%, respectively.
CTA false-negative aneurysm in a patient with multiple aneurysms. (a) CTA revealed three aneurysms located at the anterior communicating artery (long arrow), the left posterior communicating artery (short arrow) and the right middle cerebral artery bifurcation (arrowhead). (b) 3D rotational angiography confirmed the anterior communicating artery aneurysm (arrow) and the middle cerebral artery aneurysm (arrowhead). (c) Oblique rotational image showed the left posterior communicating artery aneurysm (arrow) and detected an additional very small internal carotid artery aneurysm (arrowhead). Images in a patient with multiple aneurysms. (a) Axial CTA image revealed a bilobulated internal carotid artery aneurysm (arrowheads) and an additional small aneurysm located at the internal carotid artery terminal (arrow). (b) Oblique CTA images showed a middle cerebral artery aneurysm (long arrow) and the internal carotid artery terminal aneurysm (short arrow). The very small posterior communicating artery aneurysm (arrowhead) was missed by both readers during the initial reading. (c) 3D rotational angiogram confirmed the bilobulated aneurysm (arrows) and the internal carotid artery terminal aneurysm (arrow). (d) Oblique 3D rotational angiogram revealed the internal carotid artery terminal aneurysm (small arrow)and the middle cerebral artery aneurysms (large arrow). The posterior communicating artery aneurysm (arrowhead) was clearly present on 3D rotational angiogram. 3D rotational angiography and 64-section CTA for detection of three aneurysms (arrowheads) located at the internal carotid artery in a single patient. (a) CTA demonstrated three small aneurysms located at the internal carotid artery. (b) All aneurysms present on CTA angiograms were confirmed by 3D rotational angiography. Visualization of branching artery in a patient with three aneurysms. (a) Axial CTA maximum intensity projection angiogram revealed two aneurysms located at the left (arrow) and right (arrowhead) posterior communicating artery. (b) An additional middle cerebral artery aneurysm (arrowhead) and its branching artery were clearly depicted on CTA 3D volume-rendered image. The middle cerebral artery aneurysm (arrowhead) and the two posterior communicating artery aneurysms (arrows) were confirmed at 3D rotational angiography images (c, d). Diagnostic performance of 64-section CTA according to aneurysm size. Numbers in parentheses indicate numbers of aneurysms. NPV, negative predictive value; PPV, positive predictive value. Diagnostic performance of 64-section CTA on a per-aneurysm and per-patient basis. Numbers in parentheses indicate numbers of aneurysms. NPV, negative predictive value; PPV, positive predictive value.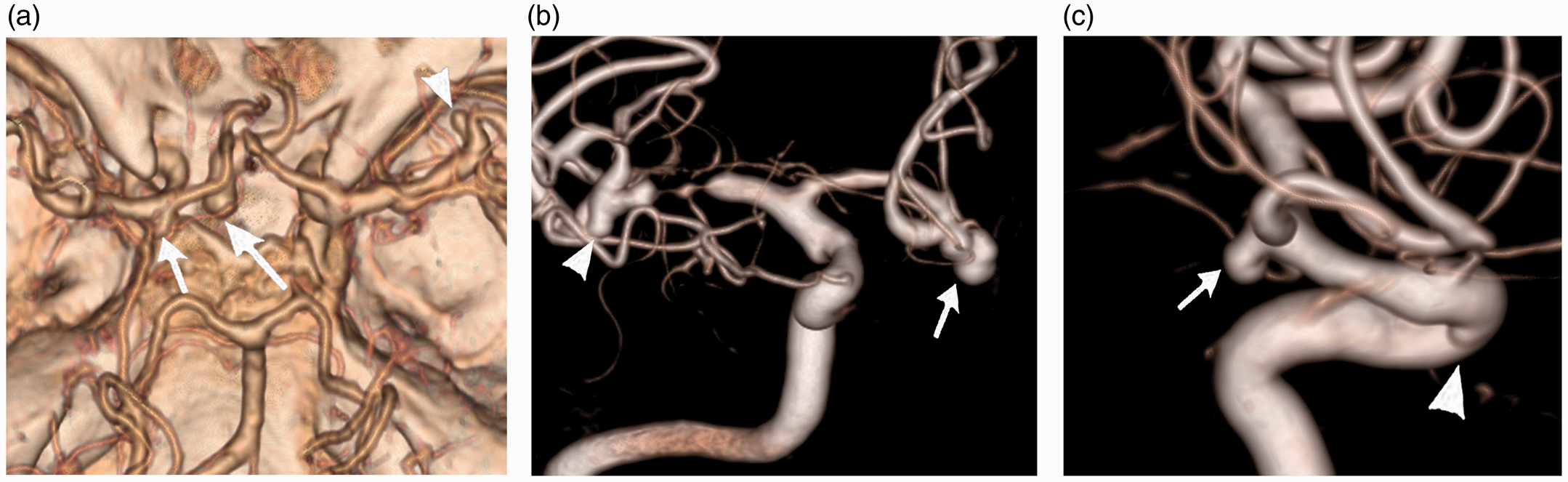


Discussion
CTA has been increasingly accepted as a noninvasive imaging method in detection of intracranial aneurysms. It is well established that CTA has high sensitivity and specificity for detecting intracranial aneurysms. In previous reports, the reported sensitivity of single section CTA for detecting intracranial aneurysm ranged from 62% to 100% (6,11,12). In recent reports, multidetector CTA has been compared favorably with conventional DSA for detection of intracranial aneurysms (3–5,7,13,14). Aneurysm size is an important factor for detection rate of aneurysms at CTA. In previous reports, multidetector CTA has demonstrated 100% sensitivity for aneurysms >5 mm. However, CTA is less useful than DSA for detection of small intracranial aneurysms (7,10–14).
In previous studies, conventional DSA missed occult aneurysms were consistently reported during the surgery of ruptured aneurysms. In a study of 536 patients, Karasawa et al. reported a 3.7% of conventional DSA missed aneurysms during intraoperative exploration of symptomatic intracranial aneurysms (15). Similar results were reported in another study of 351 patients with surgically treated aneurysms (8). The incidence of conventional DSA missed occult aneurysms may be underestimated in these surgical series because the intraoperative view is restricted to adjacent areas of the symptomatic aneurysm. It is also reported that a negative DSA result could not rule out aneurysms in patients with SAH. In an early study, Urbach et al. reported that 6% additional aneurysms were found at repeat DSA examination in patients with negative initial angiography results (16). The results of previous reports suggested that conventional DSA should not be considered the gold standard in comparative studies that evaluate the diagnostic accuracy of CTA for detection of intracranial aneurysms.
Recently, 3D DSA, which is capable of reconstruction in any chosen projection, has been introduced into clinical practice. It is reported that 3D DSA may detect considerably more aneurysms than conventional DSA (10). Another advantage of 3D DSA is that it provides more detailed information regarding morphology of the aneurysm (17). In recent years, 3D DSA has replaced conventional DSA as the new golden standard for detection and characterization of intracranial aneurysms. In our study, we compared the diagnostic performance of CTA with the new golden standard 3D DSA for detection of intracranial aneurysms. We report that the sensitivity of 64-section CTA for detection of intracranial aneurysms is 95.8% on a per-aneurysm basis. In previous studies, the reported sensitivity of 64-section CTA ranged from 92.8% to 99% for detection of cerebral aneurysms (18,19). However, the reported sensitivity may be overestimated in these studies because most authors have used conventional DSA as golden standard when comparing with CTA.
In our series, all causative aneurysms could be correctly identified by 64-section CTA. The sensitivity and specificity of 64-section CTA were both 100% on a per-patient basis. In our study, 37 of 43 (86%) very small (<3 mm) aneurysms could be correctly identified by 64-section CTA. Although seven aneurysms were missed by CTA, all missed aneurysms were very small non-causative aneurysms. In our series, all these CTA missed aneurysms were found in patients with more than two aneurysms. The causative aneurysms were all identified at CTA in these cases and the missed additional aneurysms usually do not require surgical treatment in clinical settings. Although the diagnostic performance of 64-section CTA was inferior to 3D DSA for detecting small occult aneurysms, these CTA false-negative non-causative aneurysms were generally considered clinically insignificant.
The reference standard is a key factor in the assessment of diagnostic performance of CTA for detecting intracranial aneurysms. In this study, we have used 3D DSA as the reference standard to evaluate the diagnostic performance of 64-section CTA in detection of intracranial aneurysms. We found that 64-section CTA could identify all causative aneurysms, but failed to identify several very small incidental aneurysms which were readily visualized by 3D DSA. However, those very small incidental aneurysms occur in patients with multiple aneurysms and are clinically insignificant.
In conclusion, the results of our study indicate that 64-section CTA has high sensitivity and specificity for detection of intracranial aneurysms. It could be used as an alternative imaging method to 3D DSA in the diagnostic work-up of patients with suspected intracranial aneurysms.
Footnotes
Funding
The study is supported by a grant from the National Natural Science Foundation of China (Grant No. 81200899).