
Abstract
Background
In Sweden, native and transplant kidney biopsies are usually performed in major renal medical centers.
Purpose
To clarify risk factors in native and transplant kidney biopsies to improve patient safety.
Material and Methods
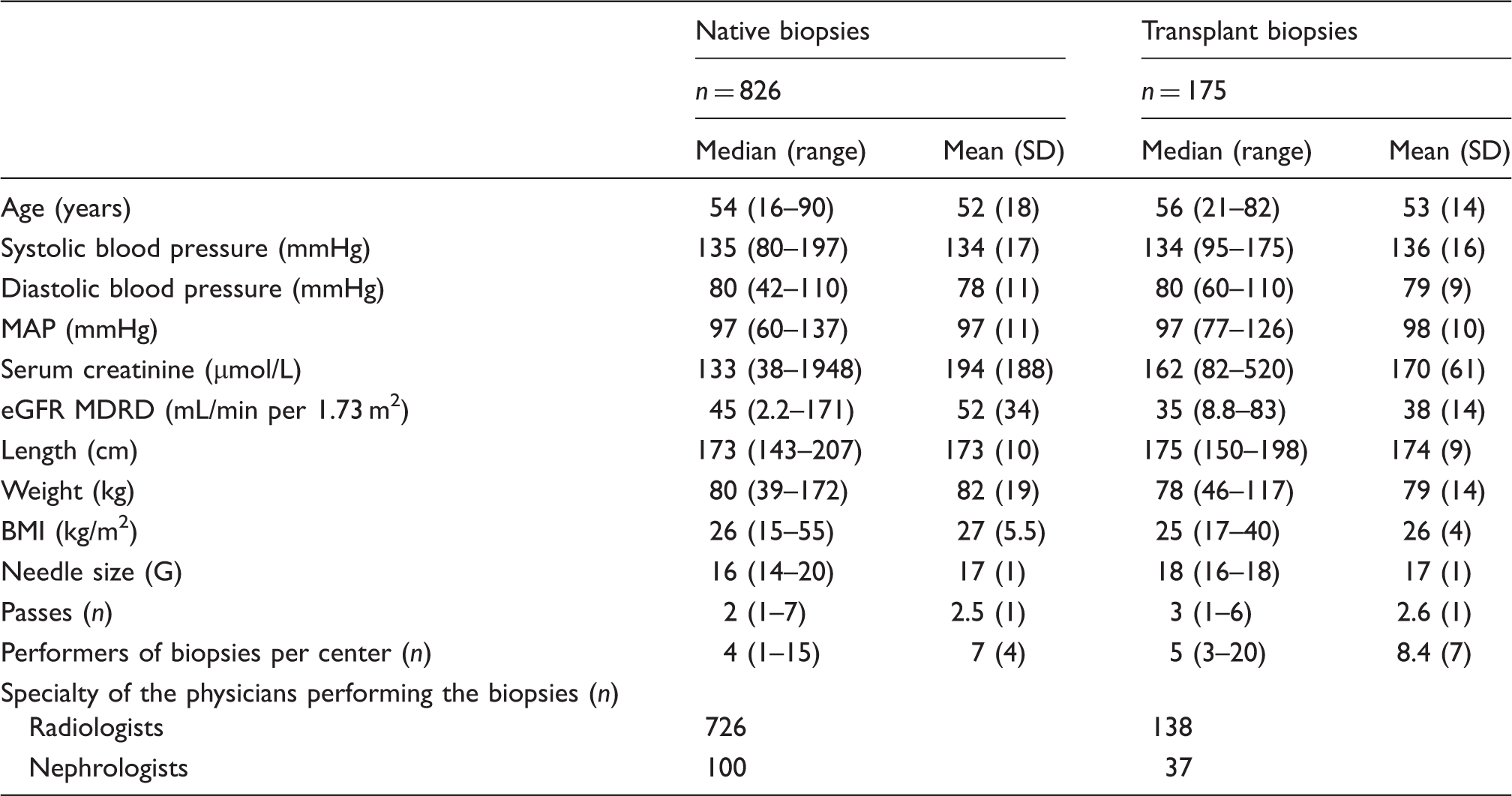
A total of 1001 biopsies (in 352 women and 565 men) were included. The median age was 54 years (range, 16–90 years). Data were derived from 826 native kidney biopsies (640 prospective and 186 retrospective) and 175 transplant kidney biopsies (170 prospective and 5 retrospective). Various factors and complications were registered while performing native and transplant kidney biopsies, focusing on major (e.g. blood transfusions, invasive procedures) and minor complications. The prospective protocol was used at six centers and at one center data were obtained retrospectively.
Results
Women were at greater risk of overall complications than men (12.2% vs. 6.5%; P = 0.003; odds ratio [OR], 2.0; confidence interval [CI], 1.3–3.1) as well as of major complications (9.6% vs. 4.5%; P = 0.002; OR, 2.2, CI 1.3–3.7). Major complications occurred more commonly after biopsies from the right kidney, in women than in men (10.8% vs. 3.1%; P = 0.005; OR, 3.7; CI, 1.5–9.5), and in patients with lower BMI (25.5 vs. 27.3, P = 0.016) and of younger age (45 years vs. 52.5 years; P = 0.001). Lower mean arterial pressure in transplant kidney biopsies indicated a risk of major complications (90 mmHg vs. 98 mmHg; P = 0.039). Factors such as needle size, number of passes, serum creatinine, and eGFR did not influence complication rates.
Conclusion
The present findings motivate greater attention being paid to the risk of major side-effects after right-side biopsies from women’s kidneys, as well as after biopsies from younger patients and patients with lower BMI.
Introduction
Kidney and transplant kidney biopsies have been performed in nephrology for many years to establish diagnoses and treatments (1–4). Real-time ultrasound guidance and an automated spring-loaded biopsy device are used today (5). Although the techniques for percutaneous kidney and transplant kidney biopsy have been improved in recent years, complications occur. The risk factors for complications are age, blood pressure, level of kidney function, and needle size (5–10).
Adverse effects can be divided into major and minor complications. Major complications require an intervention (e.g. a blood transfusion and/or invasive radiological procedures). Minor complications resolve spontaneously without the need for intervention (e.g. gross hematuria) (11). Common and minor side-effects are microscopic hematuria (nearly 100%) or asymptomatic perinephric hematoma (up to 90%) (11,12). These are usually not registered as complications. Another mostly asymptomatic consequence of biopsies is the development of an arteriovenous fistula as a result of damage to the wall of a blood vessel. If the fistula causes symptoms, a radiological or surgical intervention may be necessary (11). The frequency of major complications differs among clinical studies and depends on factors such as the techniques used (manual/automated biopsy needles, needle size, number of passes, etc.). The frequency of major complications is in the range of 1–7% and of minor complications 6.6–19.7% for native kidney biopsies (5,8,13–18). The frequency of major complications for biopsies from transplant kidneys is in the range of 0.4–2.9%. Most of the latter are protocol biopsies (15,19–21).
The aims of this study were to clarify the complication panorama and risk factors in native and transplant kidney biopsies. Furthermore, we intended to characterize the existing risks and identify new and additional risks for the development of complications in kidney and transplant kidney biopsies.
Material and Methods
Native and transplant kidney biopsies (baseline data).
We designed a protocol for prospective registration of various factors and complications associated with native and transplant kidney biopsies. The protocol was used prospectively at all medical centers in western Sweden (six centers, including one university hospital) and retrospectively at one medical center (university hospital) in northern Sweden. The data were collected from 1 January 2006 until 27 March 2013. Our study was approved by the Regional Ethical Review Board in Gothenburg/Sweden and was independent to the industry.
The collected data included the type of biopsy (native kidney or transplant kidney biopsy), date, hospital, age, sex, systolic and diastolic blood pressure, serum creatinine prior biopsy, length, weight, needle size (in gauge [G]) and needle type, number of needle passes per biopsy, localization (right, left, transplant kidney), specialty of the physician carrying out the biopsy (nephrologist, radiologist), and name of the physician who performed the biopsy. We also registered whether the biopsy was performed on an outpatient or inpatient basis, if the biopsy was planned or acute, and if the biopsy was a re-biopsy because the previous biopsy did not provide clear information. The protocol requested information about complications with the following alternatives: fall in blood pressure requiring treatment, congestion of the urinary tract, urinary bladder tamponade, infection requiring antibiotic treatment, clinically significant hematoma, bleeding requiring blood transfusion, surgical intervention after biopsy, damage to other organs during the biopsy, gross hematuria after biopsy, nephrectomy after biopsy, extended care because of complications, and a free text field.
All kidney and transplant kidney biopsies in our study, except one computer tomography (CT)-guided kidney biopsy, were performed using real-time ultrasound guidance (i.e. an ultrasound machine Logiq E9 with 2–5 MHz-sector transducer [GE Healthcare, Chalfont St Giles, UK] or similar) and an automated spring-loaded biopsy device (i.e. automated biopsy needle 16 G, 15 cm needle length, and 20 mm sampling length [HTR 16/15, Tsunami Medical, San Possidonio, Italy] or similar). For the native kidney biopsies 14-, 16-, 18-, and 20-gauge needles were used and for the transplant kidney biopsies 16- and 18-gauge needles. Radiologists and nephrologists (one center) performed the biopsies. In the native kidney biopsies performed by nephrologists, an ultrasonographer localized the kidneys and the nephrologist performed the biopsies. In the biopsy of transplant kidney performed by nephrologists, the nephrologists themselves localized the transplant kidney and performed the biopsies using real-time ultrasound.
Before the biopsies were performed, basic investigations including variables such as blood pressure, pulse, hemoglobin level, renal function panel, test for bleeding disturbances, urine samples were performed. Bleeding time was measured at two centers in the native kidney biopsies. If the blood pressure was above 160/90 mmHg, extra antihypertensive drugs were administered. Patients treated with the anticoagulants acetylsalicylic acid, clopidogrel, and warfarin were instructed to discontinue their medication 7 days before biopsy; if the patient was on NSAID treatment it was required to be discontinued 3 days before biopsy. One center performed the transplant kidney biopsies even if the patient was taking acetylsalicylic acid.
The patients were instructed to fast for 4 h before the biopsies. Patients having native kidney biopsies were turned on the side opposite to the biopsied kidney with a pillow under the flank, while patients having transplant kidney biopsies were in the supine position. Before performing each biopsy, the patient had a diagnostic renal ultrasound examination (bilateral for native kidneys) to evaluate the length and depth of kidney or transplant kidney, anatomical abnormalities, and hydronephrosis. The skin over the kidney or transplant kidney was sterilized with antiseptic solution. Then the skin and subcutaneous tissue were infiltrated with 10 mL xylocaine 10 mg/mL. This local anesthetic was injected down to and including the renal capsule, using real-time ultrasound. An incision was made with a scalpel blade (No. 11) and the automated biopsy needle inserted into the renal cortex under real-time ultrasound guidance. No microscopic control of the specimens after the biopsies was performed. The specimens were placed in a fixative (paraformaldehyde) (HistoLab AB, Västra Frölunda, Sweden) and sent to the renal pathologist for examination.
All native kidney biopsies were performed as inpatient procedures. The transplant kidney biopsies were performed as either outpatient or inpatient procedures. After an inpatient biopsy the patient stayed in bed for 4 h; the first hour lying on the side of biopsied native kidney or in the supine position for patients who had transplant kidney biopsies. Blood pressure, pulse, vital signs, and visual analogue scale (VAS) for pain were measured every 15 min for the first hour, every 30 min for the second hour, and every 60 min for a further 3 h. Patients who had outpatient transplant kidney biopsies were discharged after an observation period of 2 h of bed rest (blood pressure and pulse were measured every 15 min for the first hour and every 30 min for the second hour) and after a check of their hemoglobin levels. Patients biopsied at the inpatient ward stayed overnight for observation.
The kidney function level, i.e. estimated GFR (eGFR), was calculated using the Modification of Diet in Renal Disease (MDRD) formula (GFR in mL/min per 1.73 m2) (22).
For the statistical analysis the IBM SPSS Statistic 20 (IBM, Armonk, NY, USA) was used. Fisher’s exact test and X2 analyses were used for cross-tabulation of data. Group comparisons were made using the independent Student’s test. Pearson’s test was used for correlation analyses. Multi-regression analyses were performed with the above-mentioned risk factors included in the models. Stepwise analyses were used. A two sided P value of <0.05 was considered significant.
Results
Data on a total of 1001 biopsies were included in the study (Table 1). In addition to kidney and transplant kidney biopsies, we registered one horseshoe kidney, one single kidney, and one biopsy of bilateral kidney (left and right in the same patient and at the same time).
In the whole study population, the frequency of overall complications was 8.7%, for major complications 6.5% and 2.2% for minor complications. For native kidney biopsies the corresponding figures were 9.1% for overall, 7% for major complications, and 2.1% for minor complications, whereas the frequency of complications between left and right kidney was not significant. The complication frequency in transplant kidney biopsies was 6.9% for overall, 4% for major complications, and 2.9% for minor complications.
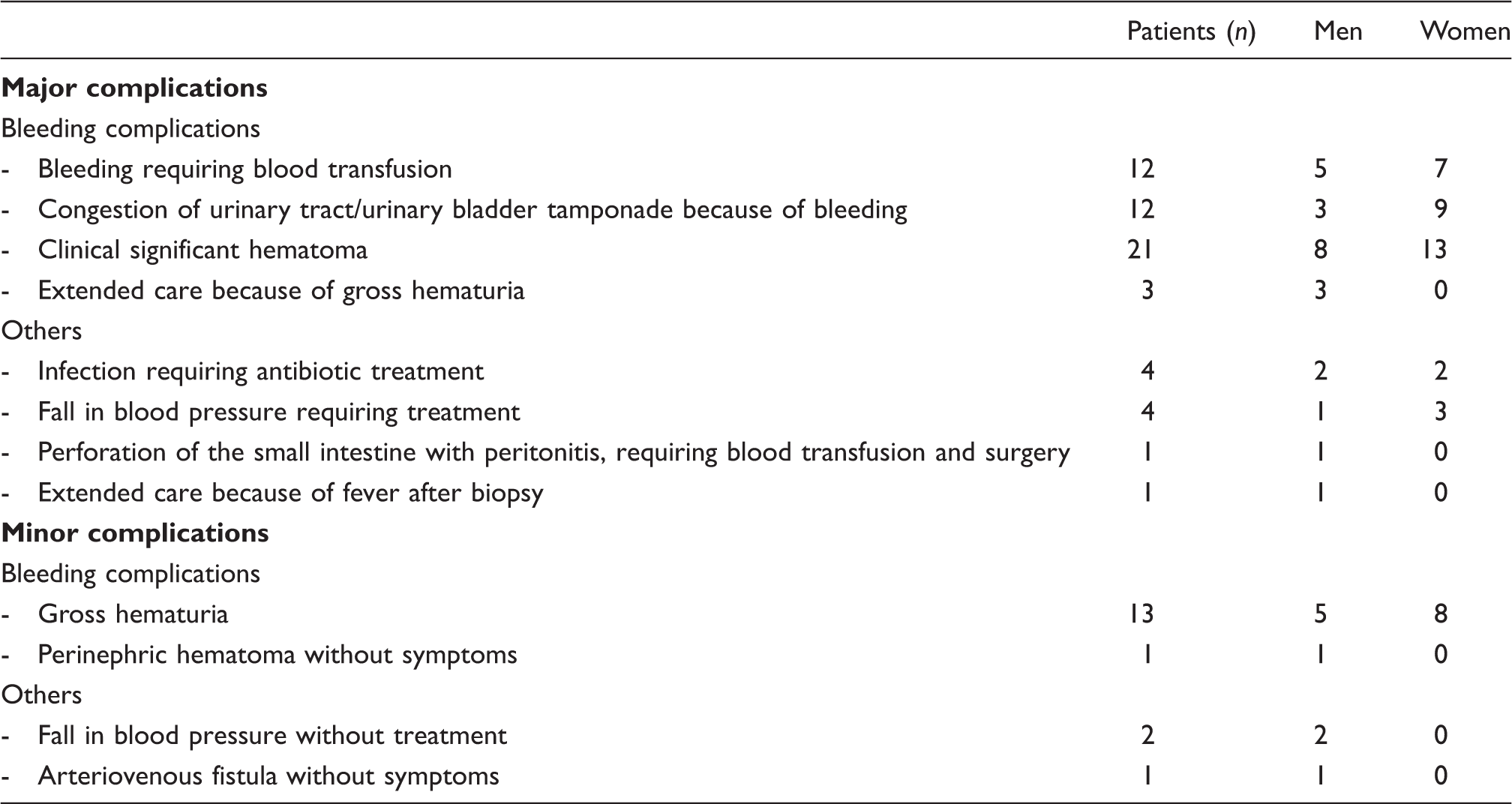
Type of complications after native kidney biopsies.
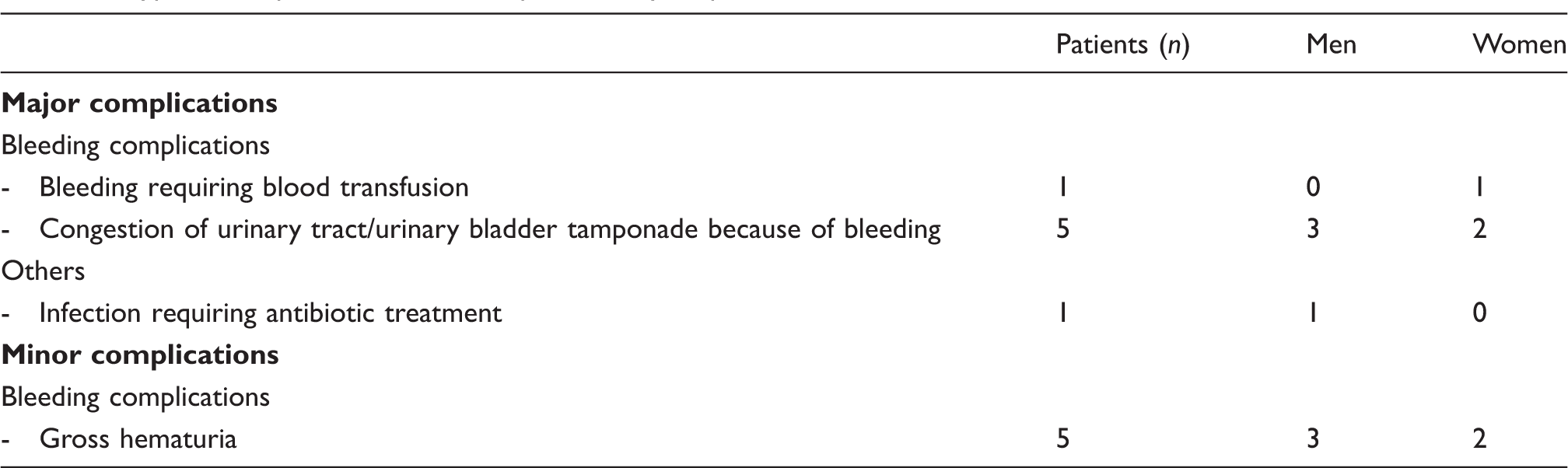
Type of complications after transplant kidney biopsies.
Analysis showed (Fig. 1) a significantly higher risk of overall complications after kidney and kidney transplant biopsies for women than for men (12.2% vs. 6.5%; P = 0.003, odds ratio [OR], 2.0; confidence interval [CI], 1.3–3.1). The risk of minor complications was not higher for women, whereas the risk of major complications was (9.6% vs. 4.5%; P = 0.002; OR, 2.2; CI, 1.3–3.7). Major complications were more commonly found after biopsies from the right kidney in women than in men (10.8% vs. 3.1%; P = 0.005; OR, 3.7; CI, 1.5–9.5). The risk of major complications was not higher after biopsies from the left or transplant kidneys. The risk of overall complications after biopsies from the left kidney (13.2% vs. 7.4%; P = 0.041; OR, 1.9; CI, 1.0–3.5) and the right kidney (13.2% vs. 5.4%; P = 0.015; OR, 2.7; CI, 1.2–5.8) was significantly higher in women than in men.
Risk of complications in women and men in percent.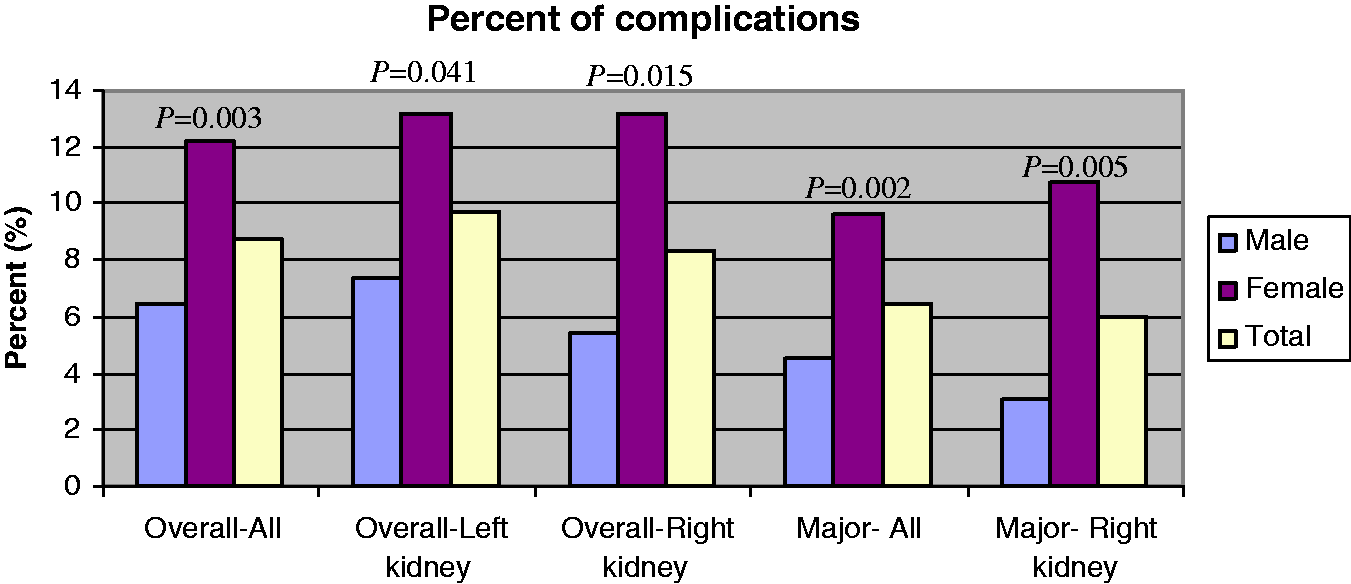
Patients with lower BMI were found to be at greater risk of both major complications (mean BMI 25.5 vs. 27.3; P = 0.016) and overall complications (mean BMI 25.8 vs. 27.3; P = 0.022) after native kidney biopsies, but not after transplant kidney biopsies. The risk of major complications after native kidney biopsies was higher for shorter patients (body length 170 cm vs. 173 cm; P = 0.011) and patients with lower body weight (74 kg vs. 82 kg; P = 0.002). The same finding applied concerning the risk of overall complications after native kidney biopsies (body length 170 cm vs. 173 cm; P = 0.008; body weight 75 kg vs. 82 kg; P = 0.002). For transplant kidney biopsies, body length and weight were not risk factors for complications.
Younger age was a risk factor for both major (45 years vs. 52.5 years; P = 0.001) and overall (46.5 years vs. 52.5 years; P = 0.002) complications in the whole study population. After native kidney biopsies, younger age was a risk factor for both major (44.8 years vs. 52.3 years; P = 0.002) and overall (47 years vs. 52.3 years; P = 0.015) complications, but not for minor complications. In contrast, in the transplant kidney biopsy population, younger age was a risk factor for minor (37.6 years vs. 53.5 years; P = 0.009) and overall (42.8 years vs. 53.8 years; P = 0.006) complications, but not for major complications.
Lower mean arterial pressure (MAP) was a risk factor for major complications (mean MAP 90 mmHg vs. 98 mmHg; P = 0.039) and for overall complications (mean MAP 92 mmHg vs. 98 mmHg; P = 0.04) in transplant kidney biopsies, but not in native kidney biopsies. Only lower systolic blood pressure was a risk factor for overall complications in transplant kidney biopsies (mean 126 mmHg vs. 136 mmHg; P = 0.028).
Factors including diastolic blood pressure, needle size, number of passes, serum creatinine, eGFR MDRD, number and specialty (nephrologists vs. radiologists) of the physicians who performed the biopsies per center did not result in an increased risk of overall, minor or major complications either in native kidney or in transplant kidney biopsies.
The multi-regression analyses showed that younger age (P = 0.005), female sex (P = 0.002), and lower BMI (P = 0.043) are risk factors for major complications in native kidney biopsies. For transplant kidney biopsies only younger age was found to be a risk factor, and only for minor (P = 0.008) and overall (P = 0.002) complications. When age and BMI are the only variables analyzed for native kidney biopsies in the model, only age turned out to be significant.
Discussion
The new information gained from this study was the presence of a greater risk of complications in women, and especially after biopsies from the right kidney, as well as in patients with lower BMI. This has not been reported before. One reason for these findings may be that the present study contained data from >1000 biopsies, and mostly prospective data. In other prospective studies the number of patients was limited, between 77 and 523 (9). The interesting finding in our study that women had a greater risk of complications is still unclear. Some authors speculate that women have lower GFRs than men for the same serum creatinine value (9). However, we did not find that serum creatinine and eGFR are risk factors for complications in our study.
Some recommend biopsy of the left kidney because it is more comfortable for the right-handed operator and far from vital organs (23). In contrast, the right kidney is preferred by others because it is situated below the last rib, accessible with mild inspiration, and far from the spleen (13,14). As far as we know, this question has not been elucidated in previous studies. This study found a greater risk of major complications in women after biopsies from the right kidney than from either the left or transplant kidneys. It may therefore be important to take into account from which kidney (right vs. left) the biopsy is taken.
The present study also showed, for the first time, that the risk of major complications after native kidney biopsies was higher in patients with lower BMI, as well as in shorter patients and patients with lower body weight. Maybe the patients with higher BMI are less mobile. Their adipose tissue may compress the wounded capsule of the kidney and the channel of the injection. On the other side the localization and visualization of the kidneys by ultrasound may be more difficult in patients with high BMI.
The present study also showed that younger age was a risk factor for major and overall complications in native kidney biopsies and for minor and overall complications in transplant kidney biopsies. Other studies in native kidney biopsies have also found younger age to be a risk factor for complications (6,24,25), although yet other studies have indicated higher age as a risk factor for complications (5,10). Few studies of transplant kidney biopsies have shown younger age (26) to be a risk factor. This may be related to the fact that younger patients are more active in the period after their biopsies.
We also found that lower mean arterial pressure (MAP) and lower systolic blood pressure were risk factors for complications after transplant kidney biopsies, but not in native kidney biopsies. These are new results. However, interpretation is difficult since the number of patients in this group with complications was low.
In contrast to many other studies, we found that the known risk factors, such as high blood pressure (7,10), needle size (4,9,27), number of passes (10), serum creatinine (5–9), and eGFR MDRD (5) did not increase the risk of complications in native and transplant kidney biopsies. The findings that the needle size and the number of passes did not affect the risk of complications are helpful in optimizing clinical practice and diagnostics.
The number and specialty (nephrologists vs. radiologists) of the physicians performing biopsies per center was not a risk factor for complications in native or transplant kidney biopsies in our study. One previous study, however, showed that severe complications were significant lower after biopsies performed by nephrologists (28). The number of the performers of biopsies per center has not been investigated previously, to our knowledge.
A limitation in our study was the mixed design (prospective and retrospective data). Therefore, for the control of the retrospective data, the main author collected, checked and completed the data after studying the medical charts personally. We have used the same protocol for registration for both retrospective and prospective data.
In conclusion, the present results motivate greater attention being paid to the possibility of major side-effects after biopsies performed in women and from their right side, in younger patients, and in patients with lower BMI. The multidisciplinary approach between the nephrologists, radiologists, and pathologists is important for patient safety.
Footnotes
Acknowledgements
The authors are grateful to renal nurses Carina Johansson, Lizett Ljungqvist, Elisabeth Rosqvist, Eva-Lena Settergren, Kristina Sjöström, Malin Skagerlind, Lena Wetterlund and the medical staff at all the centers that participated in our study.
Funding
The authors gratefully acknowledge funding from the Research Center (FOU), Skaraborg Hospital, Skövde and Research Center, Västerbotten County, Umeå.