
Abstract
Background
Mammography (MX) is a reliable modality for detection of breast cancer in asymptomatic women. Use of additional whole breast ultrasonography (US) for breast cancer screening is widely recognized, in particular in women with dense breast parenchyma.
Purpose
To determine the subgroup of women, according to breast density and age, who receive most benefit from US following MX for detection of breast cancer in an asymptomatic condition.
Material and Methods
The study was conducted in asymptomatic women who had non-fatty breast parenchyma using MX and US during January 2006 and December 2007. Mammographic breast density was classified as recommended by ACR BI-RADS lexicon. Non-fatty breast referred to D2, D3, and D4. US was performed by the same radiologists who interpreted MX with a handheld machine during the same visit. Data on demographics, cancer detection rate (CDR), and incremental cancer detection rate (ICDR) were analyzed using 95% confident interval (CI).
Results
Of 14,483 breast cancer screenings in women who had non-fatty breast density, 115 cancers were documented. The mean age of cancer patients was 49.6 years. Of 115 cancers, 105 were evidenced on images (31 with MX alone, 19 with US alone, and 55 with both MX and US). Overall CDR was 7.9 per 1000 examination (95% CI, 6.5–9.5). CDR for MX only (MX-CDR) was 6.5 per 1000 examinations (95% CI, 5.2–7.9). Additional US could significantly improve CDR (P < 0.001; 95% CI, 0.9–2.2); US-ICDR was 1.4 per 1000 examinations. According to age group, the group of 40–59 years had statistically significant improvement of ICDR (P < 0.001). The ICDR was highest in D4 breast density (D4) (US-ICDR = 2.5 per 1000 examinations).
Conclusion
Use of US adjunct to MX for detection of breast cancer in asymptomatic non-fatty, average-risk women for detection of breast cancer is a promising diagnostic procedure. A significant benefit was documented, in particular, in women aged 40–59 years old, and in women with D4 breast density.
Introduction
Screening of breast cancer with mammography (MX) is well-established, and that can benefit in mortality reduction (1,2). However, supplemental whole breast ultrasonography (US) may increase diagnostic yield in women with dense breast tissue. Previous studies demonstrated a substantial improvement in breast cancer detection with US in women with dense breast parenchyma (3–5).
According to the American College of Radiology: Breast Imaging Reporting and Data system protocol (ACR: BI-RADS) (6), breast density on MX can be classified into fatty breast (D1: <25% glandular), scatter fibroglandular breast (D2: 25–50% glandular), heterogeneous breast (D3: 51–75% glandular) and extremely dense breast (D4: >75% glandular). Dense breast tissue and young age were strong independent factors for misinterpretation on MX (7–11). In some individual women, in particular in women who had dense breast tissue and aged <50 years, additional US in detection breast lesion occulted on MX may demonstrate some benefit, with incremental cancer detection rate (ICDR) of 1.5–3.4 per 1000 examinations (12–15). However, use of addition US in asymptomatic condition was criticized because of various limitations. High false-positive rate, time consumption, and operator dependency were reported. As a result, those lesions were biopsied unnecessarily (12,16).
To the best of our knowledge, no previous publications demonstrate which women in different age groups and different breast density will receive benefit from an US in detection of breast cancer. Therefore, this study aimed to document the benefit of US in addition to MX for detection of breast cancer in a specific age group of women who are of average risk and have non-fatty breast density. Findings obtained from the study are useful when considering adjunct US in detection of breast cancer in some particular subgroup of asymptomatic women.
Material and Methods
The study was critically reviewed and approved by the Institutional Review Board. In order to exclude high-risk lesions, screenings from women with signs and symptoms of breast disease and from women who had previous history of breast cancer were excluded. As well, screenings from women with previous evidence of atypical ductal hyperplasia, atypical lobular hyperplasia, and lobular carcinoma in situ were excluded from the study. All breast cancer screenings were voluntary. Mammographic breast parenchymal density was classified into fatty (D1: <25% glandular), scatter fibroglandular (D2: 25–50% glandular), heterogeneous (D3: 51–75% glandular), and extremely dense (D4: >75% glandular), as recommended by the ACR BI-RADS lexicon (9). Non-fatty breast parenchymal density referred to D2, D3, and D4. Following MX in the same visit, additional whole US was performed when D2, D3, or D4 breast density was documented by the same radiologists who interpreted MX.
The study started from 14,770 breast cancer screenings from women who were asymptomatic and had MX and US performed at our institute during January 2006 and December 2007. Of these, 287 were fatty breast (D1) and thus were excluded from the study. Only 14,483 with non-fatty breast density (D2, D3, and D4) were included in the study. MX was conducted in the standard craniocaudal and mediolateral oblique views using digital MX (Hologic-Selenia, Bedford, MA, USA) and was reviewed by experienced diagnostic breast radiologists. All MX performed in this study were full field digital films. Whole breast handheld US was performed following the MX in the same visit by the same radiologists who interpreted MX using Logic E9, Logic 9, or Logic 7 with 10 to 14 MHz linear-array probe (GE Healthcare, Milwaukee, WI, USA). If there were previous results from the MX and US, those results were compared with the current study. Further pathological or cytological proof of benign condition was processed when image interpretation was BI-RADS 4 or 5. However, tissue or cytological biopsies were delivered in some lesions with BI-RADS 1, 2, and 3 when clinicians decided to do so with agreement with the patients. Diagnosis of benign lesion was confirmed either by histopathology or stability of lesion over the follow-up images for at least 24 months. Breast cancer was diagnosed with proven histopathology or cytology. All invasive cancers and ductal carcinoma in situ were regarded as cancer.
Cancer detection rate (CDR), incremental cancer detection rate for US (ICDR-US), and positive predictive value (PPV) in different breast tissue densities and age groups were reported. CDR was the number of cancer detected by MX or US per 1000 examinations. ICDR-US was number of breast cancer detected by US, but not on MX per 1000 examinations. PPV was the ratio between number of lesions proven to be cancer (ductal carcinoma in situ included) and number of women who had positive screening. In this study, criteria of positive screening included report assessment of BI-RADS 4 and 5, and negative screening included report assessment of BI-RADS 1–3.
Statistical analysis of CDR, ICDR-US, PPV of MX and MX plus US with 95% confident interval (CI) were reported. For categorical variables, differences between groups were tested using Chi-square test and McNemar test. The odds ratio with 95% CI in different breast tissue densities and age groups were also reported.
Results
Breast tissue density of 14,770 examinations, categorized by age. Only 14,483 with D2, D3 and D4 were included in the study.
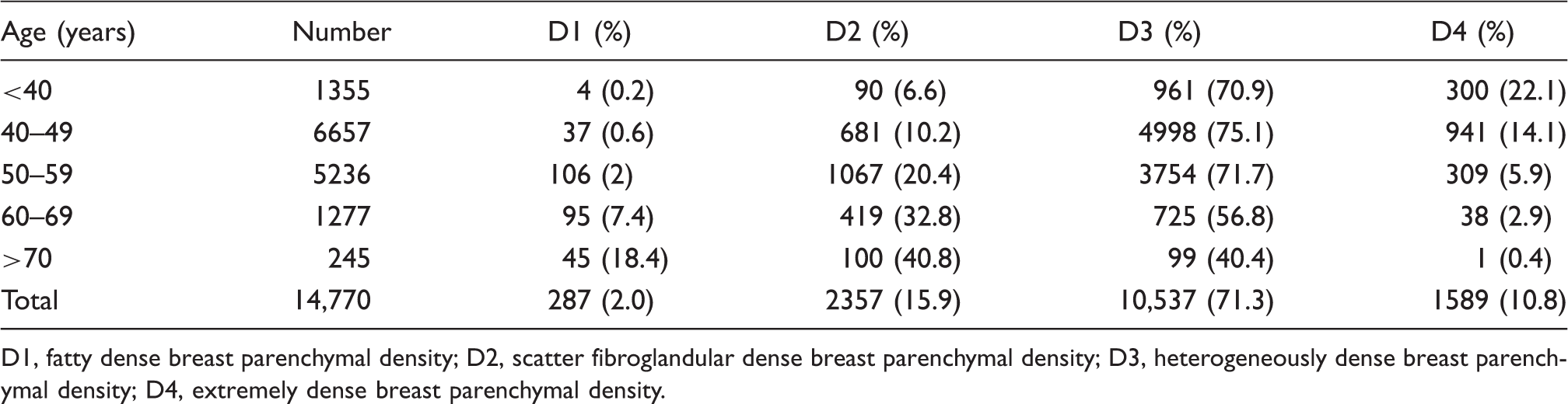
D1, fatty dense breast parenchymal density; D2, scatter fibroglandular dense breast parenchymal density; D3, heterogeneously dense breast parenchymal density; D4, extremely dense breast parenchymal density.
Of 105 cancers detected on breast imaging, 31 (29.5%) were malignant microcalcifications demonstrated on MX alone; 19 (18.1%) were evidenced with US alone, not MX; and 55 (52.4%) had abnormal finding on both MX and US. Thirty-one cancerous microcalcifications detected on MX (not US) were documented in six patients with D2, 24 patients with D3, and one patient with D4 breast density. Of 19 malignant lesions evidenced only on US; three patients had D2, 13 patients had D3, and three patients had D4 breast density.
Comparison of CDR, ICDR, and PPV between MX and MX plus US, according to age group, and breast density.
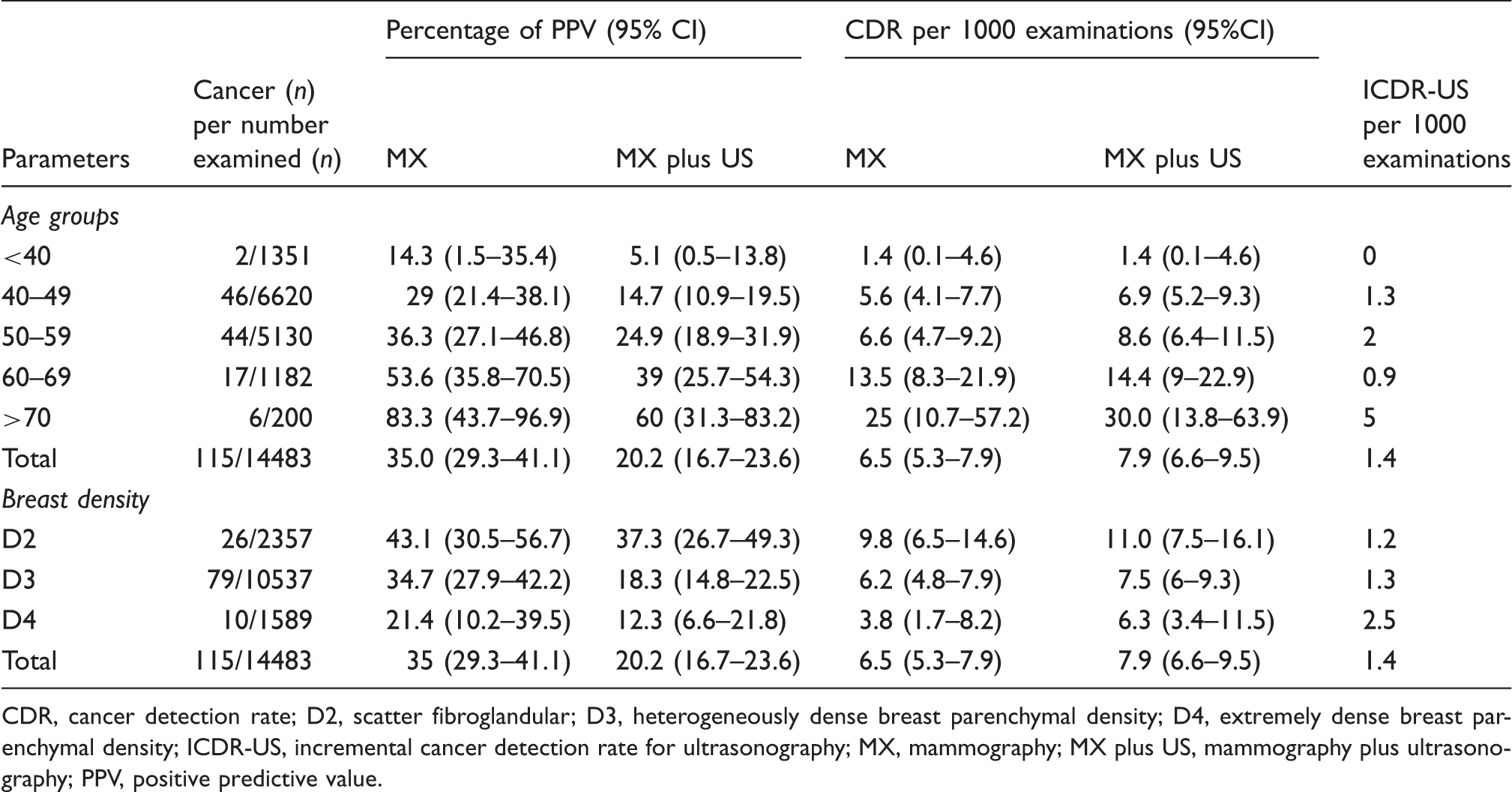
CDR, cancer detection rate; D2, scatter fibroglandular; D3, heterogeneously dense breast parenchymal density; D4, extremely dense breast parenchymal density; ICDR-US, incremental cancer detection rate for ultrasonography; MX, mammography; MX plus US, mammography plus ultrasonography; PPV, positive predictive value.
Most cancers (93%) were documented in women aged 40–69 years. According to age group, ICDR-US was highest in women aged 50–59 years (2.0 per 1000 examinations) (Table 2). ICDR-US were 1.2, 1.3, and 2.5 per 1000 examinations in women with scatter fibroglandular (D2), heterogeneous (D3), and extremely dense (D4) breast density, respectively.
Discussion
Previous publications demonstrated the benefit of MX in detection of breast cancer (3–5). In addition, adjunct whole breast US showed further benefit, in particular in women with dense breast parenchyma (4,5,12,13). Findings from our study highlighted the benefit of whole breast US in detection of breast cancer in asymptomatic non-fatty breast density. Subgroups of women who would benefit from screening US were identified, according to age and breast density. The overall ICDR-US was 1.4 per 1000 examinations, which is a statistically significant increase compared to when MX alone was used (Table 2). Previous studies documented similar findings with the ICDR of 3.4–4.6 per 1000 examinations, even higher than our study (12,14,17). High sensitivity and specificity of 96.6% and 94.9%, respectively, were evidenced in a previous study when additional screening breast US was included as a part of screening (18). The cancer detection rate was even higher in a study with additional automated whole breast US (19). These support the use of US in breast cancer screening, in particular when dense breast parenchyma is evidenced on MX (20). In women who have dense breast parenchyma, a small lesion may be occult on MX, thus breast US is useful in detection of those lesions. However, benefit of additional US must be balanced with higher false-positive rate which later leads to an increased number of biopsy. The false-positive rate of adjunct US in the previous studies varied from 0.9% to 3.1% (4,12,13,21). The use of adjunct US leads to low PPV, as demonstrated in our study (Table 2) and others (12,22). As well, the additional cost and resources used when performing US should be carefully considered (12). However, incidence of biopsied rate was improving, possibly due to better established experience of radiologist who performed US and advanced technology in high resolution US machine (12).
MX is the effective modality in detection of breast cancer, providing high accuracy. However, clinical assessment is still important. In our study, 10 women who had breast cancer (9.5%) had BI-RADS 1, 2, and 3 during MX and US done but were still diagnosed with breast cancer due to further request of the clinician in obtaining pathological or cytological examination. This highlighted the limitation of imaging in detection of breast cancer which was previously documented, in particular in invasive lobular carcinoma (23,24).
Regarding quality of MX, all MX performed in this study were full-fill digital mammogram (FFDM). Malignant conditions may be visualized better in FFDM, comparing with film-screened MX, in particular women who had high breast density (7,25). In this study, there were 29.5% of malignant lesions documented in MX alone (not in US) whereas 18.1% were documented in US alone (not in MX). Thus, additional US may add some benefit in detection of breast cancer in women who had non-fatty breast tissue. Another previous study also suggested using other modalities, apart from MX, in detection of breast cancer in non-fatty breast density (23).
Contrary to previous studies where benefit of US may be obvious in women who were aged <50 years (3), findings from our study supported that US may add some benefit for women who are aged >50 years. The explanation could be due to high percentage of D3 and D4 breast density in women aged >50 years (72.9 %). Even in women who were aged >60 years, only 9.2% had fatty breast tissue (D1). Malignant lesions were easier missed on MX in high breast density (8).
Age at first MX performed in this study was lower than as recommended by the ACR (11). Age at first diagnosis of breast cancer varies by ethnicity (26,27). Asian women tend to have early onset of breast cancer, compared with non-Hispanic white women (27). According to Table 1, in this study, there were 1355 asymptomatic women who had MX and US aged <40 years. This was due to high incidence of breast cancer in young women (age <40 years) in our region. Increased incidence of breast cancers in premenopausal women have been linked to screening and menopausal hormone use (26). In addition, prognosis and response to treatment may vary among ethnicities and ages of patients (28,29). Young women with breast cancer are likely to have more aggressive biological tumor behavior and unfavorable prognosis when compared with the cancers of older women (30). Therefore, in our institute, even in asymptomatic condition, women who were aged 35–40 years were recommended for MX at least once before entering into the normal screening program at the age of 40 years. In this study, two women with breast cancer aged <40 years had abnormalities detected in both MX and US. However, PPV was lower in MX plus US. The result from the study suggested to us that though breast cancer in this region is presented at a younger age, screening for breast cancer at age <40 years may not be useful since we could detect only two out of 1355 examinations. Also, findings from the study suggested that women aged 40–59 years received most benefit from an additional US.
Overall, women with D2, D3, and D4 breast parenchymal density received benefit from adjunct US. Overall ICDR-US was 1.4 per 1000 examinations. The most benefit was demonstrated in women with D4 breast density where ICDR-US was 2.5 per 1000 examinations (Table 2). The finding highlighted benefit of adjunct US in extremely dense breast tissue. Several previous studies demonstrated similar finding, supported use of adjunct US in dense breast parenchyma (4,5,12,22)
Nevertheless, this study had some limitations. First, findings from US were operator-dependent. Various radiologists performed breast US with their own varied experiences. Data collected into the study were not real-time data. Thus, inter-observer variation may have occurred. Second, we had a small number of women who had breast cancer in D4 and in the age >70 years subgroups. The small number may affect statistical interpretation. Further study with a larger number of patients would be statistically valuable. Finally, actual benefit of breast US alone could not be compared with MX because the radiologists were not blinded to the results of MX before performing US.
In conclusion, using supplement US adjunct to MX in of non-fatty, average-risk women for detection of breast cancer in asymptomatic women can improve detection of breast cancer in all age groups. The benefit tended to be obvious in subgroup of women who were aged 40–59 years, and in the subgroup of D4 breast density.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.