
Abstract
Background
Imaging findings of posterior cruciate ligament (PCL) injury may be equivocal, particularly when the patient has suffered a partial ligament tear. Some PCLs are positioned more horizontally, making it difficult to diagnose injury based on routine imaging planes alone due to partial volume artifact.
Purpose
To evaluate the diagnostic accuracy of combining oblique coronal imaging (PCL view) with traditional orthogonal views for PCL evaluation.
Material and Methods
This retrospective study included 20 patients with PCL injury and 43 patients with intact PCL who underwent PCL view imaging. Anatomic identification of PCL pathology on the orthogonal magnetic resonance imaging (MRI) sequences and PCL views was evaluated. Subjective scoring of the PCL was performed by two radiologists who assessed the possibility of a PCL tear based on an entire length view, an entire width view, and margin sharpness according to a 4-point scale. Diagnostic accuracy using these two views was evaluated by calculating the sensitivity, specificity, and accuracy. Arthroscopic and clinical findings were used as the reference standard.
Results
Total scores for the PCL view were higher than those of orthogonal views (P < 0.001). Both readers found that anatomic identification using the full width view and sharp margin to be superior using the PCL view compared with the orthogonal views (P < 0.001). The specificities and accuracies were higher in cases where an additional PCL view was provided, but did not show statistical significance.
Conclusion
PCL view provides better anatomic evaluation of the PCL and mild improvement in the specificity and accuracy.
Introduction
Magnetic resonance imaging (MRI) diagnosis of posterior cruciate ligament (PCL) tears is usually based on imaging characteristics including wavy contour, discontinuity, and focal or diffuse high signal intensity within the ligament on T2-weighted (T2W) images or proton density-weighted images (1). Injury of the PCL occurs less frequently than injury of the anterior cruciate ligament (ACL), and because clinical evaluation is often difficult even via arthroscopy, the diagnosis of PCL tear can be missed (2,3). Previous studies have reported that MRI may be the most reliable method for detection of a PCL injury, and that orthogonal plane imaging containing sagittal and coronal views is sufficient for evaluation of the PCL (1,4). However, we have seen a lot of confusing cases in real practice. In a considerable number of cases, imaging findings were equivocal, particularly when the patient has suffered a partial ligament tear. Rodriguez et al. (5) reported 62% of surgically proven PCL tears show apparent ligamentous continuity on MRI. Some PCLs are positioned more horizontally, making it difficult to diagnose injury based on routine imaging planes alone due to partial volume artifact. Patten et al. (6) reported that MRI findings of normal ligamentous thickness, margin, or preservation of fibers can help differentiation from false-negative cases and obtaining scans oriented directly parallel to the plane of the PCL may improve diagnostic accuracy. The purpose of this study is to evaluate the usefulness and diagnostic accuracy of combining oblique T2W coronal imaging of PCL (PCL view) with traditional orthogonal views for PCL evaluation.
Material and Methods
Case selection
We retrospectively evaluated 20 patients who were diagnosed with a PCL tear after undergoing MRI with a PCL view at our institution between January 2011 and January 2012. The PCL views were obtained from the patients routinely. The sample included 15 (75%) men and five (25%) women (mean age, 48.8 ± 10.9 years; range, 24–64 years). The same surgeon diagnosed each patient clinically. Seven patients underwent arthroscopy. The control group consisted of 43 patients who were diagnosed as having an intact PCL both radiologically and clinically. They underwent MRI with a PCL view for other causes such as meniscal injuries or other ligament injuries. The sample included 30 (70%) men and 13 (30%) women (mean age, 48.8 ± 10.9 years; range, 24–64 years). Twenty-five patients were diagnosed with a meniscal tear (14 patients in the medial meniscus and 11 patients in the lateral meniscus), five patients were diagnosed with a discoid meniscus, five patients had cartilage injury, five patients had partial tears of the medial collateral ligament, and three patients had synovial plica syndrome. Twenty-one patients underwent arthroscopy and 22 patients were diagnosed as having an intact PCL clinically based on physical examination, clinical symptoms, and radiologic finding of negative laximetry test (TELOS stress view). The same surgeon as mentioned above performed arthroscopy and diagnosed each of these patients clinically. The mean interval between MRI and arthroscopy was 20 days (range, 1–54 days) in the control group, 14 days (range, 1–28 days) in PCL tear group. The cases of posterolateral ligament complex impairment were excluded from the study because such lesion can modify the results of the physical examination of PCL injury. This study was approved by our Institutional Ethics Review Board, and the requirement for informed consent was waived due to the retrospective study design.
Clinical diagnosis
Seven of 20 patients underwent arthroscopic surgery. Operations were performed soon after the MRI, with a mean imaging to surgery interval of 15 days. No medical treatment, such as non-steroidal anti-inflammatory drugs (NSAIDs) or physical therapy, was provided during this interval. Four cases were diagnosed as partial PCL tears and three cases were diagnosed as complete tears. Other PCL tears were diagnosed based on the physical examination such as a positive posterior drawer test and clinical findings of limping, and swelling and discomfort on flexion (7). A previous study reported the posterior drawer sign to be the most accurate with an accuracy as high as 85% (8). The result of the posterior drawer test was considered positive if posterior subluxation of the tibia from the femur could be elicited with knee joint flexion (6). Radiologic findings of positive TELOS stress view and other clinical findings such as clinical course and response to the physical therapy were also included in the final diagnostic clues. An orthopedic surgeon with fellowship training in knee repair as well as 30 years of surgical experience performed all surgical procedures. During the procedure, the surgeon examined the continuity of the ligament and degree of swelling of the PCL. Once the radiologists had conducted their blind reading of the MR images, the surgeon and radiologists correlated the surgical and imaging findings.
MR parameters
All MRI was performed according to the same protocol using a 3.0 T magnet MRI scanner (Achieva, Philips Medical Systems, Best, The Netherlands) with an 8-channel knee coil. The sequences and imaging parameters are summarized in Table 1. Additional PCL views were obtained using the following parameters: TR/TE, 2000–3000/50–80; field of view, 14 cm; echo train length, 13; matrix, 450 × 350; slice thickness, 3 mm. The PCL view was obtained in the plane parallel to the line between the femoral and tibial insertion sites of the PCL based on conventional sagittal T2W images (Fig. 1).
Sagittal T2W image demonstrating the technique for obtaining the oblique coronal series. PCL views were obtained using 3-mm slice thickness parallel to the PCL insertion site on the femur and tibia. Imaging parameters for the MR sequences at 3T. FS, fat saturation; FSE, fast spin-echo; PD, proton density.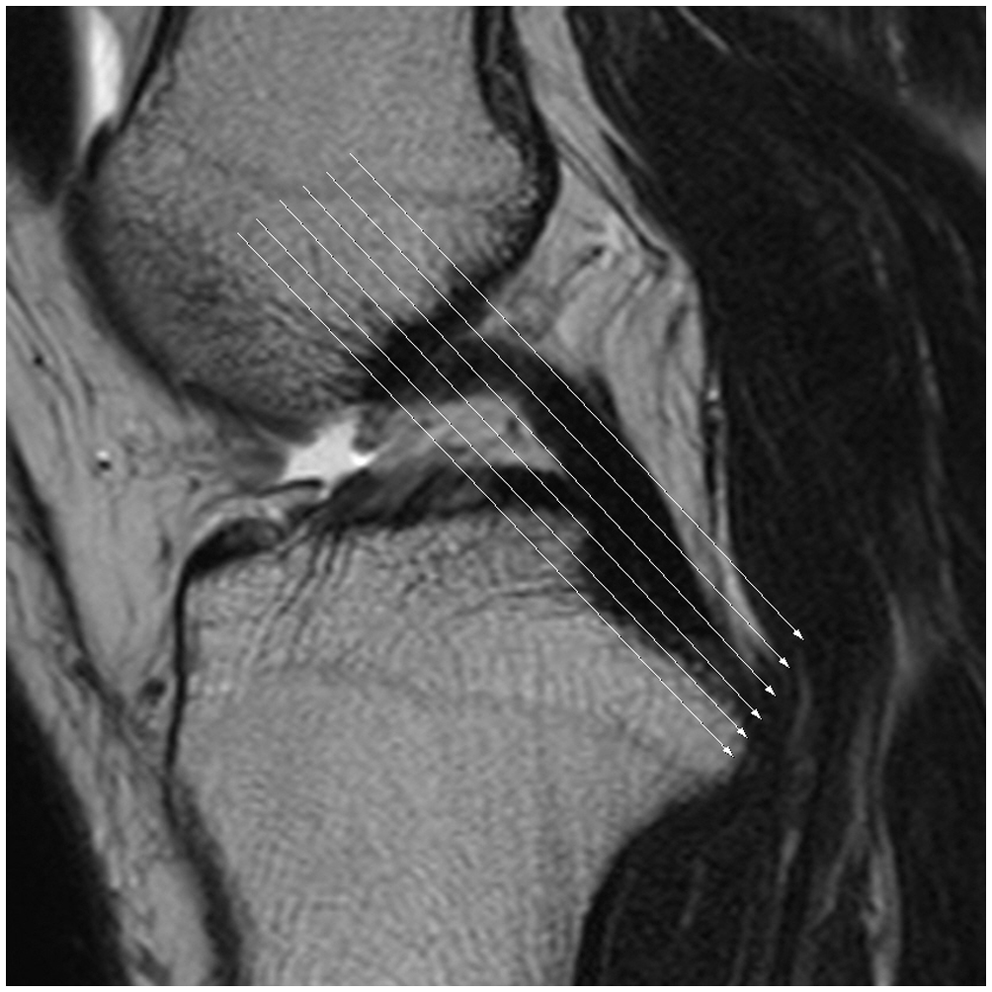
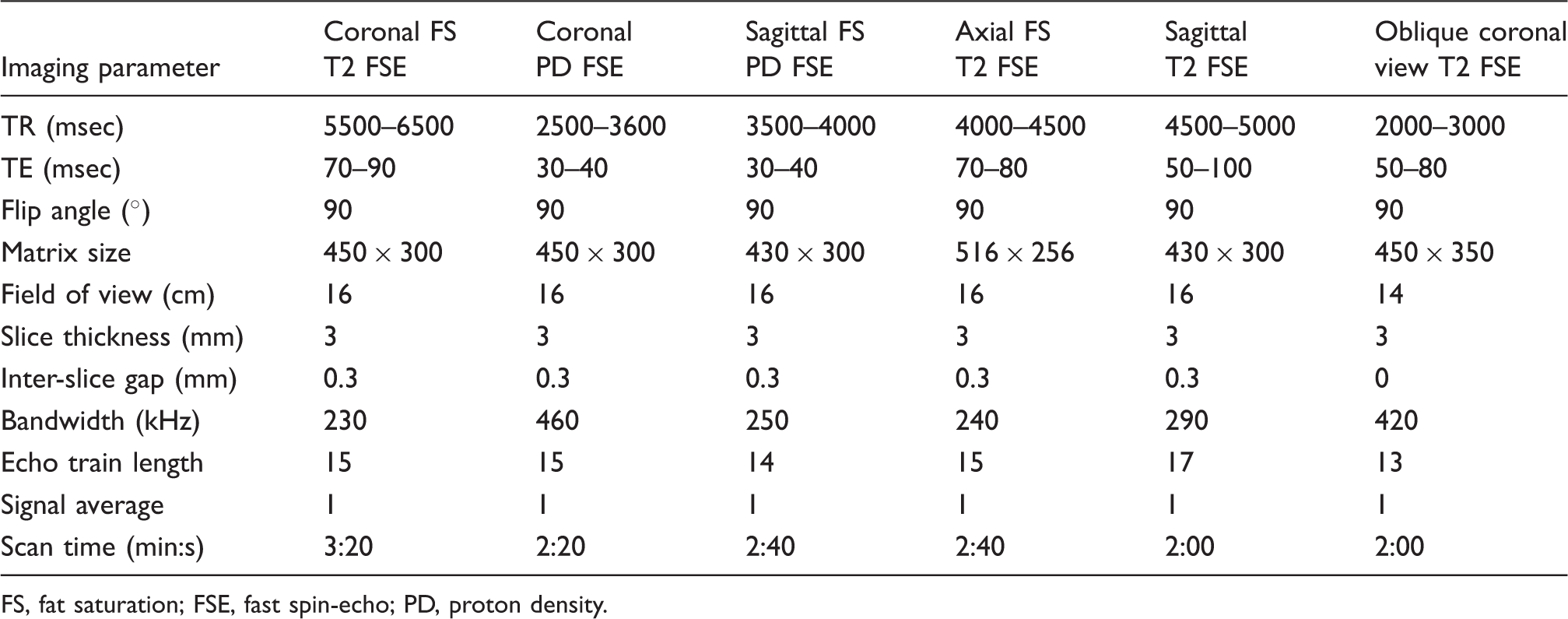
Image analysis
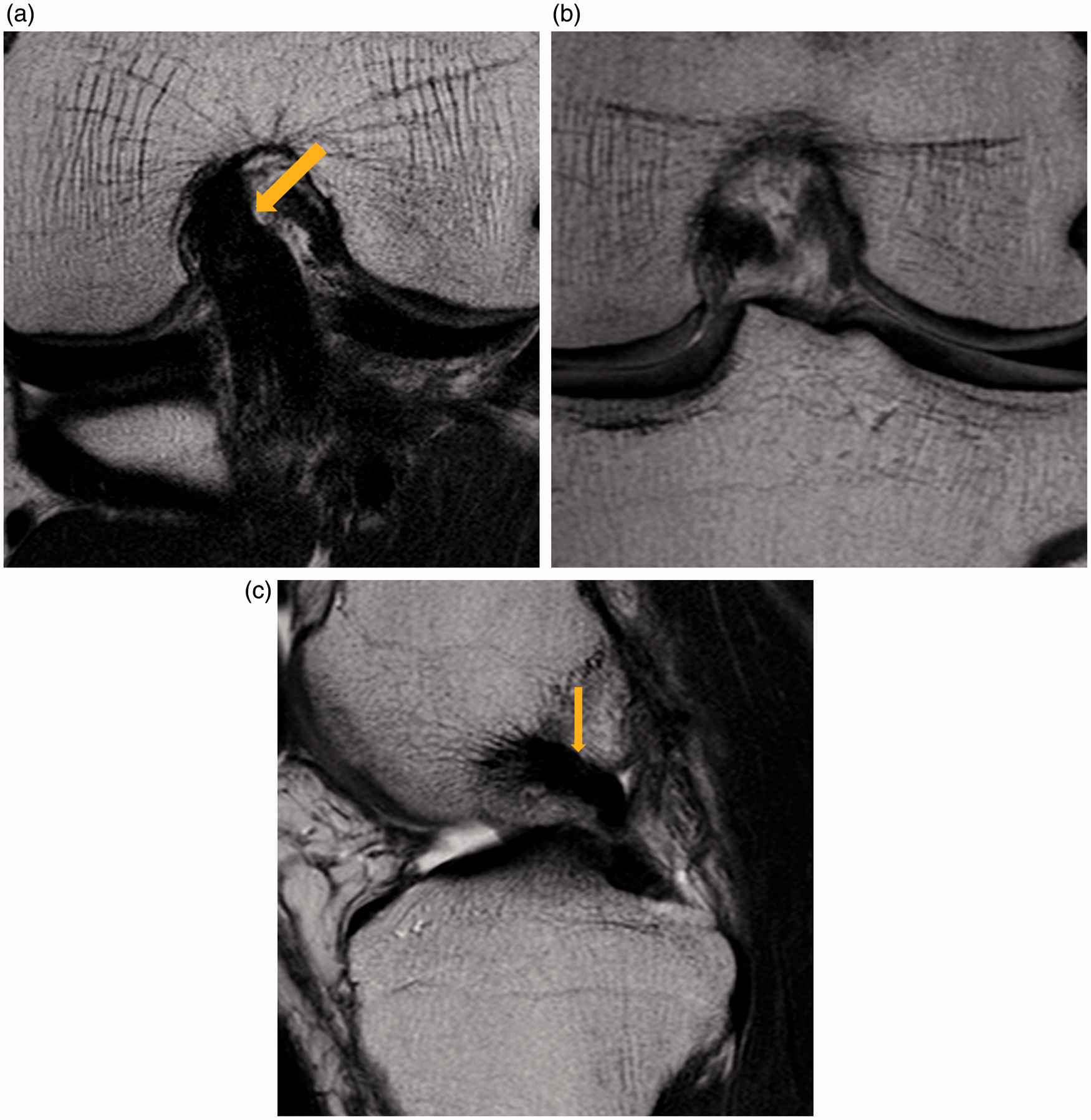
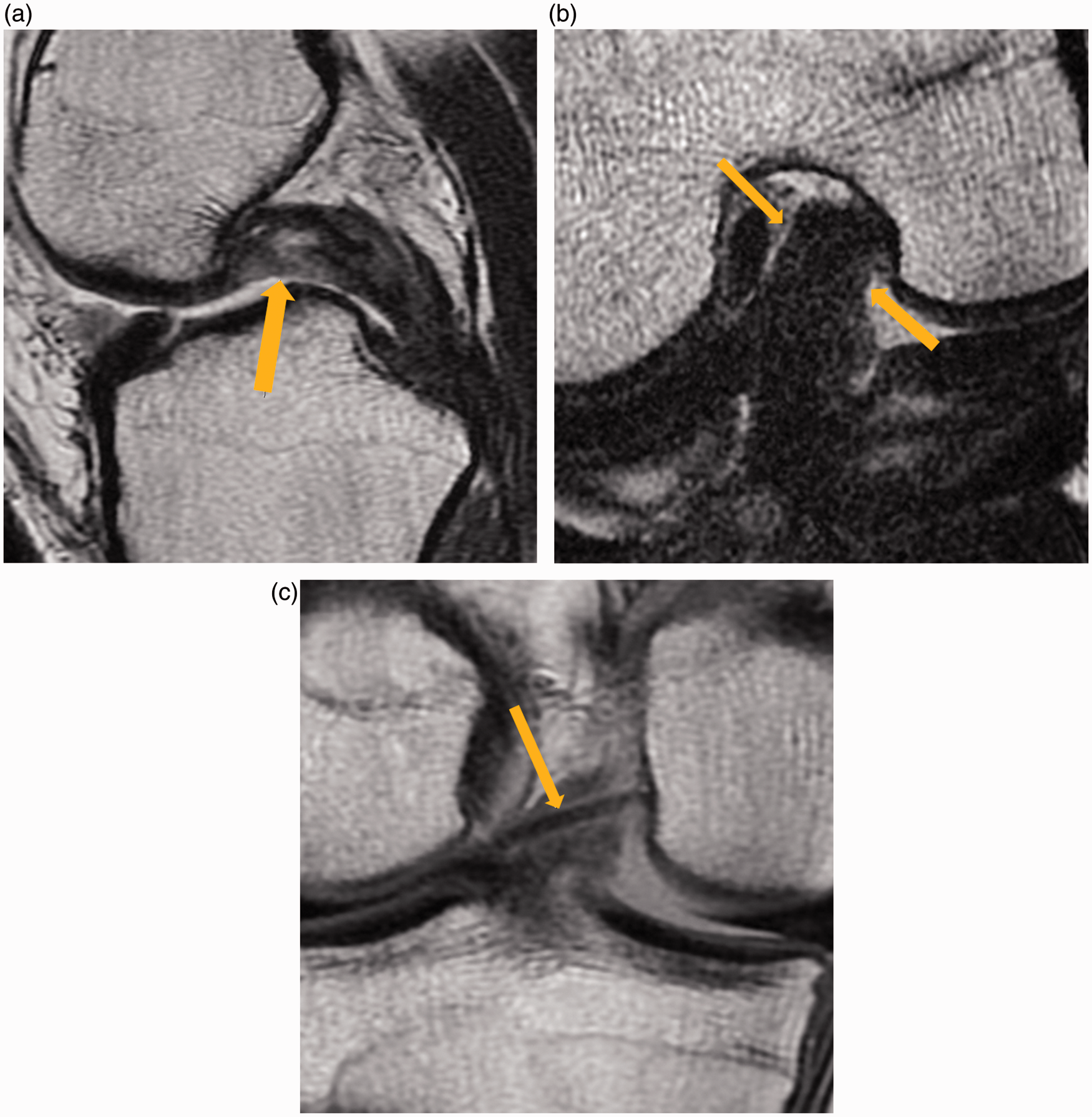
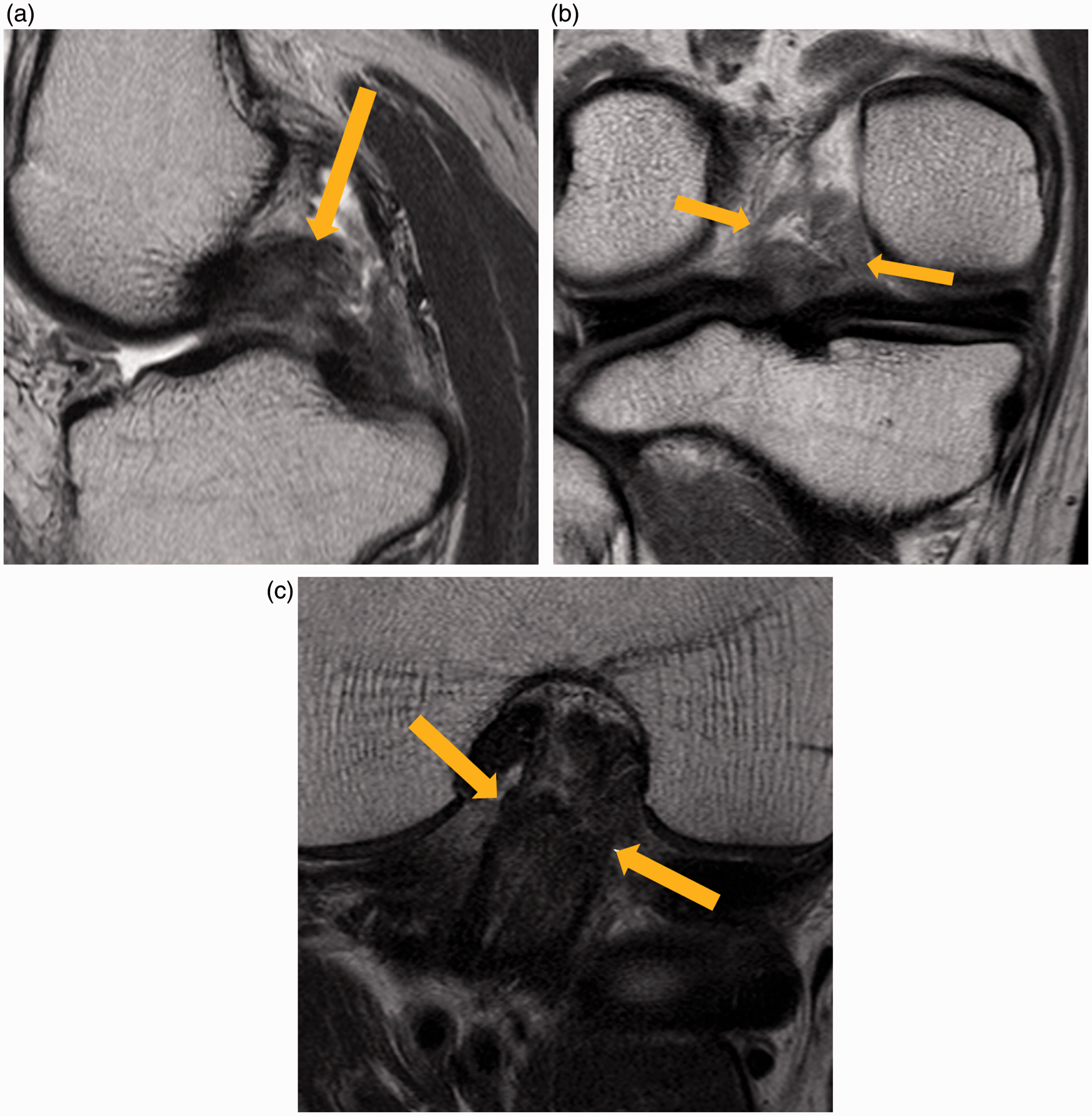
MR images were interpreted separately by two fellowship-trained musculoskeletal radiologists with 12 and 10 years of experience, who were blinded to clinical information and radiologic reports. The PCL tear group and control group were mixed randomly for the reading session. Anatomic identification of PCL pathology on orthogonal MRI sequences (sagittal T2W images and coronal proton density imaging) and the PCL view without routine sequences was evaluated. Subjective scoring of the PCL images was performed using abilities of discrimination through entire length (entire length), through entire width (entire width), and margin sharpness according to a 4-point scale (0, poor; 1, fair; 2, good; 3, excellent). The entire length score means whether the reader can perform longitudinal evaluation of the ligament from femoral end to tibial end completely. The entire width score means whether the reader can perform transverse evaluation of the ligament from medial edge to lateral edge. The diagnostic accuracy of the orthogonal MRI sequences and orthogonal MR images with additional PCL view was evaluated. The PCL was considered intact if a continuous line of low signal intensity was observed (Figs 2 and 3) (6). The PCL was considered to have a partial tear if a wavy contour or a thin but continuous band was observed, or if there was focally or diffuse high signal intensity within the PCL itself (Fig. 4). The PCL was considered to have a complete tear if there was evidence of definite discontinuity (Fig. 5).
Images from a 46-year-old man with knee pain for 3 months. There was injury to the cartilage in the femoral condyle and the PCL was intact. (a) PCL view (TR/TE, 2700/60) showing the entire width and sharp margin. (b) Orthogonal proton density coronal MR image (TR/TE, 3300/30) of the PCL showing a small portion of the PCL and a less sharp margin. (c) Sagittal T2W MR image (TR/TE, 4500/60) of the PCL showing irregularities in the proximal portion of the PCL due to partial volume averaging artifact. A 48-year-old man with knee pain for 3 years due to synovial plica syndrome with an intact PCL. (a) PCL view (TR/TE, 2700/60) showing the entire width and sharp margin. Focal indentation is seen at the proximal portion of the PCL (arrow). (b) Orthogonal proton density coronal MR image (TR/TE, 3300/30) of the PCL showing a small portion of the PCL and a less sharp margin. The indentation seen on the PCL view is absent in this image. (c) Sagittal T2W MR image (TR/TE, 4500/60) of the PCL showing only mild indentation of the proximal PCL which is seen prominently on the PCL view (arrow). A 17-year-old man with a history of knee trauma. A partial rupture of the PCL was diagnosed on arthroscopy. (a) Sagittal T2W MR image (TR/TE, 4700/70) of the PCL showing focal bright signal and discontinuity in the proximal portion of the PCL (arrow). (b) PCL view (TR/TE, 2700/80) showing a sharp margin and nearly whole contour of the PCL (arrow). Continuity of the PCL remains intact. (c) Orthogonal proton density coronal MR image (TR/TE, 2500/35) of the PCL showing poor demarcation of the PCL and the overlapping meniscofemoral ligament (arrow). A 56-year-old man with history of falls. Complete rupture of the PCL was diagnosed on arthroscopy. (a) Sagittal T2W MR image (TR/TE, 4500/100) of the PCL showing the disrupted PCL (arrow). (b) Orthogonal proton density coronal MR image (TR/TE, 3300/30) of the PCL showing disruption and poor demarcation of the PCL (arrow). (c) PCL view (TR/TE, 2700/60) showing the disrupted PCL. In this image, evaluation of the full width can be performed (arrow).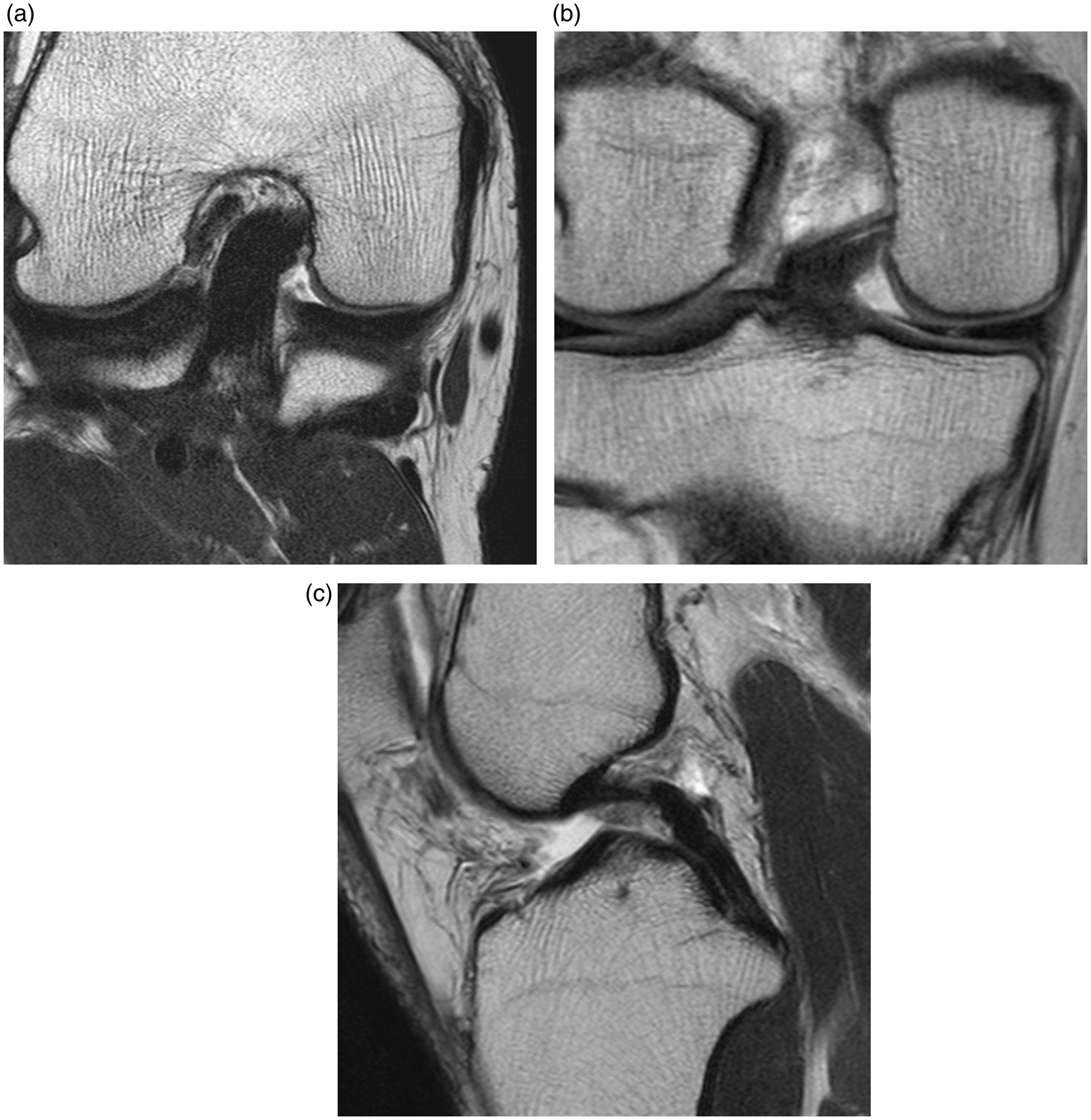
Statistical analysis
Anatomic identification using orthogonal MRI compared with the PCL view only, as graded by the two radiologists, was evaluated using paired Student’s t-tests, and inter-observer agreement between the two radiologists was analyzed using an intra-class correlation coefficient (ICC). ICC values <0.40 were indicative of poor reproducibility, while ICC values of 0.40–0.75 indicated fair-to-good reproducibility. ICC values which were >0.75 indicated excellent reproducibility. Wilcoxon signed-rank tests were used to determine the statistical significance of the anatomic identification score. Inter-observer agreement of diagnostic performance was analyzed using kappa statistics. The kappa value interpretation was as follows: poor (k < 0.1); slight (0.1–0.2); fair (0.2–0.4); moderate (0.4–0.6); substantial (0.6–0.8); and nearly perfect (0.8–1). Diagnostic performance was evaluated using the sensitivity, specificity, and accuracy for diagnosing a PCL tear as determined by the use of orthogonal images without and with an additional PCL view, respectively. The arthroscopic and clinical findings were used as the reference standard. The values (sensitivity, specificity, and accuracy) were statistically analyzed using the McNemar test. Statistical analyses were performed using PASW software version 18.0 (IBM, Armonk, NY, USA), and P values ≤ 0.05 were considered to be statistically significant.
Results
Intra-class correlation coefficients of anatomic identification scores.
Entire length = ability of discrimination through entire length.
Entire width = ability of discrimination through entire width.
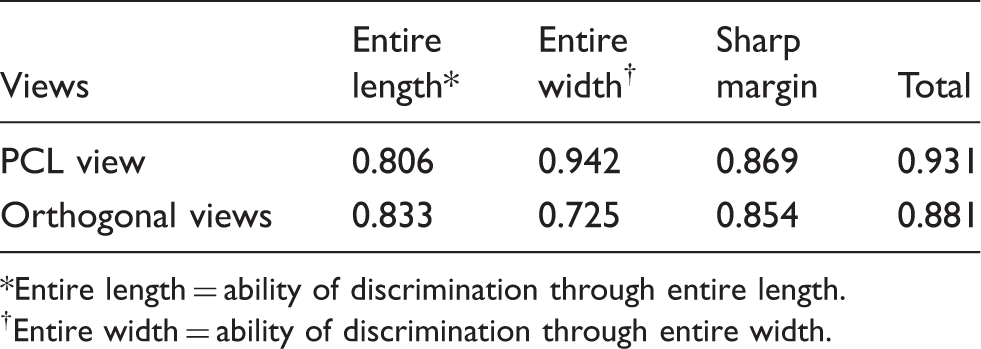
Mean scores for anatomic identification of PCL pathology on the PCL view.
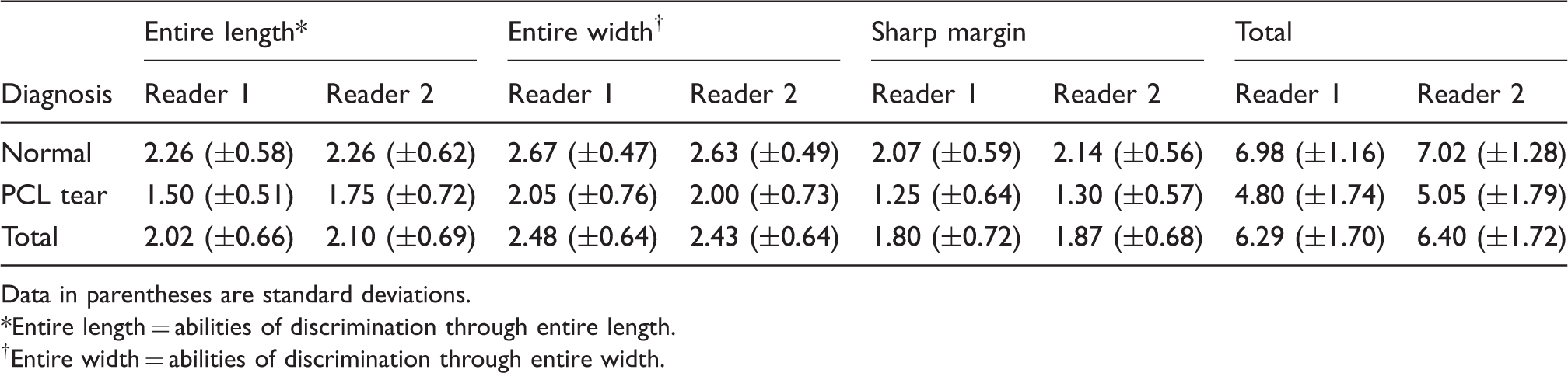
Data in parentheses are standard deviations.
Entire length = abilities of discrimination through entire length.
Entire width = abilities of discrimination through entire width.
Mean scores for anatomic identification of PCL pathology on orthogonal views.
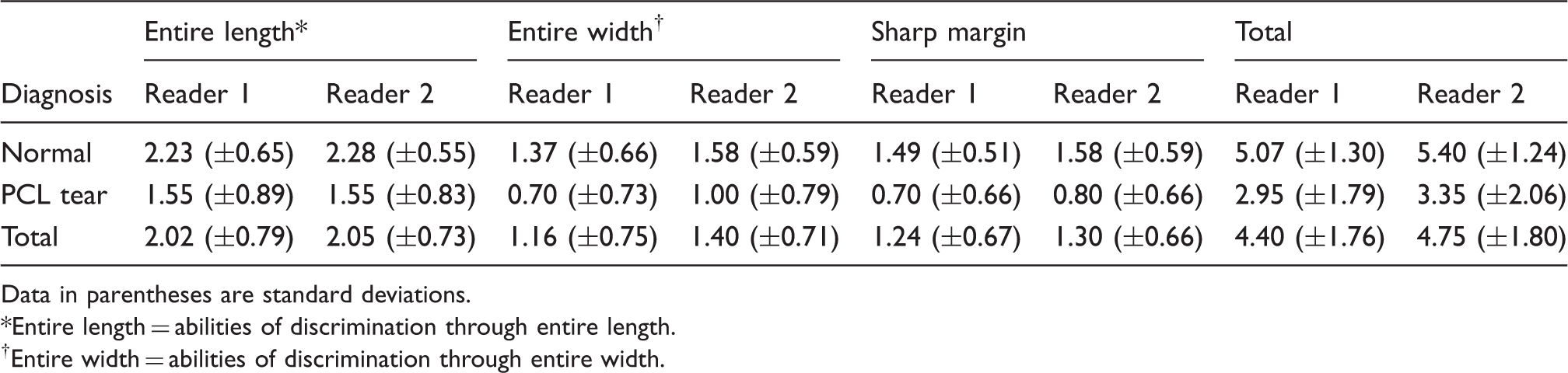
Data in parentheses are standard deviations.
Entire length = abilities of discrimination through entire length.
Entire width = abilities of discrimination through entire width.
Sensitivity, specificity, and accuracy of using the PCL view with orthogonal view (A) and the orthogonal view alone (B) in diagnosing PCL tears.

Numbers in parentheses are the numbers of patients used to calculate the percentages.
Discussion
The PCL is a spirally oriented fiber bundle that courses from the lateral aspect of the medial femoral condyle to its insertion on the posterior aspect of the intra-articular tibia. The PCL subtends a vertical angle of 30–45 degrees, depending on the degree of flexion (1). The normal PCL has low signal intensity on MRI and is arcuate in shape when the knee is in a neutral position or mild flexion, which is a common position for physical examination and MRI (4). Correct diagnosis of the PCL injury whether the lesion is partial tear or full thickness tear is important to the patient management because full thickness tears require surgical repair whereas partial tears can be conservatively treated (6). The presence of at least some intact ligamentous fibers on MRI is very important differential diagnostic point between partial tear and full thickness tear (6). Sagittal MR images are the most important in the diagnosis of PCL injury, since the majority of PCL injuries occur in the middle of the fiber bundle (1). However the entire course of the PCL is not clearly depicted on routine sagittal images and the curvilinear course of the PCL does not permit sufficient evaluation in the axial or coronal planes. Therefore, the need for oblique coronal imaging has become evident. The usefulness of oblique coronal images in the evaluation of injuries to the ACL, which is positioned similarly but in the reverse direction, is well established (9,10). Additionally, oblique coronal images can be applied to decrease partial volume averaging and to achieve full-width visualization of the PCL. Kwon et al. (9) reported that changes in the thickness signal intensity, continuity, and contour can be seen more easily on oblique coronal views in the evaluation of the ACL. We assumed that similar results might be found on oblique coronal views in the evaluation of the PCL. Our scoring system for anatomic identification showed excellent reproducibility (ICCs = 0.93 in the PCL view and 0.88 in the orthogonal views). In the evaluation of anatomic identification of PCL pathology, the PCL view was superior to the orthogonal view with regards to entire width and margin sharpness, but similar results were seen for both image types in the evaluation of the entire length view. We propose that the PCL view may be superior due to its ability to visualize the entire width of the PCL along a parallel axis, providing accurate information concerning the attachment site to the distal femur. We investigated whether addition of oblique coronal images influenced the sensitivity, specificity, and accuracy of the diagnosis of PCL tears. The kappa values of inter-observer agreements for diagnosis (that is, whether the lesion is normal, partial tear, or full thickness tear) were 0.927 in PCL view and 0.735 in orthogonal views, which mean superior reproducibility of PCL view to orthogonal views. Table 5 reveals very high values of sensitivity and specificity. We can assume that MRI of the PCL, whether on the PCL view or on orthogonal views, enables differential diagnosis of a partial tear from a full thickness tear. Our results suggest that additional PCL views may reduce false-negative diagnoses and may increase specificity and accuracy in diagnosing PCL injuries. These results, however, did not show statistical significance. We were unable to prove that the addition of the PCL views improved the ability to diagnose PCL tears in general, but in cases of diagnostic uncertainty the PCL view may be helpful in distinguishing partial tear from volume averaging artifact.
One of the limitations of this study was the lack of surgical confirmation of PCL tears. Only 35% of patients who were diagnosed with a PCL tear underwent arthroscopic surgery. However, great care was taken to acquire the best possible standard of reference in the other cases using clinical findings as well as all available MR sequences and follow-up MR. A second limitation was that our study lacked objective quantitative analysis of the anatomic identification of PCL pathology. We relied on a subjective scoring system, however as the ICCs between readers were very high, the scores are likely quite accurate. Finally, our study included a relatively small number of positive cases.
In conclusion, PCL views provide better anatomic evaluation and mild improvement in specificity and accuracy in diagnosing PCL injuries, though not statistically significant. PCL views can be considered as an ancillary method in equivocal cases of possible PCL injury.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.