
Abstract
Background
Right adrenal vein (RAV) catheterization can be a very challenging step in adrenal venous sampling (AVS). Visualization of the inferior emissary vein (IEV) may be an indication of successful RAV catheterization.
Purpose
To compare the rate of successful RAV sampling in the presence of the IEV.
Material and Methods
Retrospective review of all consecutive patients with PA who underwent AVS between April 2009 and April 2012 was performed. A total of 30 patients were identified. Procedural images, cortisol, and aldosterone values obtained from sampling of the RAV and inferior vena cava (IVC) were reviewed. Cortisol measurements obtained from RAV samples were divided by measurements from the infra-renal IVC blood samples in order to calculate the selectivity index (SI). An SI >3 was considered indicative of technically successful RAV sampling.
Results
RAV sampling was considered technically successful in 29 out of 30 cases (97%). In cases of successful RAV sampling (29 patients), the IEV was identified in 25 patients (86%). The IEV was visualized in isolation in 16 patients (64%), and in conjunction with visualization of the RAV or right adrenal gland stain in nine patients (36%). The IEV was not visualized in the one case of unsuccessful RAV sampling. Visualizing the IEV had a sensitivity of 86.2% for successful RAV sampling.
Conclusion
The IEV may serve as a reliable landmark for the RAV during RAV sampling.
Introduction
Adrenal venous sampling (AVS) has become the gold standard for localization of lesions responsible for primary aldosteronism (PA) (1). Successful catheterization of the right adrenal vein (RAV), however, can be a challenging step in AVS (2). In addition, the RAV can be confused with adjacent hepatic veins draining the caudate lobe of the liver.
A number of emissary veins arise from the surface of both adrenal glands and extend into the perirenal fat (3). On the right side, the emissary veins commonly course laterally, medially or inferiorly with respect to the adrenal gland and may communicate with the right renal vein, intercostal veins, phrenic veins, or the IVC (4). Visualization of the emissary veins has been described as confirmation of RAV catheterization (4).
In our clinical practice, we have also come to recognize the inferior emissary vein (IEV) during RAV sampling (Fig. 1). The purpose of this study was to evaluate the rate of successful RAV sampling in the presence of the IEV.
Inferior emissary vein (IEV), coursing inferomedially.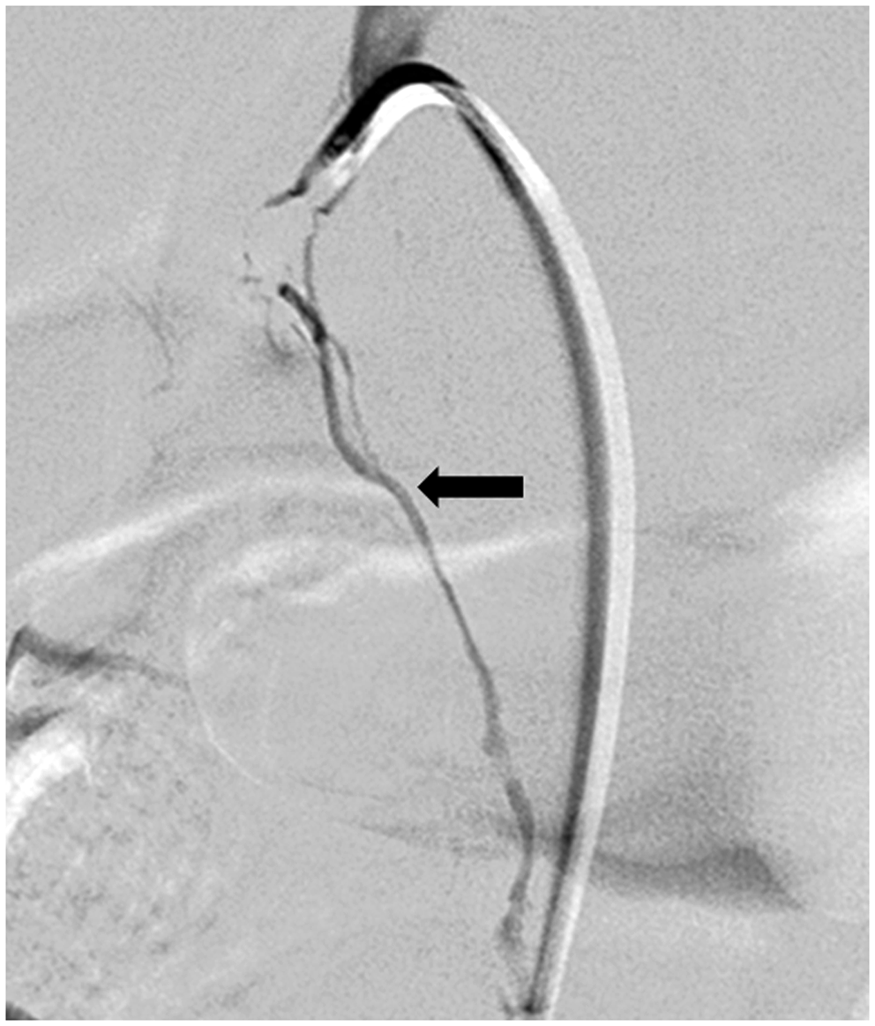
Material and Methods
Patients
This retrospective study was approved by our Institutional Review Board. Informed consent requirement was waived. A retrospective record review of all consecutive patients with PA who underwent AVS between April 2009 and April 2012 at our institution was performed. A total of 30 patients were identified (17 men, 13 women) with a median age of 53 years (age range, 13–68 years).
AVS procedure
AVS was performed on an outpatient basis using moderate sedation. Our sampling protocol entailed continuous intravenous infusion of cosyntropin (Cortrosyn, Amphastar Pharmaceuticals, Rancho Cucamonga, CA, USA) 0.25 mg in 500 mL normal saline infused at 100 mL/h for at least 1 h prior to and continuous throughout the AVS procedure.
Sampling was performed via a transfemoral approach in all patients using a 5-French Cobra 2 catheter (Cook Medical, Bloomington, IN, USA). In certain cases, a 5-French SOS catheter (AngioDynamics, Latham, NY, USA), Simmons 1 and Simmons 2 catheters (Cordis, Miami Lakes, FL, USA), and coaxially placed 3-French microcatheter (Renegade Hi-Flo, Boston Scientific, Natick, MA, USA) were used, when considered appropriate by the interventional radiologist. Single 5 mL blood samples were obtained from the infra-renal IVC and from each adrenal vein. Serum cortisol and aldosterone levels were measured for all samples.
For the purpose of this study, cortisol values from samples of the RAV and the infra-renal IVC were reviewed. Cortisol measurements obtained from RAV samples were divided by measurements from the infra-renal IVC blood samples in order to calculate the selectivity index (SI). Since all patients underwent adrenocorticotropic hormone (ACTH) stimulation, an SI >3 was used as evidence of technically successful RAV sampling (5).
Results
RAV sampling was considered technically successful in 29 out of 30 cases (97%). In cases of successful RAV sampling (29 patients), the IEV was identified in 25 patients (86%). The IEV was visualized in isolation in 16 patients (64%, Fig.1), and in conjunction with visualization of the RAV or right adrenal gland stain in nine patients (36%, Fig. 2). Of note, the IEV was not visualized in the one case of unsuccessful RAV sampling.
Inferior emissary vein (IEV), coursing inferomedially (open arrow) in conjunction with stain of the right adrenal gland (solid arrow).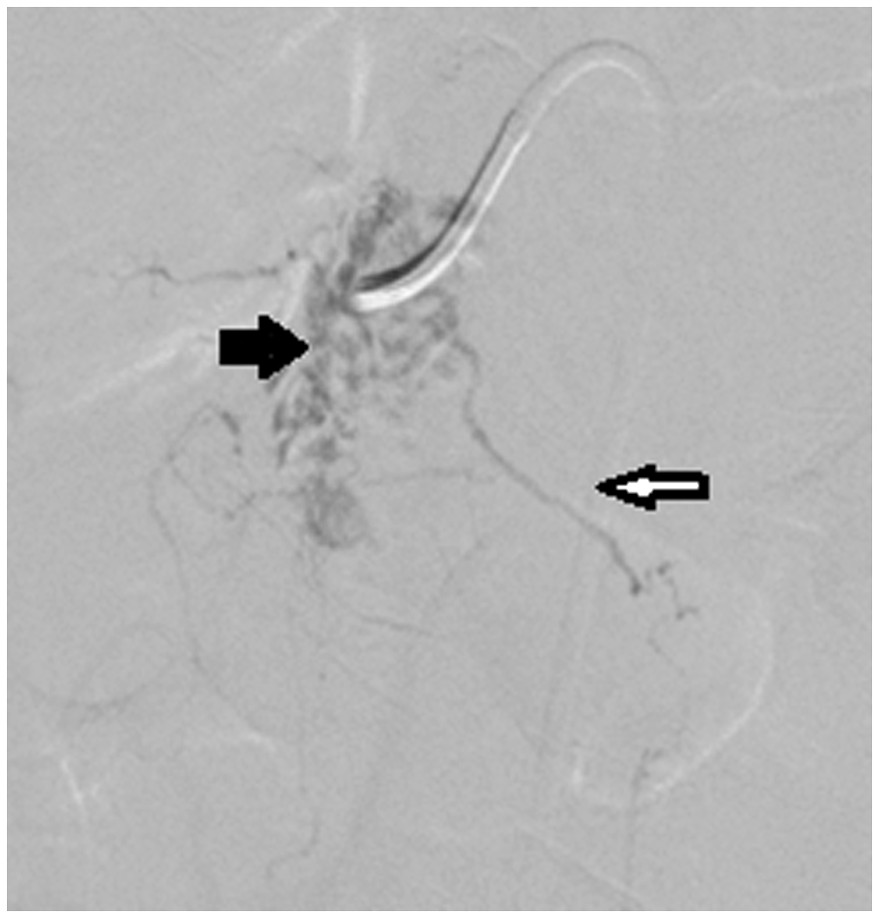
In the four cases of successful RAV sampling without visualization of the IEV, the RAV or the stain of the right adrenal gland was visualized (Fig. 3).
Stain of the right adrenal gland.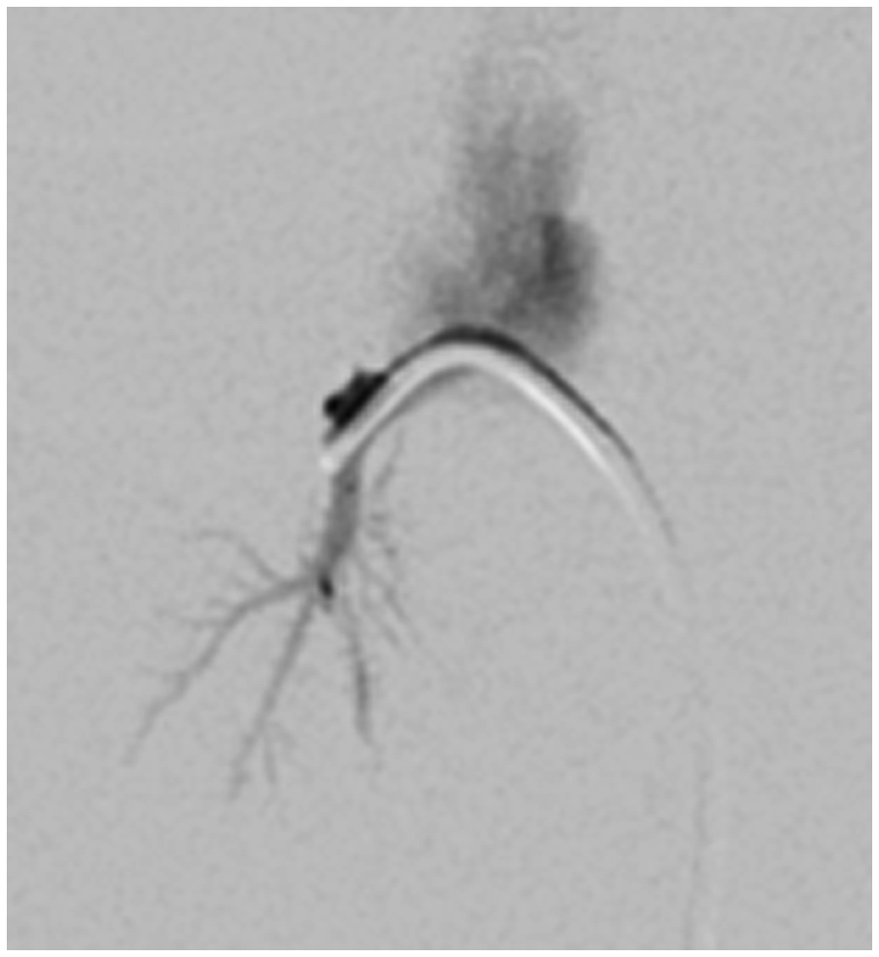
In our cohort, visualizing the IEV had a sensitivity of 86.2% (25/29) (binomial exact 95% confidence interval, 68–96%). Given only a single case of unsuccessful RAV sampling was included, which did not demonstrate the IEV, an accurate estimation of the specificity and positive predictive value (PPV) is limited (point estimates for specificity [1/1] and PPV [25/25] are both 100%).
Discussion
PA is the most common form of secondary hypertension (6). The two most common subtypes of PA are aldosterone-producing adenoma and bilateral adrenal hyperplasia (7). Distinction between these two etiologies is important as treatment for aldosterone producing adenoma is adrenalectomy, whereas bilateral adrenal hyperplasia is treated with mineralocorticoid receptor antagonists (7).
AVS is a technically challenging procedure mainly due to the difficulty in identifying and catheterizing the RAV (4). Due to the short length, anatomic variance of the RAV, and its proximity to the hepatic veins draining the caudate lobe, technical failure rates are common and result in repeat procedures in as many as 30% of patients (8).
Multiple techniques to improve technical success of RAV sampling have been previously reported. Georgiades et al. (8) reported the use of C-arm CT to confirm the location of the sampling catheter during AVS. In their report, C-arm CT images demonstrated a malpositioned RAV sampling catheter in two out of nine patients (22%) and resulted in catheter repositioning and successful RAV sampling. They reported a technical failure rate of 0% as C-arm CT allowed for real-time intra-procedural confirmation of sampling catheter position.
Miotto et al. (9) and Matsuura et al. (10) have reported the presence of a common trunk shared by the RAV and the inferior accessory hepatic vein (IAHV). Awareness of this anatomic variant may help during the procedure and also explain inadequate RAV sampling (9). Matsuura et al. (10) advocated the use of MDCT to help delineate the anatomy of the RAV, in light of the common trunk shared by the IAHV.
Trerotola et al. (11) have recommended using the IAHV as a landmark for RAV sampling. In their report, the RAV was immediately adjacent to the IAHV (i.e. distance of 0 mm) in 29% of the cases and was within 5 mm of the IAHV in the remaining 71% of cases when the IAHV was visualized. They found that when the IAHV was identified (58% of patients), RAV sampling was successful in 95% of the case.
While intra-procedural CT may aid in localization of the RAV (8,10), it increases patient radiation dose. Visualization of the IAHV may serve as a good landmark for the RAV without additional radiation. However, it was noted to be present in little over half of the patients undergoing AVS (11). Additionally, when identified, RAV sampling was technically successful in 95% of the cases. In contrast to the IAHV, the venous structure described in our report was identified in 83% of patient undergoing AVS and was always present in cases of successful RAV sampling.
In our experience, the IEV was visualized is almost all (86%) cases of successful RAV sampling. Additionally, visualization of the IEV was as sensitive and useful as visualization of the RAV or the stain of the right adrenal gland for the purpose of intraprocedural verification of correct catheter positioning. Therefore, the IEV may serve as a reliable landmark for the RAV during RAV sampling.
Our study is limited by its retrospective, single-center design and a relatively small number of patients. Due to the retrospective nature of the study, intra-procedural C-arm CT was not performed to identify the exact course of the IEV.
In conclusion, visualization of the IEV in isolation or conjunction with visualization of the right adrenal gland or RAV, is likely an excellent indicator of successful catheterization of the RAV.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.