
Abstract
Background
Given that transarterial chemoembolization (TACE) is usually a repeated procedure for treatment of hepatocellular carcinoma (HCC), repeated radiologic response assessments rather than a single time point assessment may have different clinical implications through the repeated course of TACE.
Purpose
To evaluate the efficacy of RECIST and mRECIST criteria as a survival predictor across early time points after repeated TACE of HCC.
Material and Methods
Ninety-eight patients with intermediate stage HCC received repeated iodized oil TACE. Treatment response was assessed according to RECIST and mRECIST criteria at 1, 3, and 6 months after initial TACE. Cox proportional model was used for survival analysis and the predicting power of each time point response was evaluated with C-statistics and time-dependent area under the receiver operating characteristic curve (AUC). Inter-method agreement was assessed with the κ coefficient.
Results
mRECIST was not applicable in 15 patients because of patchy uptake of iodized oil after TACE. On multivariate analysis, responders at 6 months by RECIST, responders at 3 months, and 6 months by mRECIST showed better survival than non-responders (P < 0.05). Predicting power of response criteria improved over time and mRECIST at 6 months showed the best performance. The degree of agreements was poor or fair between RECIST and mRECIST.
Conclusion
mRECIST predicted long-term survival as early as 3 months after TACE of intermediate stage HCC. The predicting power of the uni-dimensional response criteria tended to be stronger over time.
Introduction
Hepatocellular carcinoma (HCC) is one of the leading causes of cancer-related death (1). The treatment of HCC includes curative treatments, such as surgical resection or transplantation, and palliative treatments typified by transarterial chemoembolization (TACE) or sorafenib (2,3). TACE is the recommended standard treatment for intermediate-stage HCC based on the results of prospective randomized studies (2–7).
Radiological assessment of tumor response to locoregional treatment of HCC has been known to be associated with survival (8–13). However, there are substantial differences between the studies regarding the optimal method and the best timing of assessment. Furthermore, in systemic chemotherapy, if once progression is met, it is seen as treatment failure which leads to change in therapy. However, locoregional therapy of HCC, especially TACE is different. Disease progression may be successfully treated by locoregional therapy and TACE can be repeated until tumors are defined as untreatable progression such as massive liver involvement and extraphepatic spread, or liver failure which prevents safe retreatment (14). Given this daily practice, we speculated that the repeated assessment of response to repeatedly performed TACE may have clinical implications.
Currently, four radiologic response criteria are mostly used in clinical trials or daily practice, which are based either on the tumor size measurements (World Health Organization [WHO] or Response Evaluation Criteria in Solid Tumors [RECIST]) or on the contrast enhancement measurements (European Association for the Study of Liver [EASL] or modified RECIST [mRECIST]) (15–18). Although bi-dimensional criteria (WHO and EASL) seem intuitively more representative of actual treatment response than uni-dimensional criteria (RECIST and mRECIST), uni-dimensional criteria are easier to measure and more reproducible because this considers only the longest diameter of the tumor (11).
The purpose of this study was to analyze the role of uni-dimensional (RECIST and mRECIST) criteria as a prognostic factor in HCC patients which were assessed at 1, 3, and 6 months following TACE of HCC.
Material and Methods
Patients and enrollment criteria
The Institutional Review Board of our hospital approved this retrospective study and informed consent was waived. A total of 591 patients underwent TACE as the first line therapy at our hospital from January 2009 to April 2011. Among them, 98 patients were enrolled in this study. The inclusion criteria were as follows: (i) Barcelona Clinic Liver Cancer (BCLC) intermediate stage HCC (2,4); (ii) liver function of Child-Push classification A; (iii) no prior tumor treatment before TACE; and (iv) clinical and radiological follow-up of at least 6 months during which TACE was the only active treatment for HCC. The diagnosis of HCC was based on contrast-enhanced dynamic computed tomography (CT) findings (arterial hypervascularity and portal venous or delayed phase washout) (2). CT was performed with a 64-channel MDCT scanner (LightSpeed VCT; GE Healthcare, Milwaukee, WI, USA). Axial images were obtained 20–35 (arterial phase), 60–70 (portal venous phase), and 180 (delayed phase) s after i.v. contrast material injection by the bolus-tracking technique. A maximum slice thickness of 5 mm was used for CT scanning. Additional magnetic resonance imaging (MRI) was performed in 13 patients when CT findings were atypical or inadequate for the diagnosis of HCC. A 3 T whole-body MRI system (Intera Achieva 3.0 T; Philips Healthcare, Best, The Netherlands) with a 32-channel phased-array coil was used for gadoxetic acid-enhanced MRI. The liver was imaged both before and after administration of gadoxetic acid (Primovist; Bayer Schering Pharma, Berlin, Germany) at a dose of 0.1 mL/kg (0.25 mmol/mL). For dynamic imaging, arterial phase (20–35 seconds), portal phase (70 seconds), equilibrium phase (3 minutes), and 20-min delayed hepatobiliary phase images were obtained with a T1-weighted (T1W) 3D turbo-field-echo sequence (T1 high-resolution isotropic volume examination, THRIVE, Philips Healthcare) with a 2-mm section thickness, no intersection gap, and a field of view of 32–38 cm. Histological diagnosis with percutaneous biopsies was made in six patients.
TACE protocol and follow-up
After catheterization of hepatic and mesenteric arteries with a 5-F catheter (Yashiro; Terumo, Tokyo, Japan or RH; Cook, Bloomington, IN, USA), digital subtraction angiography was performed to map the vascular liver anatomy to determine the presence of tumor staining and to identify the arterial feeders of the tumor. A co-axial 2-F (Progreat α; Terumo) or 2.4-F (Microferret; Cook) microcatheter was then selectively inserted as close as possible to the tumor feeding arteries. Selective TACE was performed through the microcatheter with transarterial infusion of a mixture of iodized oil (Lipiodol; Laboratoire Andre Guerbet, Aulnay-sous-Bois, France) and doxorubicin hydrochloride (Adriamycin; Dong-A Pharm, Seoul, Republic of Korea). The doses of iodized oil (5–20 mL) and doxorubicin (10–60 mg) depended on the size and vascularity of the tumor. Transarterial infusion of the drug mixture was followed by embolization of the tumor feeding artery with gelatin sponge pledgets (Cutanplast; Mascia Brunelli, Milan, Italy), which were manually cut into approximately 1 mm3 pieces. Embolization was performed until the blood flow of the tumor feeding artery ceased. Patients were followed with MDCT 1 month after TACE. When residual and/or recurrent tumors were noted, TACE was usually repeated within 1 month of the CT evaluation. Once no radiological evidence of residual tumor or recurrence was noted, CT and/or MRI were performed every 2–3 months thereafter.
Assessment of treatment response
Treatment response was retrospectively assessed by RECIST and mRECIST criteria (15,18). Two largest tumors on the pre-TACE imaging were defined as the target lesions and other tumors were considered non-target lesions. CT was the routine follow-up imaging modality for the response evaluation and all of the measurements were made on a PACS workstation (Centricity, ver. 3.0; GE Healthcare, Barrington, IL, USA). Overall responses were assessed taking into consideration both target responses and non-target responses, as well as the appearance of new lesions and extrahepatic metastases. Target responses by RECIST criteria are based on the change of the sum of the diameter of the target lesions, which included not only the viable tumor but also the necrotic tumor portion with or without iodized oil uptake. In contrast, mRECIST takes into consideration only the viable (enhancing) tumor portion. Target response was considered complete response (CR) when the target lesions disappeared as a whole (RECIST) or when the viable tumor portion disappeared (mRECIST). Partial response (PR) was defined as 30% decrease from the baseline. Progressive disease (PD) was defined as a 20% increase from the smallest sum of the diameter of target lesions (Fig. 1). Stable disease (SD) was defined as that between PR and PD. Responses were evaluated three times in each patient, approximately 1, 3, and 6 months after the initial TACE. The patients showing overall responses of CR or PR were classified as responders and the others were classified as non-responders.
A 56-year-old man with HCC who received a single session of iodized oil transarterial chemoembolization (TACE). (a, b) Arterial phase (a) and delayed phase (b) contrast-enhanced CT images show 3.5-cm-diameter tumor (arrows) in right hepatic lobe. (c) Arterial phase CT scan obtained at 3-month follow-up after TACE shows dense uptake of iodized oil within the tumor and no residual tumor enhancement, which was assessed as complete response by mRECIST and stable disease by RECIST (target response). (d) Arterial phase CT scan obtained 6 months after TACE shows wash-out of iodized oil at inferior portion of the tumor and local recurrence in the area (arrows), which was assessed as progressive disease by mRECIST. However, the response by RECIST still meets stable disease. RECIST, Response Evaluation Criteria in Solid Tumors; mRECIST, modified RECIST.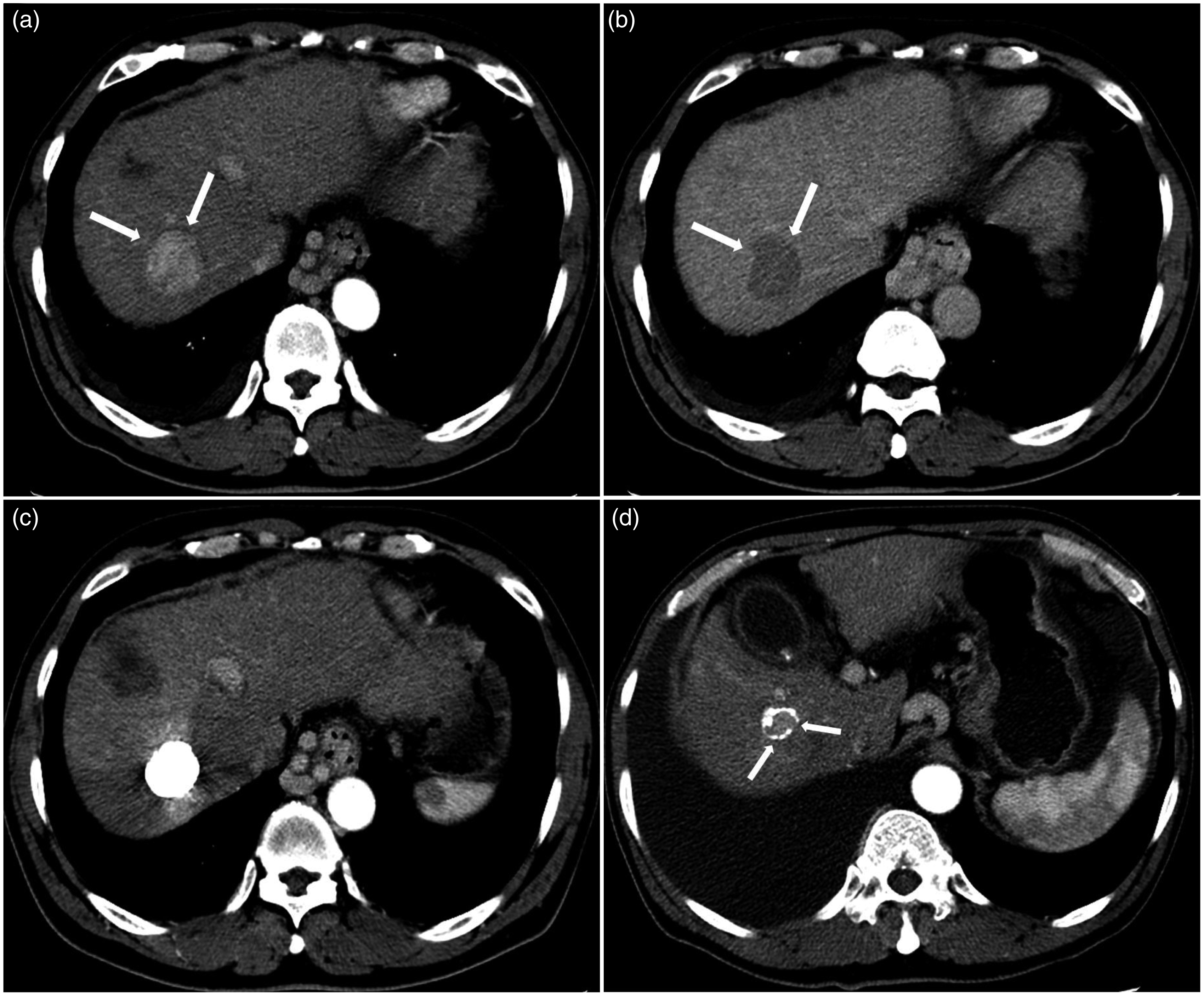
Statistical analysis
Coincidence rates between RECIST and mRECIST were assessed at each time point using the κ coefficient. A κ coefficient over 0.80 represented excellent inter-method agreement, 0.61–0.80 as good, 0.41–0.60 as moderate, 0.21–0.40 as fair, and κ coefficient less than 0.21 represented poor inter-method agreement (19). Overall survival was defined as the time from the date of the first TACE to the date of death. Survival time was censored at the date of the last follow up or at therapy change to surgical resection (n = 4), transplantation (n = 3), or radiofrequency ablation (n = 13). The Kaplan-Meier method with log-rank test was used to calculate and compare survival curves between responders and non-responders. Univariate and multivariate analyses were conducted to assess factors associated with survival using the Cox proportional hazard model, addressing whether survival was different according to response status, demographic factors such as age, sex and etiology, and tumor factors such as tumor size, number, and level of alpha-fetoprotein (AFP). Multivariate analyses were performed using six models based on each response criteria and hazard ratio (HR) estimates were based on simultaneous analysis of all variables. To determine the predicting power of each response criteria, time-dependent area under the receiver operating characteristic curve (AUC) and C-statistics were measured (20,21). SAS software version 9.3 (SAS Institute, Cary, NC, USA) and R2.15.1 (Vienna, Austria; http://www.R-project.org/, Package=‘survAUC’) were used for statistical analyses.
Results
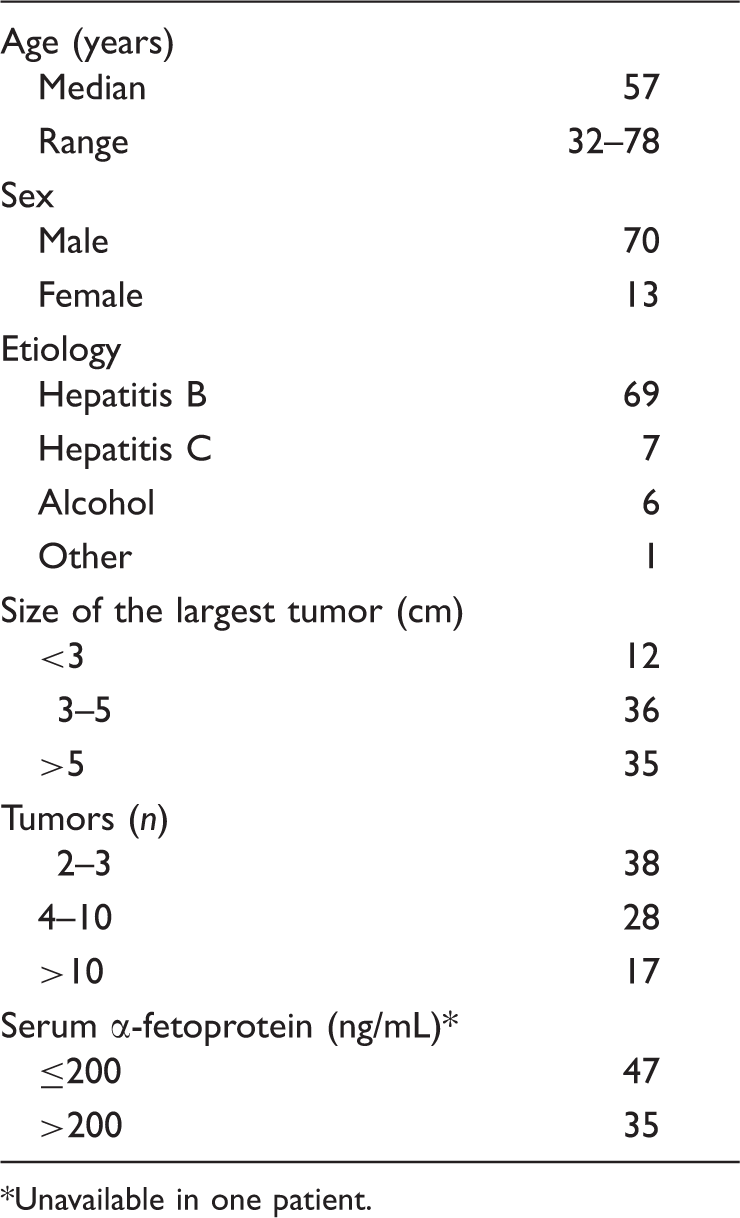
After TACE, mRECIST was difficult to apply in 15 patients because TACE caused mixed areas of viable and necrotic tumor portions consisting of diffuse patchy iodized oil uptake throughout the tumor, which prevented adding up of diameters of tumor parts showing contrast enhancement (Fig. 2). Thus, the remaining 83 patients were included in the subsequent analyses. Their baseline characteristics are summarized in Table 1. During the period of response evaluation, each patient underwent a mean of three sessions of TACE (median, 3; range, 1–5). Four patient received one session of TACE (mean survival, 44 months), 25 patients received two sessions (mean survival, 50 months), 33 patients received three sessions (mean survival, 35 months), 18 patients received four sessions (mean survival, 39 months), and three patients received five sessions (mean survival, 18 months). The mean intervals between the initial TACE and the 1-month, 3-month and 6-month response evaluation were 26 days (median, 26 days; range, 11–47 days), 84 days (median, 81 days; range, 67–137 days), and 172 days (median, 172 days; range, 142–229), respectively.
A 69-year-old man with HCC who received repeated sessions of iodized oil transarterial chemoembolization (TACE). (a) Arterial phase CT scan shows 14.5 cm-diameter hepatocellular carcinoma involving hepatic dome area (arrows). (b) Arterial phase CT scan obtained 1 month after the first TACE shows mixed areas of enhancing tumor portions with patchy uptake of iodized oil, which prevents mRECIST evaluation. (c) Arterial phase CT scan obtained 1 month after the third TACE shows that the tumor was shrunken. However, mRECIST evaluation still seems difficult to make. mRECIST, modified Response Evaluation Criteria in Solid Tumors. Patient demographics and tumor characteristics. Unavailable in one patient.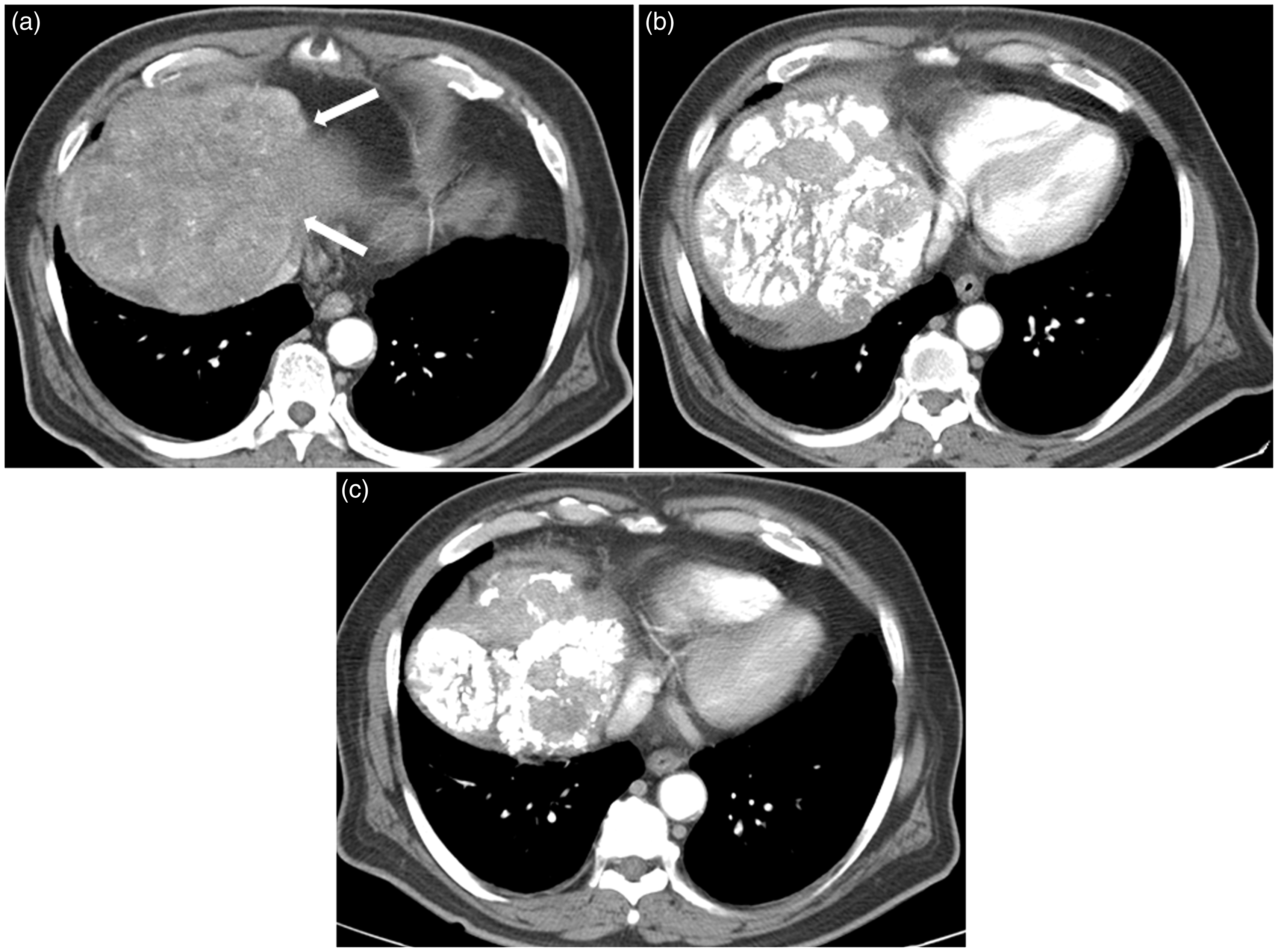
Responses at 1, 3, and 6 months according to RECIST and mRECIST.
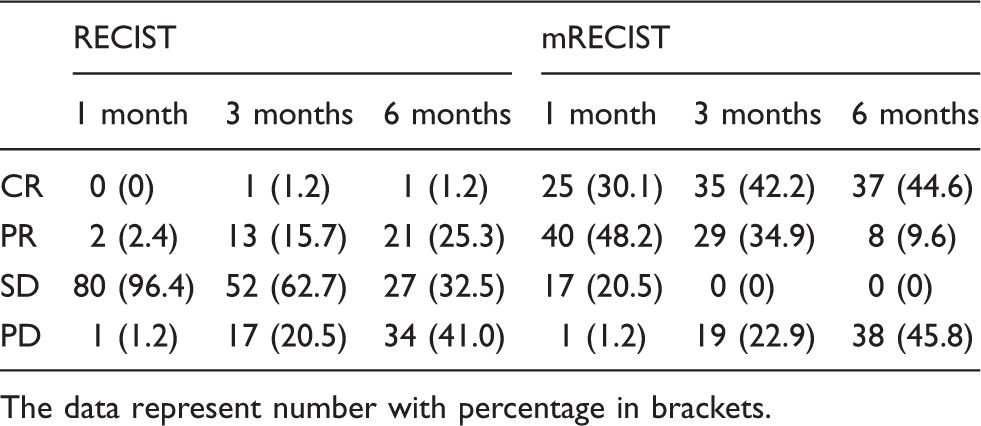
The data represent number with percentage in brackets.
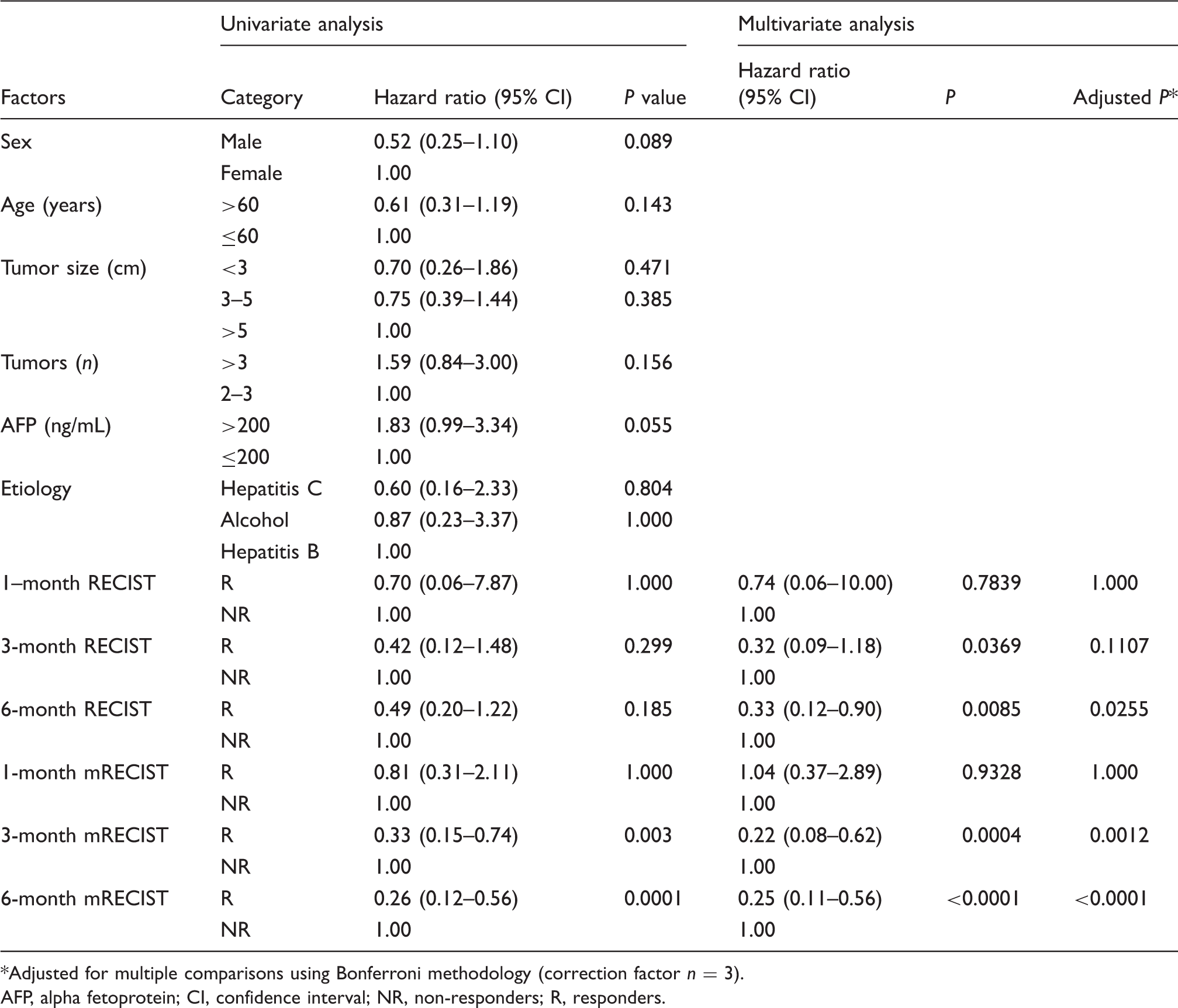
The estimated median survival of all patients was 39.2 months (95% CI, 24.6–53.8). In univariate analyses, there were significant differences in survival time between responders and non-responders by 3- and 6-month mRECIST (Table 3) (Fig. 3). No other factors were associated with survival. In multivariate analyses, responders by RECIST at 6 months (HR, 0.33; 95% CI, 0.12–0.90; P = 0.0255), and by mRECIST at 3 months (HR, 0.23; 95% CI, 0.08–0.62; P = 0.0012) and 6 months (HR, 0.25; 95% CI, 0.11–0.56; P = 0.0001) were independently associated with longer survival (Table 3).
Survival curves estimated by Kaplan-Meier analysis between responders and non-responders according to 1-, 3-, and 6-month RECIST (a, b, and c) and 1-, 3-, 6-month mRECIST (d, e, and f). Univariate survival analysis of intermediate stage HCC patients following TACE and multivariate survival analysis using six models based on each time point response. Adjusted for multiple comparisons using Bonferroni methodology (correction factor n = 3). AFP, alpha fetoprotein; CI, confidence interval; NR, non-responders; R, responders.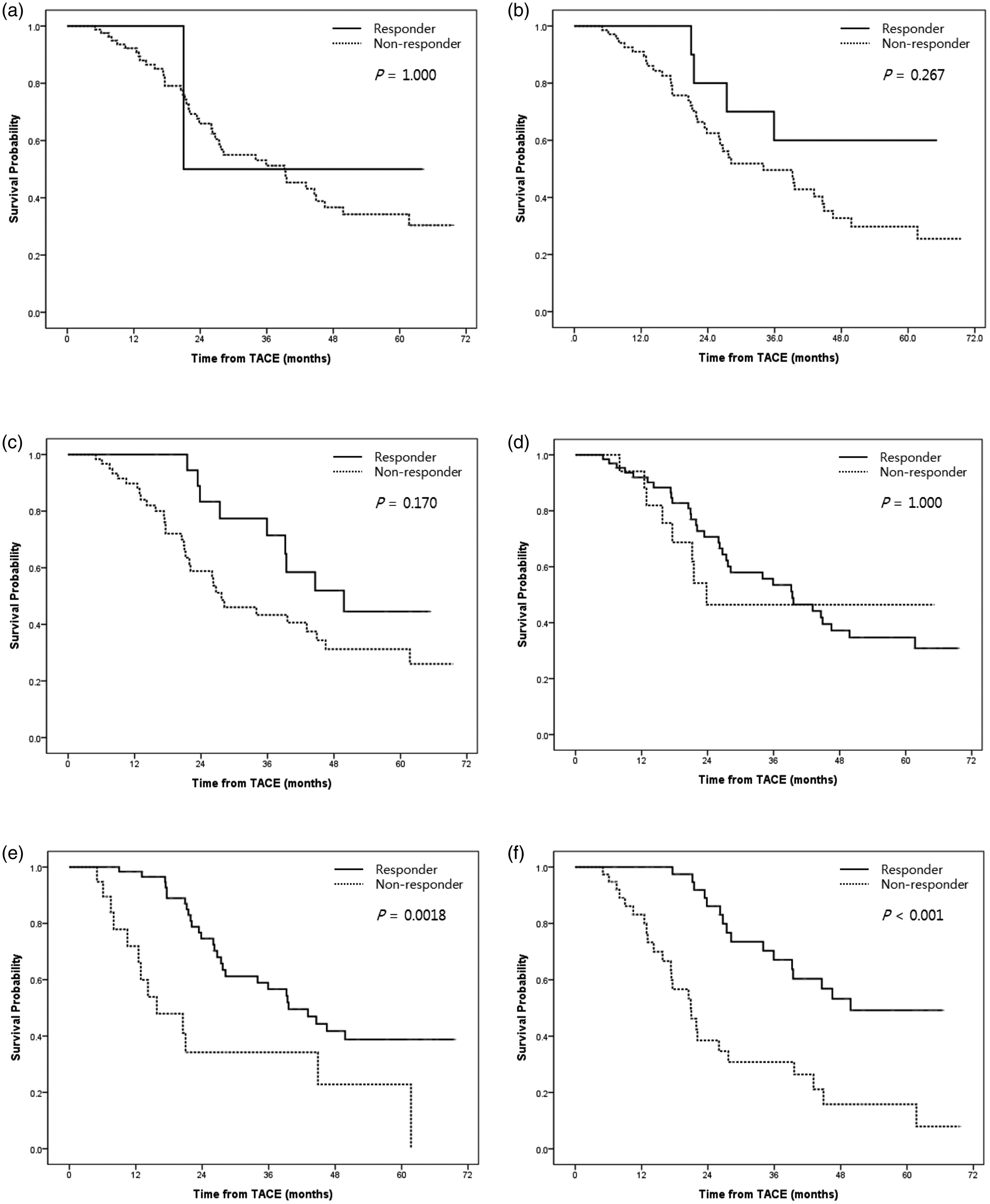
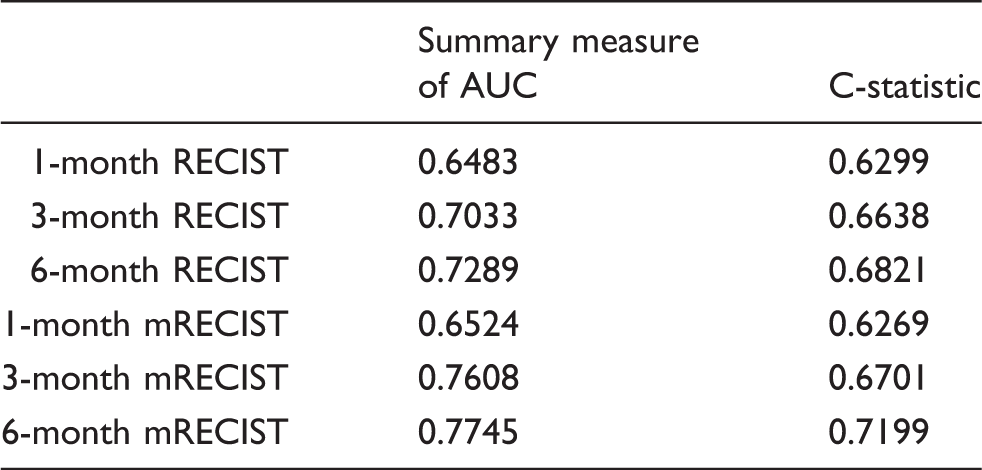
Survival predicting power analysis of each time point response.
Discussion
This study showed that mRECIST evaluated at median 26 days (range, 11–47 days) after TACE was not associated with survival. Previous studies showed that mRECIST and EASL responses assessed at an early time point of median 34 days (range, 0–113 days) and 64 days (range, 18–129 days) after initial TACE were associated with survival (8,11). Given the differences in method of study (e.g. all stage HCC vs. stage B alone HCC, drug-eluting bead TACE vs. iodized oil-based TACE), direct comparison with the previous studies may be pointless. However, our study showed a clear trend that the performance and predicting power of response assessment improved over time. Although the concept of an early single time point response reflecting long-term prognosis with accuracy is attractive, our study suggests that a too early decision may lead to underestimation of the effect of TACE and inappropriate therapy change.
With the advent of enhancement-based response criteria, the role of size-based criteria as a surrogate of survival has been undervalued (8–11,13). However, in an early landmark study by Llovet et al. (5), WHO response sustained for at least 6 months after TACE was associated with longer survival. Riaz et al. (12) also showed that WHO response after TACE or radioembolization were a prognostic factor and the median time to WHO or RECIST response was 7.7 months. The present results also suggest that tumor necrosis induced by transarterial therapy will ultimately result in the reduction of tumor size that is sufficient to meet CR or PR by size-based criteria, although the size-based response occur later compared with enhancement-based criteria.
mRECIST recommends that only well-delineated, arterially enhancing tumors should be selected as target tumors for accurate and repeat measurements (18). With this regard, mRECIST may be suitable in the setting of prospective clinical trials in which at least one well-delineated tumor can be included by trial design. However, the application of mRECIST may be difficult in the daily practice setting because a substantial portion of HCCs are infiltrative. And, patchy uptake of iodized oil, which is frequently noted after TACE may further prevent response evaluation. In our study, mRECIST assessment was impractical in about 15% (15/98) of the patients due to patchy uptake of iodized oil after TACE. MRI is known to have advantages over CT in depicting arterial enhancement after TACE using iodized oil and contrast-enhanced ultrasound may help to evaluate mRECIST (22,23). However, given that enhancement-based response criteria are inevitably based on the measurements and summation of enhancing parts of tumors and the enhancing parts of tumors, especially after TACE, may show erratic distribution in the tumor, we still believe that there will be limitations on the uniform application of enhancement-based criteria for the response evaluation after TACE of HCC. However, with repeated TACE, patchy uptake of iodized oil within the tumors may change and patients may get better evaluable over time.
In our study, most SDs by 3- and 6-month RECIST were responders when they were reclassified according to mRECIST. However, assessment with PD was almost identical with respect to both criteria because most PDs were unequivocally met by the appearance of new lesions after TACE, rather than by measurement-based progression, which is coincident with the result of a previous study (13). From this point of view, it can be argued that RECIST or mRECIST does not precisely reflect the treatment effect of TACE against target lesions because the appearance of new lesions will lead to the classification as “PD”. Prajapati et al. (11) reported that both target response and overall response had significant correlation with survival after TACE of HCC. However, Gillmore et al. (8) reported that there was no significant association between survival and target mRECIST response while overall mRECIST response was associated with survival. Other researchers also reported the association between survival and overall response (9,13). From these results, overall response may better predict the biologic behavior and aggressiveness of the tumor against certain treatments as a whole and with better accuracy than target response. Further studies are necessary to determine whether there are clear differences between overall response and target response as a prognosis predictor.
mRECIST tended to dichotomize into non-PD (CR, PR, and SD) and PD, and non-PD became equivalent to responders with the passage of time, as all SDs fell into either the responder (responding to repeated TACE) or PD (despite repeated TACE). In other words, tumor response to TACE tends to converge into PD or non-PD with time and both criteria may perform similarly in terms of differentiating PD vs. non-PD. We noted a trend toward a shorter survival with increasing sessions of TACE and this inverse relation will be the result that the more aggressive the tumors are, the poorer response the tumors will show despite repeated TACE.
Our study has limitations. First, it was based on the analysis of the results of iodized oil TACE. Radioembolization or TACE using drug eluting beads are gaining popularity and studies based on these newer therapies are warranted (24). Second, the statistical power is not strong due to the small sample size and inherent weakness in the retrospective design. The discrimination between CR and PR or between SD and PD seemed to be inappropriate due to the small sample size. Finally, we only included patients who were followed up for at least 6 months, which might introduce a bias as patients with poorer prognosis might have been excluded.
In conclusion, our study showed that radiologic tumor responses were significant prognostic factors after iodized oil TACE of HCC. mRECIST as early as 3 months after initial TACE could be used for the prognosis prediction. And in cases when mRECIST is not applicable, response to RECIST may be a prognostic factor 6 months after initial TACE.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.