
Abstract
Background
The indication of percutaneous catheter drainage (PCD) has expanded with the development of guiding modalities. Since serious complications still occur, efforts and new techniques have been continuously searched for safer PCD.
Purpose
To evaluate the feasibility and efficacy of primary tractography for establishing a safe needle pathway during PCD.
Material and Methods
A total of 42 patients (20 men, 22 women; mean age, 50.7 years) who underwent primary tractography during PCD were prospectively enrolled between April 2009 and August 2013. The locations of fluid collection included sub-phrenic (n = 8), between bowel loops (n = 21), pelvic cavity (n = 8), within solid organ (n = 2), and others (n = 3). The interposed anatomic structures were analyzed on the basis of primary tractography findings. Complications related to PCD or primary tractography were evaluated.
Results
Interposition of any significant anatomic structure was confirmed in 10 of 42 patients (23.8%). The entrapped anatomic structures were the omental vessel (n = 4), bowel (n = 2), pleura (n = 2), bile duct (n = 2), and a branch of the left inferior epigastric artery (n = 1). In one patient, both the pleura and bile duct were interposed simultaneously. The technical and clinical success rates of PCD were 97.6% and 97.6%, respectively. No complications related to PCD or primary tractography occurred during the follow-up period.
Conclusion
Primary tractography is a simple and feasible method to evaluate the entrapment of normal anatomic structure during PCD. This method may aid in preventing possible serious PCD-related complications, such as bleeding and fistula.
Introduction
Percutaneous catheter drainage (PCD) in the abdomen and pelvis was introduced in the late 1970s (1,2). Subsequently, PCD has become a mainstay in treatments for abscess, postoperative complicated fluid collection, and benign or malignant pleural effusion with the development of imaging modalities such as ultrasound and computed tomography (CT) (3–6). PCD is known as a safe method and has a low complication rate of 5–15% (5,7–10). However, as the indications for PCD have expanded, the complication rate has increased, involving serious complications such as bleeding (11).
Various types of technique have been developed to perform PCD in more challenging cases. In addition to conventional real-time ultrasonography, CT fluoroscopy, cone beam CT, and real-time MR guidance have recently been introduced (12–14). These new techniques are useful for determining both the safe pathway and the final location of the access needle. However, once the needle has passed through, the evaluation of the entrapped anatomic structures is limited. Accordingly, there is the possibility of the unexpected passage of the puncture needle through small vessels, pleural reflection, and sometimes bowel. When the drainage catheter is placed through those structures, complication such as hemorrhage, pneumothorax, and enterocutaneous fistula can occur.
Tractography has been performed to confirm access tract maturation after percutaneous transhepatic biliary drainage (PTBD) and percutaneous transhepatic gallbladder drainage (PTGBD) (15,16). Tractography of PTBD or PTGBD has the advantage of real-time evaluation of tract maturation, which can be applied to evaluate needle tract safety in risky and challenging PCD cases. However, there are no published reports regarding the feasibility and usefulness of tractography during PCD.
The purpose of this study was to evaluate the feasibility and efficacy of primary tractography in the assessment of the needle pathway during PCD.
Material and Methods
A total of 42 patients who underwent primary tractography during PCD were prospectively enrolled between April 2009 and August 2013 at a single tertiary institution. Twenty men and 22 women were included (age range, 23–76 years; mean age, 50.7 years). Written consents were obtained from all the patients or legally responsible family members. The local institutional review board approved the review of medical and image data for this study.
Summary of lesion characteristics and the results of primary tractography.
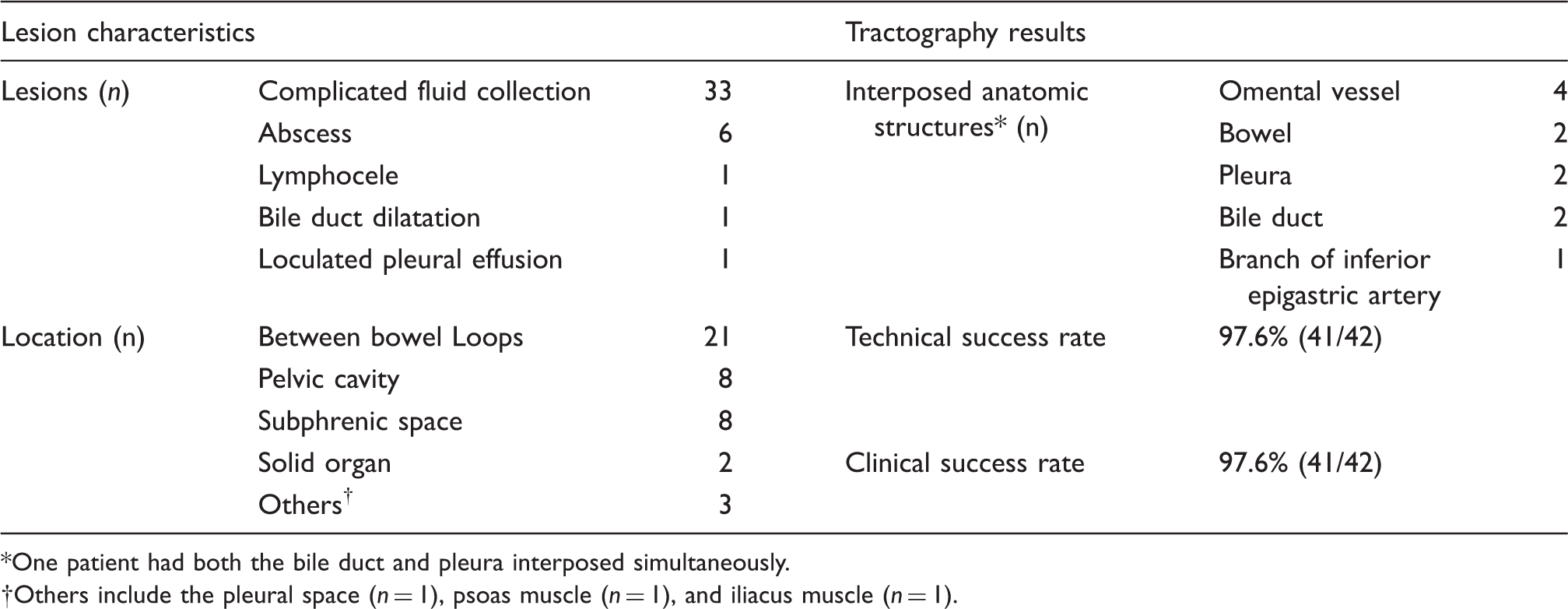
One patient had both the bile duct and pleura interposed simultaneously.
Others include the pleural space (n = 1), psoas muscle (n = 1), and iliacus muscle (n = 1).
Potential needle access tracts and skin puncture windows were evaluated on axial-, coronal-, and sagittal-reformatted CT images. The indication for primary tractography was only a single available access route for the fluid collection with less than a 1 cm in width skin access window as well as a high risk of penetrating vessels, solid organs, bowels, and pleural reflection along the path of the imaginary needle tract on CT images. After PCD, the number of needle passages until achieving a safe puncture route was recorded. The clinical importance of the anatomic structure that was entrapped in the needle tract was also recorded.
In contrast with conventional tractography, primary tractography was performed just after needle access to the target lesion was achieved. In all cases, needle access was performed with a 22-G Chiba needle (Cook Incorporated, Bloomington, IN, USA) guided by ultrasound (n = 30, 71.4%), ultrasound and fluoroscopy (n = 7, 16.7%), ultrasound and cone beam CT (n = 3, 7.1%), and fluoroscopy and cone beam CT (n = 2, 4.8%). Once the needle tip was in the target fluid collection, the stylet was removed, and a 0.018-inch wire that was 65 cm in length (hair wire, A&A Medical Device Company, Seongnam, Republic of Korea) was advanced into the target lesion through a Chiba needle. Then, the Chiba needle was withdrawn, leaving only the hair wire. A 30 cm 5-Fr catheter (Yellow Sheath, A&A Medical Device Company, Seongnam, Republic of Korea) was introduced along the hair wire. The stylet of the catheter was removed leaving the catheter and hair wire in place. The end arm of a Y-shaped connector was connected to the catheter over the hair wire. Then, a 10-mL locking syringe filled with contrast material was attached to the side arm of the connector (Fig. 1). While injecting contrast material with one hand, only the catheter (Yellow Sheath) was withdrawn from the target lesion to the puncture site on the skin with the hair wire fixed in the fluid cavity (Supplementary video). A fluoroscopic capture function was useful for recording the contrast material injection along the needle tract. Images were reviewed carefully to determine the entrapment of anatomic structures along the needle pathway. If no significant structures were observed on the primary tractogram, the procedure proceeded further in the standard PCD manner. However, in the case of penetration of any anatomic structure, a new access route was attempted until complete clearance of the needle pathway was confirmed.
The system for primary tractography. A yellow sheath (arrow) is placed with the tip in the target lesion along the 0.018-inch hair wire (arrow heads). After removal of the stylet (S), a Y-connector (curved arrow) is attached to the hub of a yellow sheath along the hair wire. A 10-mL locking syringe filled with contrast medium is connected to the side arm of the Y-connector.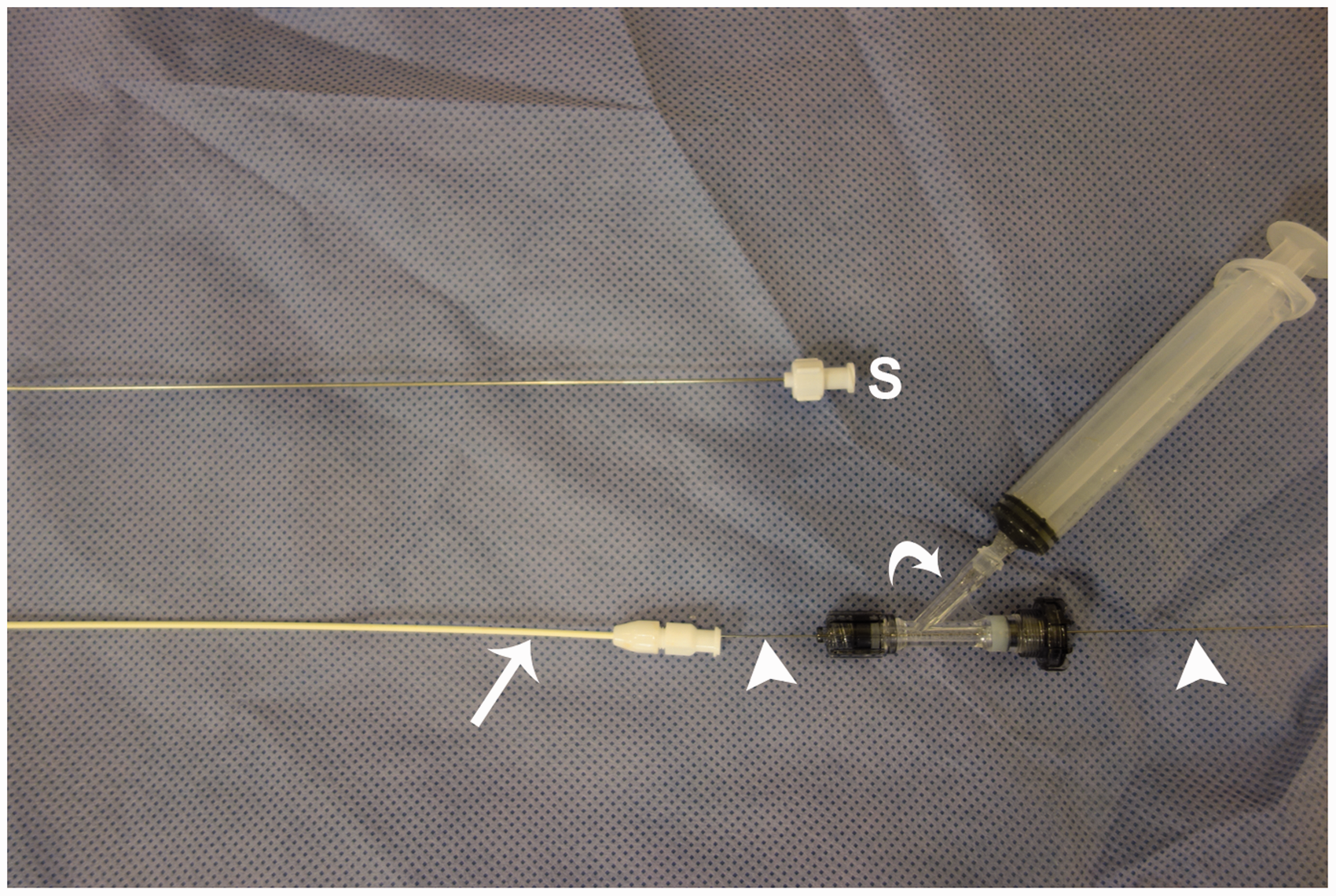
Technical success was defined as safe placement of the drainage catheter in the target fluid collection without entrapment of significant anatomic structures, including vessels, bowel, and solid organs. Clinical success was defined as successful removal of the PCD tube without procedure-related complications after the resolution of the target fluid collection. Removal of the PCD tube was based on the following criteria: less than a 10 mL amount of daily drainage, clear drainage, disappearance of clinical symptoms, and normalization of laboratory data.
The follow-up period was defined as the time period between the date of PCD and the date of the final hospital visit. The follow-up period was in the range of 1–1562 days (median, 136 days). Follow-up CT (n = 31, 86.1%), magnetic resonance imaging (n = 2, 5.6%) or ultrasound (n = 3, 8.3%) taken at least 1 month after PCD was available in 36 out of 42 patients and analyzed for both resolution of lesions and possible complications related to PCD.
Results
Table 1 summarizes the characteristics of the target lesions and the results of primary tractography.
The technical success rate of PCD was 97.6% (41/42). Penetration of any significant anatomic structure during the first PCD attempt was confirmed in 10 of 42 patients (23.8%). The entrapped anatomic structures in 10 patients were the omental vessel (n = 4), bowel (n = 2), pleura (n = 2), bile duct (n = 2), and a branch of the left inferior epigastric artery (n = 1) (Fig. 2). In one patient, both the pleura and bile duct were entrapped in the needle pathway simultaneously. During the second attempt safe PCD was performed in nine of 10 patients (90%). The remaining patient suffered postoperative complicated fluid collection around the pancreas head, which was surrounded by the omentum and stomach. Several additional PCD and primary tractography attempts failed to obtain a safe needle pathway because of omental vein interposition. Only needle aspiration was performed in this patient. The clinical success rate of PCD was 97.6% (41/42). One patient experienced recurrence of postoperative complicated fluid collection due to early removal of a drainage catheter, which improved spontaneously during the follow-up period.
Various entrapped structures detected during primary tractography. (a) Omental vein (white arrow); (b) bowel (white arrow); (c) both pleural space (white arrow head) and bile duct (white arrow); (d) a small branch of the left inferior epigastic artery (white arrow).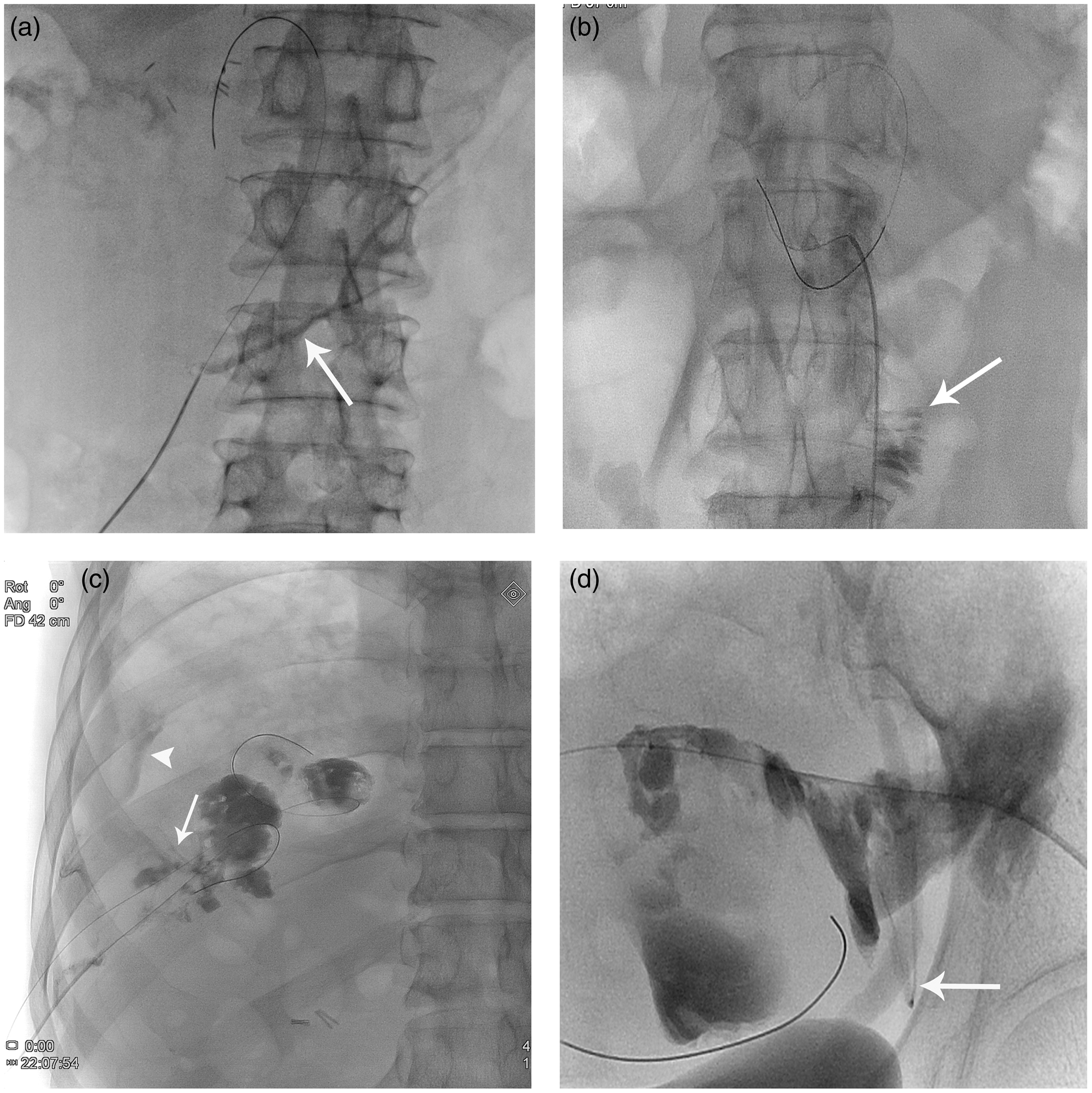
No complications directly associated with primary tractography or subsequent PCD were reported during the follow-up period up to 1562 days. The patients with entrapment of the bowel, pleura, or bile duct during primary tractography experienced no complications. The patients who had vessel penetration confirmed by primary tractography did not develop further serious complications. Two patients (2/42, 4.8%) had complications that were not related to primary tractography or PCD. One patient with Crohn’s disease underwent bowel resection because post-PCD follow-up fistulography revealed a fistula between the abscess cavity and colon. In the other patient a bronchobiliary fistula developed after a successful PCD for liver abscess due to transarterial chemoembolization of hepatocellular carcinoma.
During the follow-up period, one patient with liver abscess died from multiorgan failure not associated with the PCD procedure. On the review of follow-up images, two patients had asymptomatic residual fluid collections. However, no further invasive drainage procedures were required.
Discussion
PCD is a mainstay of treatment for any abnormal fluid collection from infection, inflammation, or operation since its introduction in 1977 (2). Compared with surgical drainage, PCD has a lower mortality and morbidity rate (17,18) as well as shorter hospital stay. However, with the advancement of complicated surgery and invasive procedures, cases requiring challenging PCD have increased. As a result, some studies have reported that the complication rate of PCD has increased (11).
Among these complications, GI perforation, hematoma, active bleeding, pneumothorax, and hemothorax are associated with inappropriate needle tract and targeting failure. In challenging cases, even when the needle tip has been successfully introduced into the target fluid collection, the needle tract may have passed through intervening significant anatomical structures. PCD-related bleeding can be caused by direct vessel penetration, late vessel erosion, and parenchymal injury (10). Bleeding from parenchymal injury is typically self-limited. While bleeding from late vessel erosion cannot be prevented and anticipated, bleeding from direct penetration of vessel in the middle of the needle tract should be avoided.
Primary tractography is useful for the evaluation of the whole needle pathway into the target fluid collection. In our analysis almost one patient out of four with carefully performed initial PCD had penetration of normal anatomic structures along the needle tract. Although the operator could achieve successful needle tip access into the target fluid, neglect of the entrapped normal anatomic structures was often the case. We had five cases of vessel penetration in the needle tract primary tractography, but there was no postprocedural bleeding because the first needle tract was abandoned, and the PCD tube was immediately placed along the other safe puncture tract. There were two patients with small bowel penetration on the first needle passage attempt, but we removed the guide wire and tractography catheter immediately after recognition of bowel penetration, which resulted in no postprocedural complications. A previous study reported that traversing the bile duct can be problematic as fistula between the tract and bile duct can persist (7). However, persistent biliary fistula can also occur in cases where the PCD tube is placed without notice of the bile duct penetration. Therefore, as observed in this study, when the needle and small-bore catheter (4F or 5F) for tractography are removed immediately after recognition of normal structure entrapment, subsequent complications are infrequent and can be prevented.
An additional advantage of primary tractography is fluid content aspiration when any other attempts fail to achieve a safe PCD placement. A 22-G puncture needle is insufficient for thick, viscous content aspiration, and a new puncture with large-bore needle for sample aspiration can be avoided. The prevention of further complications through primary tractography is cheaper than when hemorrhage and fistula formation occurs, and secondary management is followed.
The limitation of primary tractography is that a 5-Fr size catheter might be needed in the entrapped structures to evaluate the needle tract. Another limitation is the absence of a control group. Accordingly, our results may overestimate the need for primary tractography. However, the aim of this study was to assess the feasibility of a new method for safe PCD and not to emphasize the clinical importance of primary tractography.
In conclusion, primary tractography is a simple and feasible method to evaluate the entrapment or penetration of normal anatomic structure during PCD. This technique may be helpful for preventing possible serious PCD-related complications, such as bleeding and fistula.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.