
Abstract
Background
In preoperative lipiodol marking for small pulmonary nodules, lipiodol has a potential risk of distribution in the surrounding lung structure. There are no reports about the detailed accumulation and distribution of lipiodol.
Purpose
To evaluate computed tomography (CT) findings after lipiodol marking before thoracoscopic surgery for pulmonary nodules.
Material and Methods
Sixty-four consecutive CT-guided lipiodol markings for 103 nodules were performed in 55 patients. Lipiodol (0.2–0.4 mL) was injected using a 21-gauge needle near the nodule. The appearance of lipiodol spots was classified into the following three types on CT: type 1, dense; type 2, punctate; and type 3, unclear. The distribution of lipiodol was also investigated. Statistical analyses were performed on the accumulation and distribution related to nodule factors. Incidences of complications were also investigated.
Results
A total of 110 markings were performed because of seven additional procedures due to insufficient marking. All nodules were successfully resected on the same day. The appearances of the lipiodol spots were type 1 (82%), type 2 (11%), and type 3 (7.3%). The areas of distribution were lung parenchyma (54%), central bronchus (39%), peripheral bronchovascular bundle (24%), needle tract (20%), pleural space (19%), another segment of ipsilateral lung (5.5%), and contralateral lung (0.9%). Distribution into pleural space and central bronchus was frequently seen in the shallow nodules (P < 0.05). Complications were pneumothorax (61%) and pulmonary hemorrhage (35%). There were no serious symptoms.
Conclusion
The appearance of the lipiodol spot was dense in most cases, despite frequent distribution in the surrounding lung structures without serious complications.
Keywords
Introduction
Small pulmonary nodules can be resected by video-assisted thoracoscopic surgery (VATS). Preoperative marking is necessary to localize small nodules for detection during surgery. As markers, various materials have been used, such as dye (1), microcoils (2), hook wires (3), barium (4), and lipiodol (5–10). In the case of dye marking, the dye immediately diffuses into the surrounding lung tissue, so marking has to be performed within 3 h before surgery. In addition, the injection site can be unclear because of dye diffusion. Metal marking leads to the destruction of structures and complicates the histopathological diagnosis. In addition, when a hook-wire method is used, massive air embolism has been reported (11,12). Barium marking by computed tomography (CT) bronchoscopy is complex because of simultaneous use of bronchoscopy and CT. In addition, barium can induce inflammatory changes in lung tissue, making histological diagnosis difficult.
Lipiodol is a lipid-soluble contrast material. It is used for lymphangiography, for example (13), hysterosalpingography (14), and transcatheter arterial chemoembolization (TACE) of hepatocellular carcinoma (15). In marking with lipiodol, the lipiodol can be injected correctly under CT guidance adjacent to the small nodule. Lipiodol remains in place for several days, so it is easy to localize the nodule by X-ray fluoroscopy during surgery. In addition, lipiodol induces less inflammatory changes than other materials, thus reducing possible sources of error when evaluating the histological diagnosis (16). Previous reports have advocated the use of lipiodol marking (5,8,10,17). However, there is the possibility of lipiodol migration into vessels, causing systemic infarction. In this study, we evaluated the details of CT findings of the local accumulation of lipiodol spot and the distribution of lipiodol in surrounding lung structures after preoperative marking of small lung nodules.
Material and Methods
Patients
The characteristics of the 103 nodules.
Mean ± standard deviation.
Candidates for lipiodol marking were selected by consensus between interventional radiologists and chest surgeons at a case presentation conference. All procedures were performed with the patients providing written informed consent. This retrospective study was approved by the institutional review board.
Lipiodol marking
All lipiodol marking procedures were percutaneously performed by one of five interventional radiologists, who were experienced in CT-guided procedures in our institute. Local anesthesia was administered by subcutaneous injection of 1% lidocaine. A 21-gauge needle (PEIT needle; Hakko Medical, Chikuma, Nagano, Japan), the inner lumen of which had been filled with lipiodol beforehand, was advanced into the area adjacent to the nodule under CT fluoroscopic guidance (Vigor Laudator, Toshiba Medical System, Tokyo, Japan) (5). According to the location of the nodule, the marking point had been decided at a conference between the surgeons and the radiologists before the procedure. Details of the CT fluoroscopy are described elsewhere (18). The imaging parameters during CT fluoroscopy included a CT beam width collimated to 3 mm, a peak tube voltage of 120 kVp, a current of 30 mA, and a scanning speed of 0.75 s per rotation of 360 degrees. An I-I device (Hakko Medical, Chikuma, Nagano, Japan) was used, which assisted needle advancement without direct irradiation to the physician's hand under CT fluoroscopy in order to reduce irradiation of the operator (19).
After confirmation that the needle tip had advanced to the location to be marked, lipiodol (Laboratoire Guerbet, Roissy, France) was manually injected (range, 0.2–0.4 mL) under CT fluoroscopy to make a lipiodol spot. After sufficient lipiodol accumulation had been confirmed by brief fluoroscopy, the needle was withdrawn. Immediately after the lipiodol marking, whole-chest CT images were obtained using helical CT scanning to evaluate the accumulation of lipiodol and adverse events such as pneumothorax or pulmonary hemorrhage. The beam width was 5 mm, table-feeding speed 7 mm/s, and image reconstruction was performed with a width of 5 mm. Technical success was defined by sufficient lipiodol spots being obtained at a distance of within 10 mm from the nodule. When lipiodol spots were not obtained sufficiently or were far from the nodule, additional marking was performed by the same method.
When pneumothorax occurred, the area of pneumothorax on a CT scan image was visually estimated. In patients in whom the ratio of pneumothorax to the pleural space was greater than approximately 20%, manual aspiration was immediately performed (20). If the pneumothorax did not decrease, an 8-F chest tube (Trocar catheter; Nippon Sherwood, Tokyo, Japan) was placed in the pleural space of the existing pneumothorax. When pneumothorax occurred during the procedure, especially in the marking of multiple nodules in one session, a chest tube was inserted for continuous pleural air suction, to obtain lung re-expansion, providing easier access to the nodules with continuation of the procedure.
A chest radiograph was obtained just after the procedure to confirm the accumulation of lipiodol. All patients were transferred to the operating room and VATS was performed on the same day.
VATS
VATS was performed under general anesthesia. The location of the nodule could be detected using a C-arm-shaped fluoroscopic unit as radiopaque spots in multiple projections. After confirmation of the positional relationship between the lipiodol spot and the nodule using the CT images obtained at lipiodol marking, the nodules were grasped with ring-shaped forceps and resected, including the radiopaque spots. Subsequently, whether radiopaque spots were present in the resected specimens was examined under C-arm fluoroscopy for precise confirmation of the success of resection.
Investigated parameters
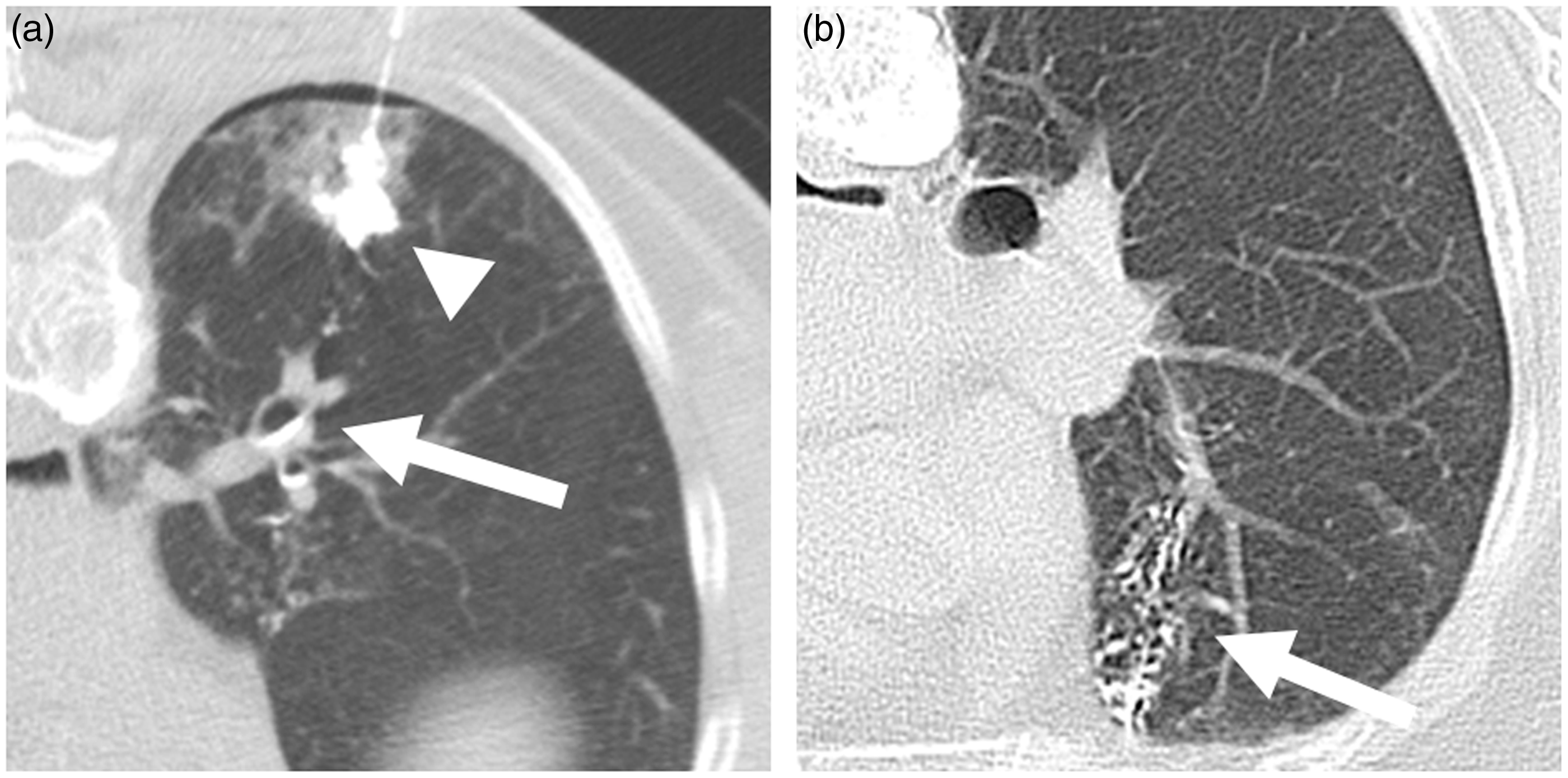
We retrospectively investigated the appearance of the lipiodol spot and the location of the distribution of lipiodol in the surrounding lung structures on CT. The appearance of the lipiodol spot was classified into the following three patterns. Type 1 was when dense accumulation was obtained, which means that lipiodol filled the alveolar space and there was no air density in the lipiodol spot on CT images (Fig. 1a). The shape of the lipiodol spot was circular or oval, and its minor axis was greater than 5 mm. Type 2 was when a lipiodol spot was obtained, but it consisted of a collectivity of multiple small punctate dense spots that had a sponge-like appearance, including air density within the lipiodol spot (Fig. 1b). The minor axis of each dense accumulation was less than 5 mm. Type 3 was when local accumulation of lipiodol was poor because of diffusion in the surrounding lung structures, and a lipiodol spot was not obtained. The distribution of the injected lipiodol was as follows: lung parenchyma, central bronchus, bronchovascular bundle, needle tract, pleural space, and migration to another segment. We also investigated the incidence of adverse events such as pneumothorax, pulmonary hemorrhage around each needle tract, and systemic embolization.
Patterns of appearance of the lipiodol spot on CT. (a) Appearance of the lipiodol spot was classified as type 1. The shape of lipiodol accumulation was round and air density of alveolar space was occupied by dense accumulation (arrow). (b) Appearance of the lipiodol spot was classified as type 2. Lipiodol spot was obtained; however, it consisted of a collectivity of multiple small punctate dense spots with a sponge-like appearance including air density within it (arrow).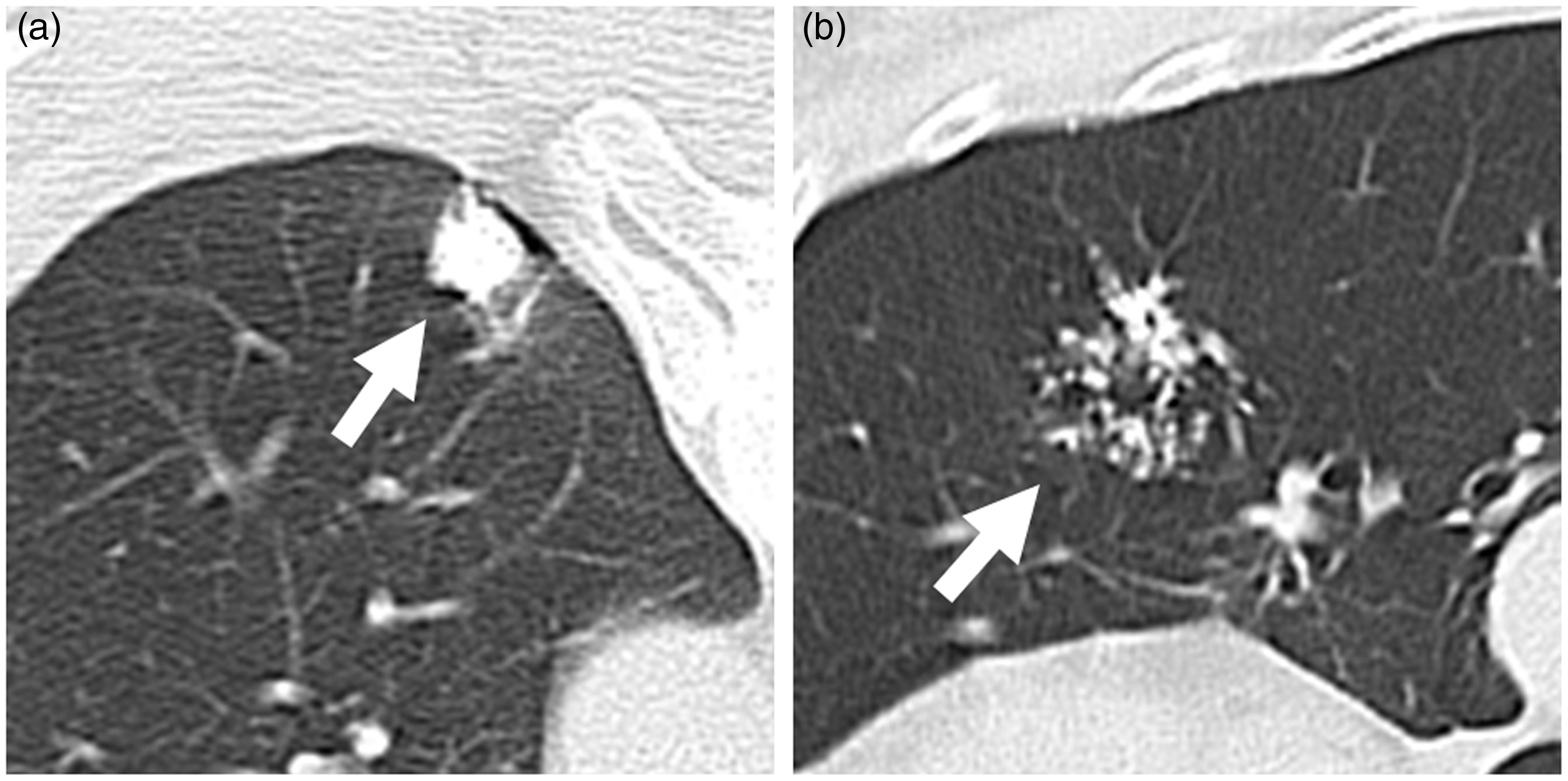
Statistical analysis
Statistical analyses were performed using JMP 9.0 (SAS, Carey, NC, USA). The accumulation and distribution of lipiodol with regard to the nodule factors (size, distance from the pleura, and presence of emphysema around the nodule) on all punctures were analyzed for statistical significance using Fisher's test, Wilcoxon's test, and the Kruskal-Wallis test. Values shown in the text and tables are means ± standard deviations. A P value < 0.05 was defined as statistically significant.
Results
A total of 110 punctures were performed for 103 nodules in 64 sessions. The number of target nodules in one session was one in 38 sessions, two in 16 sessions, three in seven sessions, and four in three sessions. For seven nodules, a second marking was added because unclear accumulation (n = 6) and mislocation of the lipiodol spot far from the nodule (n = 1) were seen after the first marking. All nodules were finally localized and resected by VATS.
The characteristics of accumulation and distribution in the 110 punctures.
Mean ± standard deviation.
Causes of unclear accumulation were injection into the central bronchus in four, spread to the pleural space in three, and location far from the nodules in one.
Patterns of accumulation in the bronchus were congestion in three and segment in 40.
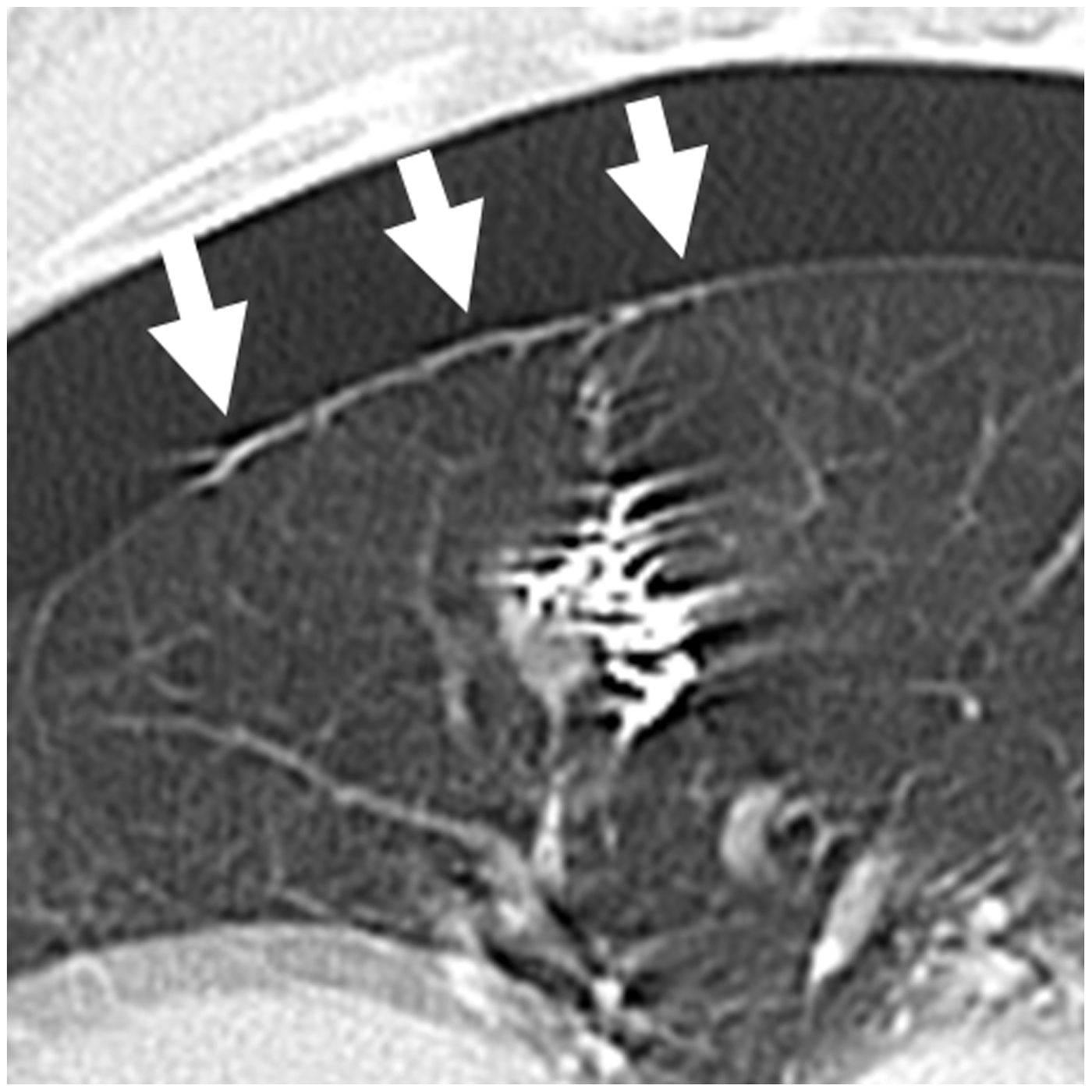
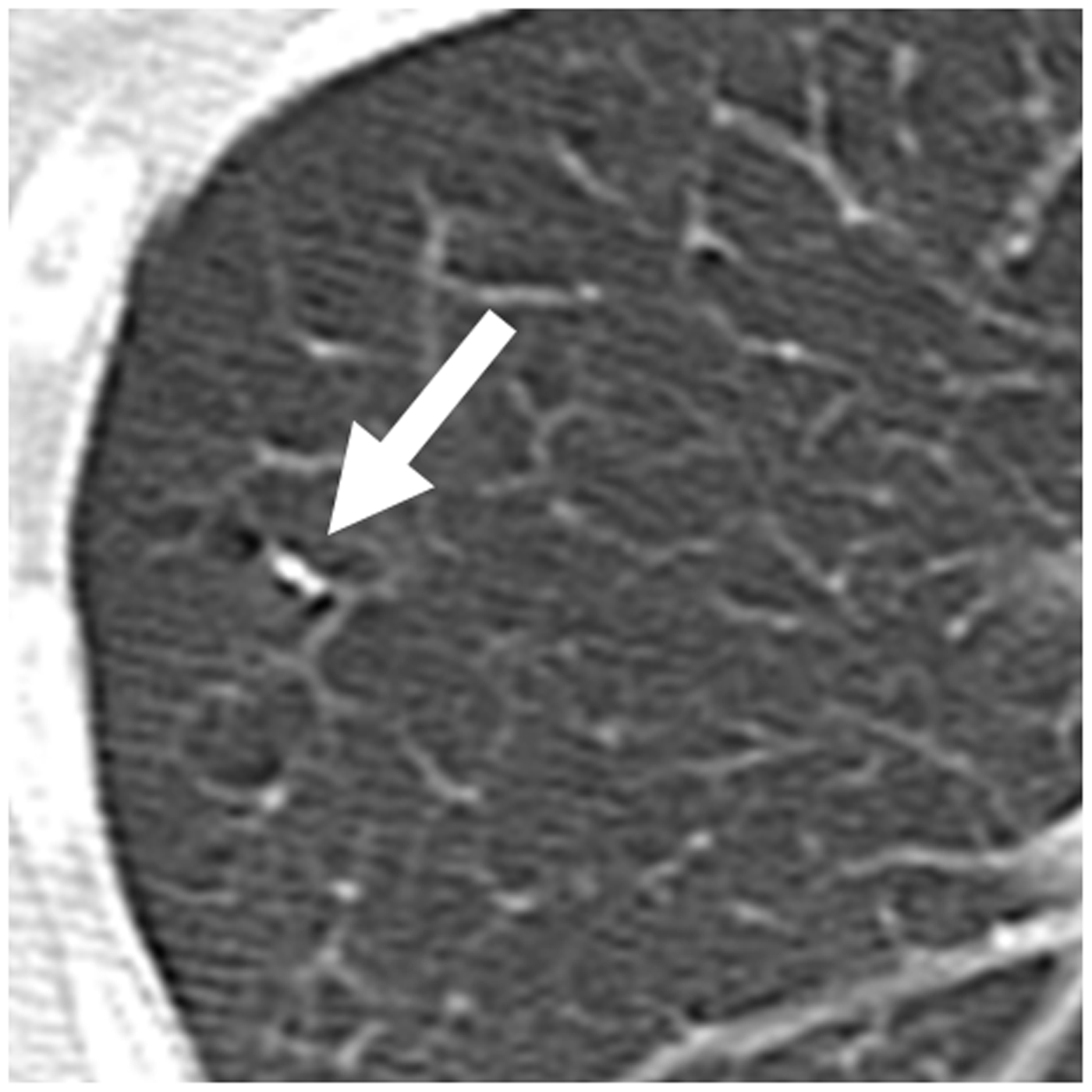
The lipiodol spots were obtained without distribution in the surrounding lung structures in 16 markings (15%). In the remaining 94 markings, there was distribution in the surrounding lung structures. The number of distributed structures on each marking was a single location in 45 (41%) and multiple locations in 49 (45%). Locations of distributed lipiodol were lung parenchyma in 59 (54%), central bronchus in 43 (39%), peripheral bronchovascular bundle in 26 (24%), pleural space in 21 (19%), and needle tract in 22 (20%). Patterns of accumulation in the central bronchus were segmental in 40 (Fig. 2a) and congestion in three (Fig. 2b). Migration to another segment of the ipsilateral lung was shown in 6 (5.5%), and migration to the contralateral lung, which was caused by movement of lipiodol through the trachea, was shown in one case (0.9%). Migrated lipiodol remained for up to 1 month after surgery; however, no symptoms were experienced by any patient and the migrated lipiodol disappeared spontaneously (Fig. 3). When lipiodol was distributed in the pleural space, it was spilled through the needle puncture point and spread along the visceral pleural membrane (Fig. 4). With regard to the distribution of the peripheral bronchovascular bundle, it was not clear whether lipiodol was injected into the bronchus or the pulmonary artery in this study (Fig. 5). However, there were no symptoms suggestive of pulmonary embolization.
Distribution into the central bronchus. (a) Distribution into the central bronchus was shown (arrow). In most cases, migrated lipiodol was detected as a dot-like shape in the central bronchus. (b) Lipiodol filled the central bronchus (arrow) and a lipiodol spot was not obtained, which was classified as type 3 accumulation of lipiodol. Migration of lipiodol to another segment of ipsilateral lung. (a) Lipiodol marking was performed in the nodule at the right lower lung. The lipiodol spot obtained was classified into type 1 (arrowhead); however, lipiodol was distributed in the central bronchus during the injection (arrow). (b) After marking, lipidol migrated into the right middle lobe (arrow). The migrated lipiodol remained until 1 month after the procedure; however, it spontaneously disappeared without any symptoms. Distribution of lipiodol into the pleural space was shown (arrow). Lipiodol had spread into the pleural space through the needle track. Distribution of lipiodol into the peripheral bronchovascular bundle was shown (arrow). It was unclear whether the bronchus or the pulmonary artery was involved. Note that no serious symptoms occurred in this case.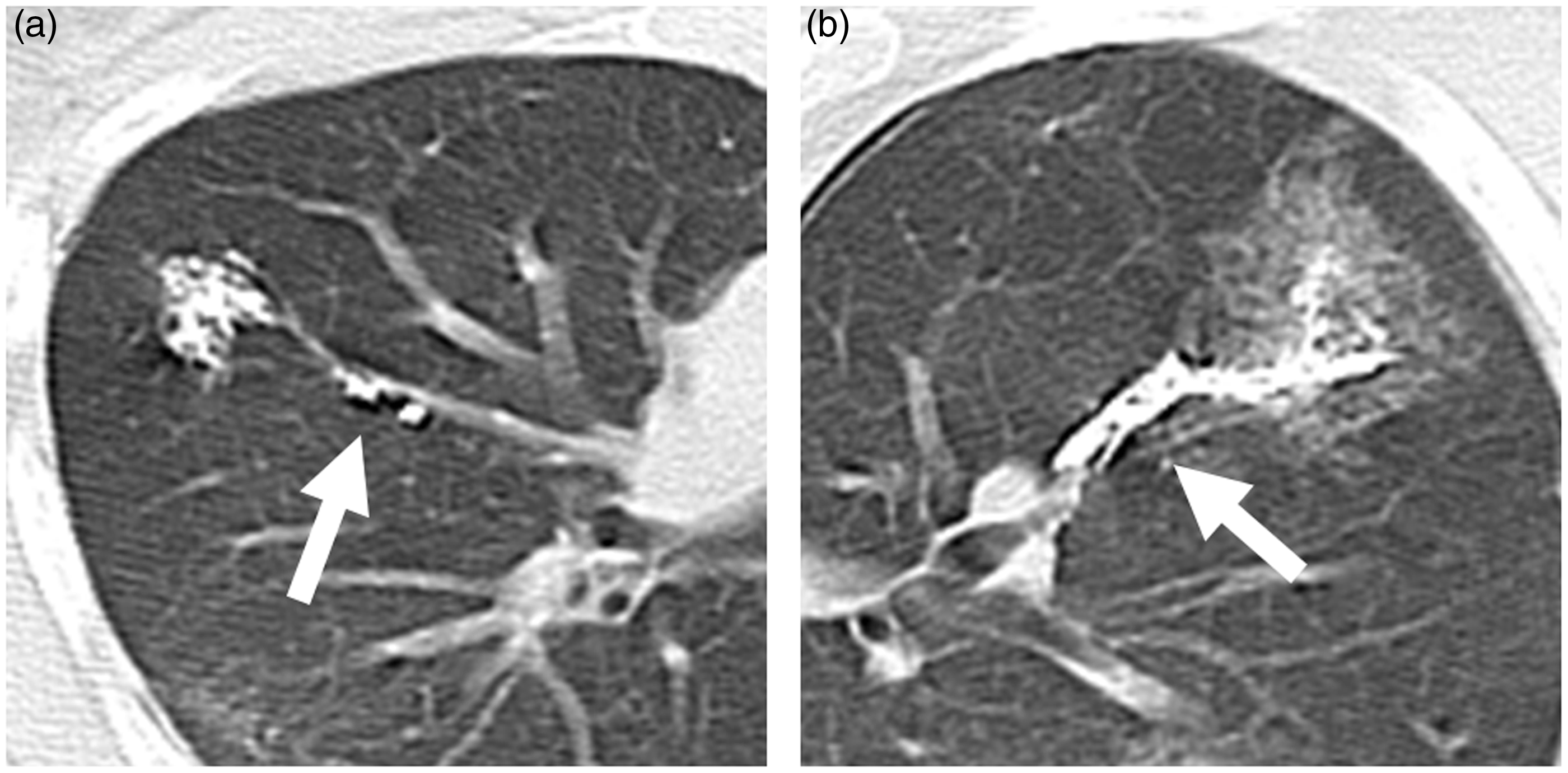
The accumulation and distribution of lipiodol with regard to the nodule-related factors.
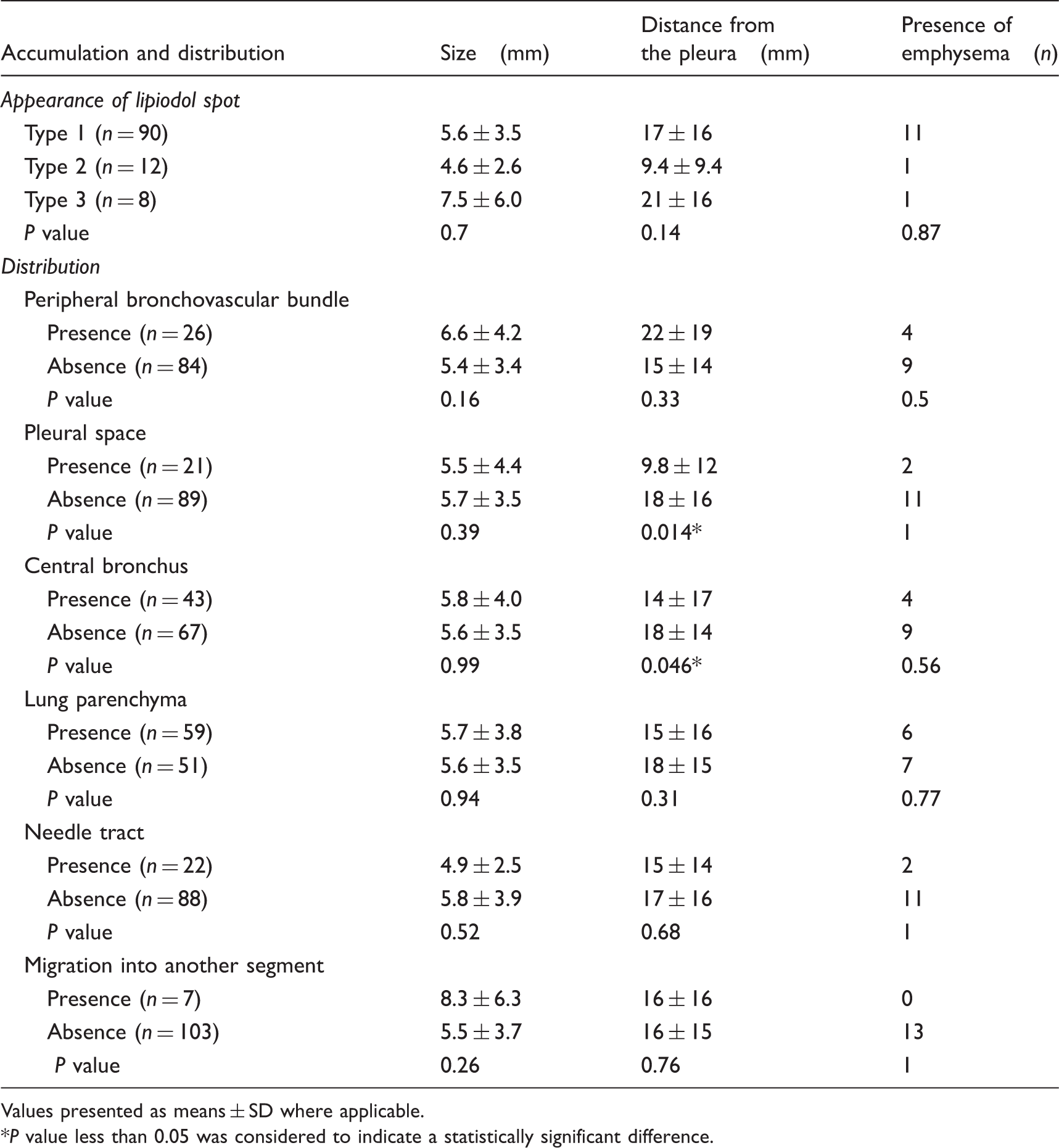
Values presented as means ± SD where applicable.
*P value less than 0.05 was considered to indicate a statistically significant difference.
With regard to adverse events, pneumothorax occurred in 39 (61%) of 64 sessions and a chest tube was necessary in 14 sessions (22%). Among 38 patients with single marking in one session, pneumothorax occurred in 17 sessions (44%), while among 26 patients with multiple markings in one session, pneumothorax occurred in 22 sessions (85%). Pulmonary hemorrhage along the needle tract occurred in 39 (35%) of 110 punctures. There were no cases with severe respiratory distress after the procedure. In addition, there was no systemic embolization.
Discussion
In this study, type 1 accumulation was obtained in the majority of cases. In these cases, the lipiodol spot was clearly shown by fluoroscopy in surgery, which led to successful resection. In the case of type 2 appearance caused by diffusion in the surrounding lung structures through the pores of Kohn, the whole lipiodol spot was shown as a round mark by fluoroscopy at surgery. Therefore, it was useful as a VATS marker. Thus, it can be said that type 1 or 2 appearance of the accumulation of lipiodol is necessary for its use as a marker for VATS. Distribution into the bronchus and lung parenchyma around the nodule frequently occurred. Distribution into the bronchus and the pleural space was a major cause of type 3 appearance of lipiodol accumulation. Hence, additional marking was necessary when type 3 appearance was seen. In our study, distribution into the central bronchus and pleural space occurred at high frequency in nodules with a short distance from the pleura.
The accumulated lipiodol was resected with the nodule at surgery; however, lipiodol that migrated into another segment through the bronchus remained. In most of these cases, it disappeared spontaneously. In a previous study, lipiodol remained for at least 1 week upon direct injection into normal experimental animal lung (16). Yamagami et al. have reported a case of pneumonia occurring 16 days after lipiodol marking because lipiodol migrated into the contralateral lung (21). In addition, injected lipiodol induced a certain inflammatory change; however, the extent was not associated with the histopathological features (22).
There is a possibility that, in lipiodol marking, the lipiodol is injected into the pulmonary artery or vein, although no reports of this appear to have been published. In lymphangiography, oil embolization to the pulmonary arteries has been reported when using >20 mL of lipiodol (23). In lipiodol marking, the amount of lipiodol is very small, less than 1 mL. Considering this, there might be less of a risk of systemic or pulmonary embolization. In our study, accumulation in the peripheral bronchovascular bundle was shown. It is not clear whether this was the bronchus or pulmonary artery; however, there were no symptoms caused by pulmonary embolism. Lipiodol marking also has a potential risk of air migration into adjacent vessels. In our study, there was no obvious air embolization. In particular, it is important to fill the lumen of the needle before accessing the nodules and to avoid the large vessels along the tract by using CT fluoroscopy. Nonetheless, it should be understood that careful injection of lipiodol is needed.
Kim et al. have reported on performance of lipiodol accumulation (8). They classified lipiodol accumulation scores on a four-point scale regarding whether accumulation within the nodule occurred or not. However, they did not mention the distribution of lipiodol in the surroundings. By their method, lipiodol was injected into the targeted nodule and a small nodule was a risk factor for low point accumulation. Direct puncture of the nodule was associated with the potential for dissemination. We injected lipiodol near the targeted nodule avoiding a direct puncture. Distribution to surrounding structures was frequently shown. However, there were no serious symptoms related to this. In our results, type 1 or 2 accumulation of lipiodol occurred even if distribution to the surrounding structures was shown and all nodules were successfully resected. The accumulation of lipiodol within the nodule might not be necessary.
Adverse events such as pneumothorax and pulmonary hemorrhage occurred due to insertion of the needle rather than the injection of lipiodol. The incidence of pneumothorax in this study was 61%, which is higher than reported in percutaneous biopsy and radiofrequency ablation for lung tumor (20,24). It was also higher than in previous reports about lipiodol marking, in which the incidence of pneumothorax was reported to be 29–31% (5,8). In our study, multiple markings in one session were performed frequently and the incidence of pneumothorax was 85% in such sessions. By contrast, the incidence of pneumothorax in patients with single marking in one session was 17 of 38 sessions (44%), which was similar to that of other transpulmonary interventional radiological procedures (20,24). More than two markings in one session could be a risk factor for pneumothorax. The incidence of insertion of a chest tube was also higher than reported in the literature. The reason for this was to avoid worsening of the pneumothorax by positive pressure ventilation of intubation at surgery. Another reason was to inflate the lung by continuous air drainage and to make puncture easier in patients with multiple markings in one session.
In conclusion, lipiodol could be well detected at the nodules upon type 1 and type 2 accumulation after lipiodol marking. However, lipiodol was also distributed in various lung structures. Fortunately, there were no serious symptoms related to the accumulation and distribution of lipiodol. When multiple nodules were marked in one session, pneumothorax frequently occurred; however, there were no serious symptoms. Lipiodol marking under CT fluoroscopic guidance is a safe procedure for the localization of small pulmonary nodules before VATS.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.