
Abstract
Background
Imaging of cervical carcinoma remains challenging as local infiltration of surrounding tissues cannot always be discriminated safely. New imaging techniques, like diffusion-weighted imaging (DWI) have emerged, which could lead to a more sensitive tumor detection.
Purpose
To evaluate the benefits of DWI for determination of size, local infiltration, and tumor grading, in patients with primary and recurrent cervical cancer.
Material and Methods
In this prospective, study we enrolled 50 patients with primary (n = 35) and recurrent (n = 15) tumors. All patients underwent 3T magnetic resonance imaging (MRI) including conventional (e.g. T1/T2 ± fs ± contrast) sequences and DWI (b-values of 0, 50, 400, 800 s/mm2). All images were analyzed by three readers with different experience levels (1, 3, 6 years), who compared image quality, tumor delineation, dimensions, local infiltration, lymph node involvement, and quantified ADC values compared to the histopathological grading.
Results
Additional use of DWI resulted in significantly better (P < 0.001) tumor delineation for the least experienced reader, but not for experienced readers. Tumor dimensions were assessed almost equally (P > 0.05) in conventional sequences and DWI. Use of DWI led to an increase in sensitivity of infiltrated adjacent tissue (from 86% to 90%) and detection of lymph node metastases (from 47% to 67%). Quantitative assessment of carcinomas showed lower ADC values (P < 0.001) with significant inverse correlations between different grading levels.
Conclusion
Our study demonstrates the overall benefits using DWI in 3T MRI resulting in a higher reader confidence, sensitivity of tissue infiltration, and tumor-grading for cervical cancer.
Introduction
Despite new surgical and conservative approaches like total mesometrial resection (1) and use of extended radiochemotherapy (2) cervical carcinoma still remains the third most common malignancy in women worldwide and is characterized by a high mortality rate (3). Imaging of local spread (e.g. involvement of the bladder, rectum, and parametrium) and the detection of lymph node involvement still remains challenging but is inevitable for determination of an adequate therapy even if surgical staging remains the most accurate diagnostic step and is especially recommended for ≤TIIb tumors according to German guidelines for cervical carcinomas (4).
Magnetic resonance imaging (MRI) is the state of the art modality for presurgical staging and follow-up examinations (5,6). A crucial prognostic factor in cervical cancer staging is the infiltration of the parametrium (FIGO IIB), which is a cut-off criterion for extended surgical approach via total mesometrial resection (TMMR), which means the resection of the morphogenetic unit of the uterus, as performed in our institution (7) or Wertheim-Meigs procedure (8), which is still seen as the surgical standard. However, especially in North America, patients with tumor staged FIGO IIB undergo a primary chemotherapy. For MRI, accuracy, sensitivity, and specificity of parametrical infiltration is in the range of 68–95%, 68–79%, and 80–84%, respectively (9), for standard imaging protocols including T1-weighted (T1W) and T2-weighted (T2W) sequences in at least two planes and T1W sequences after injection of contrast media. However, over recent years several new imaging techniques, like DWI and dynamic contrast-enhanced (DCE) imaging have emerged and also been embedded in pelvic examinations (10,11).
DWI hereby serves as a functional technique, which provides information about water mobility, tissue cellularity, and stability of membrane integrity. Present studies show promising and reliable results discriminating cervical carcinoma from healthy tissue and also to evaluate tumor grading (12) in ADC maps. Additionally, previous studies (13) show a beneficial effect using higher magnetic field strengths (3 T) in pelvic examinations with significantly higher image contrast and less motion artifacts probably due to shorter scan times. The purpose of this study was to evaluate possible advantages of DWI compared to standard T1/T2 sequences in 3T MRI regarding local tumor invasiveness, lymph node infiltration, tumor grading, and overall observer confidence.
Material and Methods
Patients
Our institutional review board approved this study and informed consent was obtained from all patients. Fifty female patients (mean age, 52 years; age range, 30–80 years) with a high clinical suspicion for primary cervical cancer (n = 35) (sonographic or palpable lesion, positive tumor markers, and/or positive histological samples) or recurrence (n = 15) of cervical cancer were prospectively enrolled in this study between March 2010 and February 2013. All patients who were clinically suspected of having cervical cancer and diagnosed by MRI also underwent further clinical evaluation including bimanual pelvic examination, chest radiography, cystoscopy, and sigmoidoscopy. After completion of initial staging 21 patients underwent a total mesometrial resection (TMMR; n = 16) or a lateral extended endopelvine resection (LEER; n = 5) and the resected specimens and lymph-node-bearing tissues were sent for histopathological workup. The decision on therapy was based on a combination of MRI results and clinical FIGO stage. A histopathological sample was obtained for all other patients (n = 29) who did not receive surgical treatment
MRI
All scans were performed on a 3 T MR scanner (Trio Tim, Siemens®, Erlangen, Germany). In order to reduce bowel movement, patients were recommended to fast 4 h prior to imaging. Depending on contraindications patients received either 1 mg glucagon (Glucagen Novo Hypokit®, Novo Nordisk, Mainz, Germany), or 20 mg butylscopolamine (Buscopan®, Boehringer-Ingelheim, Ingelheim, Germany) to prevent artifacts from peristalsis.
MRI sequences
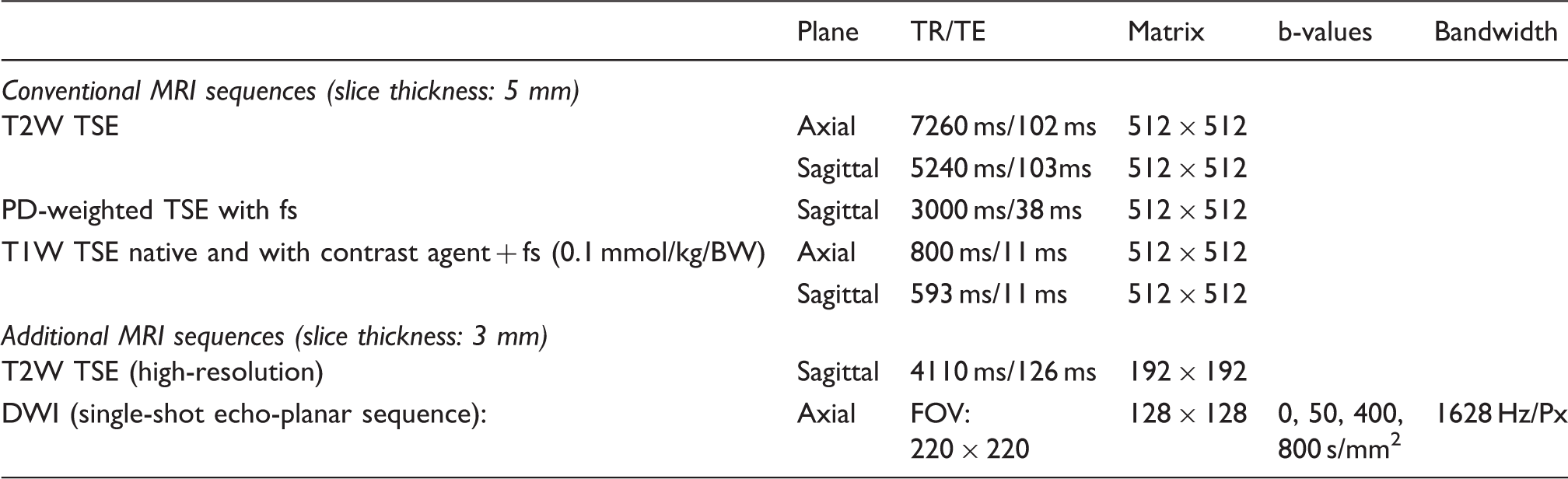
Image analysis
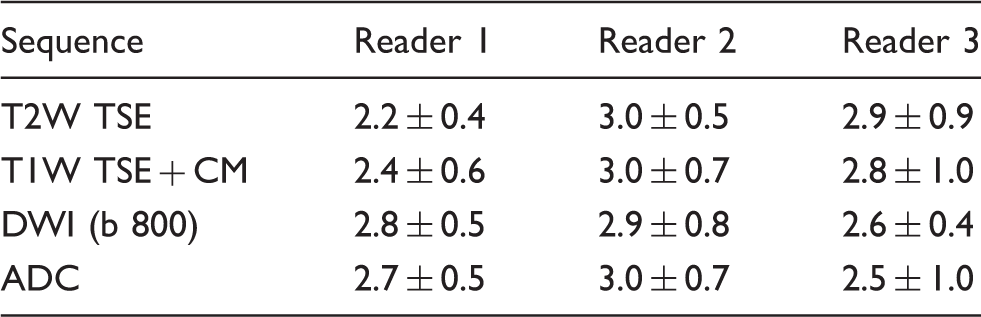
Three readers with different experience levels in gynecological MRI (Reader 1, 1 year; Reader 2, 3 years; and Reader 3, 6 years) independently reviewed all sequences. Every reader rated the image quality and tumor delineation of each sequence using a Likert-scaling system in the range of 0–4 (0, insufficient; 1, poor; 2, adequate; 3, good; 4, excellent). Criteria for image quality and tumor delineation were presence of motion artifacts, signal-extinction due to metal implants, SNR, and overall tumor visibility (according to general MR criteria with increased T2 signal, signal reduction in T1, and accumulation of contrast medium).
Largest tumor dimension, which was defined as the maximum antero-posterior (a.p.) and lateral length, was determined in every sequence, after the readers were instructed how to perform this measurement.
Local tumor extension and infiltration of adjacent tissue was rated by each reader for every single sequence, analyzing conventional datasets first and additional DWI datasets afterwards. Sequences were displayed only one after the other, so there was a natural delay of approximately 20 min from analyzing the T2W sequence and the DWI. For each dataset parameters like infiltration of the parametrium, bladder infiltration, rectal infiltration, and lymph node involvement were evaluated (0, not ratable; 1, no evidence; 2, suspicious; 3, highly suspicious) and the radiological T- and N-stage established. Criteria for the diagnosis of parametrial invasion were: disruption of the cervical margin; tumor mass inside the parametrium; thickening of the uterine ligaments; and no definable healthy cervical tissue. Criteria for the diagnosis of lymph node metastasis were: short-axis diameter >10 mm; round shape; and strong contrast medium enhancement (14).
For pelvic examinations in which MRI could detect lesions, averages of three representative (areas with visually highest alteration of diffusion/lowest ADC) polygonal-shaped regions of interest (ROIs) were defined within the lesions on the axial DW images in the slices where the largest lesion was visible, while referring to the corresponding T2W images for verification of the zonal boundaries. The ROIs were then transferred to the corresponding axial ADC map. Additionally three ROIs were defined within MR-morphological healthy cervical stroma. Maximum, mean, and minimum SI values were measured for tumor and normal cervical stroma in T2-TSE, DW images (b50, b400, and b800) and ADC-coefficients (ADCmin, ADCmean, and ADCmax) were determined.
Histopathological analysis
The histopathological examination of the radical hysterectomy specimen was made in a standardized manner as described previously (1,15,16). The tumor size was determined on the fixed specimen. All tumors were staged and classified according to the WHO and TNM classifications (17,18).
Statistical analysis
Datasets were evaluated on a syngo.via work suite (Siemens®, Erlangen, Germany). Statistical analysis was performed with the data analysis program SPSS® 20 (IBM®, Armonk, NY, USA). Statistical significance was considered for a P value less than 0.05. One-way ANOVA analysis and Mann-Whitney U test were used to compare the differences in ADC values, tumor size, and quality rating of each sequence.
Results
Image quality and tumor delineation
Evaluation of image quality and tumor delineation (Fig. 1) indicated that the reader with the lowest experience (Reader 1) scored the DWI sequence significantly better than the conventional sequences (P < 0.001). In comparison, Reader 2 ranked all sequences almost equally with approximately same values (P = 0.882), whereas Reader 3 scored the conventional MR sequences better than the additional DWI, but not significantly (P = 0.184, Table 2).
Assesment of image quality and tumor delineation for different sequences (T2, T1 postcontrast, ADC, and DWI with b = 800) by each reader with different experience (A = Reader 1 with 1 year of experience, B = Reader 2 with 3 years of experience, C = Reader 3 with 6 years of experience). Evaluation of image quality and tumor delineation in different sequences dependent on reader experience by using a Likert scale.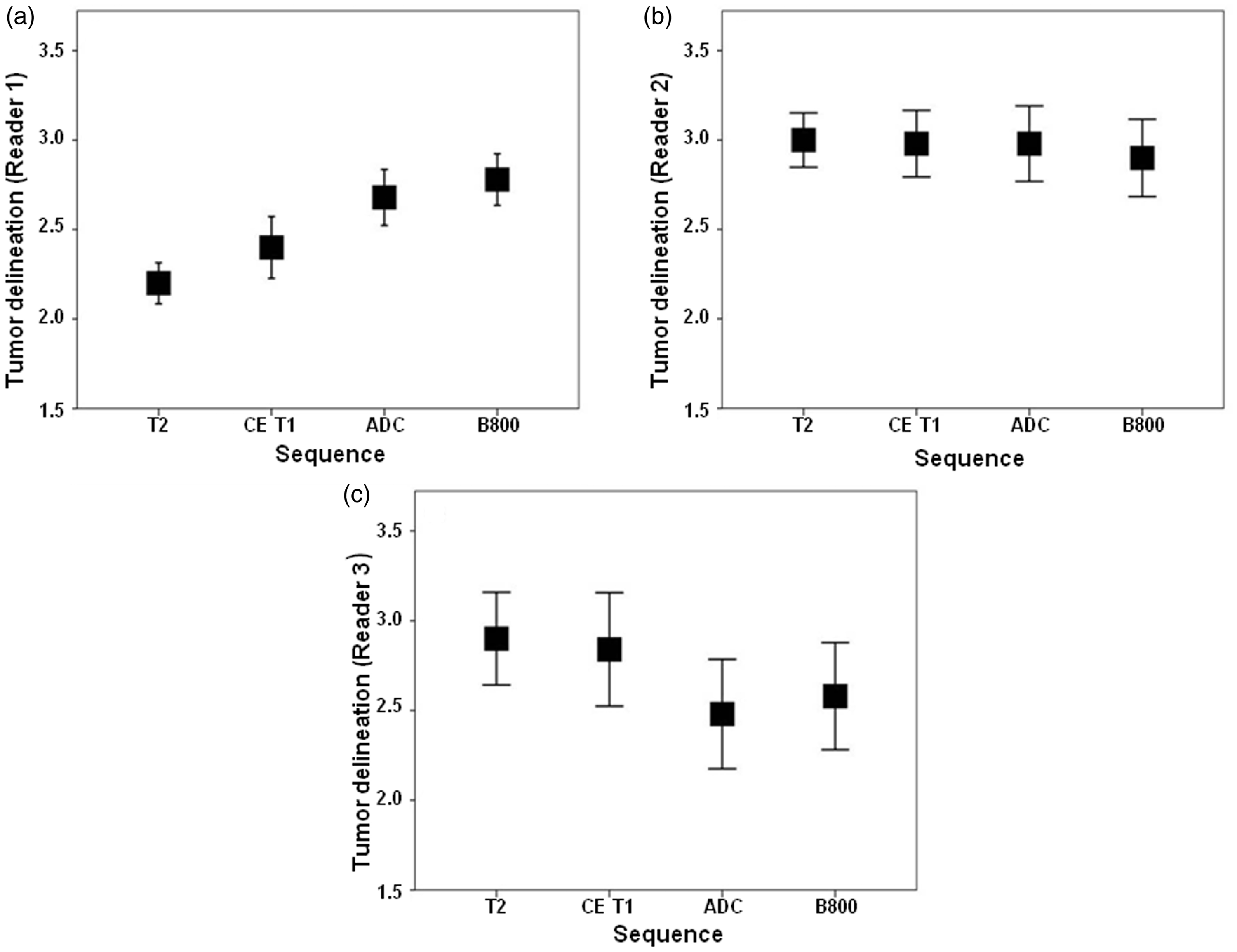
Thus, the FIGO stage of primary cervical cancer was determined according to clinical, pathological, and MRI evaluation (FIGO IB1/2, 6 patients; FIGO IIA, 1 patient; FIGO IIB, 14 patients; FIGO III, 7 patients; and FIGO IV, 7 patients).
Tumor size
Evaluation of maximum tumor dimension (mean ± SD, width × depth in cm) in different sequences dependent on reader experience.

Infiltration of adjacent tissue and lymph nodes
Sensitivity and specificity for the detection of parametrial infiltration, metastatic lymph nodes, and bladder infiltration by all three readers by the use of T1/T2 and additional use of DWI.
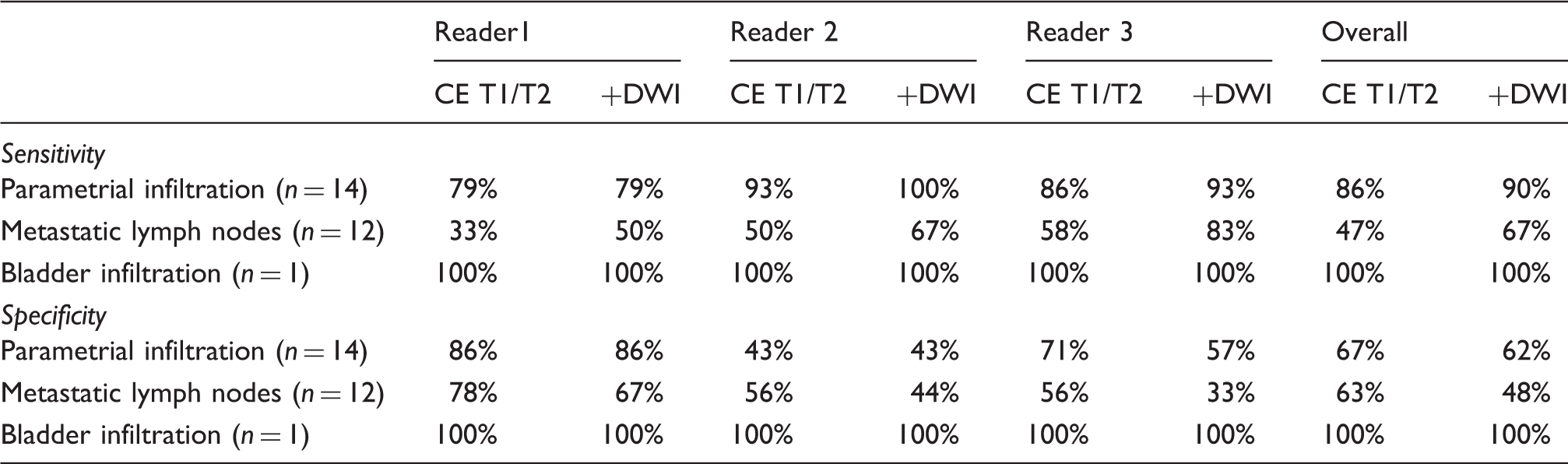
Overall evaluation of metastatic lymph node involvement showed an increase of sensitivity from 47% to 67% and a decrease of specificity from 63% to 48% applying additional DWI. Furthermore we found a slight increase of lymph node metastasis detection accuracy from 53% to 61% using additional DWI (Fig. 2).
Comparison of sensitivity and specificity for parametrial invasion and lymph node for conventional MRI sequences and additional DWI.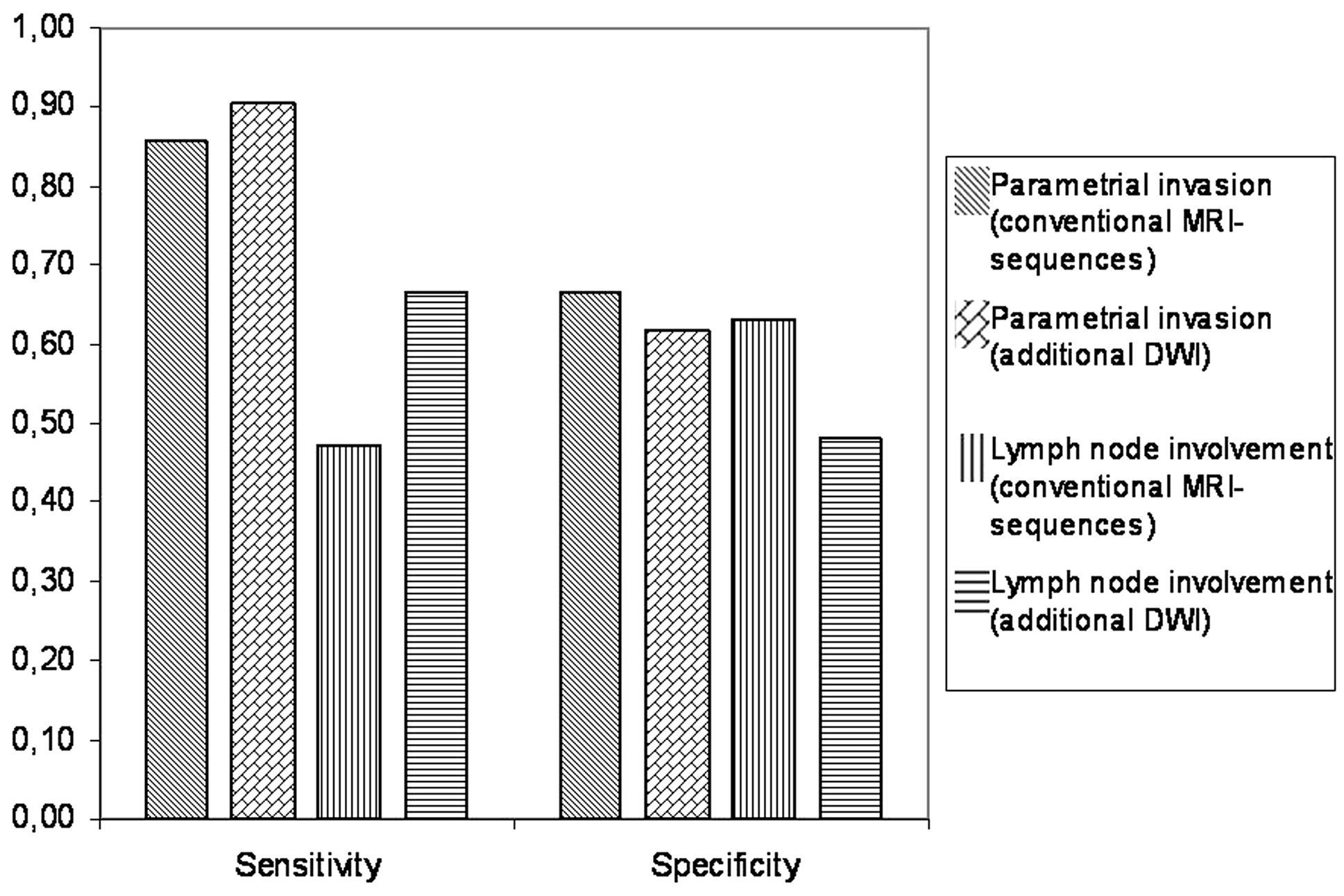
Use of DWI increased the confidence of metastatic lymph nodes detection from suspicious to highly suspicious in three cases (Readers 2 and 3) and in one/three cases for parametrial invasion (Readers 1 and 3, respectively).
ADC values
Measurement of ADC values (×10–3 mm2/s, mean ± SD) for tumor-free cervical stroma and different tumor grades.

For ADCmean values there was a significant difference between G1 and G2 (P = 0.03) and G1 and G3 (P = 0.001) but no significant difference between G2 and G3 (P = 0.56) (Fig. 3).
ADC values for different differentiation grades of tumor tissue (G1–G3) in comparision to tumor-free cervical stroma (=stroma). Graph A shows results for ADCmin, Graph B results for ADCmean, and Graph C results for ADCmax.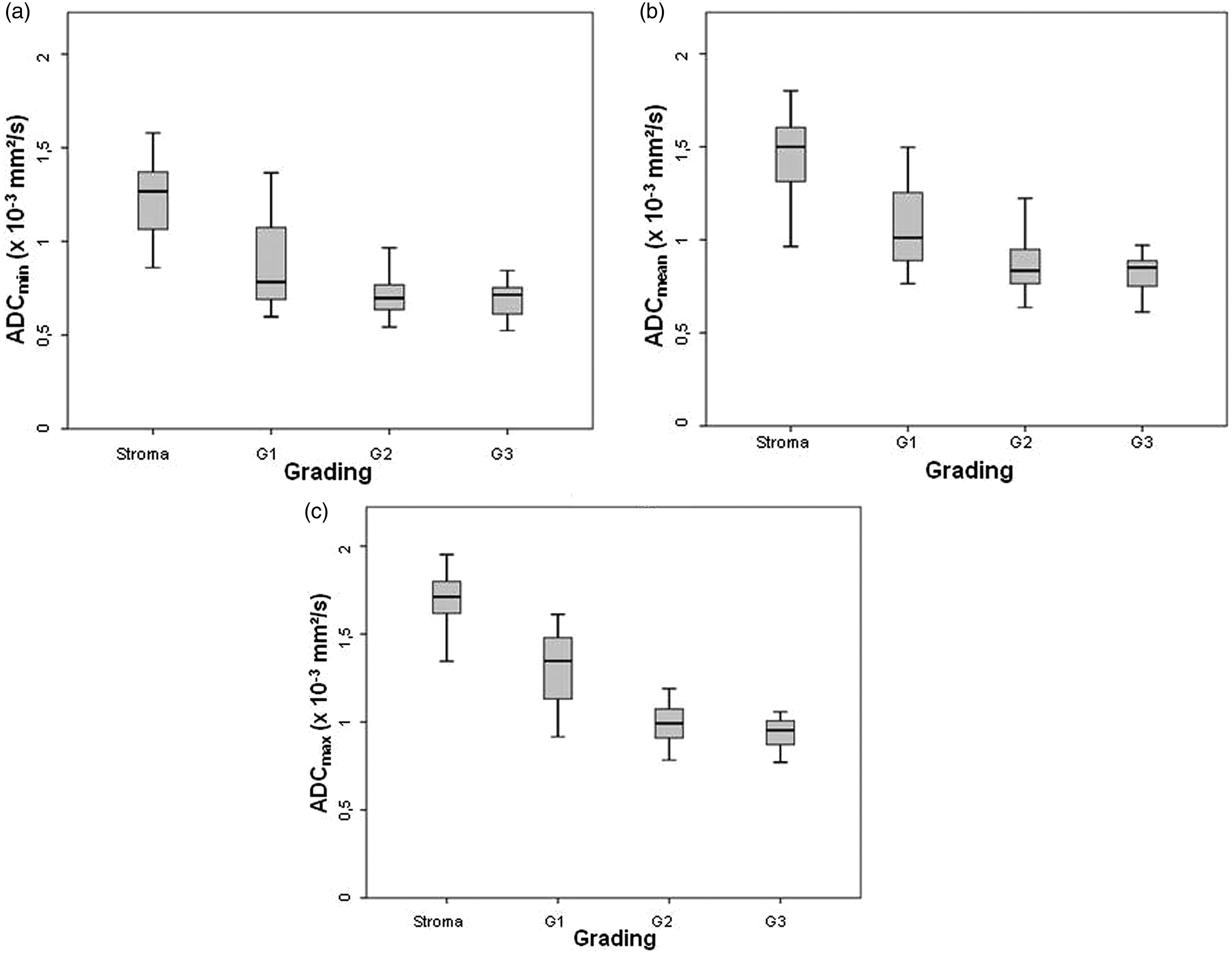
Discussion
Imaging local and distant invasiveness of cervical carcinoma with higher magnetic field strengths contributes significantly to optimized staging and is inevitable for presurgical planning and adjustment of therapy (13). Nowadays MR scanners with field strengths of 3T have become widely available in clinical routine.
Emerging from stroke assessment (19) DWI has gained a lot of attention in several imaging approaches like oncologic staging, therapy response, and characterization and detection of inflammation. In our study we analyzed the benefits of additional use of DWI with conventional contrast-enhanced T1/T2 sequences. Interestingly the reader with the lowest experience in gynecological imaging found the additional use of DWI and ADC maps more useful in detection and delineation of tumor tissue. More experienced readers, in our study with 3 and 6 years of experience seemed to prefer conventional MR sequences like high-resolution T2 and contrast-enhanced T1 images over DWI in establishing their diagnosis and delineating tumor boundaries (Fig. 4), which can be explained due to more profound experience with common MR sequences.
Large cervical carcinoma; with parametrial infiltration on the left side (white arrow = parametrial infiltration on the left side), which can be sufficiently detected in every sequence (axial plane: A = T2, B = T1CM, C = b800, D = ADC; sagittal plane: E = T2 with marked angulation of the axial plane).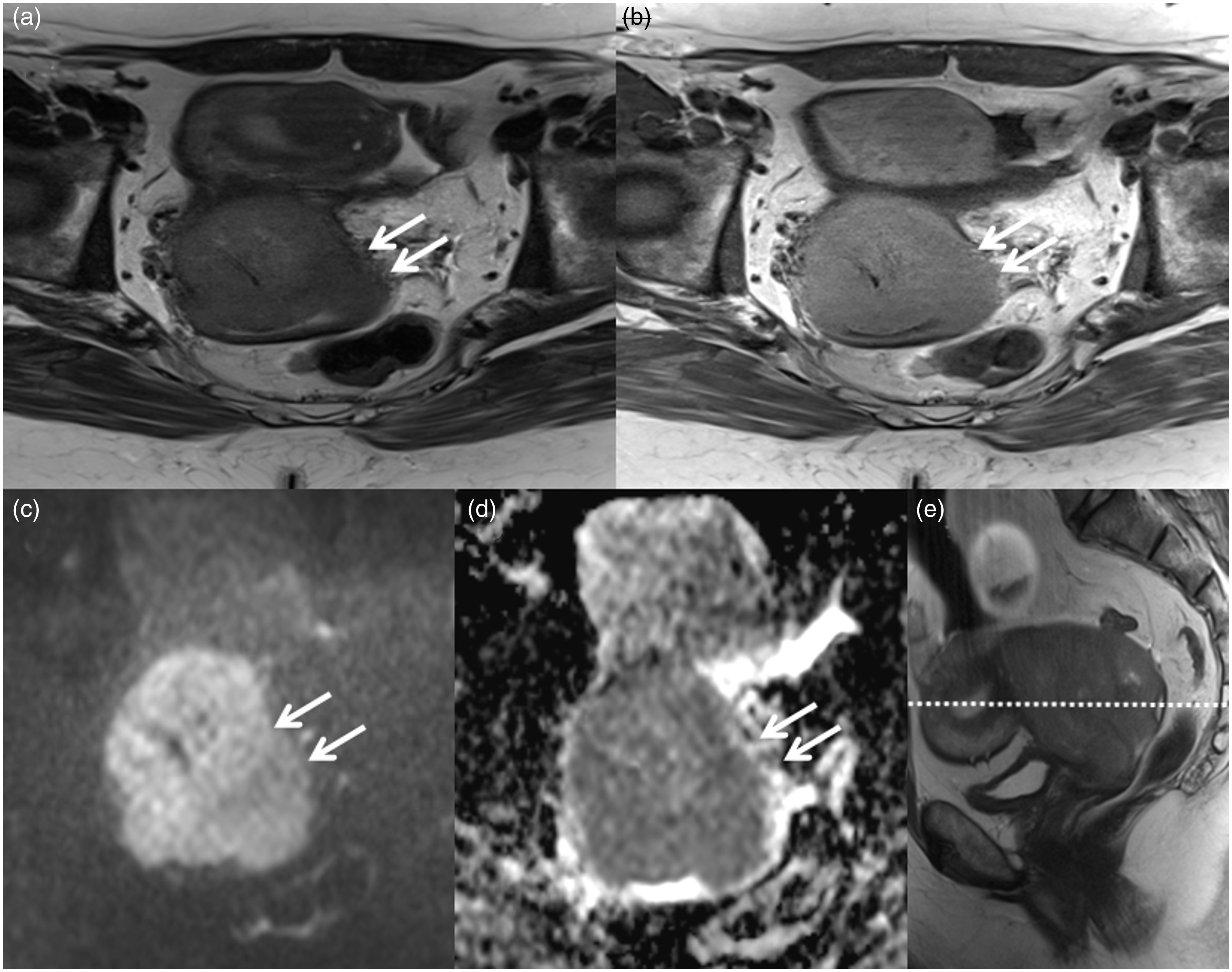
Regarding maximum tumor dimensions there was no significant difference in average size comparing conventional and diffusion-weighted sequences, which makes DWI equal to contrast-enhanced T1/T2 sequences despite reduced anatomical information.
Local tumor spread and lymph node involvement is crucial for disease outcome and therapy strategy in every malignant disease. For MR, size is the main criterion used to differentiate between nodal metastases and benign lymph nodes, and the most widely quoted threshold above which a node is considered malignant is 10 mm in short-axis diameter (14). Other, softer criteria commonly used are, for example, a round shape, central necrosis, soft tissue of the same signal intensity of the tumor within the node, and extracapsular extension of the tumor beyond the nodal capsule. The presence of visible necrosis within the node, seen as pockets of high T2 signal intensity, has a positive predictive value of 100% (20) for nodal involvement. However, in clinical routine these parameters often become secondary, especially in patients who underwent neoadjuvant radiation therapy or chemotherapy, which generally results in morphological tissue changes. Liyanage (21) investigated these standard criteria in cervical carcinoma and found that the sensitivity for detecting nodal metastases on MRI is low with a wide range of 29–86%. This is due to the inability to detect micrometastasis in normal-sized nodes. In light of that new imaging techniques for cancer staging combining nuclear and radiological hybrid techniques like PET/CT or PET/MRI have emerged to improve the assessment of lymph node involvement.
18F-fluorodeoxyglucose (FDG)-PET/CT has been proven to be a useful tool for oncological lymph node staging. Direct comparison of sensitivity in PET/CT and MRI of lymph nodes showed superior results for PET/CT with percentages of 91% vs. 73% and specificity of 100% vs. 83% in a cohort of 11 patients (22). However, there are differences concerning sensitivity with respect to micrometastasis. Leblanc (23) investigated morphological unsuspicious lymph nodes with PET and correlated the results to the histopathological samples with a sensitivity of just 33% and a specificity of 94% for PET/CT. Other issues for PET techniques, especially in the detection of malignomas of the female pelvis, are the close proximity to the bladder and ureters which often cover relevant tumor areas. However, there is evidence that PET is superior to MRI in detection of malignant lymph nodes (24). Even though these modalities become more available they should preferably just come into play when there is suspicion of distant metastasis, according to German guidelines (S3 guidelines, 4). The additional use of DWI in detection of nodal metastasis has been discussed controversially in the literature throughout the last years. We found a significant increase in sensitivity for the detection of lymph node metastasis with a decrease in specificity for all three readers. Over all there is an increase of 9% for diagnostic accuracy (Fig. 5). For the evaluation of the infiltration of surrounding tissue only a slight increase in sensitivity could be found by the additional use of DWI.
Metastatic lymph node involvement next to the external iliacal vessels (white circle = metastatic lymph node), which is not suspicious in conventional MRI sequences but does show diffusion restriction (axial plane: A = T2, B = T1CM, C = DWI with b = 800, D = ADC).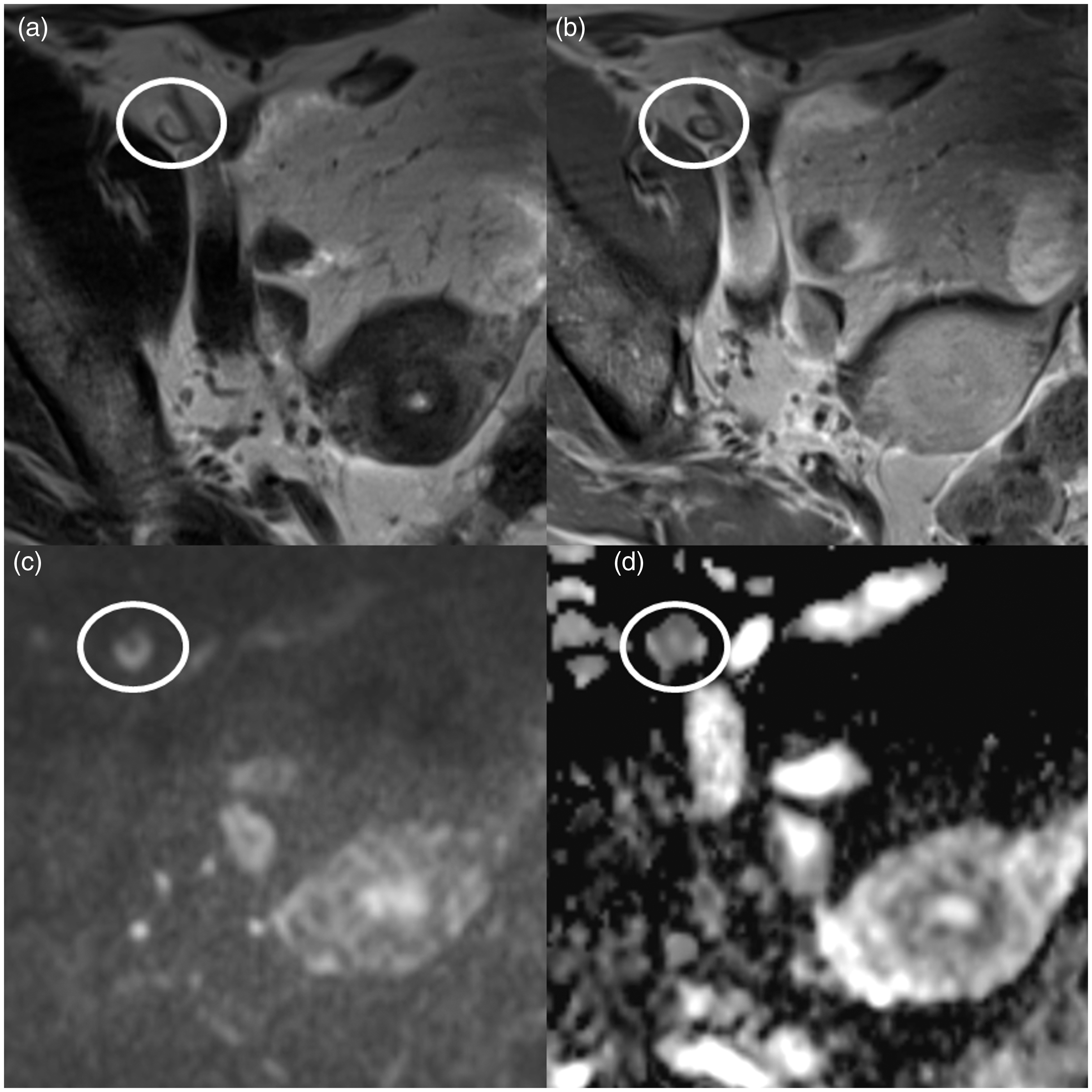
One other benefit of DWI is the determination of the tumor grade as discussed in previous studies, e.g. Kuang et al. (12). In poorly differentiated tumors water can move less freely due to the increasing cellularity with hydrophobic membrane integrity, extracellular tortuosity, and tissue disorganization, resulting in lower ADC values (25,26). Due to the significant difference between the ADC values of healthy and tumorous tissue, it is possible to differentiate tumor-free and tumorous tissue by quick measurement of ADC values through proper ROI placement. For our MR scanner we found significantly higher ADC values for healthy cervical tissue compared to malignant tissue. Assessment of differentiation levels show that well differentiated tumors (G1) have higher ADC values compared to moderate and poorly differentiated tumors (G2 and G3). Determination of a distinct cutoff value for different tumor grades remains difficult. In our study population, probably due to a relatively inhomogeneous distribution of tumor grades, we could not establish a valid cutoff value. However, it has already been shown that calculated ADC values seem to differ between MR scanners (27), so comparison of ADC values from different vendors has to be done with great caution, if at all. Compared to a study of Kuang et al. (12), we found comparable ADC values for tumor-free tissue and G2 tumors, but slightly higher ADC values for G1 and G3 tumors. Further investigation of ADC values according to the tumor grade in a larger, more homogenous patient cohort with primary cervical carcinomas and thorough histopathological workup might be helpful to define exact cutoff or normalized values for ADC to improve the tumor characterization, which could result in a more sophisticated therapy approach.
However, there are some limitations to this study. One possible limitation could be a minor reader bias based on the algorithm the images where interpreted. Even though the MR sequences were not viewed all together on one display, readers’ decisions could have been slightly influenced by viewing the conventional sequences first and the DWI afterwards (after approximately 20 min). Another limitation certainly is the missing comparison of MR measured tumor diameter to histopathological samples.
In conclusion, our study demonstrates the overall benefits and additional information given by using DWI in a 3T environment, which resulted in a higher reader confidence for lesion delineation, higher sensitivity for prediction of lymph node infiltration, and possibility of MR-based determination of tumor grading.
Footnotes
Acknowledgments
The authors kindly thank the Department of Gynaecology and Obstetrics (University Hospital Leipzig, Prof. Dr. Dr. M. Höckel, Ms Katja Schmidt) for the admission of selected patients with cervical carcinomas and providing insights into clinical procedures and relevant aspects of embryological tumor behavior. Furthermore, the authors thank the technical radiological staff for supervision of MR examinations and patient surveillance.
Declaration of conflicting interests
The author(s) declare no conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.