
Abstract
Background
Diffusion-weighted imaging (DWI) derived apparent diffusion coefficient (ADC) has demonstrated inconsistent results in pulmonary nodule differentiation. Diffusion kurtosis imaging (DKI), which quantifies non-Gaussian diffusion, is believed to better characterize tissue micro-structure than conventional DWI.
Purpose
To assess the feasibility of DKI in human lungs and to compare its diagnostic value with standard DWI in differentiating malignancies from benign pulmonary nodules.
Material and Methods
Thirty-five pulmonary nodules in 32 consecutive patients were evaluated by DKI by using 3b-values of 0, 500, and 1000 s/mm2 and conventional DWI with b values of 0 and 800 s/mm2. Two observers independently evaluated and compared diagnostic accuracy of mean kurtosis (MK) and ADC values in differentiating malignancies from benign pulmonary nodules. The intra- and inter-observer repeatability (intra-class correlation coefficient [ICC]) were also assessed for each derived measures.
Results
The diagnostic accuracy, and the area under curve (AUC) in differentiating malignancies from benign pulmonary nodule, were not significantly higher for MK (Obs. 1a: 85.70%, 0.87; Obs. 1b: 80.00%, 0.80; and Obs. 2: 82.80%, 0.91) as compared to ADC (Obs. 1a: 77.14%, 0.81; Obs. 1b: 80.00%, 0.85; and Obs. 2: 77.14%, 0.85 respectively). The intra- and inter-observer agreement (ICC) for malignant and benign lesions was substantial for each reading.
Conclusion
The initial results of this study indicate the feasibility of DKI in human lungs. However, there was no significant benefit of DKI derived MK values over ADC for malignant and benign pulmonary nodule differentiation.
Introduction
The most common manifestation of lung cancer is a solitary pulmonary nodule or a solitary pulmonary mass (1). Positron emission tomography (PET) with 18F-fluorodeoxyglucose (FDG) and computed tomography (CT) are two common non-invasive methods used to examine solitary pulmonary nodules or masses with higher diagnostic accuracy. For instance, FDG PET have reported diagnostic accuracy of approximately 90% in differentiating benign and malignant nodules (2). However, it has also been reported to give false-negative results for well-differentiated pulmonary adenocarcinoma (3,4) and false-positive results for inflammatory nodules (5). On the other hand, although the evaluation of tumor vascularity by using contrast-enhanced CT has proven to be useful for distinguishing malignant nodules from benign nodules, some false-positive results have been found with active granulomas or hyper-vascular benign tumors (6,7).
Quantitative tumor assessment has been possible by diffusion imaging. Restricted diffusion in malignant tumors, due to increased cellularity, larger nuclei with more abundant macromolecular proteins, larger nuclear/cytoplasmic ratio, and less extracellular space relative to normal tissues, serve as a basis for quantitative assessment of tumors (8). However, several studies have reported limitations of ADC in differentiating solitary pulmonary nodules (SPN), which is likely due to susceptibility artifacts (9). Moreover, in contrast to Gaussian diffusion assumption of conventional diffusion imaging, in many biological tissues, the presence of barriers, e.g. cell membranes, and compartments, e.g. intracellular and extracellular spaces, alter the water diffusion probability density function (PDF) so that the water diffusion, is not precisely Gaussian but in fact non-Gaussian (10).
On the contrary, diffusion kurtosis imaging (DKI) quantifies the “non-Gaussianity” of the diffusion distribution, thereby, assessing the complexity of tissue micro-structural environments more accurately than conventional diffusion-weighted imaging (DWI) (11). However, DKI has only been applied successfully to human and small animal brain studies so far and has been rarely used for other body organs because of the difficulty in obtaining sufficient signal to noise ratio (SNR) at high b-values. A parameter optimization is necessary to prevent low SNR, inherent in the diffusion technique, from impacting the result of key diffusion parameters (12). Moreover, the difference in magnetic susceptibility at the tumor–lung interface creates inhomogeneity in the local magnetic field disrupting the magnetic resonance signal of the lung tumor similar to the artifact that arise from heart-lung interface. Respiratory and cardiac motions also cause additional image artifacts and signal loss (13).
The purpose of this prospective study was therefore to determine feasibility of DKI in imaging lungs and to evaluate whether DKI is superior to the use of conventional DWI in differentiating malignant from benign nodules.
Material and Methods
The Institutional Review Board of Affiliated Hospital of North Sichuan Medical College approved this study, and informed consent was obtained from all patients.
Participants
This prospective study included 35 pulmonary nodules in 32 consecutive patients (18 men, 14 women; mean age, 65.7 years; age range, 31–88 years), which were detected with CT performed at the Department of Radiology in Affiliated Hospital of North Sichuan Medical College. Three patients had two pulmonary nodules, and the remaining 29 patients had a solitary pulmonary nodule.
The patients were selected according to the following criteria: one or two pulmonary nodules of 10.0–30.0 mm size detected on CT that needed further evaluation; absence of calcification or definite fat attenuation of the nodule by CT; solid and semi-solid nodules were included, but nodules with pure ground glass opacity were excluded; absence of histological diagnosis; absence of history of immunodeficiency; and the patient’s ability to undergo the procedure.
Image acquisition
Magnetic resonance imaging (MRI) examination were performed on a 3.0-T MR scanner (GE Signa Discovery 750 HD, GE Healthcare, Milwaukee, WI, USA), by using a standard 32-channel phase array upper torso surface coil (GE Healthcare). Before diffusion imaging, conventional MRI images were acquired consisting of an axial fat suppressed periodically rotated overlapping parallel lines (PROPELLER) T2-weighted (T2W) sequence (repetition time [TR], 3529 ms; echo time [TE], 73 ms; number of excitations (NEX), 2; section thickness, 4.0 mm; intersection gap, 1.0 mm; matrix, 352 × 320; field of view [FOV], 36.0 × 36.0 cm2) and axial LAVA Flex T1-weighted (T1W) sequence (TR/TE, 3.8/1.1 ms; NEX, 1; section thickness, 5.0 mm; intersection gap, 1.0 mm; matrix, 260 × 192; FOV, 34.0 × 34.0 cm2).
The subsequent diffusion images on pulmonary lesions were obtained in the transverse plane on the basis of T1W and T2W images. The DKI protocol consists of respiratory-gated, single-shot, spin-echo, echo-planar imaging (EPI) DKI with fat suppression performed in the axial plane. A total of 30 motion probing gradient (MPG) directions was used with three b values (0, 500, and 1000 s/mm2) for each direction. Other imaging parameters were as follows: slice thickness/gap, 6/0.0 mm; TR/TE, 8000.0/72.8 ms; FOV, 36.0 × 28.0 cm2; matrix, 128 × 128; NEX, 1; duration, 6–8 min (depending on the respiratory frequency of the volunteers).
For acquisition of standard DWI, a single-shot echo-planar imaging pulse sequence was obtained with following parameters: TR/TE, 3000–4500/65 ms; diffusion gradient encoding in three orthogonal directions; b value, 0 and 800 s/mm2; FOV, 36.0 × 28.0 cm2; matrix, 128 × 128; NEX, 1; duration, 6–8 min.
Image analysis
Multidirectional diffusion data were first analyzed visually for distortions and artifacts. Eddy current distortion was qualitatively estimated by drawing the thorax contours to b0 images, and copying them to diffusion-weighted images. We did not find significant eddy current distortions due to diffusion gradients. Two radiologists (Observer 1: YDJ and Observer 2: WJL), with 4 and 6 years of experience in thoracic MRI, blinded to the histopathologic reports, separately performed the region of interest (ROI) measurements on a workstation by using the commercially available software FUNCTOOL (Function tool 4.4, GE Healthcare). Observer 1 conducted measurements twice, while Observer 2 conducted one measurement. In each measurement, the four ROIs, depending upon the size of lesion (range, 40.0–65.0 mm2), were manually placed on different sections (depending upon the thickness of the lesion) of an axial b0 image of the standard DWI dataset with a reference to the T2W image or CT so as to prevent any necrotic or cavitatory region if present within the lesion. The transfer from DWI to DKI was performed automatically by the evaluation software tool ensuring that the ROI areas were equal and placed on the same anatomical location (Fig. 1). The mean and standard deviation (SD) of the MK and ADC values were calculated as averaged values of the four ROIs. The present study opted to concentrate solely on comparing the relevance of MK with that of ADC values in differentiating malignancy from benign pulmonary nodules and did not report other DKI derived parameters which otherwise could be determined from the present data.
Images of squamous cell lung carcinoma in right lower lobe in a 61-year-old man in whom diagnosis was true-positive. (a) Axial fat-suppressed T2W periodically rotated overlapping parallel lines (PROPELLER) image show mass in right lower lobe. (b) Gray-scale DWI image and (c) color-coded MK map obtained from axial chest DKI of the same patient showing ROI placement within the lesion. (d) Photomicrograph of CT-guided core lung biopsy specimen shows squamous cell carcinoma. Tumor cells are densely packed, with scant cytoplasm.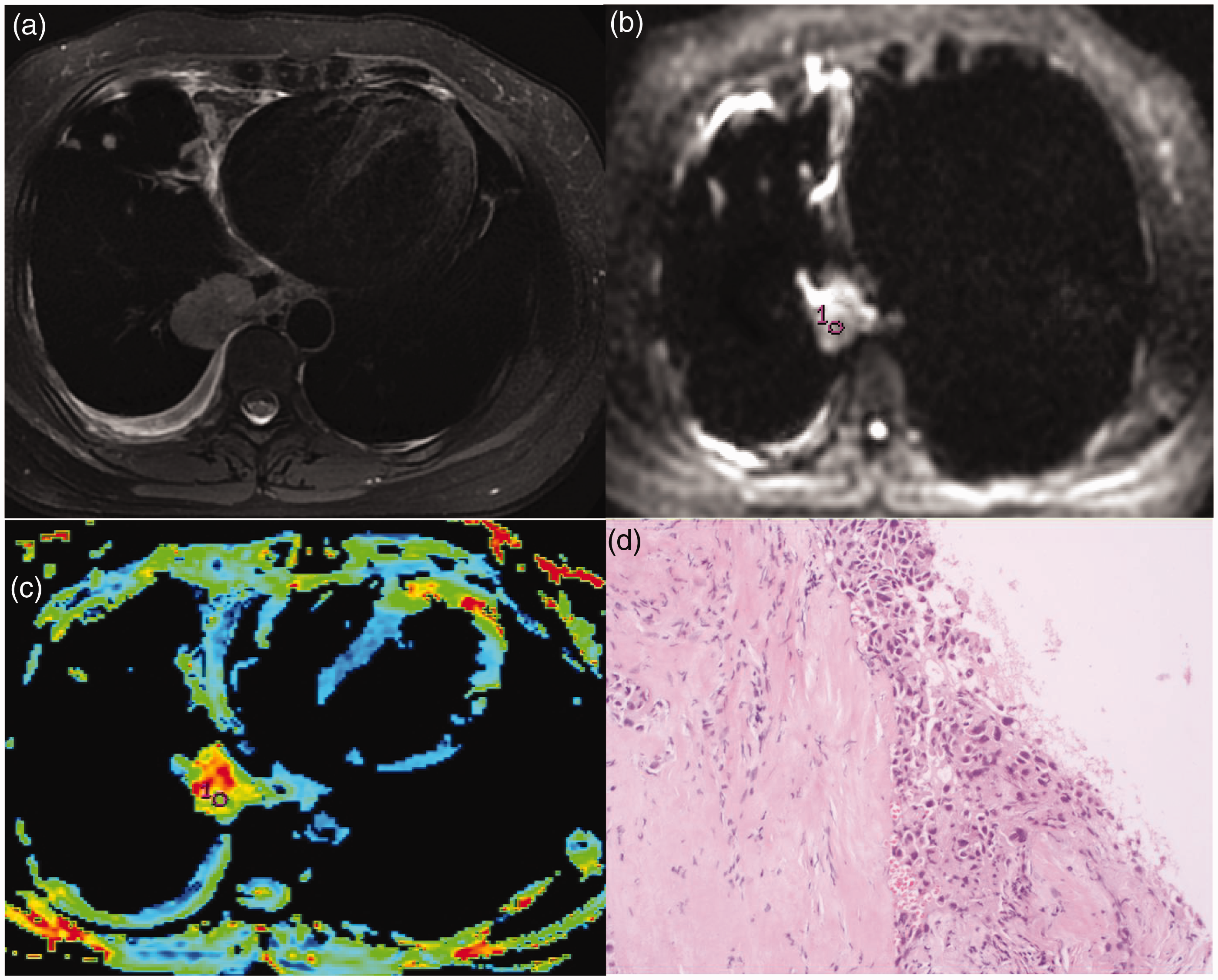
Statistical analysis
The statistical analyses were performed by using the SPSS software package (Version 20.0; SPSS Inc., Chicago, IL, USA). Receiver operating characteristics curve (ROC) were constructed to determine the optimal cutoff value and hence determine diagnostic capability of the MK and ADC value for differentiation between malignant and benign nodules. Repeatability of measurements refers to the strength of agreement between repeated measurements obtained under similar conditions. The intra-observer repeatability, i.e. the differences between repeated measurements by Observer 1 (Obs. 1a and Obs. 1b) and the inter-observer repeatability, i.e. the difference between first measurements made by Observer 1 (Obs. 1a) and the only measurement by Observer 2 (Obs. 2) were assessed using intra-class correlation coefficient (ICC) and Bland–Altman plot. The ICC values were considered to indicate excellent agreement if they were greater than 0.8 and substantial agreement if they were in the range of 0.60–0.79.
Results
Histopathological findings
Histopathological assessment revealed 20 malignant and 15 benign nodules out of 35 SPNs. Among 20 malignant lesions, nine were squamous cell carcinomas, seven were adenocarcinomas, two were small cell carcinomas, and two were metastatic lung cancers. Out of the 15 benign lesions, five were granulomas, three were tuberculomas, two were bacterial pneumonias, one was a lung abscess, two were inflammatory nodules, one was a fibrous nodule, and one was organizing pneumonia.
Mean MK and ADC values of the lesions
Intra-observer repeatability (Obs. 1a: Obs. 1b) for MK and ADC.
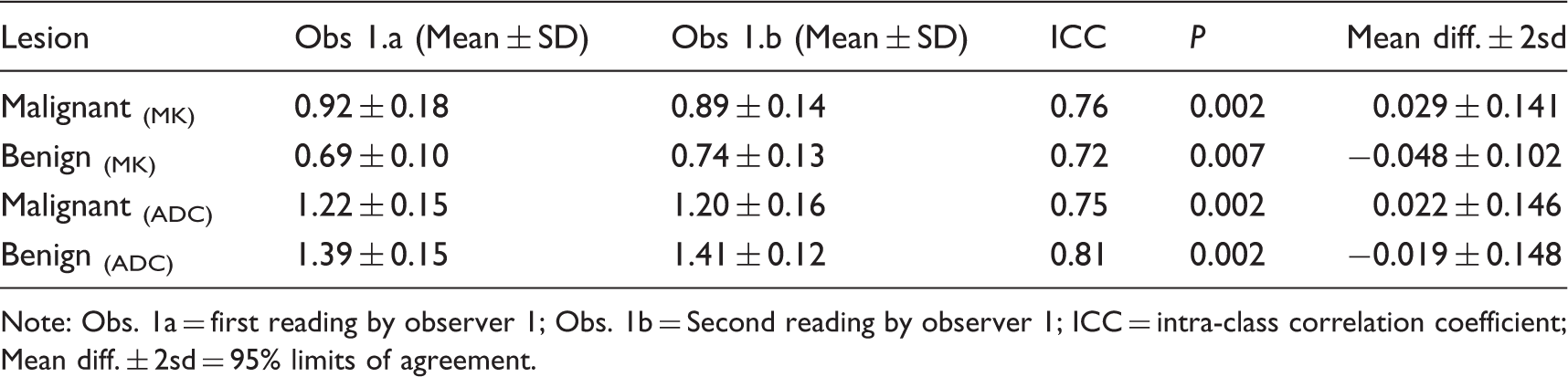
Note: Obs. 1a = first reading by observer 1; Obs. 1b = Second reading by observer 1; ICC = intra-class correlation coefficient; Mean diff. ± 2sd = 95% limits of agreement.
Inter-observer repeatability (Obs. 1a: Obs. 2) for MK and ADC.
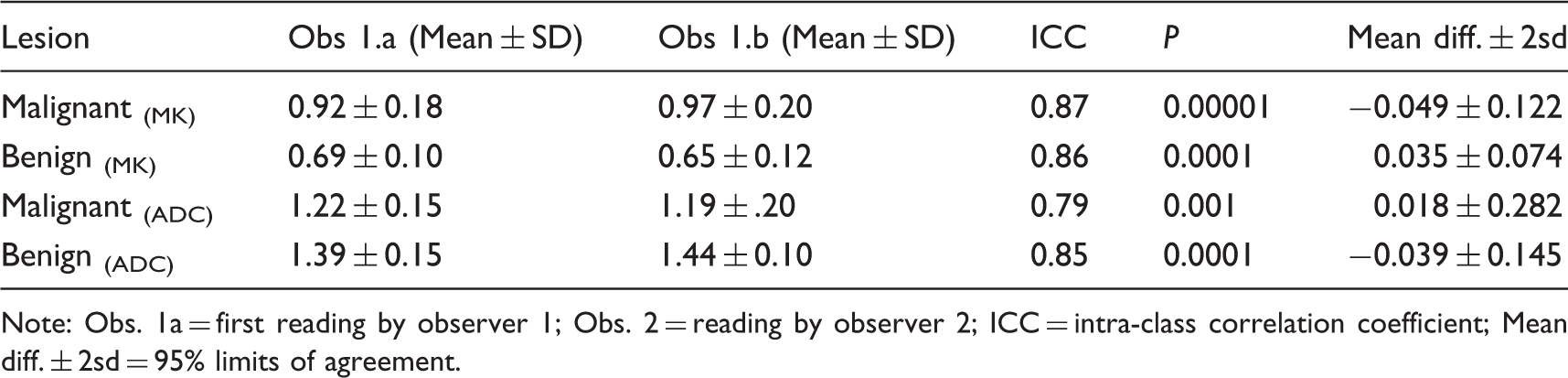
Note: Obs. 1a = first reading by observer 1; Obs. 2 = reading by observer 2; ICC = intra-class correlation coefficient; Mean diff. ± 2sd = 95% limits of agreement.
The mean MK values obtained by Observer 2 for malignant and benign lesions were (0.97 ± 0.20 vs. 0.65 ± 0.12) while ADC values for malignant and benign lesions were (1.19 ± 0.20 vs. 1.44 ± 0.10) × 10−3 mm2/s. Comparisons of MK and ADC values between malignant and benign lesions are shown in Fig. 2.
Box plot of mean kurtosis and ADC values measured by two observers for lung lesions. First reading for MK (a) and ADC (d), second reading for MK (b) and ADC (e) by observer 1 and the only reading by observer 2 for MK (c) and ADC (f) demonstrate a significant difference (P < 0.05) between malignant and benign lesions. * = outlier.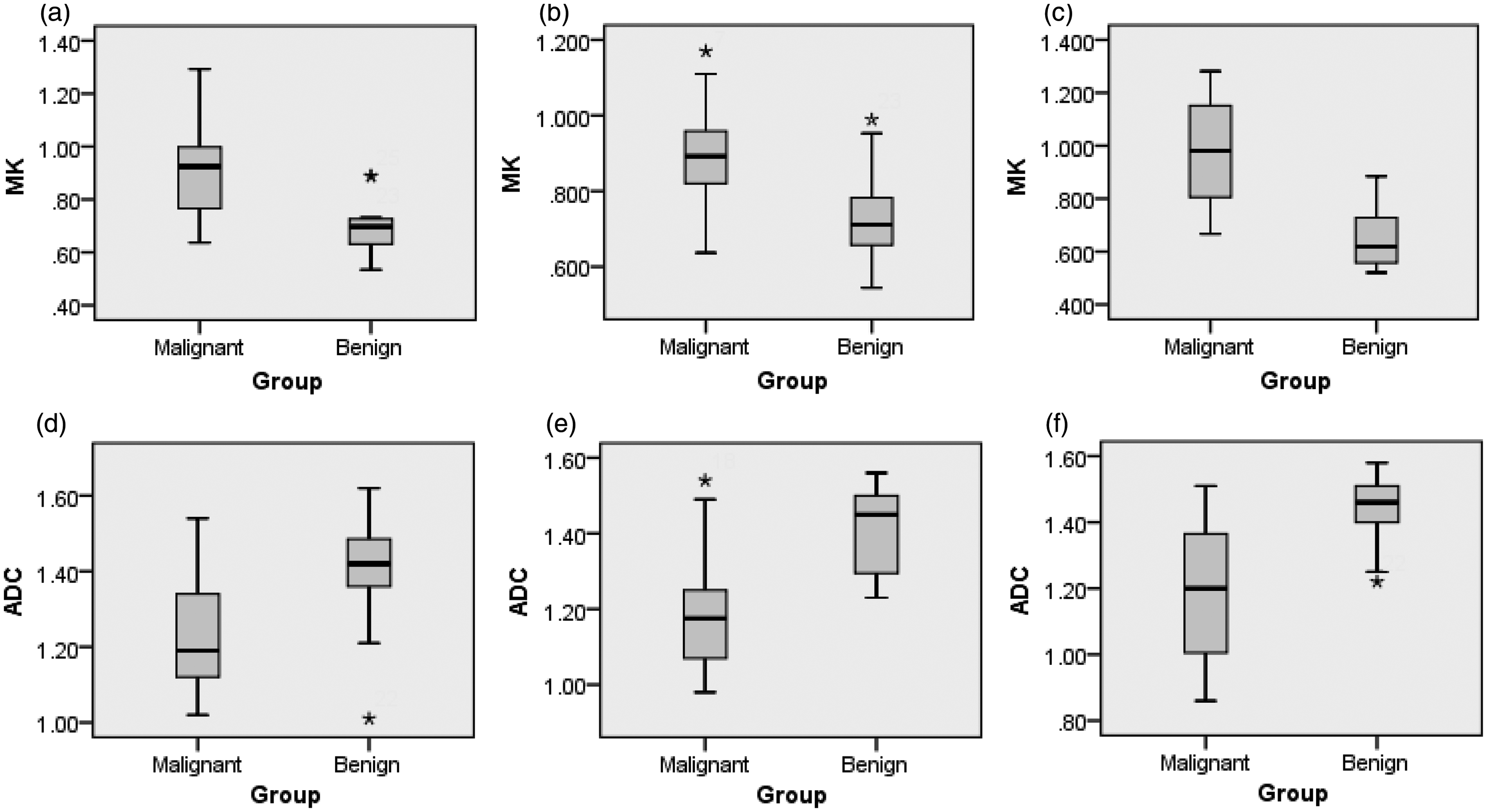
Diagnostic performance of DKI versus DWI
Higher sensitivity and specificity were achieved for MK values in differentiating malignant from benign lesions by both observers as compared to ADC values. Observer 1 obtained a diagnostic accuracy of 85.71% and 80.00% for MK values in his two readings with 0.74 and 0.78 as a cut-off value, respectively, while the sensitivity and specificity for each readings were (85.00 and 80.00)% and (86.66 and 80.00)%, respectively. The diagnostic accuracy, sensitivity and specificity obtained by ADC values were (77.14, 80.00 and 75.00)% and (80.00, 80.00, 80.00)% respectively for both the readings by Observer 1. The cut-off ADC values for two readings were 1.84 and 1.76, respectively.
On the other hand, Observer 2 obtained a diagnostic accuracy of 82.85% for MK and 80.00% for ADC with 0.80 and 1.86 as cutoff values, respectively. The sensitivity and specificity obtained at these cutoff values for MK were 80.00% and 86.66% and for ADC 80.00 and 75.00%, respectively. Diagnostic performance for MK and ADC are shown in Tables 3 and 4, respectively. The ROC curve for each observation is shown in Fig. 3.
Receiver operating characteristic (ROC) curve of the mean kurtosis (a) and ADC (b) value used for differentiating benign from malignant pulmonary nodules. The area under curve (AUC) for each observation by observer 1’s first reading (Obs. 1a) is shown with blue line; the second reading (obs. 1b) with green line and AUC by observer 2 (obs. 2) is shown with yellow line. Diagnostic Performance of MK value for differentiation of malignancies from benign pulmonary nodules. Note: Obs. 1a = first reading by observer 1; Obs. 1b = Second reading by observer 1; Obs. 2 = reading by observer 2; AUC = area under curve; FP = false-positive; FN = false-negative; NPV = negative predictive value; PPV = positive predictive value. Diagnostic Performance of ADC values for differentiation of malignancies from benign pulmonary nodules. Note: Obs. 1a = first reading by observer 1; Obs. 1b = Second reading by observer 1; Obs. 2 = reading by observer 2; AUC = area under curve; FP = false-positive; FN = false-negative; NPV = negative predictive value; PPV = positive predictive value.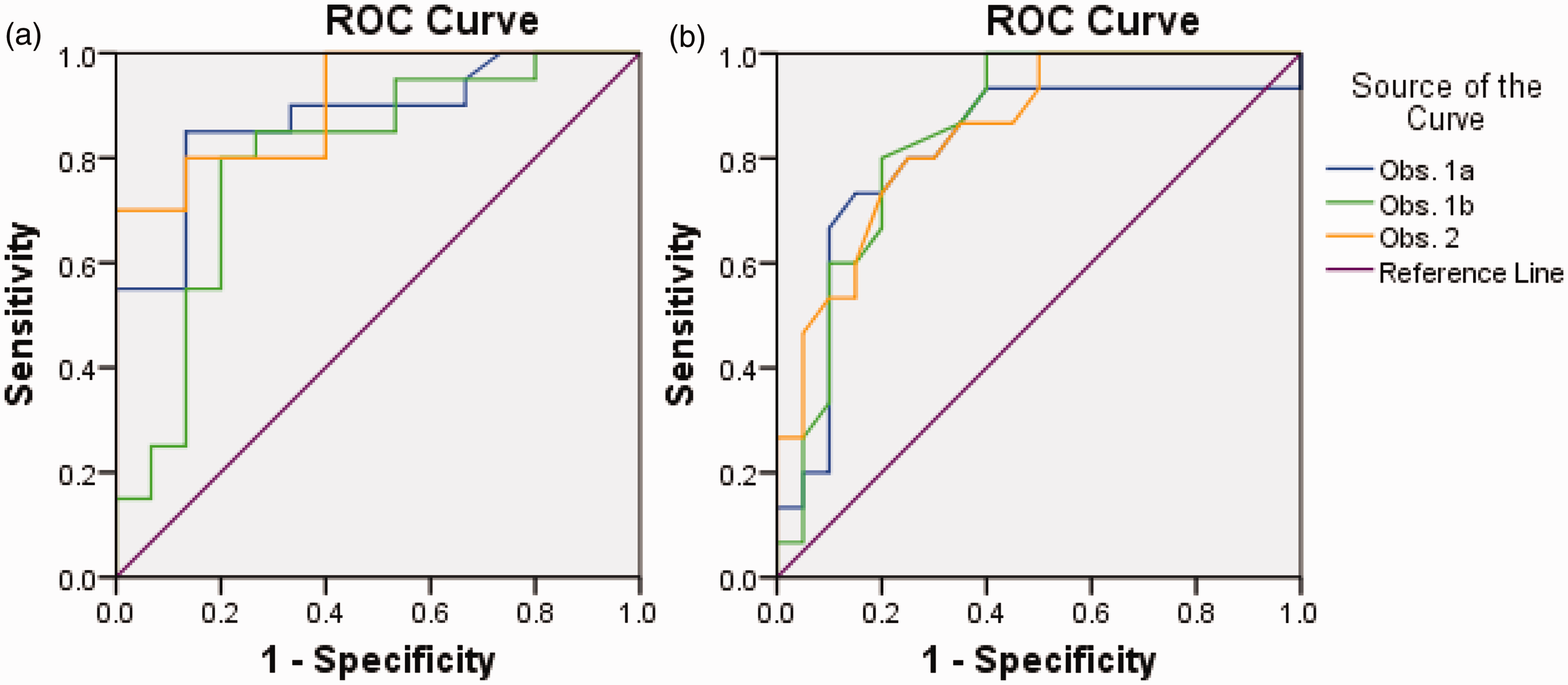


Intra- and inter-observer repeatability
Intra-observer agreement between the two readings for malignant and benign lesions were substantial (ICC = 0.76 and 0.72, respectively) for MK, whereas for the ADC, ICC was substantial for malignant lesions (0.75) and excellent for benign lesions (0.81) (Table 1). Inter-observer agreement between the two observers was also found to be substantial for both malignant and benign lesions (ICC = 0.87 and 0.86, respectively) for MK. Concerning ADC, ICC was substantial for malignant lesions (0.79) and excellent for benign lesions (0.85) (Table 2). The results of the Bland–Altman analysis for the inter- and intra-observer measurements are shown in Fig. 4.
Bland–Altman analysis of the difference between the repeated measurements of the two observers. Observer 1’s first reading versus second reading for malignant lesions for MK (a) and ADC (e); for benign lesions for MK (b) and ADC (f); Observer 1’s first reading versus reading by Observer 2 for malignant lesions for MK (c) and ADC (g); for benign lesions for MK (d) and ADC (h).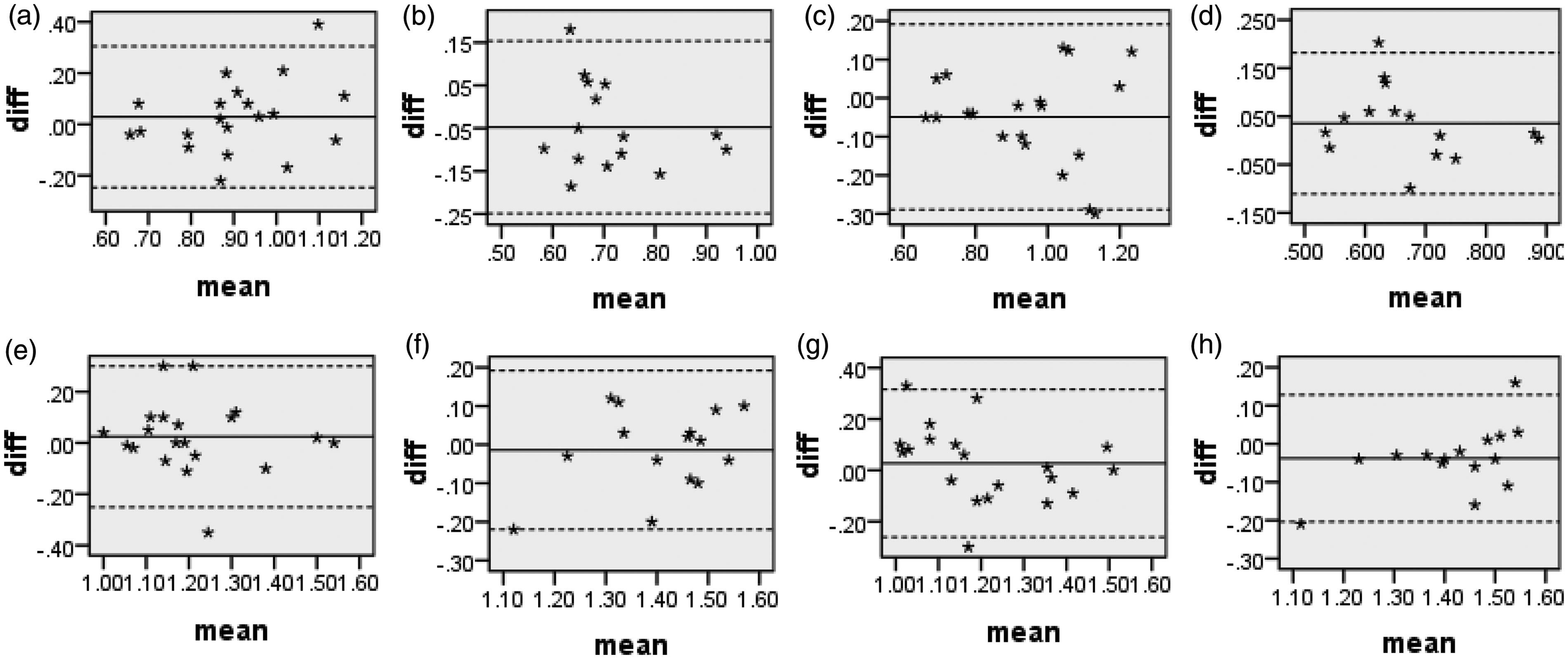
Discussion
The results of this study confirm that DKI of the human lung is technically feasible in clinical routine. The MK values derived from DKI were significantly higher in malignant lesions, which are indicative of higher non-Gaussian diffusion, i.e. higher cellular complexity, than in benign lesions as theoretically expected. Furthermore, the intra- and inter-observer agreement between the readings were excellent to substantial. However, compared with the conventional ADC obtained from a standard DWI protocol, no statistically significant differences were observed for the diagnostic accuracy of MK values derived from DKI. The area under curve for each reading obtained by MK (0.87, 0.80, 0.91) was not significantly higher than compared to those obtained by ADC (0.81, 0.85, 0.85). Therefore, although DKI is feasible in lungs and the MK value has shown promising results in this study, future studies with large population sets, comparing DKI with DWI are required to further validate its application in lung imaging.
Although at present, dynamic contrast-enhanced MRI (DCE-MRI) are the preferred imaging modality to evaluate pulmonary nodules, it is difficult, if not impossible, to distinguish the enhancing benign tumors from malignant carcinomas unambiguously based on the contrast enhancement patterns and morphologic features alone (14). Nonetheless, diffusion MRI could complement DCE-MRI in these circumstances. In contrast, diffusion imaging does not require contrast agent administration therefore making it more suitable for multiple longitudinal follow-up studies monitoring tumor growth and response to therapy. However, so far, only few studies have used conventional DWI for quantitative assessments of lung tumors and the results are inconsistent (15–20). While most studies report higher diagnostic accuracy up to over 80% (16,17), few studies also achieved diagnostic accuracy of either below 80% (18–20) or were even unable to differentiate lung cancers from benign lesions (15). In addition, the cutoff values of the ADCs in these studies varied largely from 0.834 × 10−3 to 1.4 × 10−3 mm2/s (15–20). The diagnostic accuracy in the present study is consistent with other DWI studies (18–20). Moreover, the ADC values are within the range obtained so far by other studies. However, only Ohba et al. (21) had used 3T MRI and the ADC values reported in their study was slightly higher compared to the present study. Moreover, they reported that the ADC values on 3T DWI tended to be higher than those on a 1.5-T DWI. The reason for this discrepancy between their and the present study might be variance in pathological characteristics of the lesions included in the study, as well as the differences in the DWI protocol used. For instance, low b values of less than 600 s/mm2, have been reported to be affected by perfusion effects (15), while on the other hand higher b values, increases the chance of distortion and susceptibility artifacts (22). Therefore, in the present study the chosen b value was 800 s/mm2. However, another value might be more appropriate than this and is yet to be investigated. Another reason for this discrepancy might be inability to measure ADC values of lesions located adjacent to air-containing organs because of susceptibility artifacts. Moreover, SPNs sometimes contain air, which limits the exact ADC estimation (23). In addition, Bernardin et al. (24) reported that the reproducibility of ADC in lesions <2.0 cm was relatively poor. All these aspects might have affected the results in the current study as well.
On the other hand, DKI has not been used so far in lung imaging to characterize pulmonary nodules. Although, in the present study, the MK values did not obtain significant diagnostic accuracy, they were slightly on the higher side compared to ADC values in differentiating pulmonary nodules suggesting that DKI might be potentially a promising quantitative technique for improved characterization and evaluation of lung tumor lesions, however, needs further evaluation.
In this study, respiratory gated mechanism was utilized and not breath-hold techniques as respiratory-triggered diffusion-weighted MRI (DW-MRI) affords better imaging quality than breath-hold DW-MRI and is as effective as breath-hold DW-MRI in preventing misregistration (25).
Although a maximum b-value of 2000–2500 s/mm2 is suggested in DKI studies of the brain, the use of such high b-values in other regions than the brain, is limited by SNR and faster signal decay of the transverse relaxation in these tissues. The lower sensitivity of flexible surface coils compared with head coils leads to lower SNR in tissues while the lower T2 transverse relaxation time of these tissues leads to a faster signal decay of the transverse relaxation (26). Moreover, previous studies implementing DKI on the organs other than brain, such as kidney, prostrate, neck region, etc. found maximum b-values of 600–1500 s/mm2 to be sufficient for DKI parameter estimation (27–29). Accordingly, in the present study, a maximum b-value of 1000 s/mm2 was used as a compromise between appropriate SNR and quantification accuracy of DKI parameters. Furthermore, a relatively high SENSE parallel imaging factor providing a short echo time (72.8 ms) and higher repetition time (8000 ms) was used to increase the SNR.
Several potential limitations exist in the current study. First, the findings in the current study were preliminary. A further multicenter study with a larger cohort is necessary. Second, avoiding susceptibility artifacts on DWI of pulmonary nodules are difficult. In spite of using respiratory gating artifacts due to respiratory and cardiac motion could not be avoided completely. Third, the rim of the lesion with central necrosis may be too thin for a correct ROI placement. Another limitation is the usage of higher slice thickness (6.0 mm) for the DKI measurements in order to achieve adequate SNR.
In conclusion, DKI of human lungs is feasible. DKI can improve tissue characterization of pulmonary nodules and increase diagnostic confidence of differentiation between malignant and benign lesions as compared to conventional ADC. However, further studies with larger sample sizes are warranted to explore the full potential of DKI for non-invasive imaging of human lungs lesions in clinical settings.
Footnotes
Acknowledgments
We thank Morgan A McClure, a medical editor at North Sichuan Medical College, for English grammar correction and revision.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.