
Abstract
Background
Identification of clinical features to determine the aggressive potential of tumors is highly warranted to stratify patients for adequate treatment. Computed tomography (CT) imaging features of clear cell renal cell carcinoma (ccRCC) may contribute to personalized risk assessment.
Purpose
To assess the correlation between CT imaging features and Fuhrman grade of ccRCC, and to identify the predictors of high Fuhrman grade in conjunction with tumor size.
Material and Methods
CT scans of 169 patients with 173 pathologically proven ccRCCs were retrospectively reviewed in consensus by two radiologists for the presence of intratumoral necrosis and intratumoral cyst and tumor size. Histologic grade was classified as either low (Fuhrman grade I or II) or high (Fuhrman grade III or IV). Statistical significance was evaluated by using univariate, multivariate regression, receiver operating characteristic (ROC) curve, and Spearman correlation analyses.
Results
On CT, 20 of the 173 tumors had intratumoral cysts, 60 had intratumoral necrosis, and 93 showed entirely solid tumors. The odds of high grade were higher with intratumoral necrosis and entirely solid tumor than with intratumoral cyst (P < 0.03). Intratumoral necrosis showed a significantly high odds ratio of 25.73 for high Fuhrman grade. The ROC curve showed a threshold tumor size of 36 mm to predict high Fuhrman grade for overall tumors (area under the ROC curve, 0.70). In ccRCCs with intratumoral necrosis or cyst, tumor size did not significantly correlate with Fuhrman grade.
Conclusion
Intratumoral necrosis on CT was a strong and independent predictor of biologically aggressive ccRCCs, irrespective of tumor size.
Introduction
With the widespread use of modern imaging modalities such as ultrasonography, computed tomography (CT), or magnetic resonance imaging (MRI), an increasing number of renal masses have been detected incidentally (1). Most of these incidentally detected renal masses are renal cell carcinoma (RCC), with clear cell renal cell carcinoma (ccRCC) being the most common histologic subtype of RCC. In general, most small RCCs are asymptomatic and have a slow growth rate and low metastatic potential. The peak incidence occurs in patients older than 70 years who have multiple co-morbidities (2). Thus, currently, nephron-sparing surgery has become the gold standard treatment of RCCs smaller than 4 cm, and attention has been given to minimally invasive techniques such as radio frequency thermal ablation or cryotherapy for managing small RCCs (2,3). Moreover, some studies even raised the question about an active surveillance, or “watchful waiting,” for selective patients who have extensive co-morbidities or are unwilling to undergo surgery (4,5). However, small RCCs can show biologic aggressiveness such as distant metastasis or tumor invasion of perirenal fat, and the rate of distant metastasis in T1a RCC was reported to be up to 7% (4,6). Therefore, to stratify patients for adequate treatment without the risk of undertreatment, identification of clinical features to determine the aggressive potential of RCCs is highly warranted.
The important prognostic factors of RCC include tumor subtype, TNM stage, nuclear grade, and the presence of a sarcomatoid component (7). Among these prognostic factors, nuclear grade is an important independent predictive factor of disease-specific survival in patients with RCC (8). Radiological imaging features such as cystic and necrotic appearance in RCC may help predict Fuhrman grade. Previous studies demonstrated that a cystic feature of RCC suggests a favorable histology (9–11), whereas necrosis of ccRCC correlated with an aggressive histology (12). In addition, in RCC cases, the risk of high grade tumors usually increases with tumor size (13,14). However, Hsu et al. (15) reported that RCCs of up to 3 cm in size showed a significant incidence of high nuclear grade and did not differ statistically from larger tumors (3–5 cm) with regard to nuclear grade. To the best of our knowledge, only one study has investigated tumor size and radiological imaging features simultaneously for predicting the biologic aggressiveness of ccRCC (16).
The aim of this study was to evaluate the correlation between CT imaging variables, including tumor size and imaging features, and Fuhrman grade of ccRCCs and to identify which variables are independent predictors of high grade tumor.
Material and Methods
Patients
This single-institution retrospective study was approved by the institutional review board and informed consent was waived. A computerized medical database was searched at our institution with the following eligibility criteria: patients who underwent radical or partial nephrectomy due to renal tumor at our institution between January 2005 and May 2013; renal tumor pathologically confirmed as ccRCC; and patients who underwent preoperative CT scan. This process identified 173 patients with 177 ccRCCs. Four patients with four ccRCCs were excluded because Fuhrman grade was not available in the pathologic report. Finally, 169 patients (132 men, 37 women) with 173 pathologically proved ccRCCs were included in our study.
CT imaging technique
The patients underwent contrast-enhanced multidetector CT for the characterization and pretreatment staging of RCC. CT images were obtained with various CT scanners at our institution (Somatom Volume Zoom, Siemens Healthcare, Forchheim, Germany, or Brilliance 64, Philips Healthcare, Amsterdam, The Netherlands). The most frequently used scanning parameters were as follows: tube voltage, 120 kVp; effective tube current, 300 mAs; section thickness, 5 mm; pitch and speed, 0.891:1; rotation time, 0.75 s; and collimation, 64 × 0.625 mm for 64-channel MDCT. After acquisition of a simple unenhanced scan, 2-mL/kg non-ionic contrast material containing 300–350 mg/mL of iodine (iomeprol [Iomeron 300, Bracco Altana Pharma, Konstanz, Germany], iopamidol [Pamiray 300, Dongkook Pharmaceutical, Seoul, Republic of Korea], or iobitridol [Xenetix 300, Guerbet, Villepinte, France]) was intravenously administered at a rate of 3.0 mL/s by using a standard power injector. In addition to unenhanced scan, all patients underwent two-phase and three-phase studies with various combinations of corticomedullary, nephrographic, and excretory phases. A total of 119 patients underwent three-phase studies, while 50 patients underwent two-phase studies. Corticomedullary, nephrographic, and excretory phases began at 30–40, 90–110, and 300 s after contrast injection, respectively.
Image analysis
Review of all images was performed at a picture archiving and communication system workstation monitor (INFINITT PACS, INFINITT Healthcare, Seoul, Republic of Korea) by two radiologists (DJS and SO, with 16 and 3 years of experience, respectively, in interpreting genitourinary images). The reviewers knew the diagnosis of RCC but were blinded to the Fuhrman grade. Before interpreting the images, both radiologists set the criteria for the interpretation of the CT examination results to determine the presence of necrosis, cyst, and entirely solid components in the tumor. Intratumoral necrosis was defined as a non-enhancing, low-attenuating lesions of less than 20 HU on unenhanced scans with ill-defined or irregular margins (Fig. 1). Intratumoral cyst was defined as a non-enhancing, low-attenuating lesion of less than 20 HU on unenhanced scans with well-circumscribed and round or ovoid margins (Fig. 2). Enhancement was defined as an increase in attenuation of more than 20 HU within a region of interest in the tumor between the attenuation value of the unenhanced scan and the contrast-enhanced scan (17). In cases of tumors with co-existing necrosis and cyst, the tumors were considered having intratumoral necrosis. Entirely solid tumor was defined as a tumor without necrosis or cysts (Fig. 3). Tumor size was determined as the maximal diameter of the whole tumor, including cysts or necrosis when present, on the axial, sagittal, or coronal images.
Fuhrman grade III ccRCC in a 75-year-old man with intratumoral necrosis. (a) On the axial unenhanced CT image, the tumor (arrow) in the left kidney demonstrates lower attenuation than the adjacent renal parenchyma. (b, c) The tumor (arrow) shows non-enhancing, low-attenuating lesions with ill-defined margins on axial corticomedullary and excretory phase CT images. (d) The tumor is pathologically confirmed as Fuhrman grade III ccRCC with yellowish intratumoral necrosis. Fuhrman grade II ccRCC in a 38-year-old man with intratumoral cyst. (a) On axial unenhanced CT image, the tumor (arrow) in the left kidney demonstrates lower attenuation than the adjacent renal parenchyma with septation. (b, c) The tumor (arrow) shows non-enhancing, round or ovoid, low-attenuating lesions with well-circumscribed margins on axial corticomedullary and excretory phase CT images. (d) The tumor is pathologically confirmed as Fuhrman grade II ccRCC with multilocular cysts. Fuhrman grade II ccRCC in a 67-year-old woman with entirely solid tumor. (a) On axial unenhanced CT image, an exophytic iso-attenuating mass (arrow) can be observed in the left kidney. (b, c) The tumor (arrow) shows relatively homogeneous enhancement on axial corticomedullary and excretory phase CT images. No low-attenuating lesion can be observed, suggesting the absence of necrosis or cyst in the tumor. (d) The tumor is pathologically confirmed as Fuhrman grade II ccRCC with entirely solid tumor.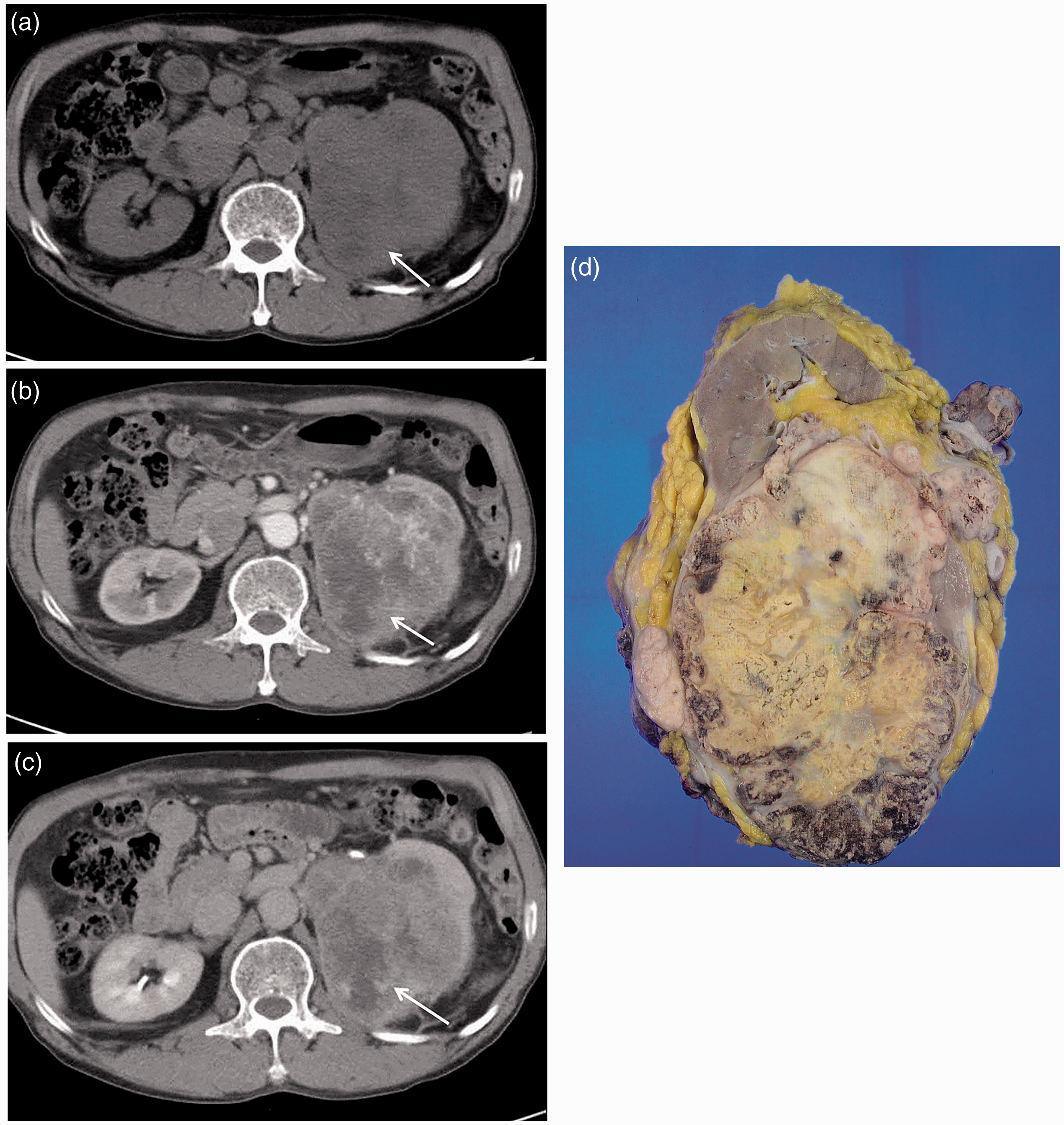


Statistical analysis
We evaluated any statistical differences in sex, age, tumor size, and CT imaging features according to the Fuhrman grade of ccRCCs. Then, all the lesions were subclassified into two groups, namely low grade (grades I and II) and high grade (grades III and IV), according to a previous report that suggested a significant difference in survival rate between these two groups (18).
Continuous variables were described in terms of median and range, and the Mann–Whitney U test was applied for explorative univariate statistics. Moreover, multiple logistic regression analysis using a backward selection method was performed to account for possible interrelationships between variables and to isolate variables with significant and independent influence on histologic grade. We calculated odds ratio (OR), 95% confidence interval (CI), and P value. The receiver operating characteristic (ROC) curve was fit to determine the cutoff tumor size in the prediction of high Fuhrman grade. Multivariate logistic regression analysis was used to confirm the significance of the cutoff value and the independent variables that would suggest high Fuhrman grade. The Spearman correlation analysis with two-tailed testing of significance was performed in each group classified according to CT imaging features in order to determine whether tumor size correlated with Fuhrman grade. Statistical analysis was performed by using IBM SPSS Statistics version 20.0 for Windows (IBM Corp., Armonk, NY, USA). A P value of less than 0.05 was considered statistically significant.
Results
Clinicopathological characteristics of the enrolled patients.
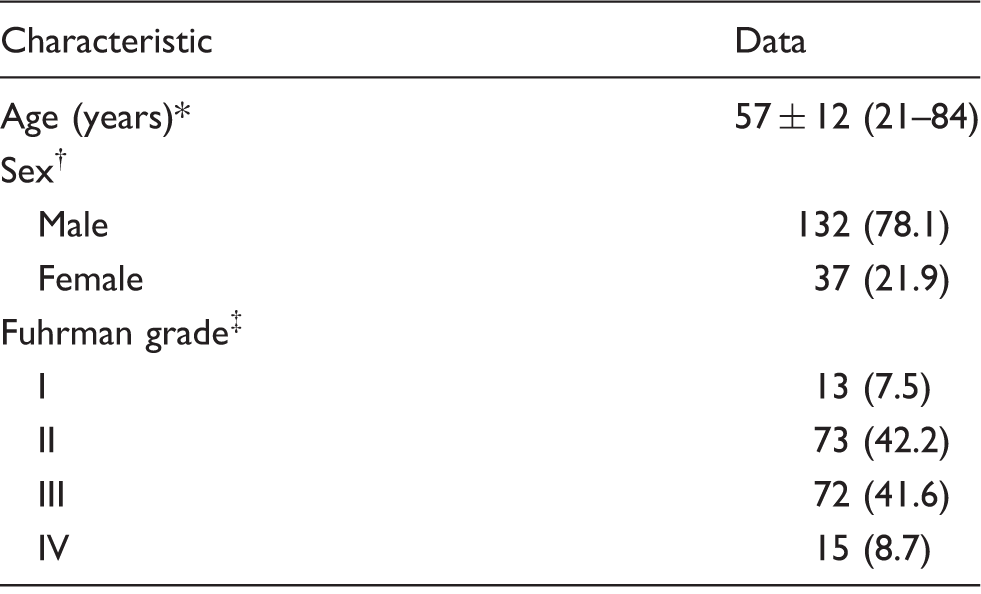
The data are presented as mean (range) values.
The data are presented as number (percentage) of patients.
The data are presented as number (percentage) of tumors.
Clinical characteristics of the enrolled patients according to histologic grade.
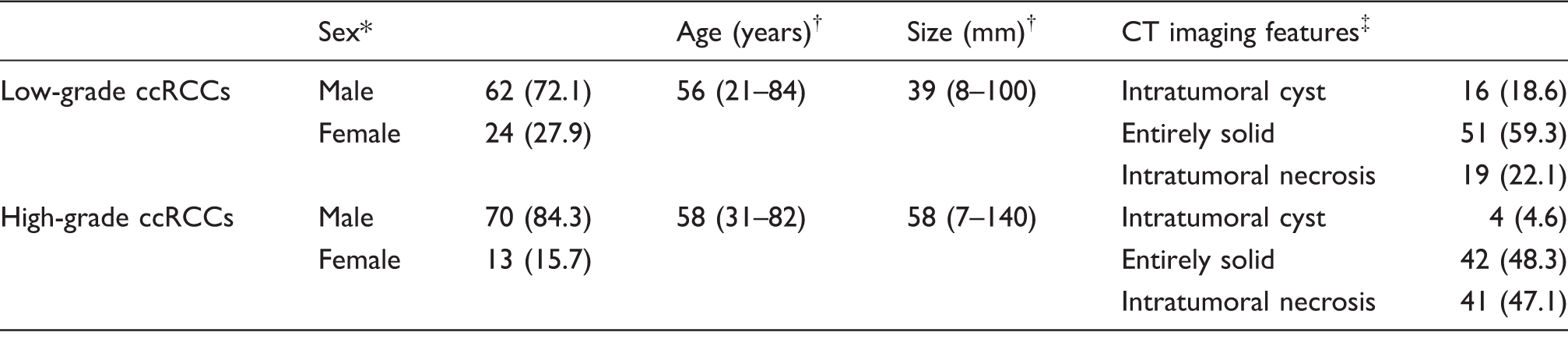
The data are presented as number (percentage) of patients.
The data are presented as mean (range) values.
The data are presented as number (percentage) of tumors.
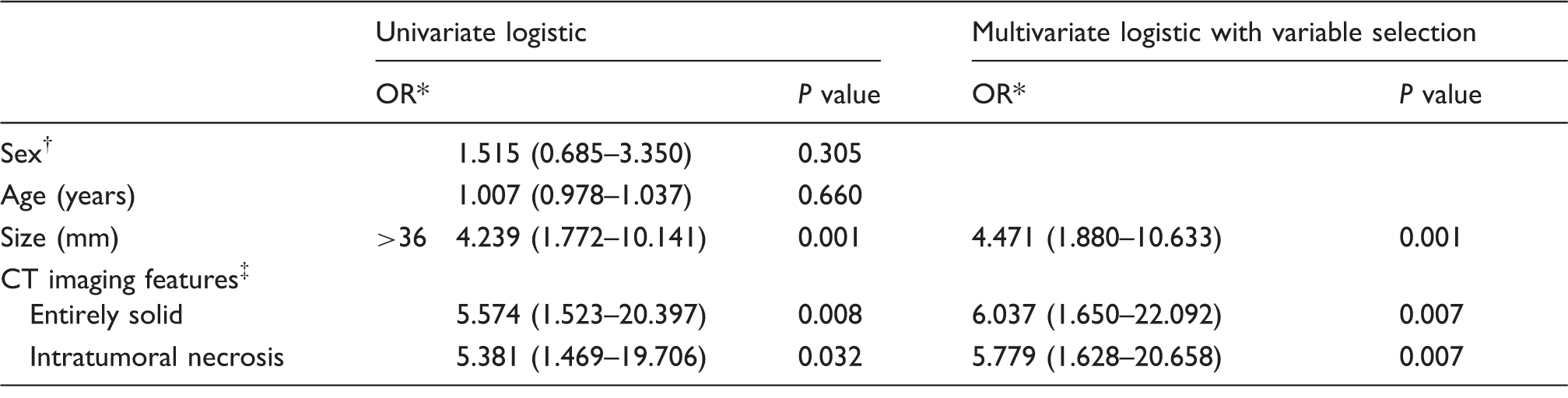
Results of the multivariate logistic regression analysis with backward selection of independent variables predictive of high Fuhrman grade.
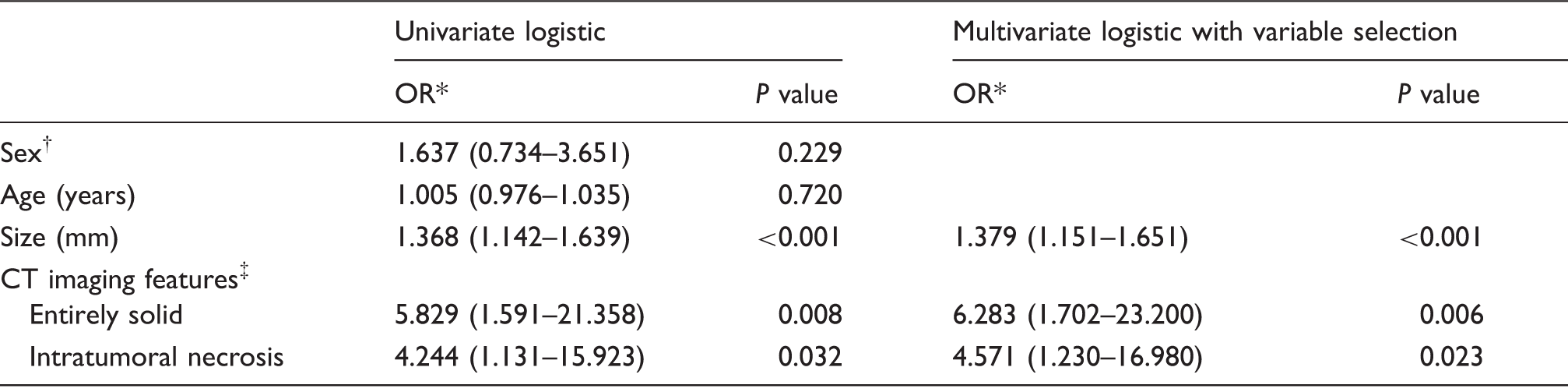
The values in the parentheses are 95% CI.
Female sex established as standard.
Tumors with intratumoral cyst established as standard.
Results of the multivariate logistic regression analysis with backward selection of independent variables predictive of high Fuhrman grade, including cutoff tumor size.
The values in the parentheses are 95% CI.
Female sex established as standard.
Intratumoral cyst established as standard.
Results of the logistic regression analysis, including the interactive term of cutoff tumor size and CT imaging features.
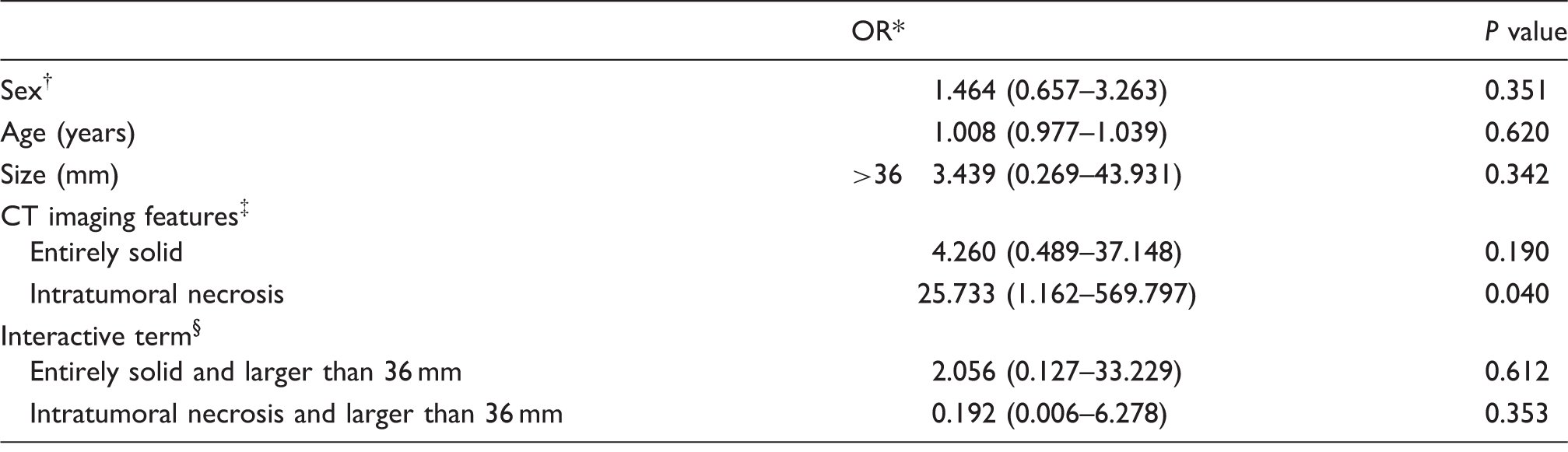
The values in the parentheses are 95% CI.
Female sex established as standard.
Intratumoral cyst established as standard.
Tumors with intratumoral cyst and size smaller than 36 mm established as standard.
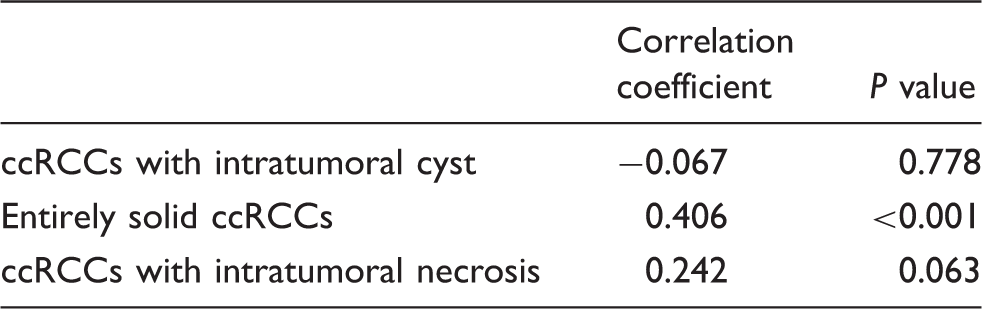
Spearman correlation coefficients between size and Fuhrman grade in each group classified according to CT imaging features.
Discussion
Fuhrman grade is the most popular and widely used system for grading RCC based on nuclear features. The grade is related to the pathologic tumor stage and metastatic potential. Higher Fuhrman grades indicate greater biologic aggressiveness and are associated with decreased disease-specific survival (19). However, because renal mass biopsy is not an accurate evaluation tool for Fuhrman grade (20,21), preoperative recognition of the biologic aggressiveness of RCC is difficult. Thus, our study aimed to determine whether CT imaging features reproducible in routine clinical imaging could predict the biologic behavior of ccRCCs preoperatively. Birnbaum et al. (22) found that homogeneous RCCs were noted to be either grade I or II, and that regions of internal heterogeneity were more prevalent as the histologic grade increased. This heterogeneity could be due to intratumoral necrosis, hemorrhage, fibrosis, and cystic degeneration in high grade tumors. In particular, intratumoral necrosis is associated with tumor aggressiveness, including higher grade and poor survival (23,24). However, low-density cystic features of RCC, which may suggest a favorable histologic profile (9–11), may mimic low-density necrosis on CT. Thus, if the low-density lesion does not obviously correspond to the cyst on CT, MRI can be warranted to confirm the cystic feature or necrosis because of its better contrast resolution.
Rendon et al. (25) reviewed the data of the natural history of small renal masses and concluded that active surveillance is a possible and safe option in patients with short life expectancy. A cutoff size of 4 cm was considered safe, although this has not yet been systematically validated. Tumor size is a major component in TNM staging of RCC and, currently, is the only readily available parameter to predict tumor progression during active surveillance. Tumor size is correlated with Fuhrman grade and larger RCC is associated with a higher risk of high grade tumor (26). In our study, for the overall tumors, tumor size was correlated with Fuhrman grade. However, this correlation was sustained only in ccRCCs that showed entirely solid tumor on CT. No significant correlation was found between tumor size and Fuhrman grade in the ccRCCs that showed intratumoral necrosis or cysts on CT. Ishigami et al. (16) also recently reported similar results as ours, but they did not assess tumor necrosis on CT. In a recent study, Beddy et al. (12) reported that the presence of tumor necrosis in ccRCCs on MRI correlated with aggressive histology, irrespective of tumor size. In agreement with the above-mentioned finding, our study demonstrated that ccRCCs that showed intratumoral necrosis on CT represented higher Fuhrman grade, which did not correlate with tumor size.
Recently, tumor enhancement of ccRCC on CT was investigated to predict Fuhrman grade, and low tumor enhancement was significantly associated with high grade tumors (27). In our study, tumor enhancement characteristics could not be evaluated because CT scans were not performed on the same scanner and the image acquisition protocols used differed. The regional spread of tumor, tumor thrombus in the renal vein and inferior vena cava, involvement of lymph nodes, and presence of distant metastases should be identified on preoperative CT in patients with RCC. These imaging features, which were not assessed in this study, represent advanced clinical stage and are associated with poor outcome. Fuhrman grade is significantly correlated with tumor stage, perirenal fat involvement, lymph node involvement, renal vein involvement, and synchronous metastases (28).
There have been some studies using MRI parameters for assessment of RCC tumor grade (29–31). High grade RCCs showed higher tumor perfusion and lower apparent diffusion coefficient values than low grade RCCs (29,30). Rheinheimer et al. (31) found a weak correlation between tumor grade and perfusion fraction f and perfusion-free diffusion coefficient D using intravoxel incoherent motion-derived parameters. However, these studies were performed including a limited number of patients (fewer than 26 patients). Furthermore, different scanners, different imaging protocols, and pharmacokinetic models can cause the inconsistency in quantitative MRI parameters. The analysis of tumor imaging features may be feasible in predicting tumor grade. In a recent study by Doshi et al. (32), cystic RCCs with T1 hypointensity were associated with less aggressive pathologic features.
To date, an active surveillance protocol has not been established for patients with RCCs. Some nomograms to predict the biologic aggressiveness of RCC, which produce results based on tumor size, sex, age, and symptoms at presentation, have been performed with limited ability (33,34). Nomograms obtained by using quantification of renal tumor anatomy, namely the RENAL nephrometry score, may be useful to predict high grade RCC (35,36). However, as far as we know, a nomogram incorporating imaging features of RCC that can predict the likelihood of indolent or potentially aggressive nature has not been developed yet. Integration of CT imaging features such as intratumoral necrosis or cyst in a predictive model may be useful in risk stratification in patients with RCC. Further studies are necessary to support the ability of an imaging-directed nomogram to predict potentially aggressive ccRCC.
This study had several limitations. First, the CT findings were not correlated with histopathologic findings except Fuhrman grade of ccRCC. Prospective studies with histopathologic correlation are needed to validate our results. Second, Fuhrman grade was obtained from pathologic reports only and was not reviewed again by a single pathologist. Third, only ccRCCs were assessed and other RCC subtypes were not included. Most investigators have affirmed the prognostic validity of nuclear grading for ccRCC, but not for papillary and chromophobe RCCs (37,38). Fourth, this was a retrospective study conducted by consensus reading at a single institution, and the results might have been influenced by selection bias and inter-observer variability. Finally, as mentioned earlier, CT scans were obtained by using different protocols on different scanners.
In conclusion, irrespective of tumor size, intratumoral necrosis on CT was a strong and independent predictor of aggressive biologic activity in patients with ccRCC. Cystic features, on the other hand, reflected a lower malignant potential. These imaging features may help to select adequate treatment strategies, and active treatment, in particular, could be considered regardless of tumor size in patients with ccRCC demonstrating intratumoral necrosis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.