
Abstract
Sacrococcygeal teratomas are the most common solid tumor in newborn infants. The diagnosis is not difficult in many cases; however, there should be additional information on imaging studies in order to manage those infants properly. Details include histology, morphologic classification, complications such as rupture, bleeding, and mass effects on the adjacent structures. Although imaging features cannot accurately predict the histologic subtypes of the tumors, thorough evaluation of the imaging features can help distinguish malignant tumors from benign tumors. In this article, pathogenesis, histological characteristics, clinical considerations, and morphologic characteristics will be discussed.
Keywords
Introduction
Extragonadal germ cell tumors (GCTs) are defined as GCTs arising outside the testes or the ovaries. Extragonadal GCTs typically develop in midline locations and involvement sites vary with age. In adults, the anterior mediastinum, retroperitoneum, and the pineal and suprasellar regions are most commonly involved. In infants and young children, the most common site is the sacrococcygeal region, which accounts for 40–70% of teratomas (1). Sacrococcygeal teratomas (SCTs) are the most common GCT in neonates occurring in approximately 1 in 27,000 live births (2) with a female prevalence in a 3:1 to 4:1 ratio (3,4). At birth, the great majority of SCTs are benign (2). Benign SCTs can manifest malignant degeneration and malignant transformation can occur in children with advanced age. Approximately 70% of SCTs are malignant at the patient age of nine months (3,5–7). Furthermore, although SCTs are diagnosed as benign tumors, they can recur as malignant SCTs after surgical resection (5,7,8). Therefore, prompt surgical resection is required and imaging studies play an important role in confirming the diagnosis, demonstrating intra-abdominal extension and effects on adjacent structures. In this article, we discuss the pathogenesis, pathologic features, imaging features, complications due to mass effects of the tumor, and clinical management of SCTs.
Pathogenesis
SCTs develop at the base of the coccyx and are thought to be derived from Hensen’s node (primitive knot), a rounded and elevated area at the cranial end of the primitive streak (9–11) (Fig. 1). The primitive streak is a longitudinal ridge of ectodermal cells at the caudal end of the bilaminar embryonic disc. This structure appears at the beginning of the third embryonic week and is formed by proliferation of the ectodermal cells, which move towards the midline of the embryo. The primitive streak consists of totipotent cells, which are able to transform into any type of cells. The primitive streak forms the intra-embryonic mesoderm, septum transversum, and notochord. This structure determines the future craniocaudal axis of the embryo and demarcates the embryo into left and right halves. After formation of the intra-embryonic mesoderm, the primitive streak normally regresses and completely disappears by the end of the fourth week or becomes an insignificant structure in the sacrococcygeal region of the embryo. If totipotent cells of the primitive streak remain after the fourth week, these cells give rise to a SCT (10,12). The degree and type of differentiation of these totipotent cells decide the specific type of tumor (13). Primordial germ cells, which are totipotent cells found in the gonadal ridge of a late embryo, remaining in a primitive undifferentiated state lead to embryonal carcinoma. If differentiation proceeds beyond the embryonal carcinoma stage into a pathway of embryonic structure production, mature or immature teratoma may occur. Differentiation along an extra-embryonic pathway leads to yolk sac tumor or choriocarcinoma (13).
Embryology in development of the caudal region. Drawing of a 16-day embryo (left) shows the primitive streak, which is a longitudinal ridge of ectodermal cells at the caudal end of the bilaminar embryonic disc. Drawing of a 20-day embryo (middle) demonstrates that the primitive streak moves caudally and undergoes regression. Drawing of a four-week embryo (right) shows a regressed primitive streak and Hensen’s node located ventral to the developing sacrum and coccyx.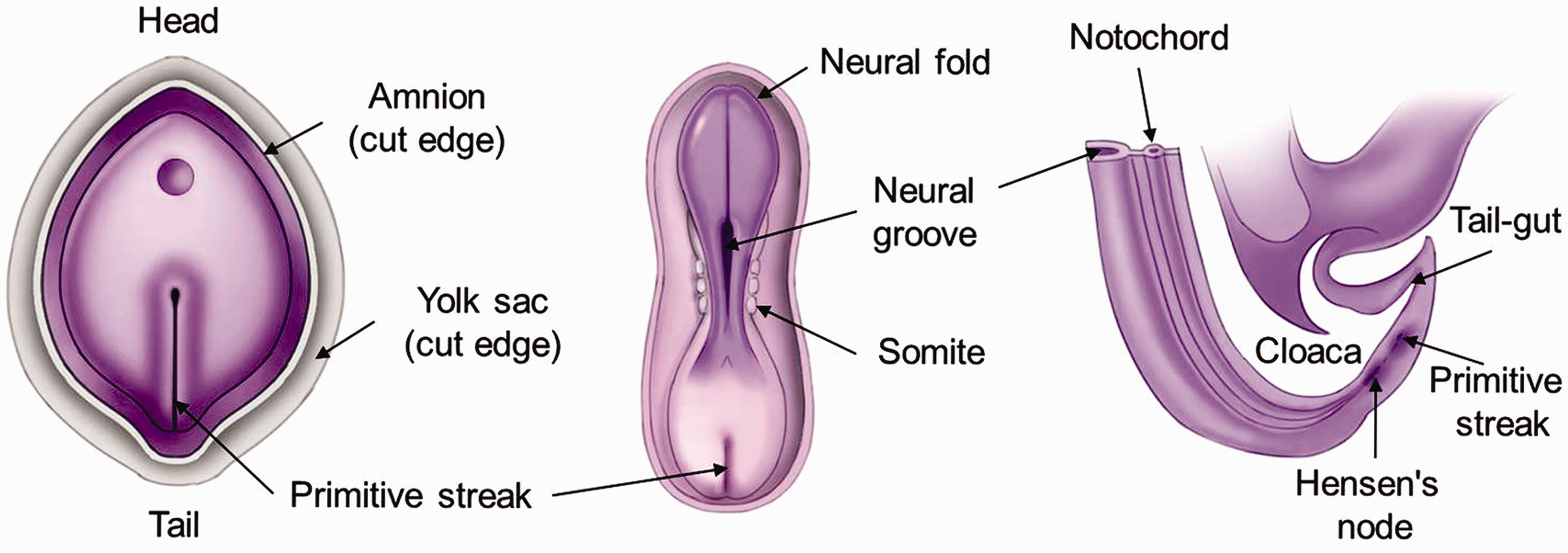
Histologic classification
By definition, teratomas are composed of more than one germ cell layers (ectoderm, mesoderm, and endoderm) (10). SCTs contain a variety of tissues from more than one germ cell layer. SCTs are categorized into three histopathologic types: mature teratomas; immature teratomas; and malignant teratomas (14). Mature SCTs consist of well-differentiated tissues from various somatic sites. These tissues include functional glandular structures such as pancreatic Langerhans cells or sebaceous glands and fully developed bones, hair, and teeth. Immature teratomas have immature embryonic elements or incompletely differentiated tissue foci. A primitive neuroectodermal feature is commonly present. Mature and immature teratomas are considered as benign tumors. SCTs that contain malignant elements are considered to be malignant tumors. The most common malignant elements are yolk sac components. Other malignant elements, such as embryonal carcinoma and primitive neuroectodermal tumors, can be present. It is possible that microfoci of malignant elements may escape being sectioned on pathologic examination. Therefore, very extensive sectioning of the SCT is necessary to avoid missing the presence of malignant components. The majority of SCTs are benign (5,6,15–20). Histologically mature SCT accounts for about 50–60% and immature SCT accounts for about 18–34% of sacrococcygeal GCTs (1,5,8,18,21). Malignant SCTs account for approximately 12–14% of sacrococcygeal GCTs (8,18). There is a grading system for SCTs as follows: grade 0 = tumors contain only mature tissue; grade 1 = tumors contain rare foci of immature tissues; grade 2 = tumors contain moderate amounts of immature tissues; grade 3 = tumors contain large amounts of immature tissue with or without malignant yolk sac elements (22). However, this grading system is not correlated with prognosis, unlike that of the ovarian teratoma. The overall recurrence rate of SCTs is in the range of 11–16.4% (23–25). The recurrence rates of mature teratomas, immature teratomas, and malignant teratomas are 0–26%, 12–55%, and 0–36%, respectively (23–25). Both mature and immature teratomas can undergo malignant transformation (24,26) and malignant teratomas are also prone to benign recurrence (Fig. 2).
Malignant recurrence of a mature teratoma as an endodermal sinus tumor in a female neonate. Initial sagittal T2W imaging (left) shows a presacral mass (type IV) with cystic (arrow) and fat (arrowhead) components within the tumor. The mass was confirmed as a mature teratoma after surgical resection. Sagittal-enhanced CT image (right) obtained two years after mass excision shows a large heterogeneous enhancing mass (asterisk) in the presacral area. Adjacent sacral bone destruction (arrows) and epidural extension (arrow head) are shown.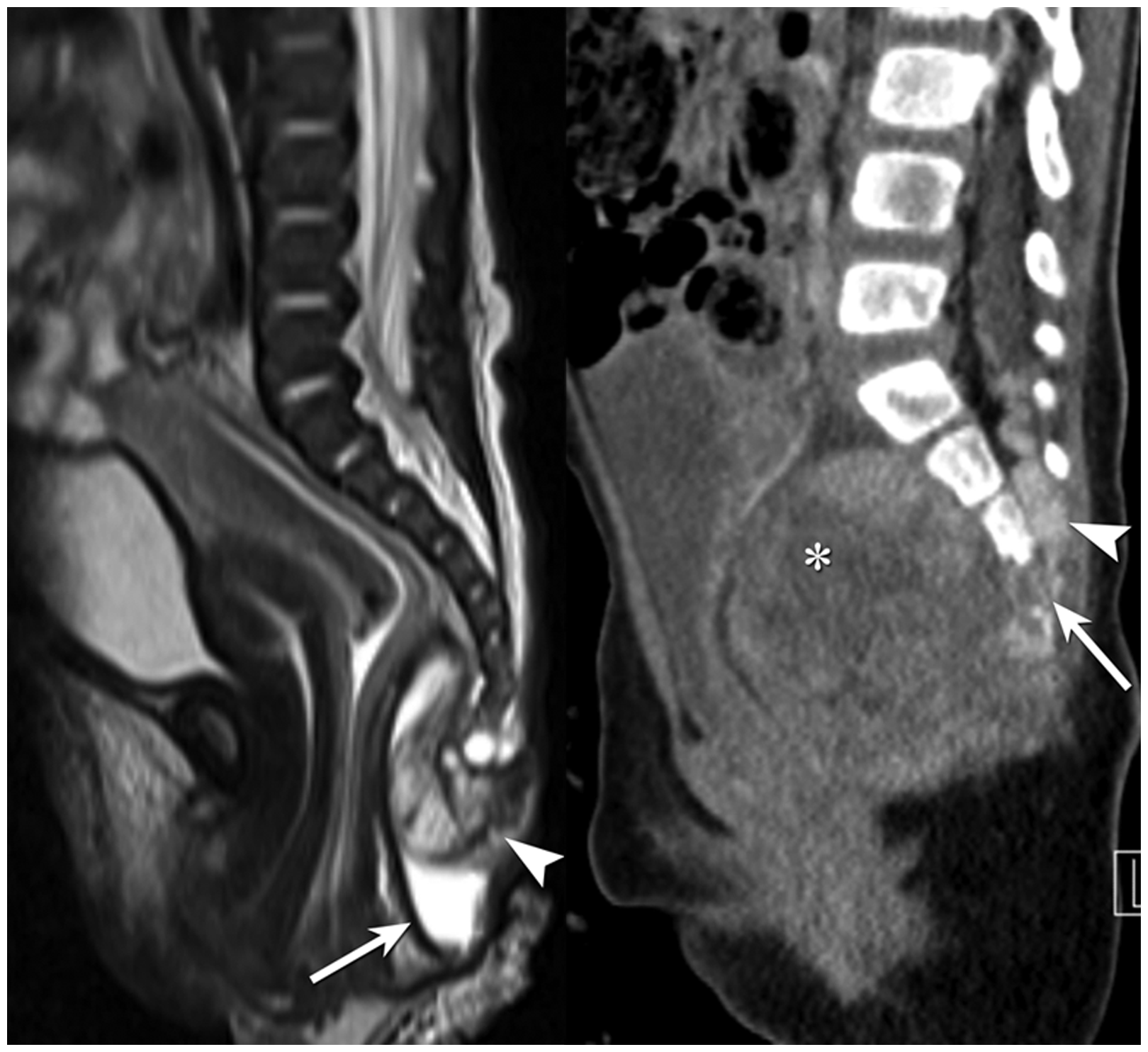
Clinical considerations
SCTs are currently detected by prenatal screening ultrasound (US). When the tumor is too large, dystocia or difficulty in delivery can occur. After birth, the tumor is present as a skin-covered tail mass. If the tumor is quite large, the skin covering the mass can be ulcerated and necrotized. The anus can be displaced anteriorly (Fig. 3). Rectal examination to look for the internal component should be considered. Patients with SCTs can be asymptomatic or have signs of obstruction of the rectum or colon, such as constipation or frequent stools, or obstruction of the bladder neck (27).
Immature SCT in a male neonate. Clinical photograph depicts a large tail mass with swelling of the overlying skin, scrotum, and both thighs. The anal opening, which is anteriorly displaced, is present through the tumor (arrow). The patient suffered from constipation even though the tumor was successfully resected.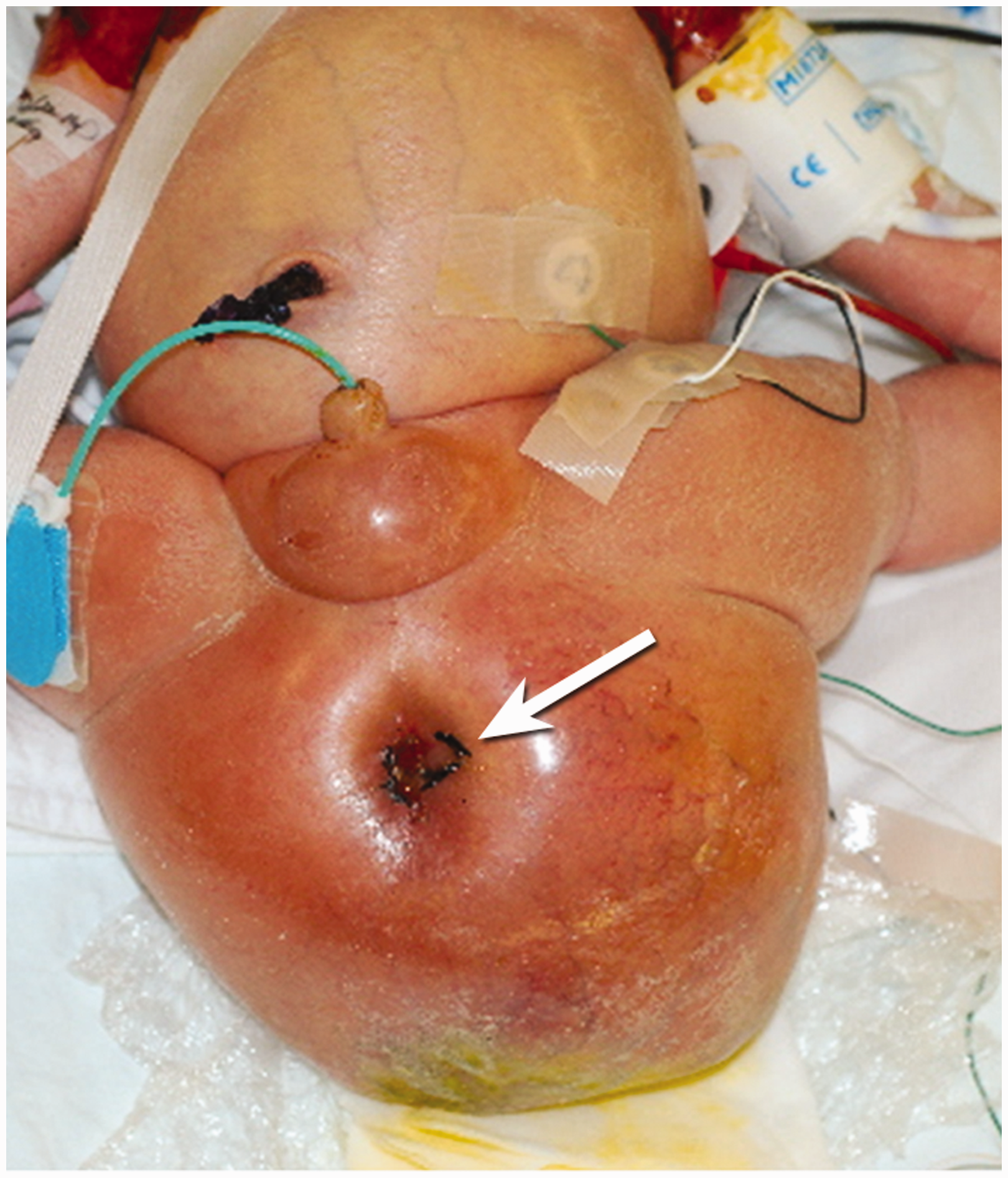
The reported incidence of congenital malformations associated with SCTs is in the range of 5–43% (27–30). The majority of these are anorectal and genital malformations. Other various anomalies have been reported including spinal dysraphism, sacral agenesis, hip dislocation, meningocele, Currarino’s triad (anorectal malformation, sacrococcygeal osseous defect, presacral mass), and vertebral anomalies (10,27,31,32).
Malignant SCTs may have elevated tumor markers (3,19,33). The most commonly produced tumor marker is alpha fetoprotein (AFP) because yolk sac components are the most common malignant elements (3,34,35). Other malignant elements can produce beta human chorionic gonadotropin (beta-hCG). Therefore, serum AFP and beta-hCG levels should be evaluated at the initial diagnostic work-up to look for malignant components and assessed to monitor tumor relapse during the follow-up periods.
SCTs are generally diagnosed at birth or in infancy. Serum AFP level is normally elevated in this period because AFP is produced by the yolk sac, fetal liver, and fetal gastrointestinal tract (36). Therefore, interpretation of an elevated AFP level at birth or in infancy requires careful attention. Normally, elevated serum AFP level decreases and reaches adult level by eight months after birth. Serial follow-up levels should be measured to properly interpret this tumor marker (37).
Morphologic classification
SCTs arise from the base of the coccyx and may continuously grow in the posterior direction forming an external protrusion, or in the anterior direction dissecting and distorting surrounding structures such as the rectum, vagina, and bladder (5,10). Thus, the tumor may have internal and external components. Based on this morphologic characteristic, the American Academy of Pediatrics Surgery Section Survey suggested a classification system, which categorizes SCTs into four types (Fig. 4) (5): type I SCTs are predominantly external with a minimal presacral component; type II SCTs are present externally but have a significant intrapelvic component; type III SCTs have an apparent but small external component with a significant pelvic mass extending into the abdominal cavity; type IV SCTs occupy the presacral area with no external presentation. The most common type of SCT is type I, followed by types II, III, and IV (8). Type IV SCTs are detected later than types I, II, and III because they have no external components. Malignant elements are more frequently observed in types IV SCTs and are lowest in SCTs with a large external component (1,5,21). In order to have accurate communication with surgeons, radiologists should appropriately use the morphologic classification of SCTs when describing the type of mass, because complete resection of the mass is the cornerstone for management of this tumor.
Morphologic classification of SCTs according to the American Academy of Pediatrics Surgery Section Survey. Type I is primarily external in location. Type II has equal amounts of internal and external components with a dumbbell shape. Type III has a small external component and is primarily located within the abdomen and pelvis. Type IV is entirely internal without a visible external component.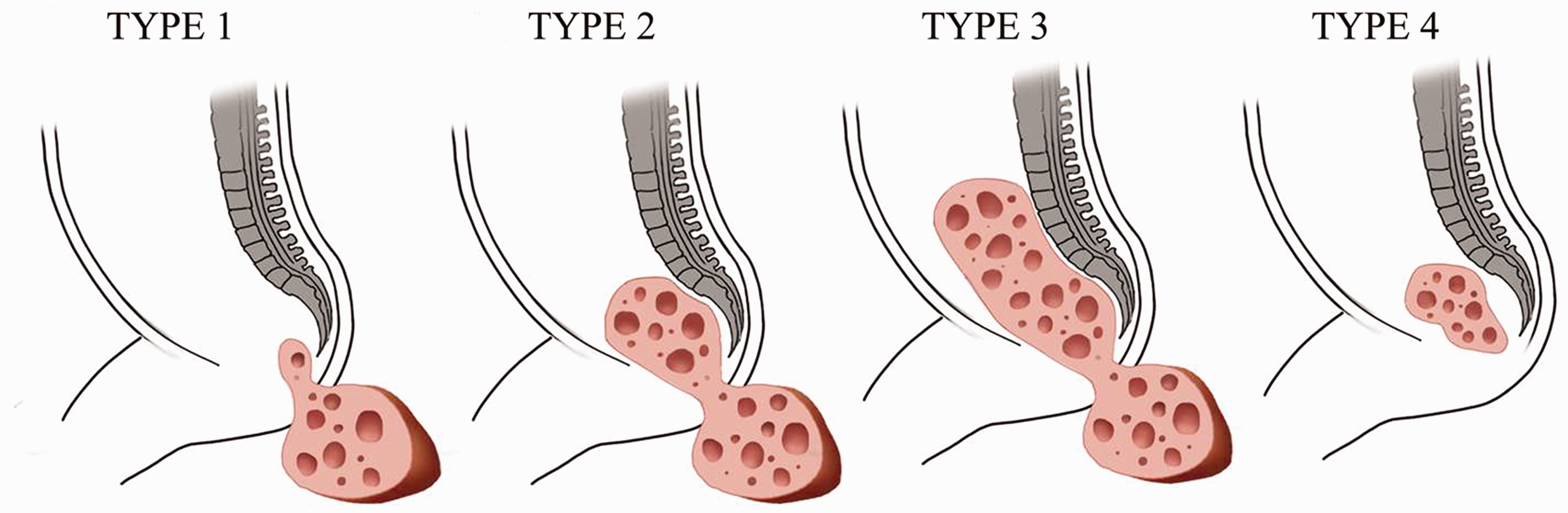
Imaging techniques
Prenatally, most SCTs are diagnosed in utero by US screening. If a SCT is suspected on prenatal US screening, in utero fetal magnetic resonance imaging (MRI) is recommended where available. In utero fetal MRI can depict accurate tumor size and characteristics including intraabdominal extent and effect on adjacent organs (38–40). This additional information provided by in utero fetal MRI can be helpful in prenatal counseling as well as preoperative surgical planning. In case of in utero fetal MRI was not performed, abdominopelvic MRI should be obtained after birth in order to evaluate tumor characteristics and relation with adjacent other structures. US is also frequently performed as a first imaging modality due to easy accessibility and lack of radiation. However, US has intrinsic disadvantage of operator dependency, and MRI is preferred imaging modality. Computed tomography (CT) can be another option for postnatal imaging of SCTs; however, it is not generally used due to exposure to ionizing radiation.
Imaging pattern-based approach for diagnosis of SCT
Sacrococcygeal teratomas consist of variable tissues from all three germ cell layers. Therefore, imaging findings of SCTs are heterogeneous and variable. These tumors may have variable amounts of cystic and solid components. Not infrequently, they may show a combination of both cystic and solid components. Although imaging findings of SCTs cannot predict the histologic subtypes of the tumors, benign SCTs are more likely to have cystic components, calcification, and prominent fat tissue than malignant SCTs. The presence of hemorrhage and/or necrosis within the mass is more likely to be suggestive of malignant SCTs.
Cystic components of SCTs are usually seen in benign tumors (Fig. 5). Mild peripheral rim enhancement along the cystic wall may present after gadolinium contrast material injection. Contents of the cystic component can be variable due to various degrees of fat, hemorrhage, or other materials. Therefore, imaging characteristic of cystic components can be altered according to the internal contents.
Mature SCT in a male neonate. (a, b) Sagittal T2W imaging (a) and gadolinium-enhanced fat saturated T1W imaging (b) show a multiseptated cystic mass (type II) with mild enhancement along the septa and cystic wall. (c) Photomicrograph (hematoxylin and eosin [H&E] stain, ×200) shows most of the tumor consists of mature epithelial tissues (arrow), mesenchymal tissues (arrowhead), and mature neural tissues (asterisk).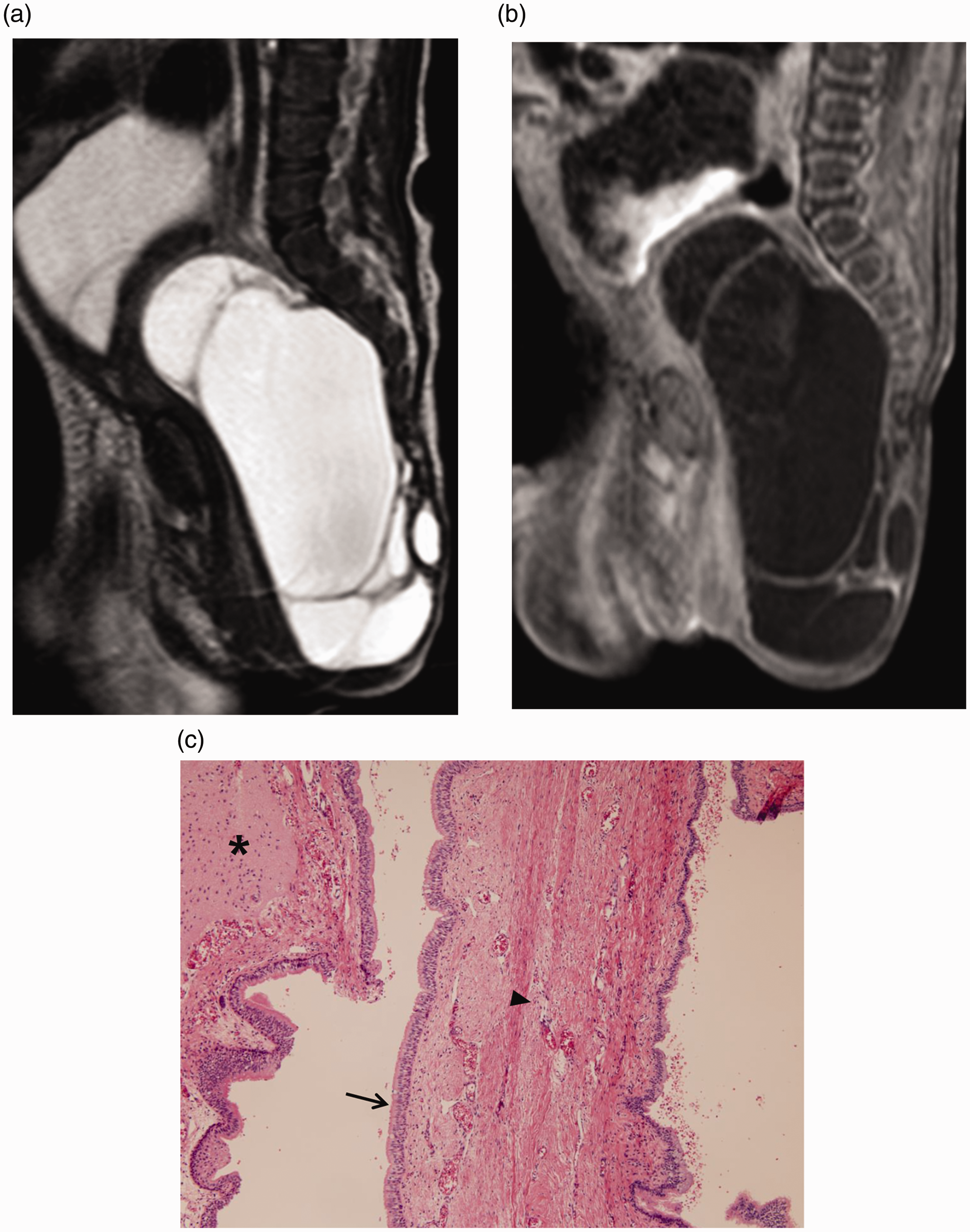
Calcification is frequently seen in benign SCTs but it can be present in case of malignant form (10,13,41). Radiographs can depict calcifications, but CT is the most sensitive imaging modality to demonstrate calcifications. However, considering the ionizing radiation hazard of CT scans in neonates, CT is not routinely used to find calcifications in SCTs.
SCTs with considerable fat components are usually benign (13) (Fig. 6). Distinguishing fat components in SCTs from the normal subcutaneous fat tissue on ultrasound (US) images alone is not easy. CT and MR scans are the best choice for demonstrating fat components, but MRI is superior to CT considering the ionizing radiation hazards of a CT scan.
Mature SCT in a female neonate. (a) Sagittal T2W imaging demonstrates predominantly fatty mass with mostly external location (type I). There are T2 hyperintense cystic components (arrows) with solid components (arrowheads). (b) On photomicrograph (H&E stain, ×0.5), the tumor is mainly composed of mature mesenchymal tissues and there are abundant fat tissues with intervening fibrous septa and mature chondroid tissue (asterisk).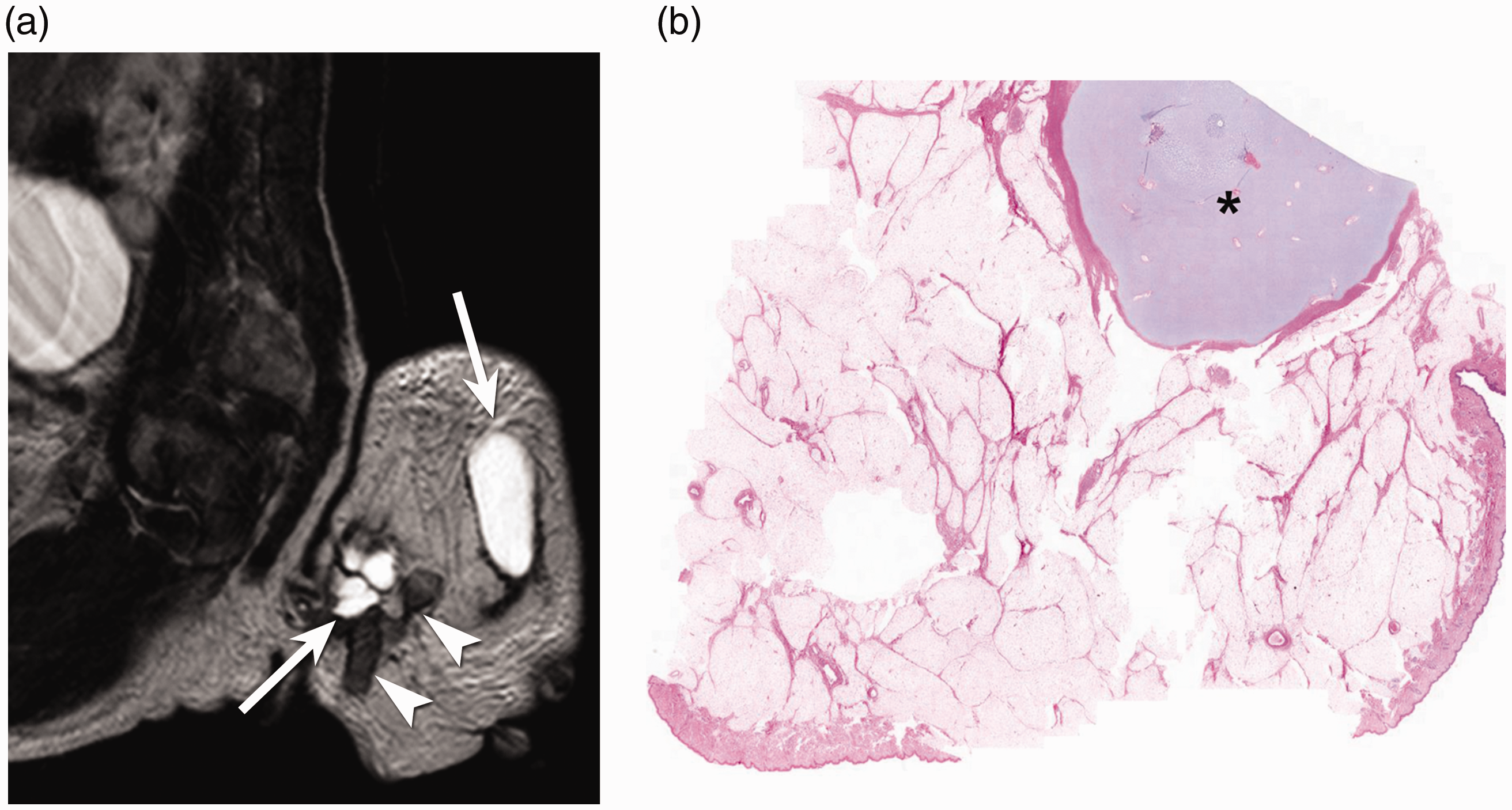
Masses with predominantly solid components are highly suggestive of malignant SCTs (Fig. 7). Solid components are seen as hyperechoic areas by US. CT or MRI plays an important role in demonstrating solid components. On MRI, solid components may show iso- or hyposignal intensity on T1-weighted (T1W) imaging and iso- to high signal intensity on T2-weighted (T2W) imaging. Solid portions show heterogeneous enhancement on CT or MRI after intravenous contrast material injection.
Malignant SCTs in a female neonate. (a) Prenatal Doppler US image at 28 weeks and five days demonstrates a large, predominantly solid sacrococcygeal mass with internal vascularity. (b) Clinical photograph shows massive bleeding and rupture of the mass. Hypovolemic shock with disseminated intravascular coagulation (DIC) was developed in this patient due to bleeding. After surgical resection, the mass was proven as a yolk sac tumor. (c) Axial contrast-enhanced CT image obtained after surgery shows lobular contour with capsular retraction and areas of low attenuation in the liver, suggesting submassive hepatic necrosis after prolonged DIC and hypovolemic shock. (d, e) The tumor was composed of 70% of immature teratomas (d) and 30% of yolk sac tumor (e) with immunopositivity for alpha fetoprotein and spalt like transcription factor 4 (not shown).
A significant amount of hemorrhage and/or necrosis is highly suggestive of malignant SCTs (Fig. 7). Therefore, complex heterogeneous areas appearing in the mass should be carefully evaluated. Sacral bony destruction, invasion of surrounding structures, or metastatic disease are also important clues indicating malignancy.
Differential diagnosis between mature and immature teratomas based on imaging features is limited. Immature teratomas are more likely to be large in volume and show complex cystic and solid masses (Fig. 8). Because SCTs can generally have a variable combination of various tissue components in an individual case, even a malignant SCT can have a large cystic component, calcification, or fat tissue. Radiologists should be aware that prediction of histologic characteristics based on their appearance on imaging studies is limited, and the most important role of imaging is making a diagnosis of a SCT and providing the necessary information for surgical planning. CT and MRI are excellent modalities for depicting tumor extent and those two modalities are complementary to one another. However, MRI is superior to CT imaging in soft tissue characterization.
Immature SCTs in a female neonate. (a) Coronal T2W imaging shows a complex cystic and solid coccygeal mass. (b) There is small amount of hyperintense fluid on T1W imaging, representing hemorrhage. (c) On gadolinium-enhanced coronal T1W imaging, mild enhancement in the solid component and along the cystic wall is noted. (d) Photograph of the cut surface of the mass depicts a solid mass with multiple small cystic portions. (e) Immature neuroepithelial components are frequently observed on the microscopic finding, which is appropriate for immature teratoma, grade III.
Complications
Due to high output cardiac failure resulting from arteriovenous shunting within the tumor and/or anemia due to intratumoral hemorrhage, fetal hydrops can occur (42). Fetal hydrops is known as a prognostic factor for fetuses with SCTs, thus, prenatal careful monitoring is mandatory (42). Hemorrhage or rupture may occur with traumatic delivery because the SCT is a highly vascular tumor (Fig. 7) (10,13).
SCTs are usually large enough to have a significant mass effect on adjacent structures, and the mass effect begins during fetal development. Various co-morbidities due to mass effects such as obstructive hydronephrosis, anterior displacement of the anorectum, bowel distension, hypoplasia of pelvic muscles, mucocolpos or hip dislocation, may be present on imaging studies (10,27,31,32) (Fig. 9). These complications are frequently accompanied by SCTs with significant internal components. Large type II, III, or IV SCTs show anterior displacement of the anus and hypoplastic pelvic floor muscles, and these conditions may result in functional problems such as fecal incontinence or constipation. If internal components of SCTs obstruct the urinary tract during fetal development, obstructive hydronephrosis and urinary bladder outlet obstruction can develop. These conditions may cause neuropathic bladder, ureter obstruction, and vesicoureteral reflux (43). Occasionally, a large SCT may cause abnormal position of the fetus in utero; therefore, hip dislocation may occur. These conditions may be associated with potential long-term sequelae despite successful surgical resection of the primary tumor (44,45). Therefore, radiologists should carefully evaluate the urogenital system, gastrointestinal system (especially the anorectum), and hip and interpret subsidiary imaging findings besides the tumor itself.
Mature SCT in a female neonate. (a) Sagittal T2W imaging shows a large multicystic sacrococcygeal mass with internal and external components. In order to release the urinary obstruction, a Foley catheter was inserted (arrow) in the urinary bladder. (b) Coronal T2W imaging depicts fluid signal intensity mixed with intermediate signal intensity in the dilated vagina (arrow), indicating mucocolpos. (c) Bilateral hydronephrosis (arrows) was noted on an axial T2W imaging. Asterisk indicates the superior portion of the mass. (d) Dislocated bilateral hip joints (arrows) are seen on an axial T2W imaging.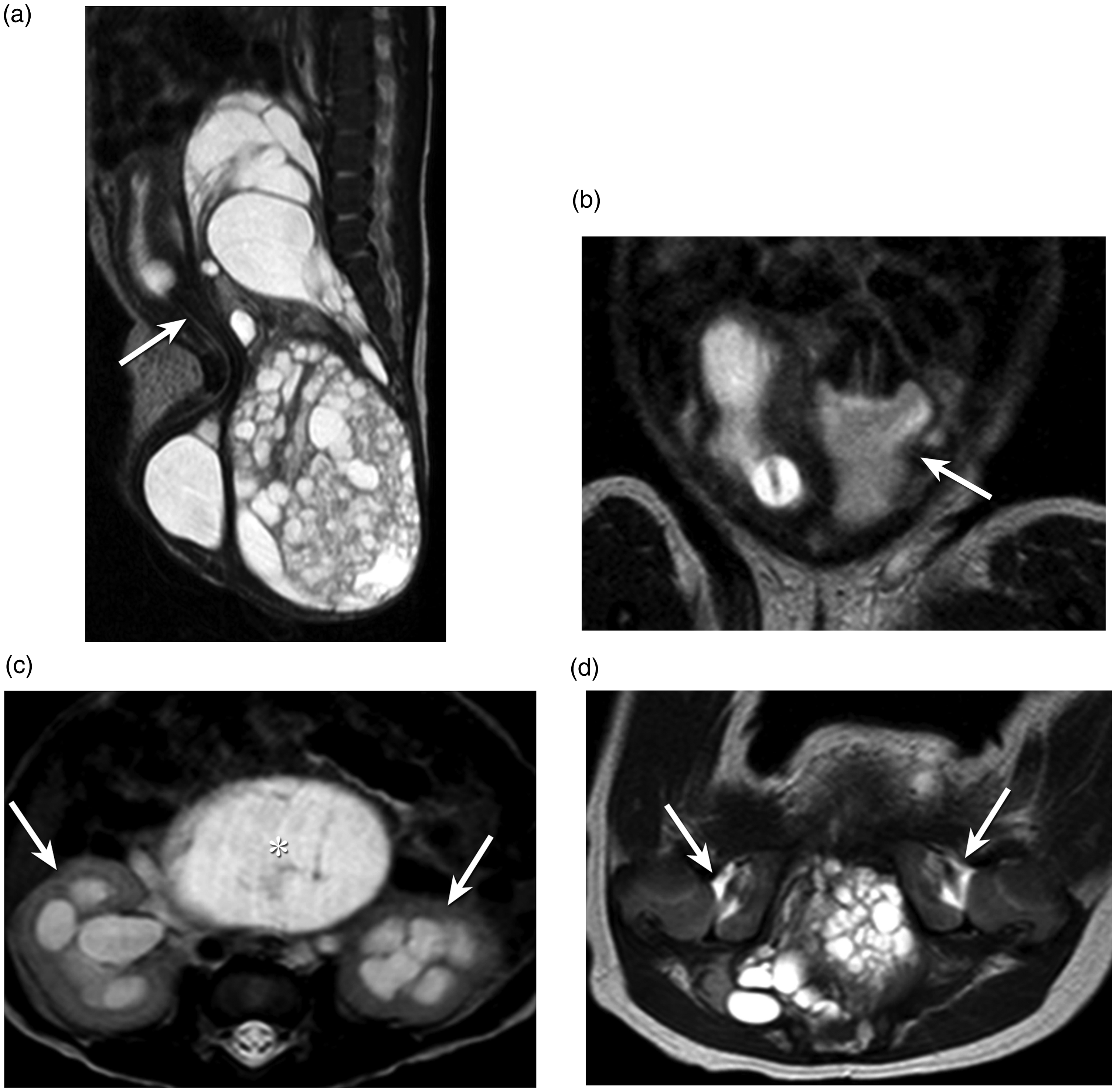
Clinical management
Thanks to advances in prenatal detection of masses and improvement in prenatal intervention, in utero open fetal surgery is a treatment option for some high-risk SCT fetuses. Minimally invasive in utero approaches have been recently introduced to treat fetuses with hydrops. Approaches include laser (46,47) or radiofrequency ablation techniques (48,49), urinary bladder drainage for obstructive uropathy (50,51), and aspiration of cystic components (52) (Fig. 10). Minimally invasive techniques focus on inducing tumor necrosis, which allow the surgeon to perform a lower-segment uterine incision instead of a classic incision during Cesarean delivery.
A case of a SCT treated with prenatal radiofrequency ablation (RFA). Prenatal US at 22 weeks and five days (left) shows a large sacrococcygeal solid and cystic mass. After cystic fluid aspiration with RFA at 26 weeks (right), the cystic portion of the mass disappeared and size of the mass was reduced.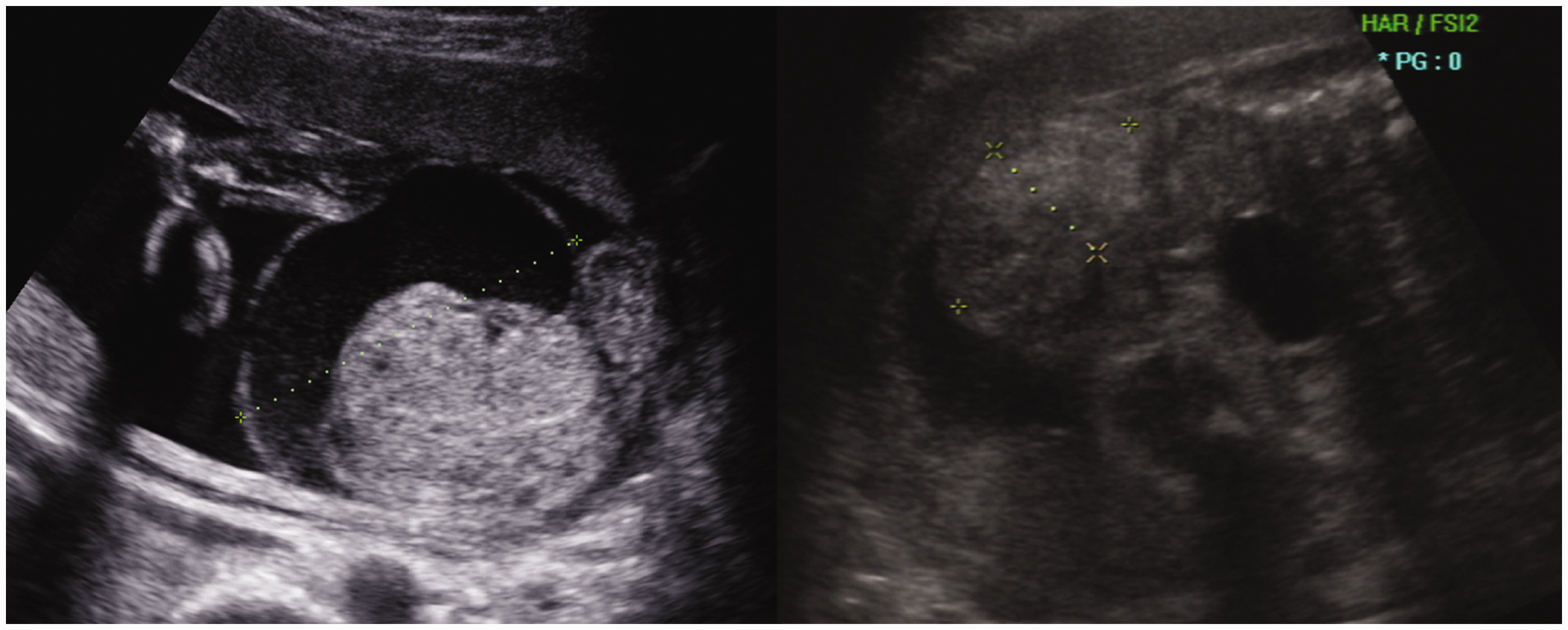
After birth, early and complete surgical resection is key to management of mature and immature SCTs, regardless of the size of tumor or the patient’s age (5,25,34,35,53–55). Incomplete resection is a major cause for recurrence (24,35); therefore, the coccyx should be resected with the tumor. Complete excision is adequate for management of mature and immature teratomas. Although immature histology is known as a risk factor for recurrence (24), adjuvant chemotherapy has no benefit in those patients (35,54). Thus, observation with complete resection is recommended in patients with immature teratomas (34). Platinum-based chemotherapy is the most important component after surgical resection for treatment of patients with malignant SCTs. Chemotherapy has been used for patients with advanced disease before surgical resection to reduce the tumor volume (35,56,57). Large, hypervascular SCTs with arteriovenous shunting may cause heart failure, hemolysis, rupture, or bleeding (27,58). Obstruction of the tumor-feeding arteries might be helpful to prevent this challenging situation (Fig. 11). Thus, preoperative embolization of the feeding arteries can reduce blood loss during operations and enable faster and safer tumor resection (58,59).
A case of an immature teratoma treated with preoperative embolization. (a) IV contrast-enhanced coronal CT scan demonstrates a type II SCT with tortuously enlarged tumor vasculature (arrows). (b) Abdominal aortography in the lateral projection shows feeding arteries from the bilateral internal iliac arteries (c) After embolization of feeders using gel foam, polyvinyl alcohol, and coils, decreased arterial flow was seen through the feeders.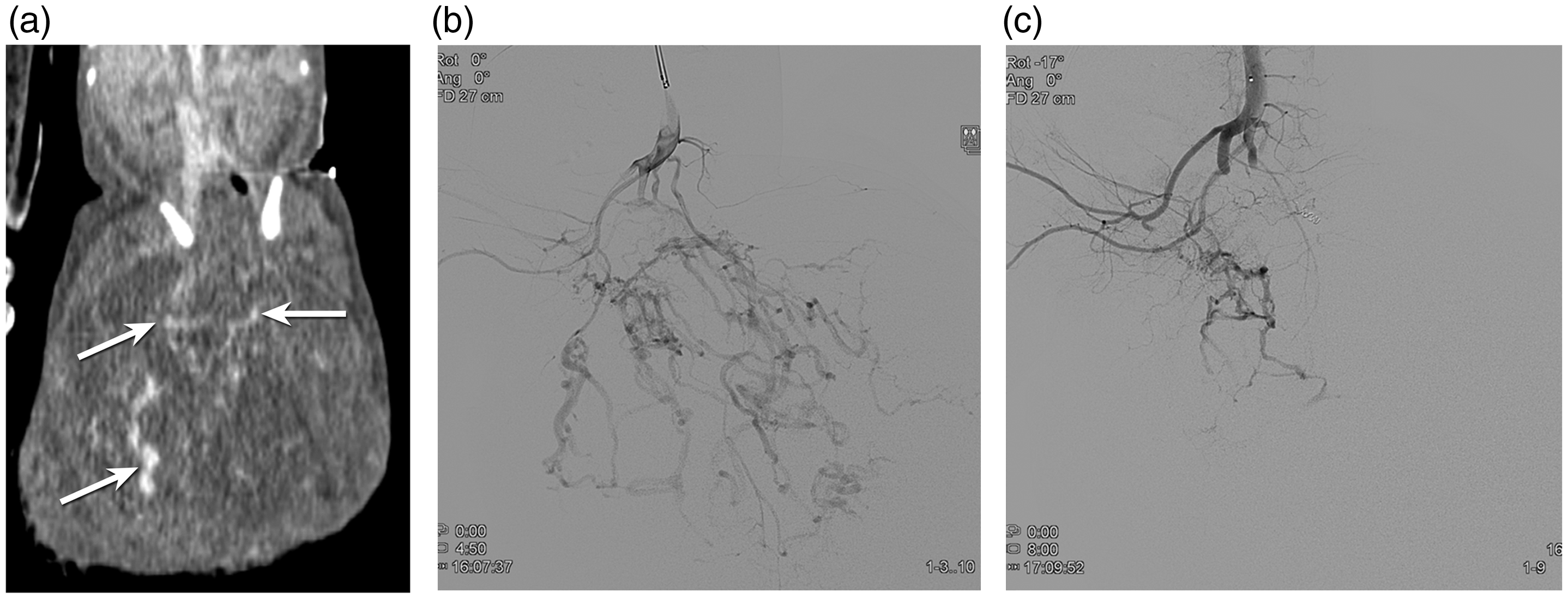
Conclusions
SCTs are the most common solid tumor in newborn infants. Three histopathologic types exist: mature teratomas; immature teratomas; and malignant teratomas. Morphologic classification plays an important role in predicting outcomes and for preoperative surgical planning. Although imaging features cannot accurately predict the histologic subtypes of the tumors, thorough evaluation of the imaging features can help distinguish malignant tumors from benign tumors. Occasionally, complications such as rupture, bleeding, or co-morbidities including urogenital and anorectal obstruction, hypoplasia of pelvic muscle, or hip dislocation, may occur and those imaging features should be interpreted in the radiologic report. Surgical resection is the cornerstone of treatment. When a tumor is too big for a baby to be delivered safely, prenatal minimal invasive treatment could be one treatment option.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.