
Abstract
Background
Breast tomosynthesis is more sensitive than mammography and can detect lesions that are not always visible with conventional methods such as digital mammography (MG) and ultrasonography (US). No standardized approach is available for the management of lesions that are detectable with tomosynthesis but are not visible on MG or US.
Purpose
To review suspicious breast lesions detected with tomosynthesis but not visible on two-dimensional (2D) MG or US and to determine the management options for these lesions.
Material and Methods
Ethical committee approval was obtained. The radiological records, biopsy or surgery results, and follow-up findings of 107 patients who had a tomosynthesis-positive but MG- or US-negative breast lesion between 2011 and 2016 were retrospectively evaluated.
Results
Of 107 lesions visible only with tomosynthesis, 74% were architectural distortions and 26% were asymmetrical opacities. All patients underwent magnetic resonance imaging (MRI) for further evaluation. Among the 48 (45%) MRI-negative lesions, none had a suspicious alteration during the follow-up period. Among the MRI-positive lesions, 28% of the 50 architectural distortions and 11% of the nine asymmetrical opacities were malignant.
Conclusion
Given the inherent high false-positive rate of breast tomosynthesis, breast MRI prior to biopsy may reduce the number of unnecessary biopsies for suspicious breast lesions that are tomosynthesis-positive only.
Introduction
Mammography (MG) is the only imaging modality for breast cancer screening that has been proven to reduce cancer-related mortality (1). However, several factors, such as younger age, menopausal status, and glandular tissue density and distribution, affect mammographic sensitivity. Tomosynthesis technology facilitates lesion detection and characterization by eliminating glandular tissue superposition with three-dimensional (3D) cross-sectional imaging. Breast tomosynthesis (BT) is now widely used alongside MG as a complementary screening tool with valuable contributions, such as revealing occult lesions due to glandular superposition, potentially reducing false-positive findings. The use of BT also reduces the need for additional problem-solving mammographic examinations. According to the results of mammographic screening studies, tomosynthesis provides increased cancer detection rates (2–8). However, the reported numbers on recalls are conflicting, with both decreased recall rates (2–5) and increased recall rates attributed to BT (6–8). Lesion characterization is also significantly enhanced with tomosynthesis (9–13). Masses and non-mass lesions can both be detected with BT and MG. Architectural distortion, which is the third most common finding in breast cancer after mass lesion and microcalcifications is detected more frequently with BT compared with MG (11–13). Asymmetrical densities within the extremely dense breast are often occult in ultrasound (US) but are easily detected with BT in daily practice. The aim of this study was to review suspicious findings detected only with BT and undetectable with US or MG and to discuss radiological approaches for these lesions based on biopsy results or follow-up findings.
Material and Methods
Institutional ethical committee approval was obtained. Patients who underwent simultaneous MG, BT, and US examinations and had suspicious findings only on BT between January 2011 and June 2016 were retrospectively reviewed. Patients who had breast surgery were excluded.
Imaging: A total of 36,647 patients were referred to our breast imaging unit for MG examination between January 2011 and June 2016 and 15,183 were examined with both MG and BT. Women with breast complaints or physical examination findings underwent diagnostic examinations, and women without any complaints or findings underwent screening examinations. Tomosynthesis indications included dense breasts and all abnormal mammograms for both the diagnostic and screening groups. Microcalcifications and lesions with accompanying microcalcifications were excluded because these lesions were visible on DM images. Mass and non-mass lesions such as architectural distortions and asymmetrical opacities were included. Of the 15,183 women who underwent MG, BT, and US examinations, lesions were detected only with BT in 107 women (0.7%).
MG and tomosynthesis examinations were performed in the same session with a Mammomat Inspiration (Siemens, Erlangen, Germany) unit. Standard two-view mammography (craniocaudal and mediolateral oblique) and mediolateral oblique tomosynthesis were applied. Tomosynthesis was obtained with a 25° arc movement of the tube. Both the mammography images and the reconstructed tomosynthesis images with a 1-mm slice thickness were evaluated on a MG-specific workstation (MammoReport, Siemens).
The MG and BT images were reviewed in consensus by three radiologists (with 12, eight, and three years of breast radiology experience, respectively). Breast densities were recorded according to the BI-RADS® system (14). The number, size, and morphological characteristics of the lesions were noted. In dense breast tissue, an opacity that could not be differentiated from the dense parenchyma and could only be seen with BT was named “unidentified asymmetrical opacity.” Stellate-shaped distortions or spiculations without a visible mass were named “architectural distortions.”
In our department, all diagnostic mammography examinations and opportunistic screening examinations revealing dense breasts, parenchymal asymmetry, or any other mammographic findings are accompanied by bilateral breast and axillary US. US examinations were performed with a 6–13 MHz broadband matrix transducer on an Acuson Antares Doppler US unit (Siemens, Erlangen, Germany). Second-look US was performed in the case of positive magnetic resonance imaging (MRI) findings and the findings were recorded.
Problem-solving breast MRI was conducted in the presence of BT-positive but MG- and US-negative findings.
MRI examinations were conducted with a 1.5 T MRI unit (Achieva, Philips MS, Eindhoven, The Netherlands). The MRI acquisition parameters were as follows. A T1-weighted (T1W) axial spin echo sequence (TR/TE = 454/10 ms, field of view [FOV] = 300, matrix = 432, slice thickness = 3 mm) was obtained with a seven-channel dedicated breast coil. Then, T2-weighted (T2W) axial short tau recovery (STIR) (TR/TE = 2000/173 ms, FOV = 300, matrix = 432, slice thickness = 2 mm) images were obtained. For dynamic imaging, a three-dimensional (3D) T1W axial gradient echo sequence (THRIVE) (TR/TE = 7/3, 4 ms, FV = 340, matrix = 352, flip angle = 10°, slice thickness = 1 mm) was acquired before and repeated six times after contrast material administration. A gadolinium-based contrast agent (Gadoterat meglumine, Dotarem®, Guerbet, Villepinte, France, n = 57 cases; Gadobutrol, Gadovist®, Bayer, Berlin, Germany, n = 31 cases; Gadodiamide, Omniscan®, GE Healthcare, Milwaukee, WI, USA, n = 28 cases) was administered at 0.1 mM/kg with an automatic injector (Medrad Spectris Solaris EP, Bayer Radiology Solutions, Whippany, NJ, USA) at a rate of 2 mL/s intravenously. Then, the line was flushed with 20 mL of saline solution.
Three radiologists evaluated the MRI images by consensus. If present, lesions were named according to the BI-RADS® classification. Four mass-enhancing lesions detected with second-look US were sampled under US guidance and the remaining lesions that were positive only on MRI were sampled with an MRI-guided 10G vacuum-assisted biopsy technique. All MRI-guided biopsies were performed by a single radiologist with 12 years of experience in breast imaging. Patients with MRI-positive lesions and pathology results of high-risk benign diagnosis underwent wire-localized surgical excision.
Radiological follow-up: Cases without any lesions on MRI underwent six-month and one-year follow-up BT examinations. The average follow-up time was 32 months (range = 7–61 months). MRI-positive lesions with benign pathological diagnoses were followed up with MRI.
Data collection: Age, menopausal status, presence of any risk factors, physical examination findings, and imaging findings were retrospectively recorded. The histopathological results of patients who underwent imaging-guided biopsy or surgical excision were obtained from the pathology department archive and the follow-up imaging results were also recorded.
Results
The average age of the patients who had only BT-positive lesions was 52 ± 10 years (age range = 30–72 years). Fifty-four percent of the patients were premenopausal women and 46% were postmenopausal.
Imaging findings: During the study period, a total of 15,183 cases were examined with MG, BT, and US, of which 107 had suspicious findings only on BT, without any findings on MG or US. The breast density classification results were as follows; 0% = BI-RADS 1, 16% = BI-RADS 2, 52% = BI-RADS 3, and 32% = BI-RADS 4. Seventy-nine (74%) of these 107 lesions were architectural distortions and 28 (26%) were unidentified asymmetrical opacities (Figs. 1 and 2).
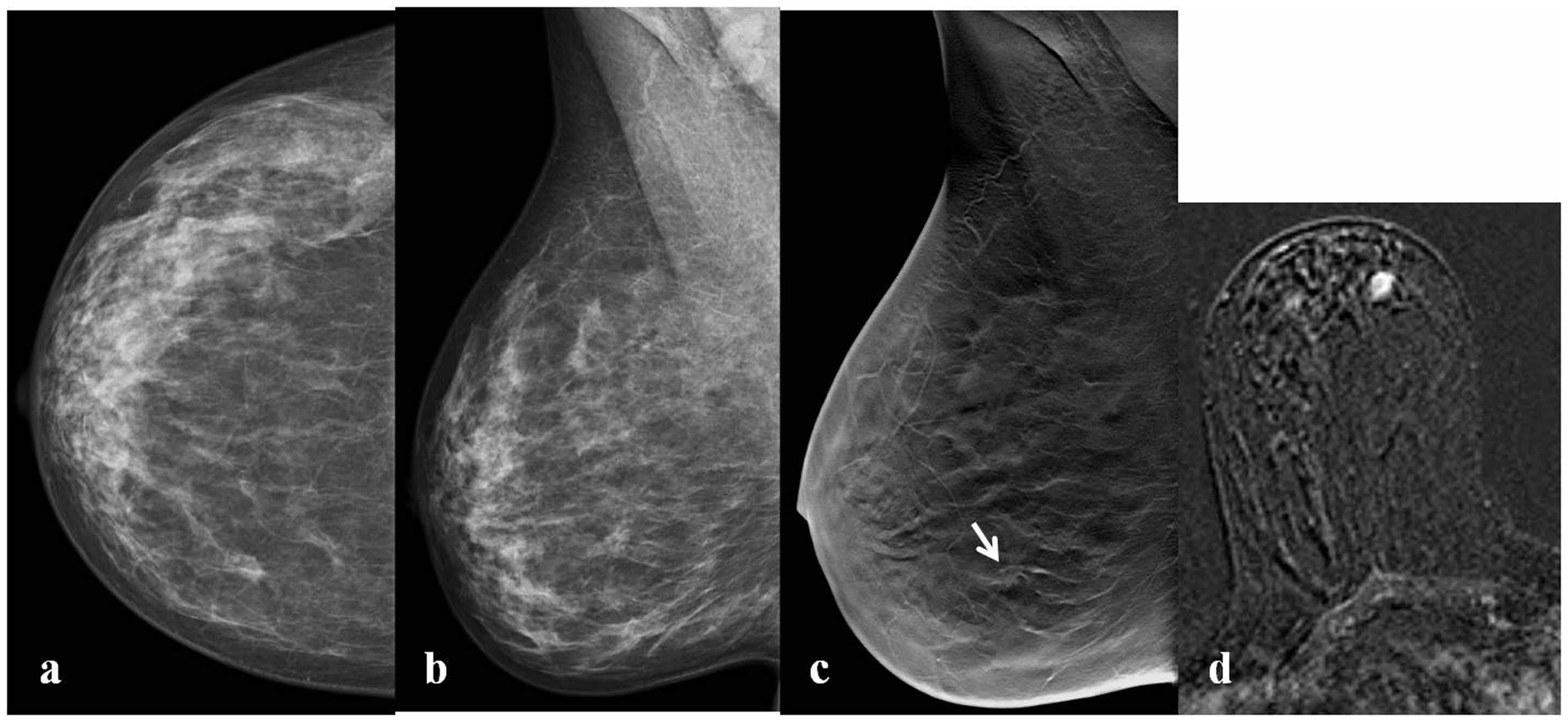
A 49-year-old asymptomatic woman. No visible abnormality was present in the left breast in (a) craniocaudal (CC) and (b) mediolateral oblique (MLO) mammograms. A subtle architectural distortion (arrow) was seen in an MLO tomosynthesis image (c). There was no abnormality on sonographic examination (not shown). Axial post-contrast subtraction MRI (d) revealed a non-mass enhancement. Axial second-look ultrasonography (e) showed a non-mass lesion. Invasive ductal cancer was diagnosed after US-guided 14 G core-needle biopsy. A 57-year-old asymptomatic woman. No visible abnormality was present in the right breast in (a) craniocaudal (CC) and (b) mediolateral oblique (MLO) mammograms. An unidentified asymmetrical opacity (arrow) was seen on MLO tomosynthesis (c). There was no abnormality on sonographic examination (not shown). Axial post-contrast subtraction MRI (d) revealed a mass enhancement. Invasive ductal cancer was diagnosed after MRI-guided 10 G vacuum-assisted biopsy.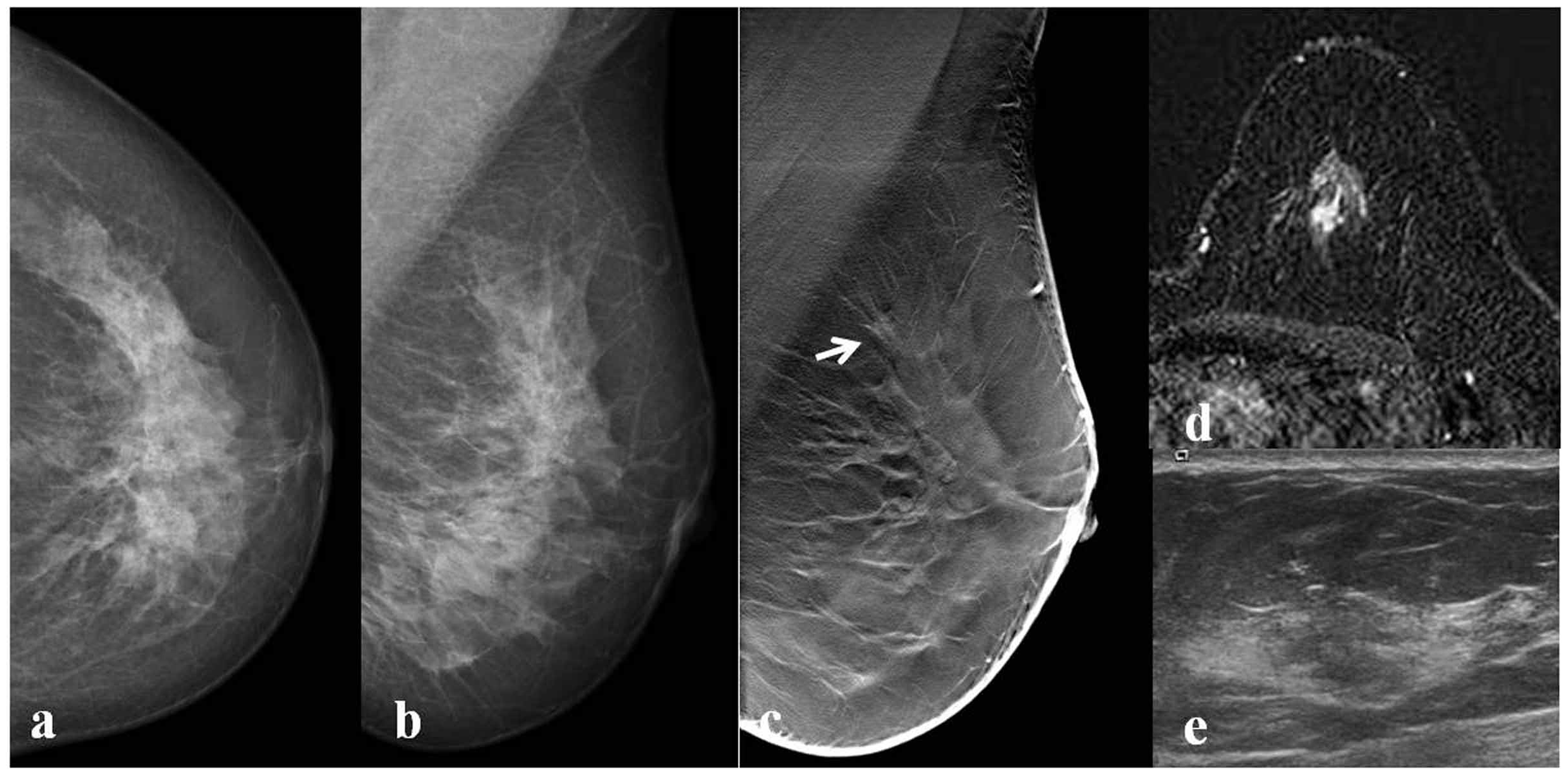
Forty-eight (45%) lesions were MRI negative. Among the 59 (55%) remaining MRI-positive lesions, 52 of them showed non-mass enhancement and seven had mass enhancement. Five architectural distortion lesions and two unidentified asymmetrical opacity lesions showed mass enhancement patterns. According to histopathology, six of these mass-enhancing lesions were malignant and only one was benign. Most of the non-mass-enhancing lesions showed focal or regional enhancement patterns (76%).
Four lesions that had mass-enhancement patterns on MRI were also detected with second-look US and these lesions were sampled by US-guided biopsy. The remaining 55 lesions underwent MR-guided biopsy.
Histopathological results: Fifteen (25.5%) of the 59 BT-positive and MRI-positive lesions were malignant and 44 (74.5%) were benign. Twenty-three (52%) of these benign lesions were high-risk lesions and four were found to be malignant after surgical excision. Radial scar, atypical ductal hyperplasia, and lobular carcinoma in situ (LCIS) were classified as high-risk lesions. The malignancy upgrade rate of these high-risk lesions was 17.3% (two radial scars and two atypical ductal hyperplasia). The false-negative rate of breast biopsy was 27% (4/15).
Fifty of the 79 (63%) architectural distortion lesions had an MRI finding. Histopathological evaluation revealed that 14 (28%) of these lesions were malignant and 36 (72%) were benign. All of the malignant lesions were invasive cancers (11 invasive ductal and three invasive lobular cancers). All four high-risk benign lesions that were upgraded to malignancy after surgical excision were architectural distortions.
Distribution of MRI findings according to histopathological results.
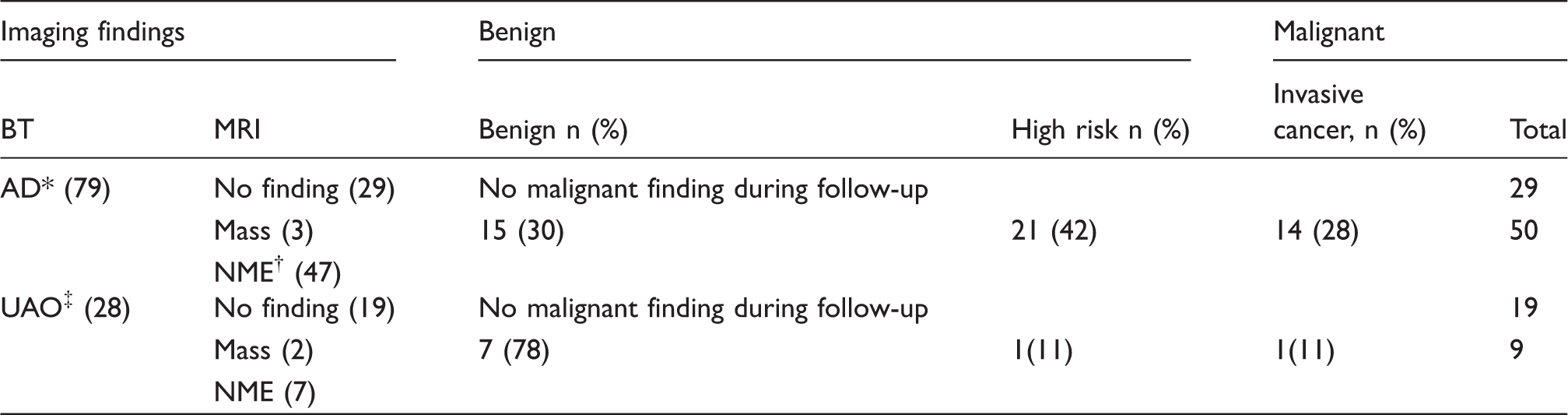
Architectural distortion.
Non-mass enhancement.
Undefined asymmetrical opacity.
Follow-up results: A total of 48 lesions were positive on BT but negative on MRI. These lesions were followed up with BT. No alterations suspicious for malignancy were observed during an average follow-up period of 32 months. Twenty-eight BT- and MRI-positive lesions (21 architectural distortions, seven unidentified asymmetrical opacities) were followed up with both BT and MRI; none of these lesions had any suspicious alterations during the follow-up period.
Discussion
BT remains under investigation as a complementary screening tool to MG. More masses and architectural distortion lesions are detected with tomosynthesis (11–13,15–17). Our aim was to evaluate non-calcified lesions detected only on BT. Approximately 74% of the BT-positive and MG- or US-negative lesions presented in this study were architectural distortions. Architectural distortions can be present in either malignant or benign conditions. In addition to invasive ductal or lobular cancers, ductal in situ cancers may also be seen as architectural distortions. The presence of an architectural distortion should be verified before biopsy, according to our clinical experience and consistent with the literature (13). In a screening series by Lang et al. (single-view MLO tomosynthesis), the positive recall rate was 1.7% for BT and 0.9% for MG. Stellate-shaped architectural distortions, radial scars, and postoperative scars are more frequently detected by BT than MG (17).
Most lesions that cannot be seen on MG but are present on BT can also be detected with US. Visualization of a lesion by US verifies its presence and is the preferred mode of imaging guidance for biopsy. However, as shown in the present study, some of these lesions cannot be detected with US. In these cases, MRI is a good choice for problem solving. In this study, 63% of architectural distortions were detected with MRI and 28% of the architectural distortions detected by MRI were malignant. In a study by Ray et al., 74% of MG-negative but BT-positive lesions were architectural distortions and 36% were malignant (18). Patryka et al. reported a malignancy rate of 21% for lesions detected by BT (19). The main difference between the present study and these previous studies is the evaluation of US-negative lesions. Freer et al. surgically excised 36 architectural distortions after wire localization that were seen only on BT and were negative on MG or US, of which 47% were malignant (20). The malignancy rate in the presented study was somewhat lower, probably due to differences in case selection and the nomenclature used to describe the findings. However, considerable malignancy potential is expected among architectural distortion lesions detected only with BT. US-negative lesions require further evaluation. Among lesions described as asymmetry or focal asymmetry, BT has lower recall rates than MG, according to a study by Laurenco et al. (21). By contrast, the same study reported higher recall rates of BT for mass-, calcification-, or architectural distortion-type lesions. In the present study, 32% of “unidentified asymmetrical opacity” lesions had suspicious findings on MRI and 11% were found to be malignant. As the number of unidentified asymmetrical opacity lesions in this study was limited, performing MRI examination before biopsy appears to be an appropriate approach.
In general, second-look US has a crucial role in cases with positive MRI findings. If an MRI-positive lesion can be localized with US, the case can be resolved easily with US-guided biopsy, which is more practical than MRI guidance. However, only four mass-enhancing lesions were detected with second-look US in this study and all non-mass enhancing lesions were US negative. These results suggest that second-look US is not very beneficial for subtle BT findings with a non-mass enhancement pattern on MRI.
In this study, none of the MRI-negative patients had a progressive finding on BT follow-up and no malignancy was detected during the follow-up period. Using this approach, 45% of patients avoided unnecessary biopsy.
There are limitations to this study. The retrospective nature of the present study is a major limitation; however, the results of this study are important for the discussion of approaches to BT-positive and otherwise negative lesions. Another limitation is that we did not use BT-guided biopsy or wire-localization approaches. Biopsy under BT guidance, which is a reliable biopsy option for BT-positive but otherwise negative lesions, is not available in our institution. Breast biopsy under BT guidance is a relatively novel technique and only a limited number of studies are available in the literature (22,23). Surgical excision after BT-guided wire localization is another option for such lesions. High technical success and cancer detection rates were achieved in a study in which lesions were excised after BT-guided wire localization and the authors concluded that this technique is a convenient and mandatory diagnostic approach (20).
Similar to MG, biopsy and follow-up options should also be meticulously evaluated for women with BT-positive lesions and the most non-invasive approach possible should be chosen. The lesions presented in this study differ from MG and/or US lesions due to their faint characteristics and most were non-mass lesions. For such lesions, cancer must be clearly ruled out, and the most minimally invasive approach should be selected. False-positive faint architectural distortions are frequently seen on BT. An increase in clinical experience may have a positive impact by lowering the false-positive rate of BT for such lesions. Further prospective, multi-center, and multi-reader studies are needed to verify and explain our findings.
In conclusion, until sufficient clinical experience is obtained, MRI examination before biopsy is a convenient approach for BT-positive but US-negative lesions when BT-guided biopsy option is not available. The best diagnostic option—follow-up, BT-guided biopsy, MRI-guided biopsy, or surgical excision with BT-guided wire localization—can easily be chosen by the radiologist based on the MRI findings.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.