
Abstract
Background
Non-mass enhancements (NME) with invasive components account for 10–42% of total malignant NMEs. The factors associated with invasiveness on magnetic resonance imaging (MRI) could be useful for clinical assessment and treatment.
Purpose
To evaluate the clinical significances of the distributions and internal enhancement patterns (IEP) of malignant NMEs on 3-T breast MRI.
Material and Methods
A total of 448 consecutive women with newly diagnosed breast cancer that had undergone preoperative MRI and surgery between February 2013 and March 2016 were identified. After exclusions, 72 malignant NMEs without a mass in 72 women (mean age = 51.5 years) were included. Two readers independently assessed distributions and IEPs of NME, according to the Breast Imaging Reporting and Data System lexicon fifth edition. Collected data included the presence of invasion and histopathologic factors.
Results
A clustered ring IEP was significantly associated with invasive cancer (75.0%, P = 0.001, Reader1; 72.9%, P < 0.001, Reader 2), absence of necrosis (79.0%, P < 0.001; 72.1%, P < 0.001, respectively), and high Ki-67 expression (74.2%, P = 0.048; 74.2%, P = 0.003, respectively). A clumped IEP was related to ductal carcinoma in situ (33.3%, P = 0.025; 50.0%, P = 0.001, respectively), absence of lymph node metastasis (24.1%, P = 0.029; 31.5%, P = 0.030, respectively), and presence of necrosis (34.5%, P = 0.003; 44.8%, P = 0.001, respectively).
Conclusion
The presence of a clustered ring IEP in patients with breast cancer was found to be significantly associated with invasive breast cancer and high Ki-67 expression.
Keywords
Introduction
Non-mass enhancement (NME) on breast magnetic resonance imaging (MRI) is defined as an area of enhancement without an associated mass (a space occupying lesion) in the Breast Imaging Reporting and Data System (BI-RADS) lexicon of the American College of Radiology (ACR). The fifth edition of the BI-RADS lexicon eliminated ambiguities, and reorganized and consolidated terminologies from the fourth edition. The term ductal enhancement in the distribution of NME was eliminated, as were the terms reticular/dendritic enhancement and stippled/punctate enhancement for the internal enhancement patterns (IEPs) of NME. The term clustered ring was added. Thus, the fifth edition makes possible precise descriptions of the distribution and IEPs of NME, facilitates quality assurance, concise communication with physicians, and improves patient care (1,2).
NME may be benign or malignant, and NMEs with invasive components reportedly account for 10–42% of total malignant NMEs (3,4). Furthermore, ductal carcinoma in situ (DCIS) lesions have been found to exhibit NME at high rates in the range of 69–90% (5,6).
Preoperative identification of invasion in malignant disease of the breast is important because lymph node staging procedures are required in invasive disease (7). The risk of sentinel lymph node metastasis is higher for patients with a final diagnosis of DCIS with microinvasion than for patients with pure DCIS (9.3% vs. 4.8%) (8,9). Also, invasive carcinomas are capable of metastasis to distant sites and have poorer prognoses than DCIS.
Screening mammography is used for the early detection of breast cancer and ultrasound is mainly used as a diagnostic modality and for guided biopsies. Contrast-enhanced MRI now plays a pivotal role in breast cancer staging in conjunction with mammography and ultrasound and can be used as a roadmap for treatment planning (10,11). It has been shown in previous studies that kinetic enhancement curves on MRI are a very useful cancer diagnostic tool for mass-like breast lesions, though they are not as effective for non-mass-like lesions (12). However, dynamic contrast-enhanced MRI distribution and IEPs appear to be useful for analyzing the characteristics of NME (13,14). Regarding the MR features of breast lesions showing NME, Tozaki et al. (15) analyzed 30 consecutive lesions showing NME and reported that a combination of BI-RADS MRI descriptors and clustered ring enhancement criteria aided the differential diagnosis of lesions showing NME. However, their analyses included only morphologic findings according to the first edition of the MRI lexicon, which was issued in 1992. To our knowledge, correlations between patterns of malignant NME according to the revised fifth edition of the BI-RADS lexicon and histopathologic factors ranging from invasiveness to immunohistochemistry biomarkers have not been described in the scientific literature.
This study was undertaken to evaluate the clinical significances of the distributions and IEPs of malignant NMEs on 3-T breast MRI by assessing their associations with the presence of invasion and histopathologic factors.
Material and Methods
Case descriptions
Our institutional review board approved this retrospective study and waived the requirement for informed consent. A review of medical records between February 2013 and March 2016 at our institution resulted in the identification of 448 consecutive women with newly diagnosed breast cancer who had undergone preoperative breast MRI and subsequent breast cancer surgery. All MRI scans were reviewed by one senior radiologist with six years of breast imaging experience, who did not otherwise participate in this study. In 94 of the 448 women, MRI demonstrated breast cancer as NME without a mass, and of these 94 patients, 22 patients were excluded for the following reasons: (i) a postoperative state, including excision (n = 21); and (ii) MR image acquisition after neoadjuvant chemotherapy (n = 1). Thus, 72 malignant NMEs were identified in 72 patients (age range = 26–79 years; mean age = 51.5 years) and these patients constituted the study population.
Imaging methods
MRI was performed using a 3.0-T system (Skyra, Siemens Healthcare, Erlangen, Germany). A body RF coil was used for excitation and a bilateral breast coil (16-channel phased array coil) was used as the receiver. Dynamic MRI was performed using a three-dimensional fat-suppressed volumetric interpolated breath-hold examination sequence with parallel acquisition technique (GRAPPA factor 4) before and five times after injecting a bolus of gadobutrol (0.1 mmol/kg; Gadovist, Bayer Schering Pharma, Berlin, Germany) at a rate of 2 mL/s and a subsequent 20-mL saline flush, all administered using an automatic injector. Both breasts were examined in the sagittal plane on five dynamic images, which were acquired every 90 s after contrast injection. Additionally, subtraction images were obtained using pre- and post-contrast series to suppress bright fat signals. The parameters used for dynamic MRI were as follows: TR/TE = 6.35/2.92 ms; flip angle = 24°; field of view = 25 × 18.75 cm; matrix = 448 × 269; receiver bandwidth = 330 Hz per pixel; interpolated slice thickness = 1.5 mm; partitions = 224; and acquisition time = 90 s.
Imaging sequences included a localizing sequence, an axial T2-weighted sequence, an axial diffusion-weighted sequence, a sagittal fat-saturated T1-weighted (T1W) sequence before and five times after contrast injection, and an axial T1W sequence after dynamic enhancement.
Review sessions
Two radiologists with four and 13 years of experience in breast radiology, respectively, independently reviewed all breast MR images at full resolution using a commercial workstation equipped with 5-MP monitors. Before analysis, the two radiologists had reviewed by consensus multiple breast MRI cases with diverse distributions and IEPs of NME as described in the BI-RADS lexicon fifth edition. During the review of the 72 image sets, the two radiologists were aware that all were breast cancer cases, and of the lateralities and breast quadrants affected by NMEs. However, other clinical information and pathologic findings were withheld. The readers independently classified the distributions and patterns of the malignant NMEs into groups as described by the ACR BI-RADS lexicon fifth edition. Distributions were classified as focal, linear, segmental, regional, multiple regions, or diffuse, and IEPs as homogeneous, heterogeneous, clumped, or clustered ring. First, distribution was evaluated mainly using maximum intensity projection (MIP) images and one of the six distribution types was chosen for each case. Second, presence of each of the four IEPs within NMEs was analyzed using sagittal fat-saturated T1W sequence obtained first times after contrast injection and its subtraction images.
Pathologic analysis
Histopathologic information was acquired from pathology reports stored in our institution’s electronic archive. Final histopathologic results of surgical specimens were reviewed to determine tumor type, invasiveness (invasive vs. in situ), presence of a metastatic lymph node (LN), presence of necrosis, lymphovascular invasion, and the statuses of estrogen receptor (ER), progesterone receptor (PR), human epidermal growth factor receptor 2 (HER-2), and Ki-67.
In situ cancer was defined as a proliferation of malignant epithelial cells that had not breached the myoepithelial layer. When malignant epithelial cells had breached the basement membrane and invaded adjacent stroma to a depth of ≤1 mm, microinvasion (MI) was deemed to be present (16). We divided the histopathologic results of surgical specimens into two groups based on invasiveness (invasive vs. in situ), and cancers exhibiting microinvasion were classified as invasive.
Breast cancer guidelines advise sentinel lymph node biopsy (SLNB) in patients with DCIS by core biopsy at high risk of invasive cancer or in cases of mastectomy. Thus, all patients in this study underwent SLNB based on our surgeons’ decision.
ER and PR positivity were determined by using a cut-off value of <10% positively stained nuclei. Tumors with HER2 scores of 3+ (strong homogeneous staining) were considered positive, and for tumors with HER2 scores of 2+ (moderate complete membranous staining in ≥10% of tumor cells), silver-enhanced in situ hybridization was used to detect the presence of HER2 amplification (gene copy number >6 or HER2/chromosome 17 ratio >2.2). For Ki-67 expression status, nuclear staining ≥14% was considered to indicate a high level of expression (17).
Statistical analysis
Relations between distribution of NME as assessed by the radiologists and invasiveness (invasive or in situ) were evaluated. In addition, we searched for relations between IEPs of NMEs and invasiveness, and between IEPs and other histopathologic factors (lymph node metastasis, presence of necrosis, lymphovascular invasion, hormone receptor [ER or PR], HER-2, and Ki-67) using the chi-square or Fisher’s exact test. The student’s t-test was used to analyze the relation between invasiveness and tumor size as determined by MRI.
Inter-observer reliability for distribution of the NME was assessed using intraclass correlation coefficients (ICCs), where an ICC of 0.61–0.80 was taken to indicate substantial agreement and an ICC of >0.80 to indicate almost perfect agreement (18). The κ statistic was used to determine inter-observer agreement for IEPs. A κ value of <0.20 was taken to indicate poor agreement, 0.21–0.40 fair agreement, 0.41–0.60 moderate agreement, 0.61–0.80 good agreement, and >0.80 excellent agreement (19). The analysis was performed using SPSS ver. 18.0 (SPSS Inc., Chicago, IL, USA) and statistical significance was accepted for P values of <0.05.
Results
Study participants
Of the 72 patients, 44 had invasive ductal carcinoma (IDC; 61.1%), 24 DCIS (33.3%), two invasive lobular carcinoma (ILC) (2.8%), and two invasive papillary carcinoma (2.8%). We classified patients into two categories in terms of invasion: invasive cancer (n = 48, 66.7%) and carcinoma in situ (n = 24, 33.3%). Pathologically proven lymph node metastasis was present in 18 patients (25.0%), necrosis in 29 (12.5 %), and lymphovascular invasion in 14 (19.4%). Forty-nine (68.1%) patients were hormone receptor positive (ER positive or PR positive), 29 (40.3%) demonstrated HER-2 expression, and 31 showed high Ki-67 expression (43.1%).
Mean tumor size of NMEs on MRI (n = 72) was 5.97 ± 2.51 cm (median = 6.25 cm, range = 1.00–10.00 cm) and mean sizes of invasive cancer (6.29 ± 2.36 cm) and carcinoma in situ (5.32 ± 2.73 cm) were not significantly different (P = 0.124).
Relations between distributions and internal enhancement patterns and histopathologic factors
The relation between the distribution and internal enhancement patterns of malignant non-mass enhancement and invasiveness in the 72 breast cancer patients by two readers.
P < 0.05.
The relation between internal enhancement patterns of malignant non-mass enhancement and pathologic factors in the 72 breast cancer patients by two readers.
P < 0.05.
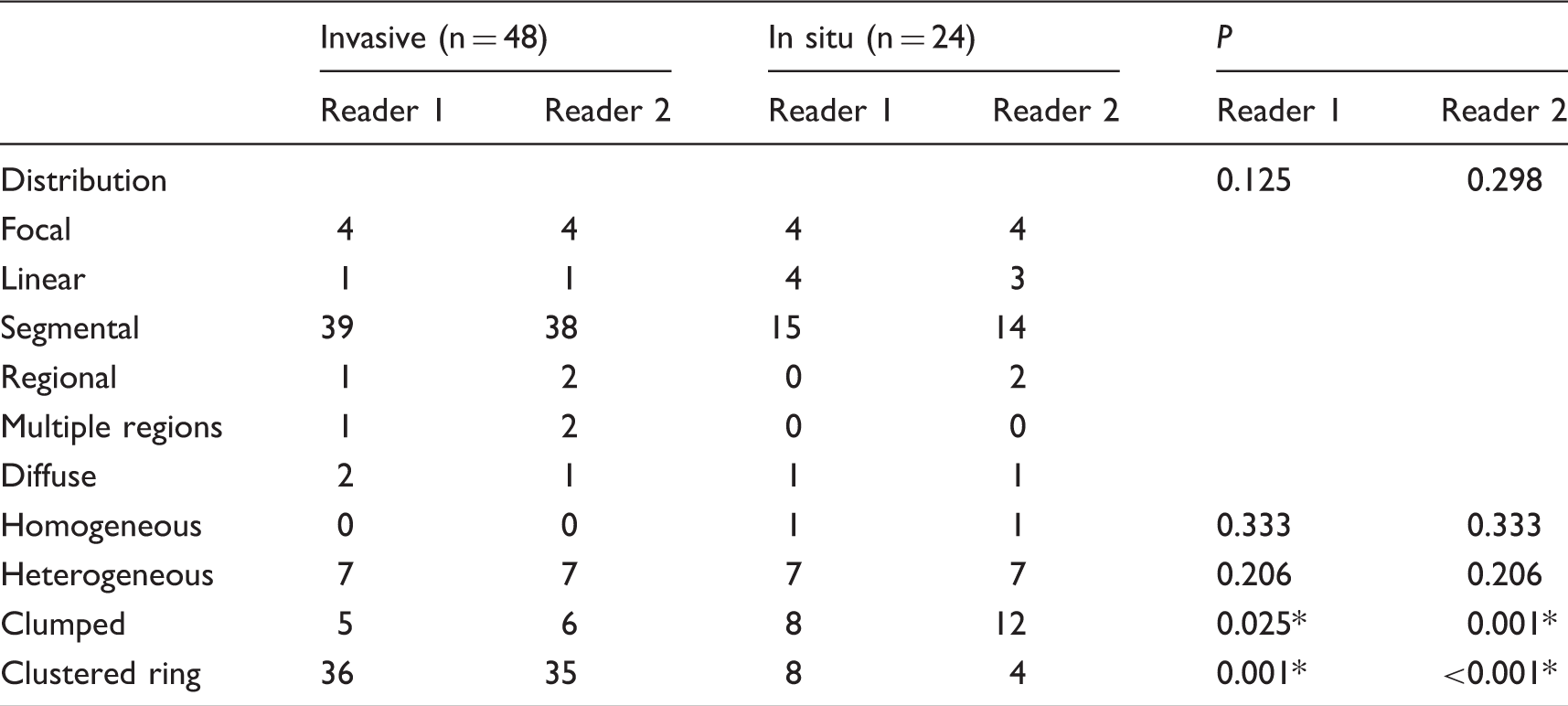
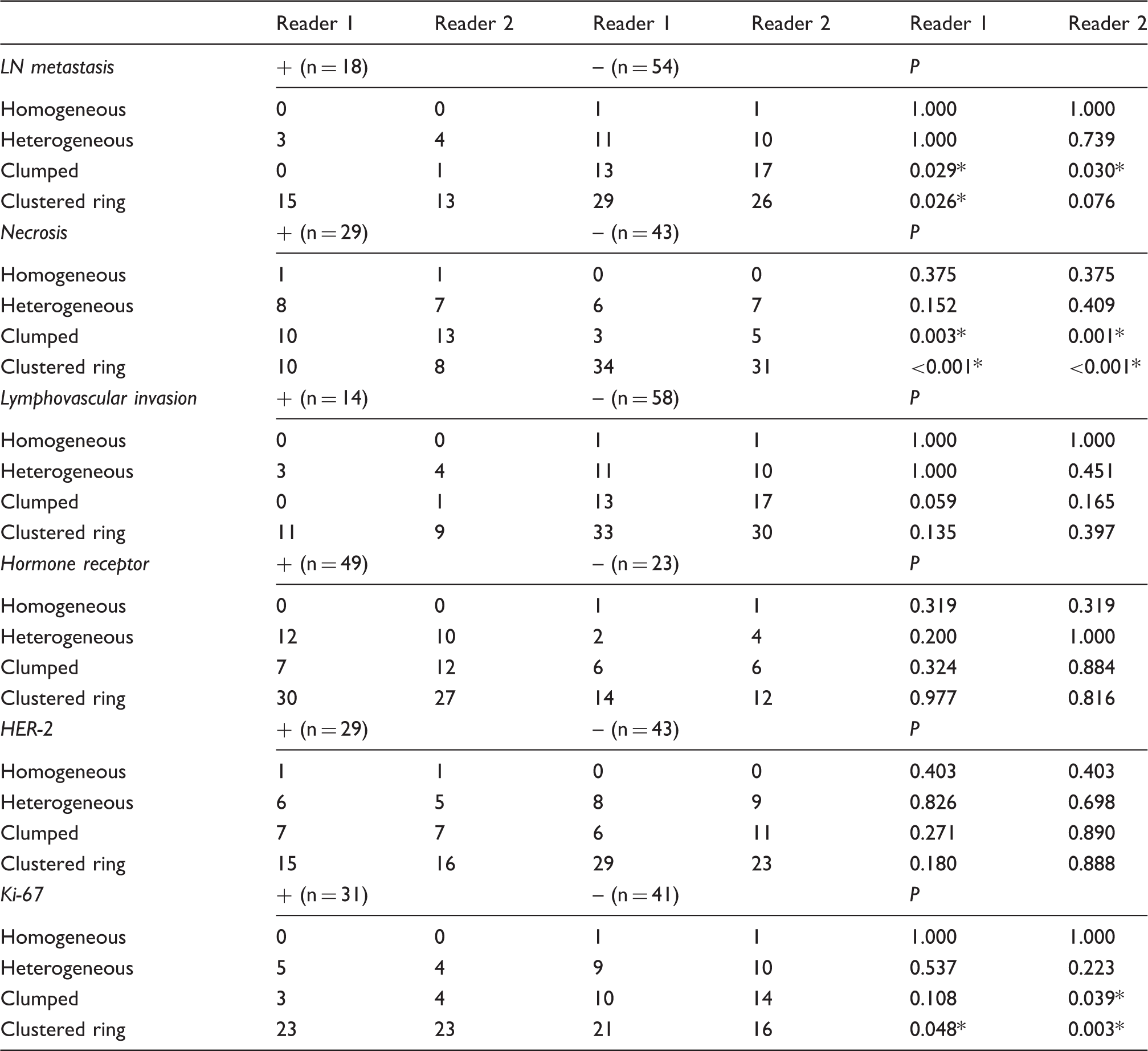
The results of both readers revealed a clustered ring IEP was significantly associated with invasive cancer (75.0%, P = 0.001, Reader 1; 72.9%, P < 0.001, Reader 2), the absence of necrosis (79.0%, P < 0.001, Reader 1; 72.1%, P < 0.001, Reader 2), and high Ki-67 expression (74.2%, P = 0.048, Reader 1; 74.2%, P = 0.003, Reader 2). A clumped IEP was found to be significantly associated with DCIS (33.3%, P = 0.025, Reader 1; 50.0%, P = 0.001, Reader 2), the presence of necrosis (34.5%, P = 0.003, Reader 1; 44.8%, P = 0.001, Reader 2), and the absence of LN metastasis (24.1%, P = 0.029, Reader 1; 31.5%, P = 0.030, Reader 2).
No significant difference was observed between patients with invasive cancer and carcinoma in situ in terms of distribution (P = 0.125, Reader 1; P = 0.298, Reader 2).
Inter-observer agreement regarding the distributions and internal enhancement patterns of NMEs
The two readers showed almost perfect agreement for the distributions (ICC = 0.957; P < 0.001) and excellent to good agreement for the presence of IEPs. More specifically, reader agreements were as follows: homogenous: excellent (κ = 1.000; P < 0.001); heterogeneous: excellent (κ = 0.823; P < 0.001); clustered ring: excellent (κ = 0.802; P < 0.001); and clumped: good (κ = 0.796; P < 0.001).
Discussion
According to the World Health Organization, more than 450,000 cases of breast cancer were diagnosed in 2012, which meant it accounted for >28% of all female malignancies (20). IDC is the most common type of breast cancer and accounts for 65–75% of all breast cancers (21); according to a report released in the United States, DCIS accounts for >20% of newly diagnosed cases (22). Preoperative MRI is now considered by most to be an essential imaging modality in breast cancer. Lee et al. (23) reported ∼43% of patients with a preoperative diagnosis of DCIS have histopathologic evidence of DCIS with an invasive component, which concurs with previous reports. Therefore, it would seem methods capable of predicting DCIS with an invasive component preoperatively would facilitate comprehensive care planning. The majority of studies on DCIS with an invasive component have characterized masses by MRI, but NME is the most common manifestation in DCIS, although DCIS may exhibit variable morphologic features on MR images. IDC also may exhibit NME.
In our study, invasive cancer was noted in 66.7% (48 patients) of malignant NME cases and this rate is higher than rates (10–42%) reported in previous studies (3,4). Furthermore, pathologically proven lymph node metastasis was present in 25.0% (18/72 patients) and all tumors with lymph node metastasis were invasive cancer. Accordingly, the prediction of the presence of an invasive component in malignant NME is of considerable importance.
In the present study, a clustered ring IEP was strongly associated with invasive cancer, which is in line with previous results. Machida et al. (7) showed a clustered ring IEP had higher odds of containing an invasive component. In another study (24), the authors demonstrated clustered ring enhancement was significantly more common in microinvasive ductal carcinoma than in DCIS (57.1%). Furthermore, Tozaki et al. (15,25) reported that the MRI finding with the highest positive predictive value for malignancy was clustered ring enhancement in a non-mass lesion. Clustered ring enhancement represents periductal enhancement and is the result of contrast material pooling in periductal stroma or the ductal wall of DCIS, and possibly of contrast washout from enhancing tumor cells in ductal lumen (26). Tozaki et al. (24) reported a washout kinetics pattern in 55% of malignant lesions exhibiting clustered ring enhancement. Together these observations indicate that tumors exhibiting clustered ring enhancement have more aggressive behaviors.
In addition to conventional histopathologic parameters, proliferation is one of the major factors for the treatment decision-making in breast cancer patients and for predicting the risk of recurrence (27). Ki-67 is a nuclear protein that is positively associated with cellular proliferation. In a large cohort study conducted by Inwald et al. (28), Ki-67 was found to be an independent prognostic parameter of disease-free and overall survival in breast cancer patients, that is, tumors with a high-Ki-67-labeling index were associated with poorer disease-free and overall survival than tumors with a low-Ki-67-labeling index (28). Thus, our result that Ki-67 expression was significantly higher in patients with a clustered ring NME indicates its potential use for predicting prognosis and survival.
A 47-year-old woman with an 8.5-cm IDC in the left breast (ER+/PR+/HER−/Ki−67+). (a) Maximum intensity projection image showing a segmental distribution (arrow) in the upper quadrant of the left breast. (b) Sagittal fat-saturated T1W image obtained first time after contrast injection showing a clustered ring internal enhancement pattern. (c) Axial fat-saturated T1W image after dynamic enhancement revealed an enlarged lymph node with a lobular shape (arrow) at left axilla level I. Final histopathology revealed metastatic involvement of the lymph node.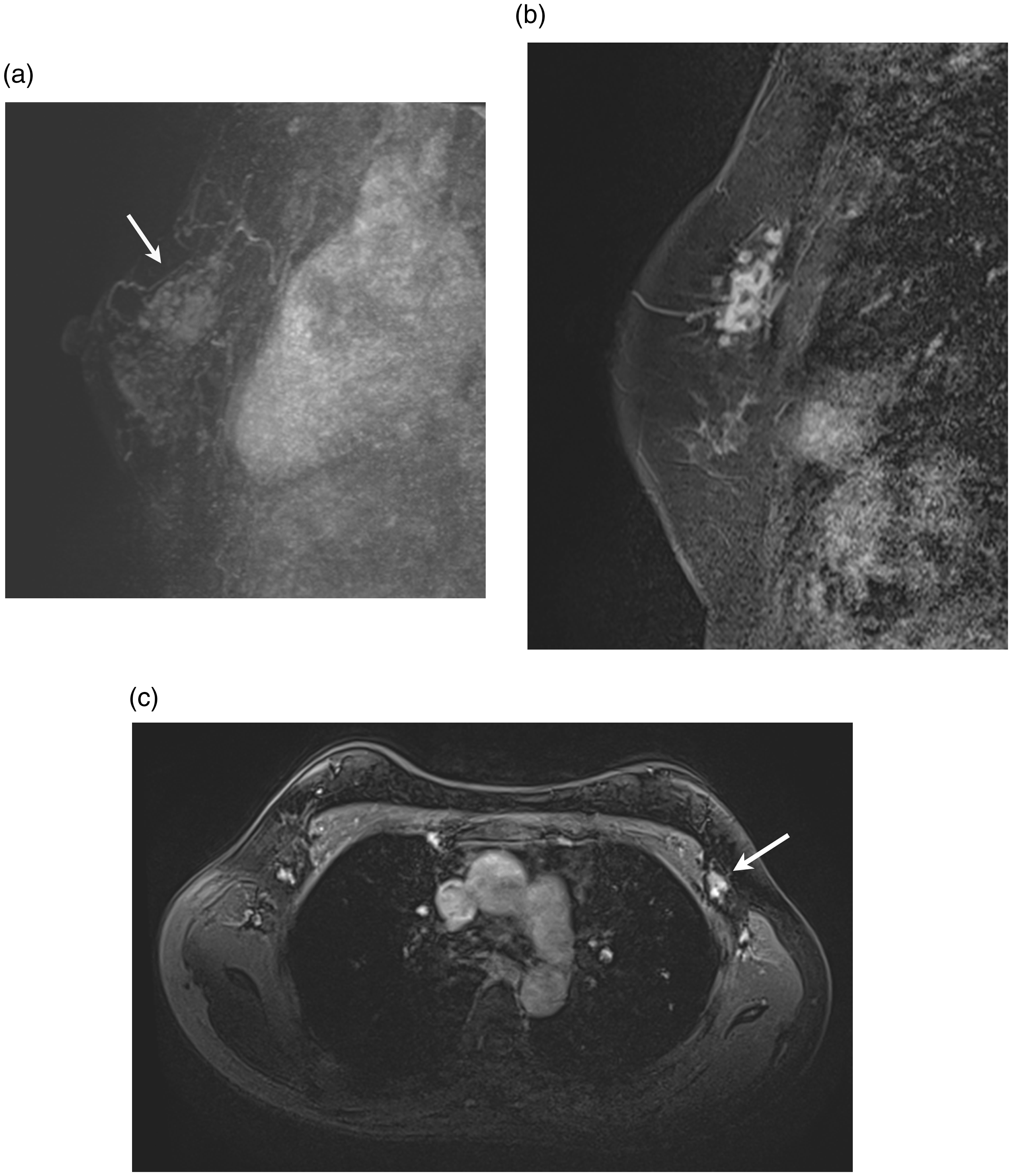
Whereas the results obtained by our two readers showed a clumped IEP was positively associated with DCIS. Similarly, Raza et al. (29) demonstrated that this pattern is the most common IEP found in pure DCIS, and Jansen et al. (30), concluded the dominant MR features of pure DCIS lesions were non-mass enhancement and a clumped IEP.
On the other hand, Hahn et al. (24) reported that a segmental distribution was a dominant feature of microinvasive ductal carcinoma, whereas no statistically significant association between this distribution and invasive cancer was detected in this study.
In the present study, inter-observer agreement was almost perfect for the distributions (ICC = 0.957; P < 0.001) and was excellent to good for the IEPs, whereas Machida et al. (7) found only fair to moderate inter-observer agreement (κ = 0.26–0.45) for the distributions and moderate agreement (κ = 0.41–0.42) for a clustered ring IEP. We ascribe the better results obtained in the present study to the consensus pretesting conducted by the two readers using the BI-RADS lexicon fifth edition.
Some limitations of the present study should be mentioned. First, we retrospectively reviewed MR images at a single institution, and thus, patient selection bias is inevitable. Second, the readers had different levels of experience, which might explain their different results, although overall inter-observer agreement was excellent. Third, the number of cases was relatively small, and not many patients had a homogeneous IEP, or diffuse, multiple regions, or regional distributions on MRI. Furthermore, no case with lymph node metastasis from DCIS was included, and all cases with lymph node metastasis were of invasive cancer. This may have biased relations between IEPs and lymph node metastasis because nodal involvement is more characteristic of invasive cancer. Fourth, ILC accounted for only 2.8% of malignant NME lesions in our study. However, the overall proportion of ILC at our institution during this period (1.8% [8/448]) was lower than ILC proportion reported in the United States (about 10%) (31,32). Considering the overall proportion (1.8%) at our institution, ILC presenting as NME was not a small percentage (2.8%). Fifth, our study included only NMEs without a mass, although cancers present more frequently as masses than NME lesions. Further prospective multi-institutional studies are warranted to validate our results.
In conclusion, the presence of a clustered ring IEPs was found to be significantly associated with invasive breast cancer and high Ki-67 expression when a cancer was visualized as NME without mass by preoperative MRI in patients with breast cancer.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.