
Abstract
Background
Diffusion-weighted imaging (DWI) and quantitative apparent diffusion coefficient (ADC) values are widely used in the differential diagnosis of ovarian tumors.
Purpose
To assess the diagnostic performance of quantitative ADC values in ovarian tumors.
Material and Methods
PubMed, Embase, the Cochrane Library, and local databases were searched for studies assessing ovarian tumors using quantitative ADC values. We quantitatively analyzed the diagnostic performances for two clinical problems: benign vs. malignant tumors and borderline vs. malignant tumors. We evaluated diagnostic performances by the pooled sensitivity and specificity values and by summary receiver operating characteristic (SROC) curves. Subgroup analyses were used to analyze study heterogeneity.
Results
From the 742 studies identified in the search results, 16 studies met our inclusion criteria. A total of ten studies evaluated malignant vs. benign ovarian tumors and six studies assessed malignant vs. borderline ovarian tumors. Regarding the diagnostic accuracy of quantitative ADC values for distinguishing between malignant and benign ovarian tumors, the pooled sensitivity and specificity values were 0.91 and 0.91, respectively. The area under the SROC curve (AUC) was 0.96. For differentiating borderline from malignant tumors, the pooled sensitivity and specificity values were 0.89 and 0.79, and the AUC was 0.91. The methodological quality of the included studies was moderate.
Conclusion
Quantitative ADC values could serve as useful preoperative markers for predicting the nature of ovarian tumors. Nevertheless, prospective trials focused on standardized imaging parameters are needed to evaluate the clinical value of quantitative ADC values in ovarian tumors.
Keywords
Introduction
Ovarian tumors are common gynecological tumors. Histologically, ovarian neoplasms are categorized as malignant, borderline, or benign. Ovarian cancers are the second most common gynecologic malignancy (1). Due to the lack of symptoms in early stages, most women are diagnosed in the late stage of the disease, with five-year survival rates of approximately 30–50% (2). Patients with ovarian cancers generally need to undergo radical staging surgery with postoperative chemotherapy. However, ovarian cancer still has a high likelihood of recurrence. Therefore, ovarian cancer is a serious threat to women’s reproductive health. Borderline ovarian tumors comprise up to 15% of primary ovarian tumors (3). As a type of low malignant tumor, borderline ovarian tumors exhibit epithelial stratification, mitotic activity, and mild nuclear atypia but lack stromal invasion (4). They often occur in young women and are mainly localized to the ovary at the time of presentation (5). Patients with borderline ovarian tumors who desire to preserve their fertility can elect fertility-sparing surgery, with an overall five-year survival rate of up to 90% (6). Therefore, preoperative differentiation of benign from malignant ovarian tumors or borderline from malignant ovarian tumors is crucial for determining the surgical strategy.
Magnetic resonance imaging (MRI) has clearly been demonstrated to be the best imaging tool to detect and characterize ovarian neoplasms due to its superb tissue contrast (7). Diffusion-weighted imaging (DWI) is a type of functional MRI that provides information on tissue cellularity and cell membrane integrity by detecting the extent of diffusion of free water molecules. The apparent diffusion coefficient (ADC) can quantify the diffusion of water molecules in tissues. In previous studies of breast, kidney, and prostate neoplasms (8–10), significant inverse correlations were reported between the ADC values and tumor cellularity.
Previous studies have indicated that ADC values differ among malignant, borderline, and benign ovarian tumors and can be helpful for differentiating malignant from benign or borderline ovarian tumors (11–13). Nevertheless, these studies have included limited numbers of patients and reported varied diagnostic performances. Therefore, we performed a meta-analysis of the literature to summarize the diagnostic worth of quantitative ADC values in ovarian tumors.
Material and Methods
Search strategy
A literature search including three electronic databases—PubMed, Embase, and the Cochrane Library —and the local databases CBM, VIP, CNKI, and Wanfang was conducted by two independent observers (SP and RC). The searches were conducted using both medical subject headings and the text words “ovarian neoplasms,” “ovarian masses,” “ovarian lesions,” and “ovary tumors,” combined with the medical subject headings and text words “diffusion magnetic resonance imaging,” “diffusion weighted imaging,” “DW-MRI,” and “DWI.” The searches had no language restrictions and no limitation was set for the beginning date, with the search updated until 28 June 2017.
Study inclusion and exclusion criteria
Studies were eligible if the following criteria were met: (i) clinical studies assessing the diagnostic accuracy of quantitative ADC values for the differentiation of malignant from benign ovarian tumors or borderline from malignant ovarian tumors; (ii) evaluation of the solid portions of ovarian tumors; (iii) histopathology used as the reference standard; and (iv) sufficient data available in the fourfold (2 × 2) tables, corresponding to true positive (TP), false positive (FP), false negative (FN), and true negative (TN). Studies with cysts, mature teratomas, and endometriomas were excluded. To minimize selective bias in small samples, studies with < 25 cases of ovarian masses were excluded.
Quality assessment and data extraction
Methodologic quality was independently assessed by two observers (SP and RC) using the Quality Assessment of Diagnostic Accuracy Studies (QUADAS-2) tool, which has been recommended for use in systematic reviews to evaluate the risk of bias and the applicability of primary diagnostic accuracy studies (14). Additionally, two authors (SP and RC) extracted relevant data, including baseline data and main outcome indexes, from each study. The following baseline data were collected: author; year; magnetic field strength; b values; ADC threshold values; and the histological types of the benign ovarian tumors group. The main outcome indexes extracted were number of malignant, borderline, or benign ovarian tumors and the sensitivity and specificity of each primary study. Disagreements between the two reviewers were resolved by a third reviewer (JWQ) and the majority opinion was used in the final analysis. This meta-analysis followed the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) recommendations.
Meta-analysis
Meta-analyses were performed using the software Meta-disc version 1.4 (Universidad Complutense, Madrid, Spain) (15). A random-effects model was used to pool the sensitivities and specificities from various studies. The summary receiver operating characteristic (SROC) curves and the corresponding areas under the curve (AUCs) were obtained. A heterogeneity test was performed using the I-square test. An I-square > 50% suggested notable heterogeneity. If significant heterogeneity occurred, subgroup analysis was then performed depending on study-level covariates (study design, magnetic field, histological types of the benign group, or b value). The threshold effect is another source of heterogeneity, which can be used to compute the Spearman correlation coefficient between the logit of sensitivity and the logit of 1-specificity. A strong positive correlation of > 0.6 or P < 0.05 was suggestive of the threshold effect. If the threshold effect existed, SROC curves were constructed to evaluate the sensitivity and specificity. The AUC was used to analyze the diagnostic value of quantitative ADC values in differentiating among ovarian tumors.
Results
Literature search
A flowchart illustrating the study selection is shown in Suppl. Fig. 1. In total, 742 records were found in the databases, and 330 duplicated records were removed. Then, 259 records were excluded by assessing titles and abstracts. After full-text examinations of the remaining 153 articles, 137 were further excluded. Finally, 16 articles (11–13,16–28) were eligible for inclusion in the systematic review. For discrimination between malignant and benign lesions, ten articles (11,12,16–23) including 722 malignant tumors and 298 benign tumors in total were found in the literature. For differentiating borderline tumors and malignant tumors, six studies (13,24–28) were eligible for meta-analysis, including 144 borderline tumors and 229 malignant tumors.
Forest plot of sensitivity and specificity for quantitative ADC values in the differential diagnosis between malignant and benign ovarian tumors.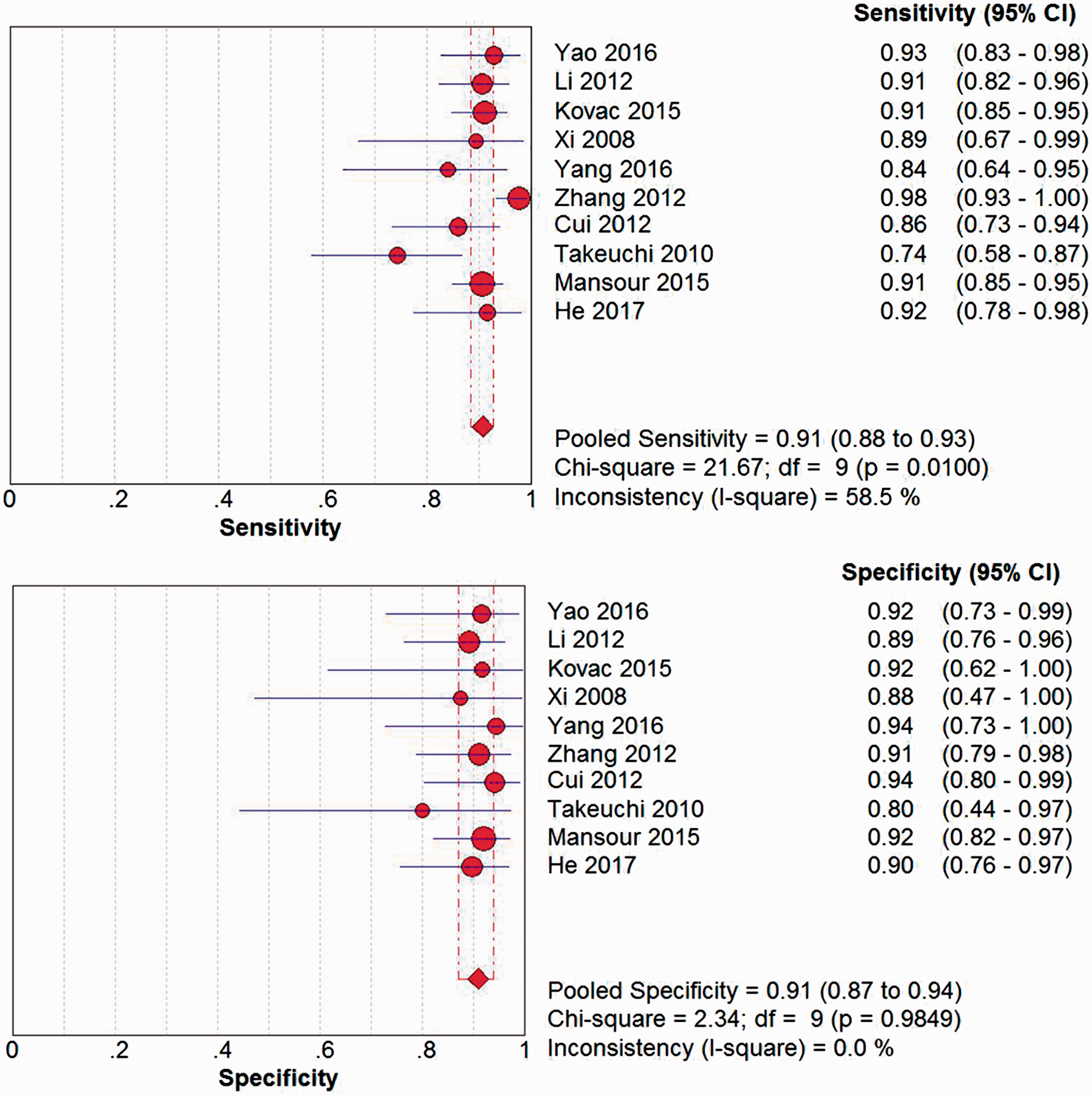
Study characteristics
Baseline data and main outcome indexes of the included studies of benign vs. malignant ovarian lesions.
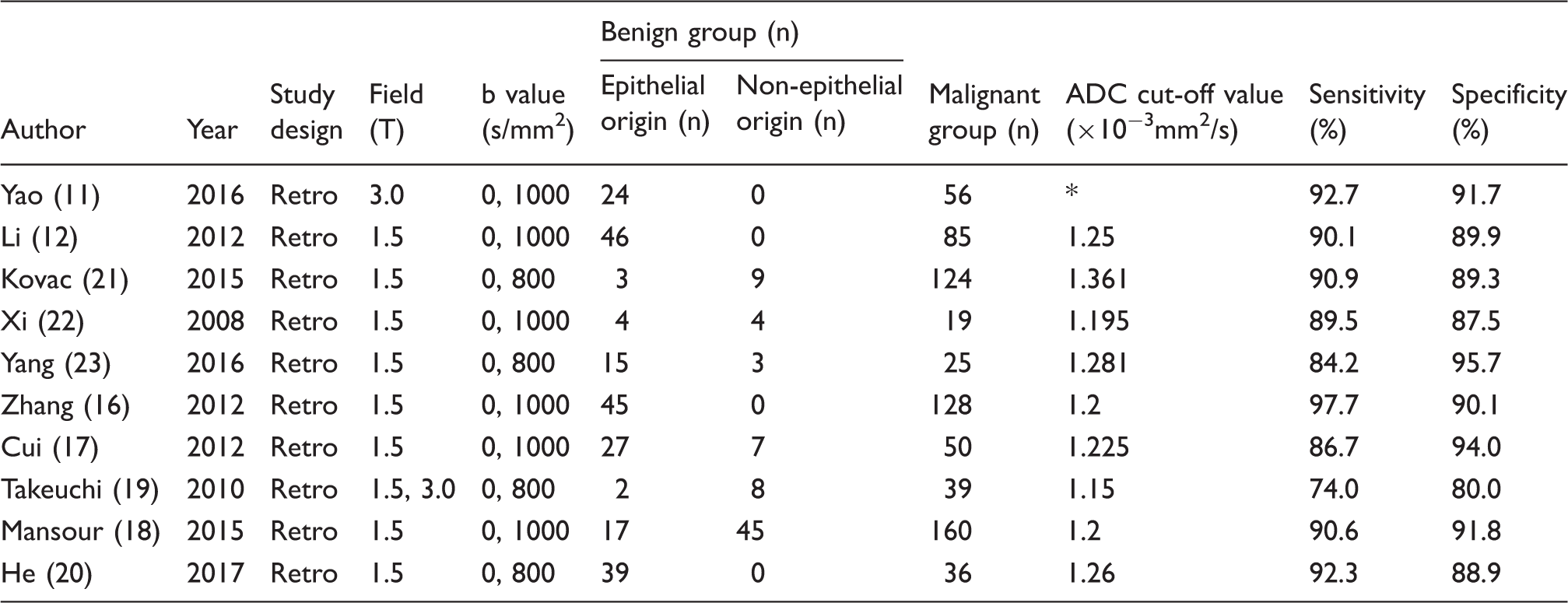
not mentioned.
Retro, retrospective; ADC, apparent diffusion coefficient.
Baseline data and main outcome indexes of the included studies of borderline vs. malignant ovarian lesions.
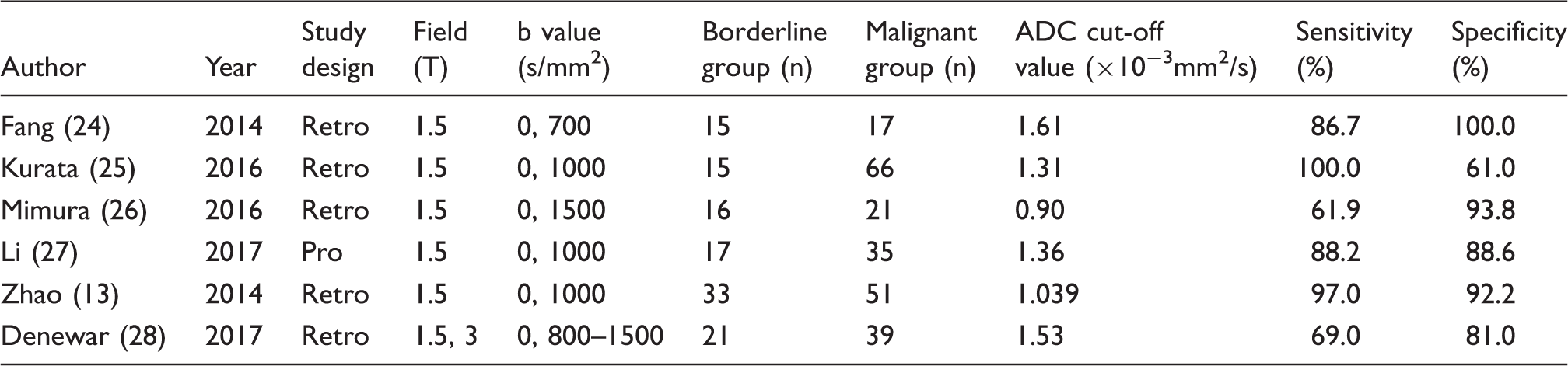
Retro, retrospective; Pro, prospective; ADC, apparent diffusion coefficient.
The risk of bias and applicability concerns of the included primary studies were based on QUADAS-2 (Suppl. Table 1). The quality of all 16 studies was moderate.
Quantitative ADC values distinguishing malignant from benign ovarian tumors
The threshold effect was explored by plotting sensitivity against 1-specificity for each study in an ROC space. The pattern of the resulting points did not suggest a “shoulder-arm” shape, indicating that a threshold effect may not exist. Therefore, Spearman rank correlation analysis was performed to further assess the threshold effect. A correlation coefficient of – 0.03 (P = 0.93) was obtained, which indicated that no threshold effect was observed in accuracy estimates among the individual studies.
The diagnostic performance of quantitative ADC values in distinguishing malignant and benign ovarian tumors was measured as pooled sensitivity and specificity. The pooled estimated values were a sensitivity of 0.91 (95% confidence interval [CI] = 0.88–0.93) and a specificity of 0.91 (95% CI = 0.87–0.94); the AUC was 0.96. These results indicated excellent diagnostic performance of quantitative ADC values in ovarian tumors. Forest plots and SROC curves for the ten studies are shown in Figs. 1 and 2.
SROC curve of the included studies using quantitative ADC values to differentiate between malignant and benign ovarian tumors.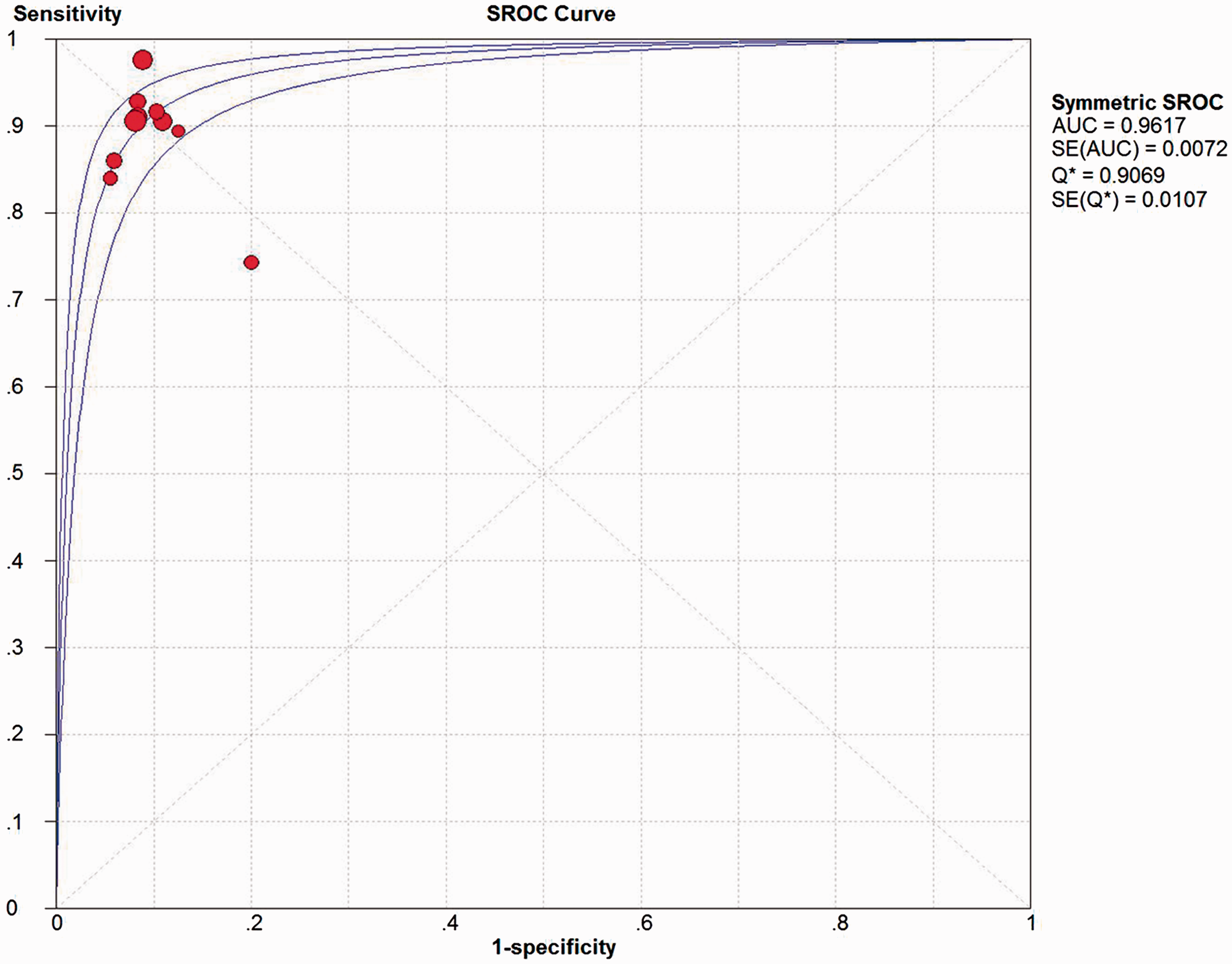
Results of pooled estimates of all studies and of different subgroups.
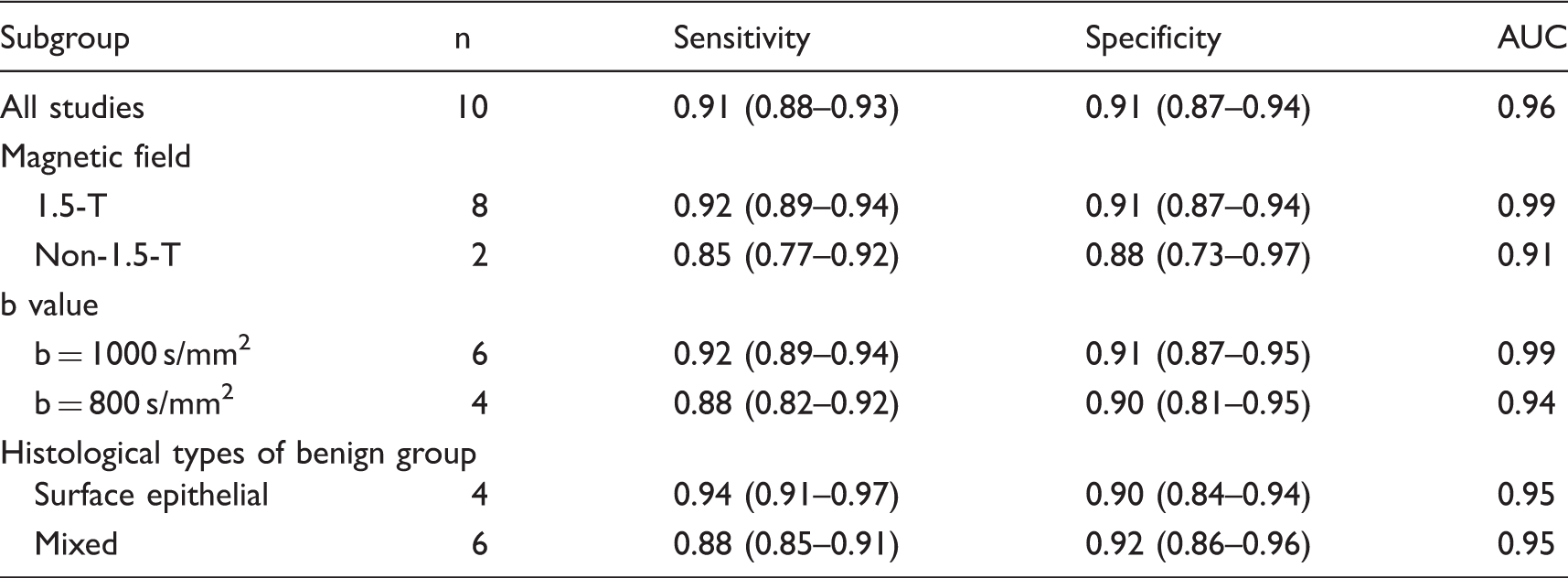
AUC, area under the curve.
Quantitative ADC values distinguishing borderline from malignant ovarian tumors
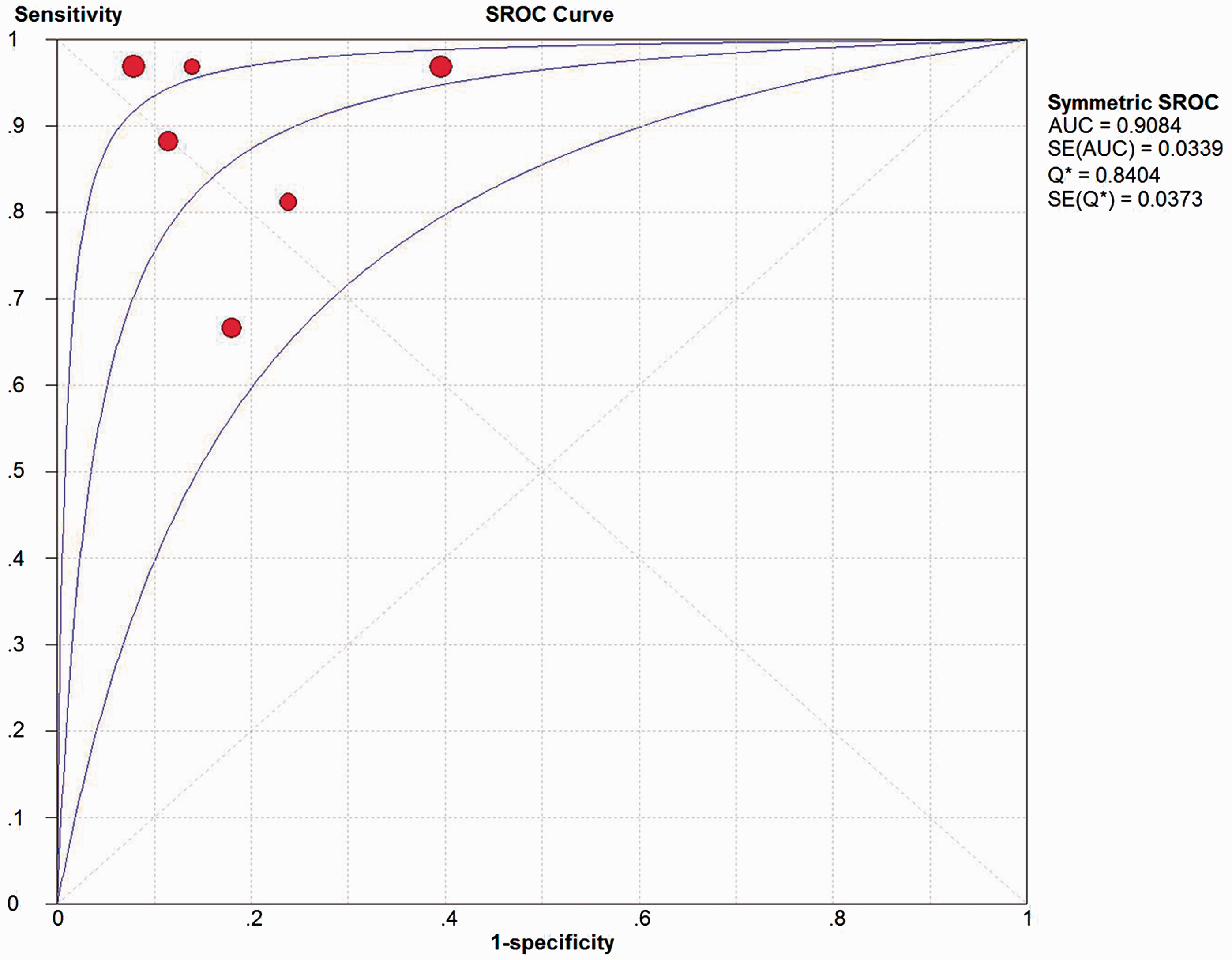
The six eligible studies for differentiation of borderline from malignant ovarian tumors included 229 malignant ovarian tumors and 117 borderline ovarian tumors. The Spearman correlation coefficient was –0.41 (P = 0.43), which indicated absence of the threshold effect. The pooled sensitivity and specificity (Fig. 3) were 0.89 (95% CI = 0.82–0.94) and 0.79 (95% CI = 0.73–0.84), respectively, and the AUC (Fig. 4) was 0.91, indicating moderately accurate test performance in differentiating borderline from malignant ovarian tumors. The forest plot of sensitivity and specificity indicated that heterogeneity existed.
Forest plot of sensitivity and specificity for quantitative ADC values in the differential diagnosis between borderline and malignant ovarian tumors. SROC of the included studies using quantitative ADC values to differentiate between borderline and malignant ovarian tumors.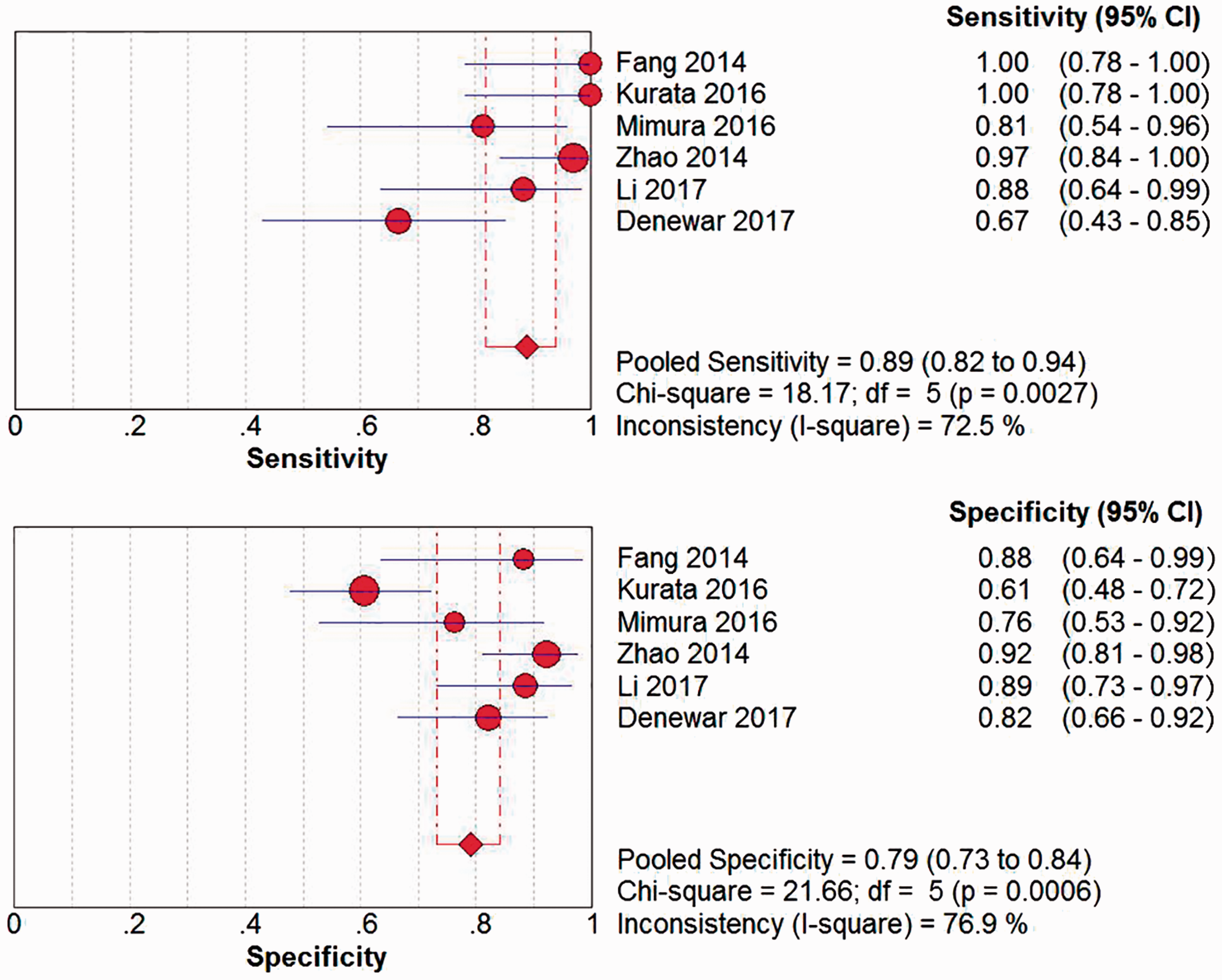
Sensitivity and specificity estimates of all studies and of different subgroups.
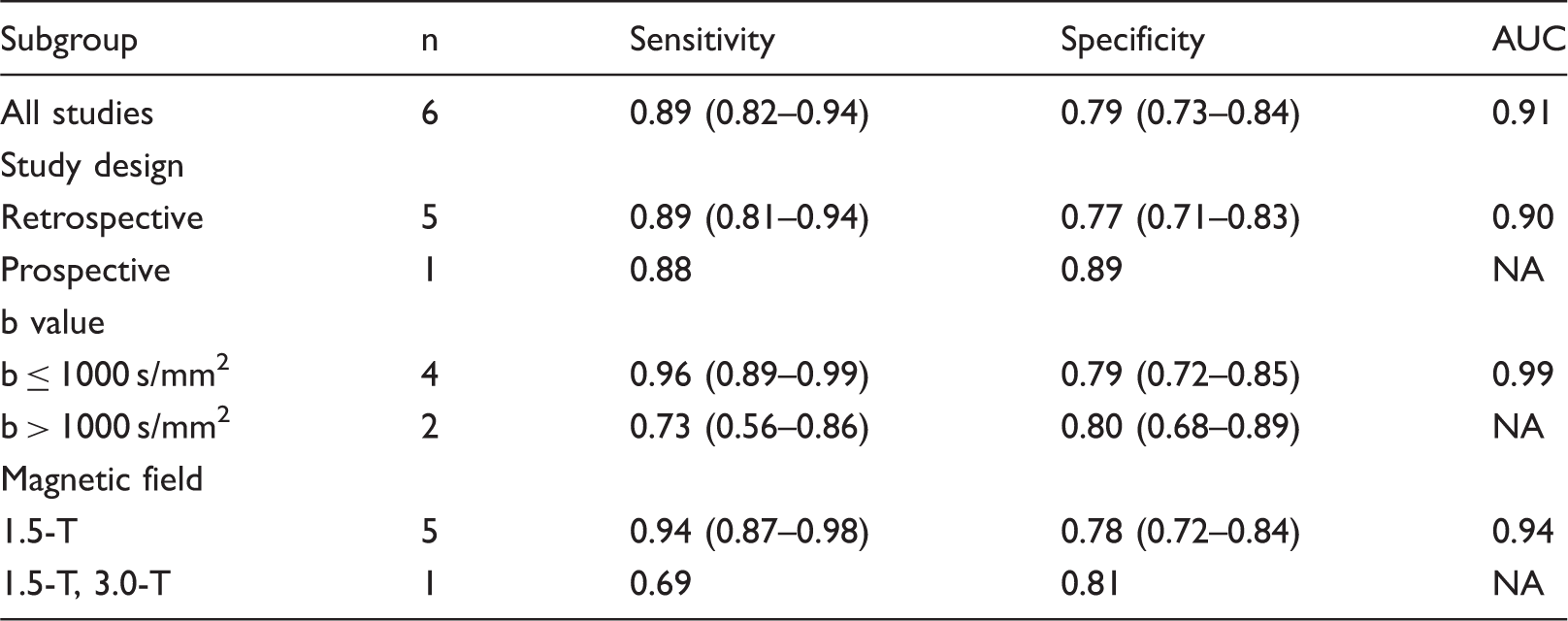
AUC, area under the curve; NA, not applicable.
Discussion
Ovarian tumors constitute a serious threat to women’s health and are clinically difficult to manage. Preoperative diagnosis of ovarian tumors by conventional MRI has historically been difficult, especially in discriminating borderline from malignant ovarian tumors. Therefore, new imaging techniques are required.
As a functional MRI technique, DWI can reflect the micro-movements of water molecules in in vivo tissues. The increased cellularity and reduced extracellular space of malignant tumors restrict water molecules movement in the tissue, which leads to a high signal intensity on DWI and a low ADC value. Previous studies have demonstrated the diagnostic effectiveness of ADC values in prostate, kidney, and breast lesions. Based on the characterization of ADC values, a meta-analysis was performed to evaluate the diagnostic worth of quantitative ADC values in ovarian tumors. The included studies assessed the solid components of ovarian tumors, as cystic components have low relevance with ADC values for characterizing ovarian tumors, which has been underlined in previous studies (12,29). The meta-analysis results provide an estimate of the diagnostic performance of quantitative ADC values for predicting malignancy, with pooled sensitivity and specificity values of 0.91 and 0.91, respectively, and an AUC of 0.96. These findings demonstrated that quantitative ADC values are useful diagnostic markers for distinguishing between malignant and benign ovarian lesions.
However, some previous studies have demonstrated that quantitative ADC values could not contribute to distinguishing between benign and malignant ovarian tumors (30,31). This apparent discrepancy is likely due to the different histological types of benign ovarian tumors, such as sex cord-stromal tumors, Brenner tumors, and cystadenofibromas. Due to the abundant collagen-producing fibroblastic cells and a dense network of collagen fibers within the extracellular matrix (30), these benign tumors are characterized by low ADC values that do not significantly differ from the ADC values of malignant tumors. However, a solid component with low signal intensity on T2-weighted images and DWI is an effective criterion for predicting the presence of benign disease (30). In Zhang’s study (16), after excluding cystadenofibromas, fibrothecomas, and Brenner tumors from their analysis, the sensitivity for distinguishing malignant from benign ovarian tumors improved from 66.7% to 97.7%. In this meta-analysis, substantial heterogeneity was found in the estimation of accuracy: the I2 was 63% for sensitivity. Therefore, a subgroup analysis was performed based on the histological architecture of benign ovarian tumors. In our subgroup analysis, the pooled sensitivity of surface epithelial type tumors was higher than that of mixed histological type tumors, demonstrating that histological type of the benign group may be the origin of the heterogeneity. Furthermore, quantitative ADC values were more helpful when applied to discriminate benign ovarian surface epithelial tumors from malignancies.
For discriminating borderline ovarian tumors from malignancies, the pooled sensitivity and specificity values of the included studies were 0.89 and 0.79, respectively, and the AUC was 0.91. These results indicated that quantitative ADC values are useful diagnostic parameters for distinguishing borderline from malignant ovarian lesions. Further subgroup analysis showed that b values in the range of 700–1000 s/mm2 may be more suitable for discriminating borderline from malignant ovarian tumors. To our knowledge, this is the first study to estimate the accuracy of discriminating borderline from malignant ovarian lesions.
A previous systematic review (31) for ovarian neoplasm characterization summarized ADC values without examining test performance. It demonstrated that the ADC values were not significantly different between malignant and benign ovarian neoplasms. This controversial conclusion may be due to the different inclusion criteria employed. The study evaluated the cystic or solid portion of ovarian neoplasms, while only the solid components were considered in our study. We also excluded lesions that exhibited high T1-weighted (T1W) signals on conventional MR sequences (teratomas, endometriomas, or dermoid cysts). This exclusion may be considered selection bias, but Moteki et al. (32) recommended that all tumors with high T1W signals should be excluded before DWI sequences, as they exhibit low ADC values. Furthermore, teratomas and endometriomas can be accurately diagnosed on conventional MRI and do not represent diagnostic challenges. Other studies (33–35) also demonstrated that DWI can differentiate malignancies from benign ovarian tumors. The evaluation methods in these previous studies were based on DWI sequences, a qualitative method that is particularly susceptible to researcher bias. In contrast, our study attempted to evaluate ovarian tumors using a quantitative method based on ADC values. Without standardized imaging parameters, some bias in the index test may occur; nevertheless, our findings support the need for prospective studies using uniform DWI parameters to establish the technology’s best use.
We should acknowledge several inherent limitations in the meta-analysis when interpreting these results. First, identifying the solid portions of tumors for ADC measurements was somewhat dependent on the availability of dynamic contrast-enhanced MR sequences. The diagnostic performance of DWI is relatively unclear without contrast-enhanced imaging, or as an independent test, although DWI is potentially useful when there are contraindications to gadolinium contrast agents. Optimizing the DWI protocol can minimize most of the challenges encountered during DWI acquisitions. Second, technical differences due to the equipment used or how trials were conducted seemed to have a major impact on the ADC values. To ensure that quantitative ADC values have similar indications across equipment vendors and institutions, it is absolutely necessary that there are agreements among all manufacturers on standards for both acquisition protocols, repeatability and post-processing procedures (36). Third, measurement bias existed. Both the region-of-interest (ROI) methods and inter-observer variability can influence the ADC values (37). Further investigations are needed to standardize ROI methods and to establish reproducible measurement methods for calculating ADC values. Fourth, the number of included studies for discriminating borderline from malignancies was limited; thus, more studies are needed to confirm the diagnostic value of quantitative ADC values in borderline vs. malignant ovarian tumors.
In conclusion, the current evidence showed that quantitative ADC values provide a high diagnostic value in ovarian tumors. Nevertheless, large-scale prospective multicenter clinical trials using standardized imaging parameters may help to guide the use of ADC values for characterizing ovarian tumors.
Supplemental Material
Supplementary Figure 1 -Supplemental material for Utility of DWI with quantitative ADC values in ovarian tumors: a meta-analysis of diagnostic test performance
Supplemental material, Supplementary Figure 1 for Utility of DWI with quantitative ADC values in ovarian tumors: a meta-analysis of diagnostic test performance by Shan Pi, Rong Cao, Jin Wei Qiang and Yan Hui Guo in Acta Radiologica
Supplemental Material
Supplementary Table 1 -Supplemental material for Utility of DWI with quantitative ADC values in ovarian tumors: a meta-analysis of diagnostic test performance
Supplemental material, Supplementary Table 1 for Utility of DWI with quantitative ADC values in ovarian tumors: a meta-analysis of diagnostic test performance by Shan Pi, Rong Cao, Jin Wei Qiang and Yan Hui Guo in Acta Radiologica
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of PR China (grant no. 81471628) and the Shanghai Municipal Commission of Health and Family Planning (grant nos. 2013SY075 and ZK2015A05).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.