
Abstract
Background
Intravoxel incoherent motion magnetic resonance imaging (IVIM-MRI) acquires tumor perfusion information without injection of contrast medium, which is promising in tumor assessment. However, its consistency with dynamic contrast-enhanced MRI (DCE-MRI), a more widely used method for tumor perfusion evaluation, is not revealed in rectal cancer.
Purpose
In this study, we aimed to investigate the correlation of perfusion-sensitive parameters derived from IVIM-MRI with DCE-MRI and measurement reproducibility of IVIM-MRI parameters in rectal cancer.
Material and Methods
Forty-seven rectal cancer patients underwent IVIM-MRI with 16 b-values and DCE-MRI. The perfusion fraction (f), pseudo-diffusion coefficient (D*), and f·D* were measured by two radiologists independently and correlated with the transfer constant (Ktrans), reflux constant (kep), and extravascular extracellular fractional volume (ve) obtained from DCE-MRI.
Results
Pearson’s correlation analyses of IVIM-MRI and DCE-MRI parameters showed fair to moderate correlation between f and Ktrans (r = 0.461, P = 0.001), followed by f and kep (r = 0.430, P = 0.003), f·D*, and Ktrans (r = 0.425, P = 0.003), f·D*, and kep (r = 0.384, P = 0.008). There was no significant correlation between ve and f, ve and D*, ve and f·D*, D* and Ktrans, and D* and kep. The reproducibility of IVIM-MRI measurements was moderate. For parameter f, intraclass correlation coefficient (ICC) = 0.71 (0.53–0.82), coefficient of variation (CV) = 13.05 ± 0.02%, limit of agreement (LoA) = −0.05–0.04; for parameter D*, ICC = 0.55 (0.32–0.72), CV = 20.28 ± 3.23%, LoA = −9.6–8.4.
Conclusion
Perfusion-sensitive parameters derived from IVIM-MRI correlated fairly to moderately with DCE-MRI in rectal cancer patients and showed moderate measurement reproducibility. IVIM-MRI supplements routine high-resolution MRI without contrast enhancement to provide information of tumor microcirculation.
Keywords
Introduction
Tumor angiogenesis and microvascular perfusion influence on the treatment strategy and prognosis of rectal cancer (1). However, it is still a challenge to evaluate tumor microcirculation before any treatment. Nowadays, dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI) allows qualitative and quantitative assessment of tumor microcirculation (2,3). The quantitative parameters derived from DCE-MRI based on a “two-compartment model” (4), including volume transfer constant (Ktrans), extravascular extracellular space (EES) fraction (ve), and reflux constant (kep), were reported to show not only blood volume but also microvascular permeability of various tumors (3,5,6). Unfortunately, DCE-MRI does not suit the patients with renal insufficiency because it needs intravenous injection of contrast agent (4).
Diffusion-weighted imaging (DWI) is a functional MRI sequence that quantifies Brownian motion of water molecules in tissue (7). Apparent diffusion coefficient (ADC) derived from DWI has been used to evaluate tumor cellular density in previous studies (8–10). Based on this theoretical principle, intravoxel incoherent motion MRI (IVIM-MRI) was introduced to quantify microscopic translational motions in each MRI voxel (11). By performing bi-exponential IVIM model fitting to the multiple b-value DWI data, IVIM imaging acquires simultaneously tumor diffusion and perfusion information without injection of contrast medium, which is especially valuable in patients with impaired renal function (11). Quantitative parameters of IVIM-MRI include: (i) perfusion factor (f ) that represents fraction of water flowing in the perfused capillaries; (ii) perfusion-related incoherent microcirculation known as pseudo-diffusion coefficient (D*); and (iii) true diffusion coefficient (D). The stability and reproducibility of IVIM-MRI perfusion-related parameters varied as reported in previous studies (12–14).
For this reason, we aimed to determine the correlation of perfusion-sensitive parameters derived from IVIM-MRI and DCE-MRI, and also to investigate the reproducibility of IVIM-MRI parameters.
Material and Methods
Patient population
This prospective study was approved by our institutional ethics review board and informed consent was obtained from each patient. From February to December 2015, 47 patients (27 men, 20 women; mean age = 57 ± 13 years; age range = 22–83 years) diagnosed with rectal cancer by endoscopic biopsy were recruited. All of them were free from history of pelvic surgery and contraindications to MRI examination. All included patients underwent IVIM-MRI and DCE-MRI simultaneously before surgery or neoadjuvant chemoradiotherapy (CRT).
MRI protocols
MRI was performed on a 3.0-T system (Magnetom Verio; Siemens Healthcare, Erlangen, Germany) using a standard six-element body-matrix coil centered over the pelvis. Patients were injected intramuscularly with 20 mg of anisodamine hydrochloride to minimize intestinal peristalsis and an appropriate amount (60–120 mL) of ultrasound gel was also poured into the rectum 5–10 min before examination to better outline the tumor. Routine MRI was performed with 3-mm slice thickness and no inter-slice gap including sagittal (TR/TE = 3000/87 ms, flip angle [FA] = 150°, field of view (FOV) = 180 × 180 mm, matrix = 256 × 320, acquisition time = 2 min 30 s, 19 slices) and coronal (TR/TE = 4000/77 ms, FA = 137°, FOV = 220 × 220 mm, matrix = 307 × 384, acquisition time = 2 min 52 s, 25 slices) T2-weighted (T2W) images followed by oblique T2W (TR/TE = 3000/84 ms, FA = 150°, FOV = 180 × 180 mm, matrix = 320 × 320, acquisition time = 3 min 18 s, 24 slices) and T1-weighted (T1W) (TR/TE = 644/12 ms, FA = 120°, FOV = 180 × 180 mm, matrix = 320 × 320, acquisition time = 3 min 17 s, 20 slices) sequences angulated perpendicular to the long axis of the tumor.
IVIM-MRI was then performed with single-shot spin-echo echo-planar-imaging (SS-SE-EPI) sequence (TR/TE = 3800/74.4 ms, FOV = 245 × 300 mm, acquisition time = 6 min 1s, slice thickness = 6 mm, number of excitations = 2), 16 b-values (0, 5, 10, 20, 30, 40, 60, 80, 100, 150, 200, 400, 600, 1000, 1500, 2000 s/mm2), and parallel imaging acceleration factor of 2.
DCE-MRI was performed using a three-dimensional (3D) dynamic sequence with high spatial and temporal resolution based on time-resolved technique with interleaved stochastic trajectories (3D-TWIST). After intravenous injection of 0.1 mmol/kg body weight of gadopentetate dimeglumine using a power injector at a rate of 3.0 mL/s followed by 25 mL saline flush, axial 3.6-mm thick images were obtained in 75 dynamic phases with 4.25 s temporal resolution (TR/TE = 4.83/1.87 ms, FA = 12°, FOV = 260 × 260 mm, matrix = 192 × 192, acquisition time = 5 min 24 s). Post-contrast coronal 3D T1W images (TR/TE = 10.0/4.9 ms, FA = 10°, FOV = 380 × 200 mm, matrix = 384 × 384, acquisition time = 3 min 10 s, 144 slices) with 1.0-mm slice thickness and 0.2-mm slice interval were also obtained after DCE-MRI.
MRI post-processing
IVIM-MRI data were processed using a prototype post-processing software-based MATLAB (Mathworks, Natick, MA, USA) with a segmented bi-exponential fitting algorithm. A voxel-by-voxel fitting of IVIM data was performed on the basis of the following equation:

DCE-MRI data were analyzed by commercial software Tissue 4D (Siemens Healthcare, Erlangen, Germany) in Siemens Workstation. Three permeability parameters maps (Ktrans map, ve map, and kep map) were automatically generated and the mean value of each permeability parameter within the drawn ROI was recorded.
Using corresponding axial T2W images as reference, three irregular ROIs were placed to include most of the solid tumors on DCE-MR images and IVIM-MR images, respectively (Figs. 1 and 2), which ensured ROIs were selected the same as possible for the two methods. The mean value of each permeability parameter within a ROI on DCE-MR images was recorded. Meanwhile, f and D* were measured in a ROI and multiplied to obtain f·D* on IVIM-MR images. The values of three ROIs were averaged for each patient. Furthermore, IVIM-MRI was processed independently by two radiologists with 20 and 4 years of experience in MRI to determine inter-observer reproducibility.
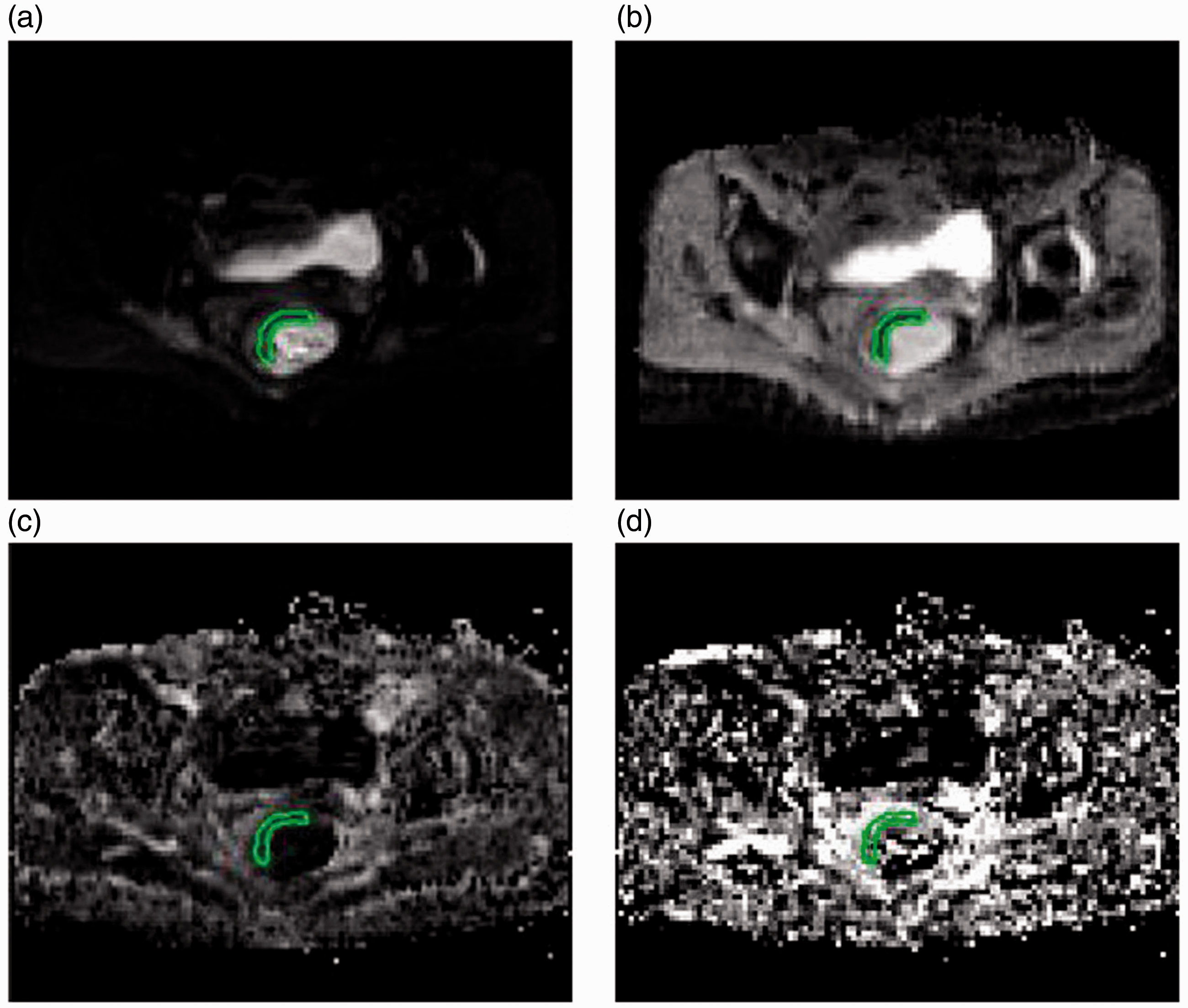
A 72-year-old woman with stage IIA (pT3N0M0) rectal cancer. (a) Axial T2W image shows right anterolateral mural tumor. (b) ROIs are placed within the tumor (red and green), normal rectal wall (yellow), and gluteus maximus muscle (blue) on DCE-MR image and (c) concentration-time curves are generated. (d) Volume of interest is selected and (e) Ktrans parametric map is generated using the Tofts model showed in (f); (g) DCE-MR image where the first ROI is placed; (h) perfusion parameters including Ktrans, kep, and ve are calculated and present for the ROI outlined with red dotted line; and (i) T2W image where the first ROI is placed. IVIM-MRI of the same patient showed in Fig. 1. Using axial T2W imaging and (a) SS-SE-EPI at b = 0 s/mm2 as reference, ROIs are placed on the right anterolateral mural tumor to measure the true diffusion coefficient (b), fraction of diffusion linked to microcirculation (c), and pseudo-diffusion coefficient (d) on the corresponding D, f, and D* parametric maps, respectively.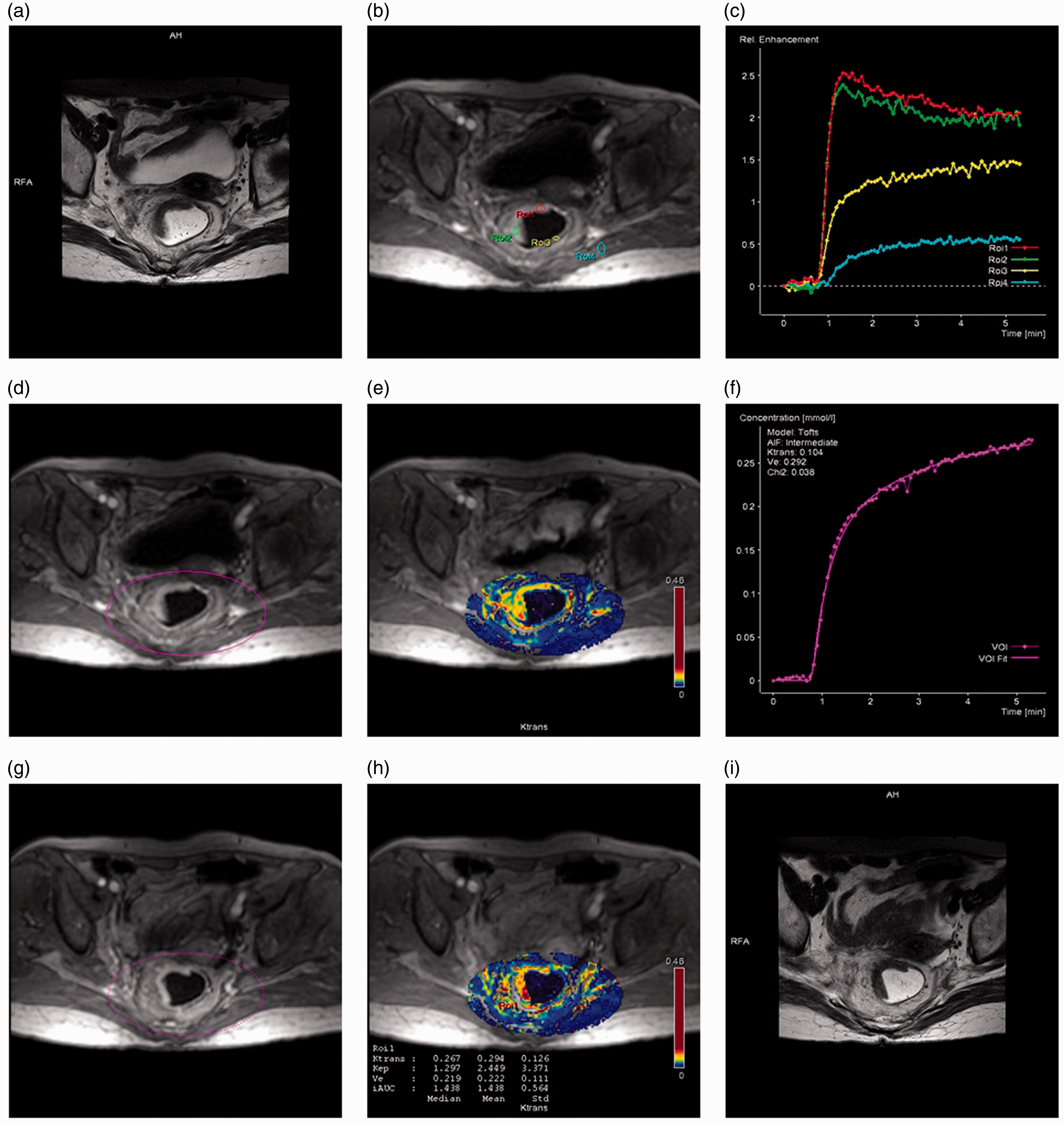
Statistical analyses
Statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS, version 13.0, Chicago, IL, USA) and MedCalc Statistical Software (version 14.8, Ostend, Belgium).
Pearson’s correlation test was used to assess the association between IVIM-MRI and DCE-MRI parameters. A coefficient r value < 0.2 indicates poor correlation; 0.2–0.4, fair; 0.41–0.6, moderate; 0.61–0.8, good; and >0.8, excellent.
Two methods were introduced to evaluate IVIM measurement reproducibility. First, intraclass correlation coefficient (ICC) and coefficient of variation (CV) were calculated. As given by Cicchetti (15), an ICC value < 0.40 indicated poor inter-rater agreement; 0.40–0.59, fair; 0.60–0.74, good; and 0.75–1.00, excellent. CV in the range of 10–25% was similarly interpreted as moderate reproducibility according to that reported in previous studies (13,16). Second, Bland–Altman plots were constructed and limits of agreement (LoAs) based on the plots were estimated.
Results
Quantitative parameters
IVIM-MRI and DCE-MRI perfusion-sensitive parameters in 47 patients with rectal cancer.
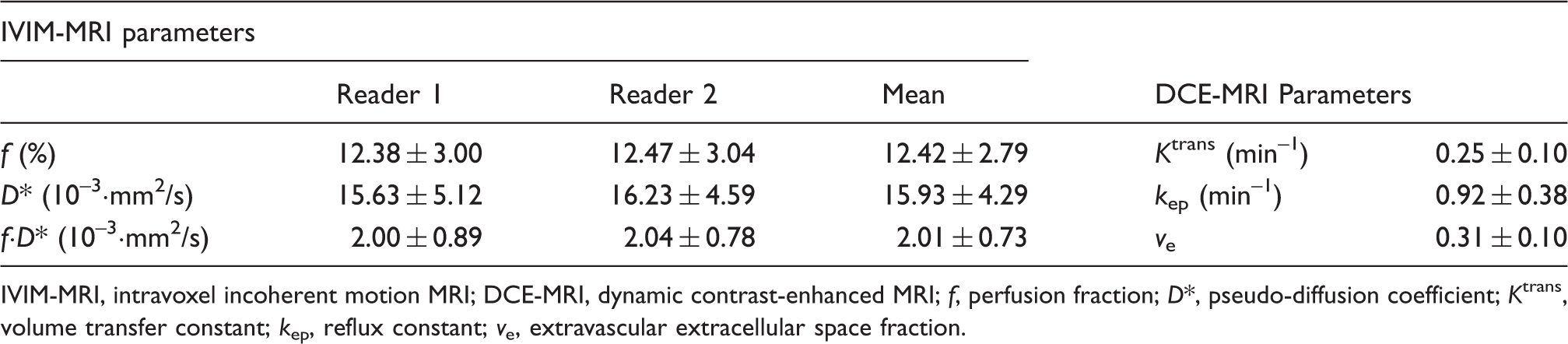
IVIM-MRI, intravoxel incoherent motion MRI; DCE-MRI, dynamic contrast-enhanced MRI; f, perfusion fraction; D*, pseudo-diffusion coefficient; Ktrans, volume transfer constant; kep, reflux constant; ve, extravascular extracellular space fraction.
Correlation analyses
Correlations between perfusion-sensitive parameters derived from IVIM-MRI and DCE-MRI in 47 patients with rectal cancer.
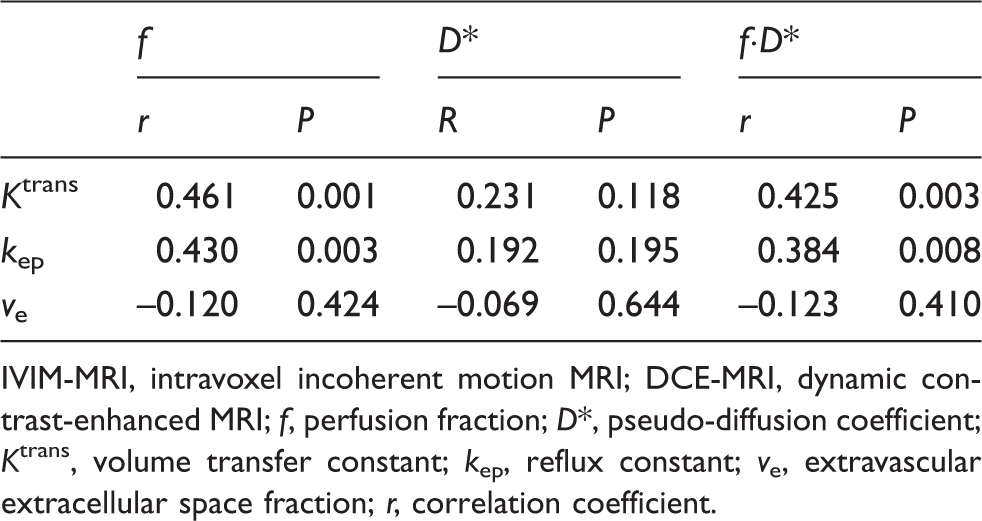
IVIM-MRI, intravoxel incoherent motion MRI; DCE-MRI, dynamic contrast-enhanced MRI; f, perfusion fraction; D*, pseudo-diffusion coefficient; Ktrans, volume transfer constant; kep, reflux constant; ve, extravascular extracellular space fraction; r, correlation coefficient.
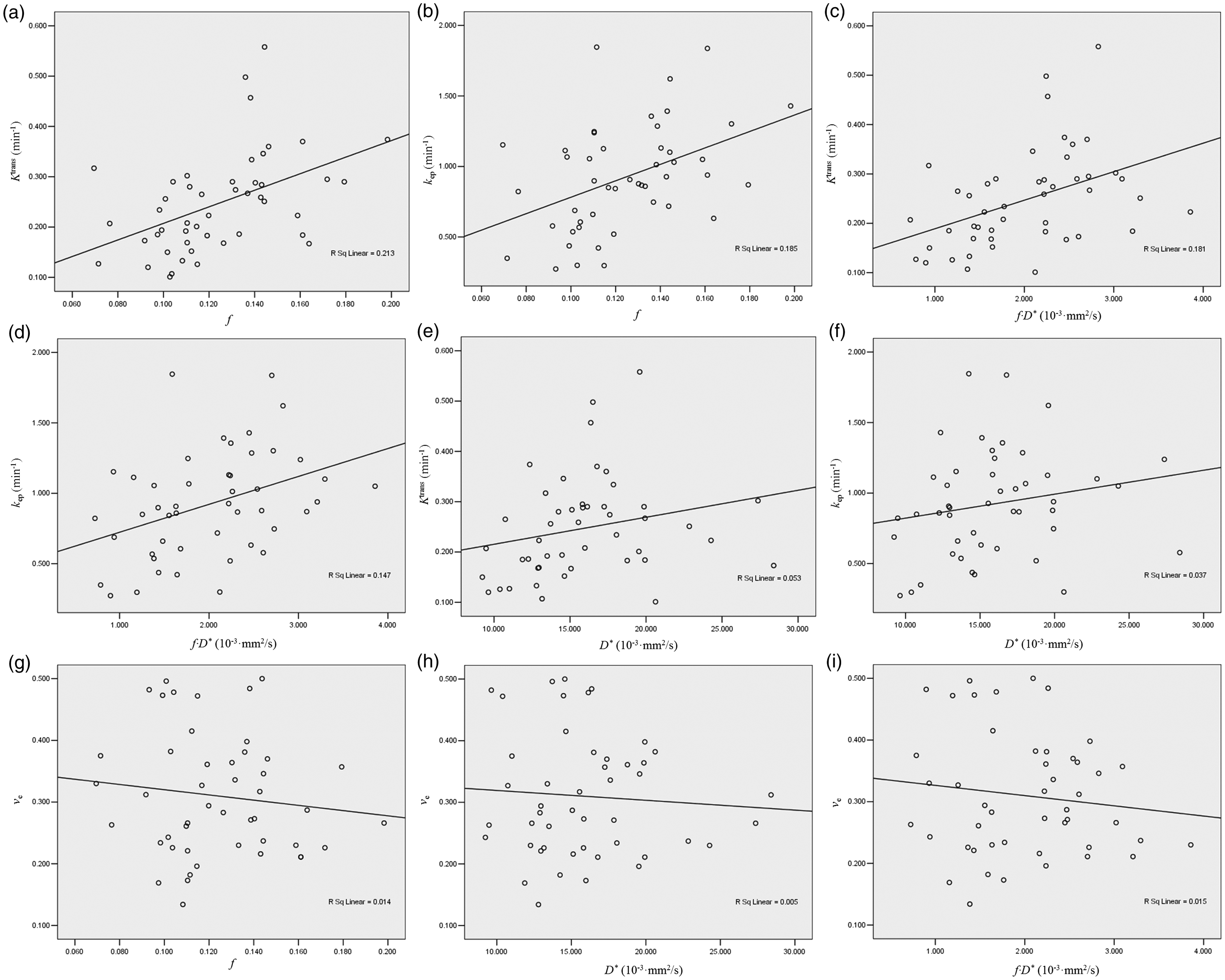
Scatter plots of parameters derived from DCE-MRI and IVIM-MRI show highest correlation (a) between f and Ktrans (r = 0.461, P = 0.001), followed by (b) f and kep (r = 0.430, P = 0.003), (c) fċD* and Ktrans (r = 0.425, P = 0.003), (d) fċD* and kep (r = 0.384, P = 0.008). There was no significant correlation (e) between D* and Ktrans (r = 0.231, P = 0.118), (f) D* and kep (r = 0.192, P = 0.195), (g) ve and f (r = –0.120, P = 0.424), (h) ve and D* (r = –0.069, P = 0.644), and (i) ve and f·D* (r = –0.123, P = 0.410).
Reproducible analyses
Inter-reader reproducibility of IVIM-MRI parameters in 47 patients with rectal cancer.
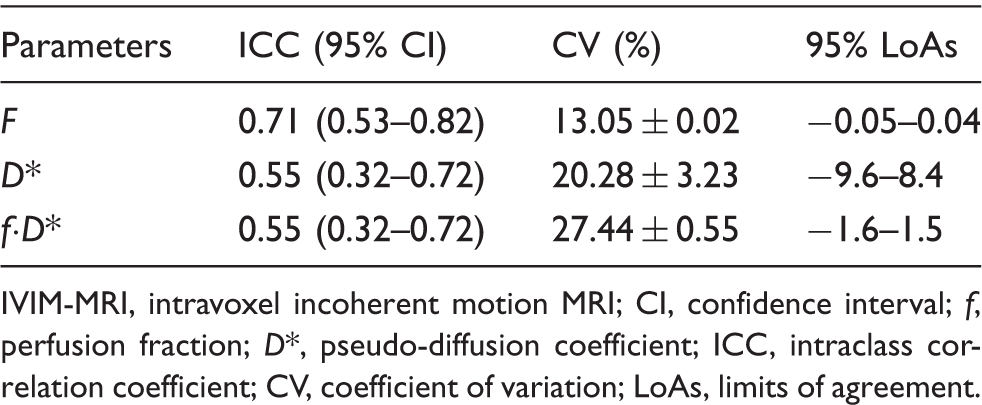
IVIM-MRI, intravoxel incoherent motion MRI; CI, confidence interval; f, perfusion fraction; D*, pseudo-diffusion coefficient; ICC, intraclass correlation coefficient; CV, coefficient of variation; LoAs, limits of agreement.
The Bland–Altman plots of IVIM-MRI parameters showed no relationship between discrepancy and the level of measurement (Fig. 4), so that the LoAs were valid (Table 3). Compared with the mean value of each parameter, values of their 95% LoAs indicated mild absolute inter-reader variability for parameter f and moderate variance for parameters D* and f·D*.
Bland–Altman plots of f (a), D* (b), and f·D* (c) show inter-reader variance of IVIM-MRI measurements. Central line reflects mean difference, top and bottom lines correspond to 95% limits of agreement.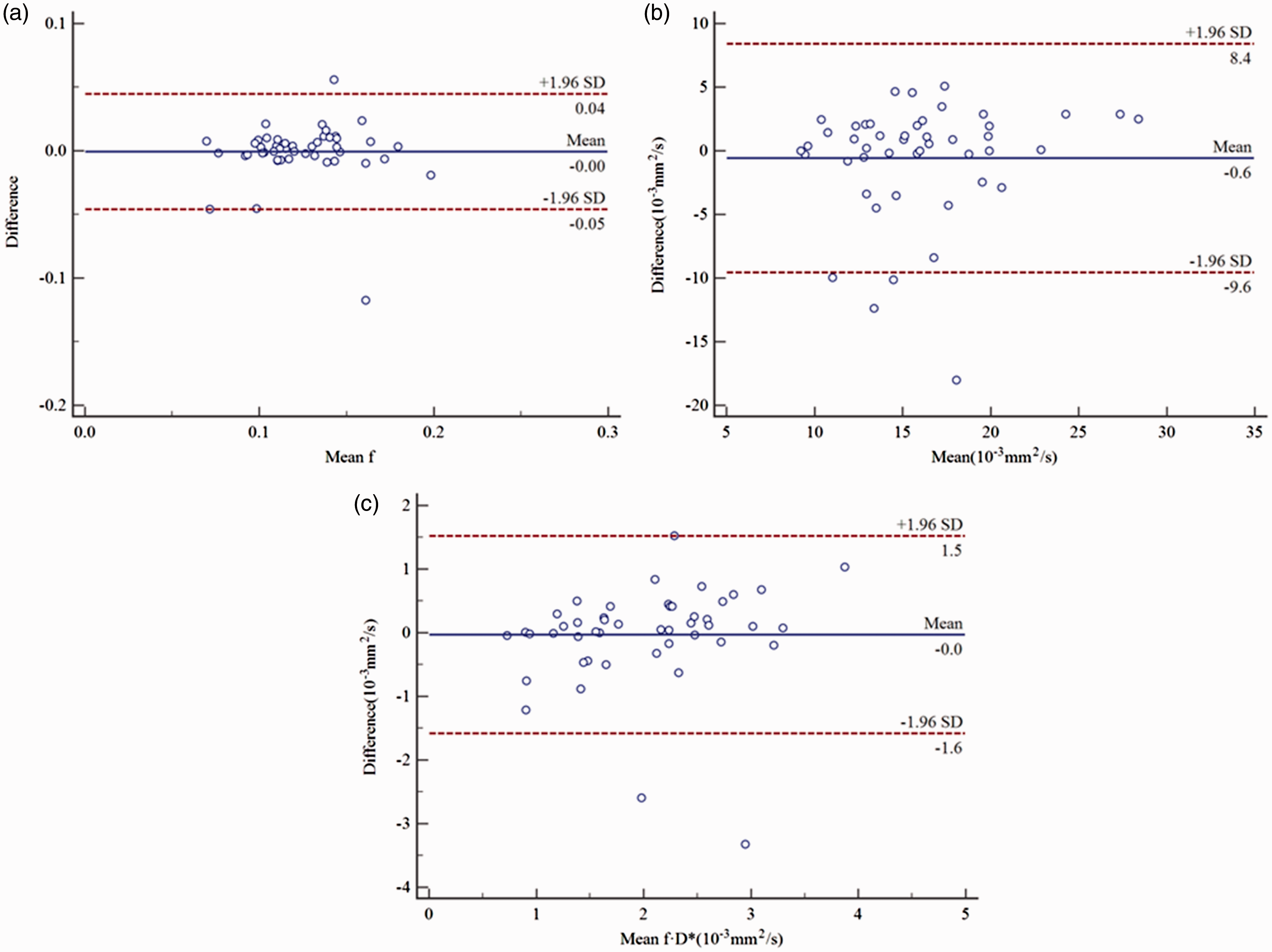
Discussion
Pelvic MRI has been recommended as a routine examination before surgery in the rectal cancer guidelines of the National Comprehensive Cancer Network (NCCN) (17), although it is insufficient in providing tumor pathophysiological information. However, angiogenesis plays a central role in tumor therapy (18). With the increasing use of antivascular drugs and preoperative CRT in locally advanced rectal cancer (19–22), microcirculation might be a key point in evaluating therapeutic response. Vascular endothelial growth factor (VEGF) has been reported as a microvascular related biomarker accessing the response to CRT (23), but immunohistochemistry is invasive and in vitro.
A few previous studies (3,24) have evaluated tumor microcirculation by using non-invasive methods in vivo, such as DCE-MRI and IVIM-MRI. It comes to a consistence that tumor with abundant blood supply has higher Ktrans and kep than normal tissue, the same as D* and f (4,11). DCE-MRI or IVIM-MRI has been reported separately to estimate tumor perfusion in rectal cancer (11,25–28), but we still do not know the relationship between these parameters clearly.
In this study, we performed both DCE-MRI and IVIM-MRI on the same patients to correlate the perfusion parameters of these two techniques. It was found that f and f·D* from IVIM-MRI correlated fairly to moderately with Ktrans and kep from DCE-MRI.
Ktrans and kep reflect the contrast agent volume transfer between capillaries and EES, which are determined by tissue blood volume and microvascular permeability (4). IVIM model fitting assumes perfusion or microcirculation of blood in the capillary network to be an incoherent motion due to the pseudorandom organization of capillary network at the voxel level. Water flowing in these randomly oriented capillaries mimics Brownian motion and contributes to the diffusion measured by DWI. The fraction of diffusion linked to this capillary perfusion is measured as parameter f whereas D* represents the combination of true diffusion and perfusion fraction (11). Therefore, f and D* are mainly affected by the volume of blood flowing inside the capillaries. Because Ktrans and kep are also influenced by tissue blood volume, they were found to correlate with f and f·D* in our study. However, Ktrans and kep are also affected by microvascular permeability. Therefore, the correlation of perfusion parameters from DCE-MRI and IVIM-MRI measured in our study was fair to moderate but not good. This result was similar to a previous cervical cancer study (29).
It was a pity that we did not find correlation between D* and DCE-MRI parameters. On one hand, D* includes true diffusion and perfusion fraction, which means perfusion contributes a part of the value. On the other hand, D* is quite sensitive to noise; as a result, the value measured for D* is not stable. Similarly, the lack of correlation between ve and IVIM-MRI parameters was related to the extravascular extracellular volume assessment in ve, which could not be evaluated by f and D*.
Although reproducibility of IVIM-MRI parameters has been reported to be variable in nasopharyngeal carcinoma and hepatocellular carcinoma (13,16,30), we found moderate to good inter-observer reproducibility of the perfusion factor f in rectal cancer. This might be related to anisodamine hydrochloride and ultrasound gel preparation that allowed clear demonstration of tumor and normal rectal wall. The reproducibility of the D* measurement was suboptimal due to the limited perfusion signal in the low b-value and was also reported in previous studies (16,30).
Because MRI of rectal cancer is usually recommended to be performed without contrast enhancement for pre-operation evaluation (31), IVIM-MRI is able to assess both perfusion and diffusion in this condition. In our study, we found a fair to moderate correlation between perfusion parameters derived from IVIM-MRI and those of DCE-MRI reflecting different aspects of tumor perfusion. Moreover, the perfusion factor f showed moderate to good inter-observer reproducibility. Thus, we conclude that IVIM-MRI provided perfusion information of tumor microcirculation without intravenous contrast media injection. It perhaps supplements routine MRI in a non-invasive way.
Our study is limited by the small study cohort of 47 patients and a lack of the correlation with immunohistochemical results such as microvessel density (MVD) and VEGF. Although the ROIs were drawn to include most of the tumors, tumor heterogeneity should be evaluated using voxel-by-voxel measurements of the entire tumor.
In conclusion, perfusion parameters derived from IVIM-MRI were moderately reproducible and correlated fairly to moderately with DCE-MRI. Currently IVIM-MRI without contrast enhancement provides microcircular information as a non-invasive examination. It supplements routine MRI in rectal cancer patients with renal insufficiency. This study merely seemed to be a pilot, but we cumulated experiences from it for further study. In the next stage, we aim to modify IVIM-MRI protocol and then try to use it to evaluate and monitor the therapeutic response of CRT in rectal cancer. It might bring benefits to clinical treatment strategy.
Footnotes
Acknowledgments
The authors thank Dr Pui Margaret Hing Wah and Yan Xu for their great help in the precious suggestions and revisions on the earlier drafts.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Supported by Science and Technology Planning Project of Guangdong Province, China (No. 2014A020212126).