
Abstract
Background
Percutaneous therapy with various sclerosants is an established treatment of venous malformations in general. We investigated the safety and effectiveness of polidocanol in the craniofacial region.
Purpose
To present and evaluate our subjective and objective mid- and long-term results of patients with craniofacial venous malformations (CFVM) after percutaneous sclerotherapy using polidocanol.
Material and Methods
Twenty patients with CFVM treated by percutaneous sclerotherapy were followed up and asked to fill in a questionnaire comparing levels of the following CFVM-related symptoms before and after treatment: pain; functional impairment; cosmetic deformities; and impairment in daily life. Additionally, both size reduction as well as procedural-related complication rates were analyzed.
Results
Evaluation of the questionnaire revealed an improvement or complete relief of CFVM-related symptoms with significant reduced impairment in daily life after percutaneous sclerotherapy. Eighteen (90%) patients noticed a post-sclerotherapy improvement of at least one of their corresponding symptoms and expressed satisfaction with regard to their treatment. For 13 patients, a > 50% size reduction of the CFVM could be observed, while seven exhibited a < 50% size reduction. One minor complication was encountered in 56 treatment sessions (1.8%).
Conclusion
Percutaneous sclerotherapy using polidocanol is a well-tolerated treatment for CFVM with a low complication rate. Size reduction and positive results with improvement of different clinical symptoms can be achieved.
Introduction
Venous malformations (VM) are one of the most common vascular malformations, of which >40% are located in the head and neck region. VM are congenital vascular lesions composed of dysmorphic venous channels lined by flattened, but mature endothelium and deficiencies of smooth muscle cells (1). Patients usually present with soft-tissue masses that increase with Valsalva maneuver, crying, or bending over. Symptoms of craniofacial venous malformations (CFVM) vary and range from asymptomatic lesions to cosmetic complaints and severe clinical symptoms including pain and swelling. CFVM, moreover, can complicate speech and breathing as well as swallowing. CFVM do not regress spontaneously and tend to enlarge over time. They can become more symptomatic and may require treatment. Percutaneous sclerotherapy is a well-established treatment option of CFVM. In the majority of cases, patients tend to have a long medical history and distinct psychosocial burden (2–4). Considering this context, patient satisfaction and improvement of CFVM-related clinical symptoms are recognized as very important outcomes (5). The aim of this study was to analyze the CFVM-related symptoms before and after percutaneous sclerotherapy with polidocanol and to evaluate both size reductions and procedural-related complications in a single center.
Material and Methods
Patients
Out of our database with 70 vascular anomalies of the head and neck region, we retrospectively reviewed all medical files of patients diagnosed with CFVM. We identified 20 patients who were treated in our department between 2003 and 2016. Written informed consent was obtained from all patients who were in scope for this study, as well as the approval from the local hospital’s institutional review board. The following clinical data attributes were taken from the patients’ medical files: demographics; location of the venous malformation; total number of treatments; type of sclerosant agents; and age at the beginning of treatment. The exact localization and extent of the VM were analyzed before the percutaneous treatment with magnetic resonance imaging (MRI) (Figs. 1 and 2). Arteriovenous, lymphatic, or any combined vascular malformations as well as hemangiomas were excluded from the study. According to the classification system for venous malformations, described by Puig et al., we categorized the CFVM in four types based on the drainage pattern on direct puncture phlebography images (6).
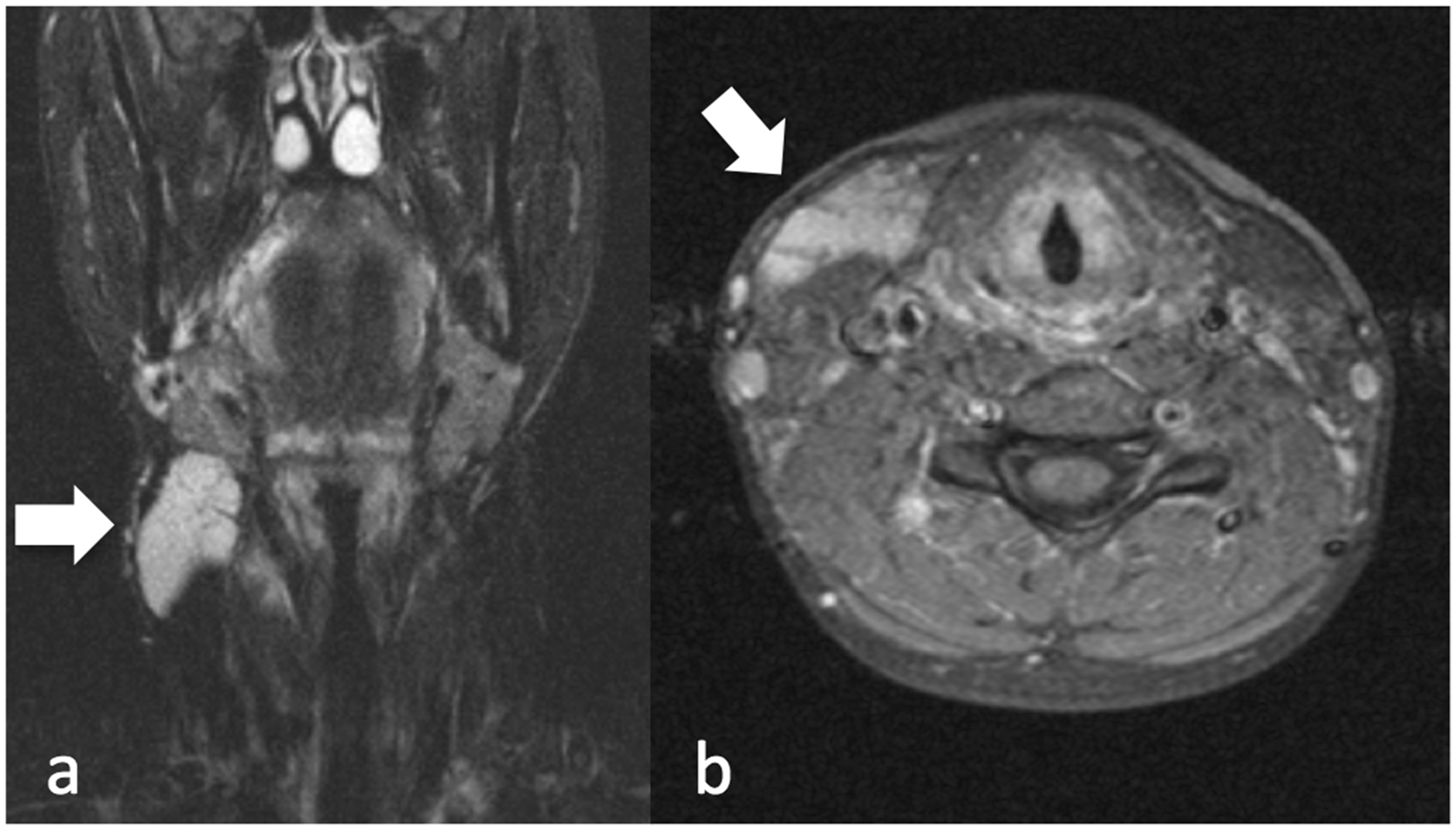
A young female patient presented with a small but painful and disturbing swelling and redness of the right submandibular region. (a) Coronal short T1 inversion recovery (STIR) and (b) axial T1W fat-saturated MRI with contrast showing a right submandibular vascular anomaly (arrows). The VM typically presents hyperintense on STIR sequences and with a strong contrast enhancement.
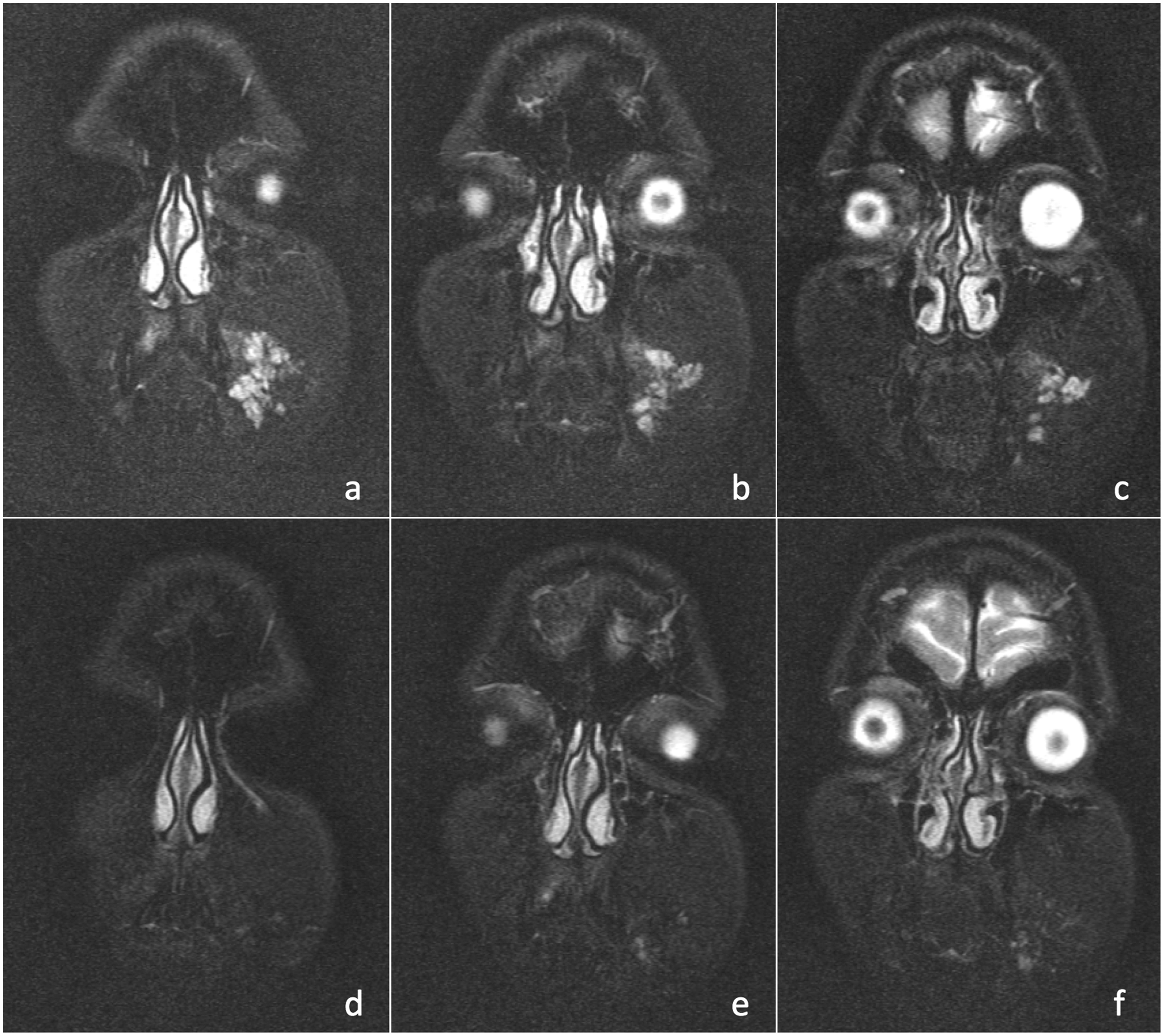
A young patient presented with a cosmetically impairing lesion of the left cheek that caused a psychosocial burden with impairment in daily life. Coronal STIR weighted images (a–c) before and (d–f) after percutaneous sclerotherapy showing a hyperintense left buccal lesion, suspicious for a CFVM. Post-sclerotherapy MRI demonstrates marked size reduction of the CFVM (d–f).
Patients were followed up and retrospectively analyzed by a questionnaire focused on clinical symptoms. Furthermore, procedural-related complications were collected. Size and extension of CFVM were evaluated with physical examination performed by the interventionalist and the referring physician (e.g. vascular surgeon, pediatrician) and with MRI reviewed in consensus by two experienced neuroradiologists.
Pre- and post-treatment MRI included at least the following sequences: axial T1-weighted (T1W) imaging; axial and coronal contrast-enhanced fat-suppressed T1W; short T1 inversion recovery (STIR), or fat-suppressed T2-weighted (T2W) imaging in all three planes. The latter two sequences are known to provide a high accuracy in demonstrating the extension of soft-tissue vascular malformations (7,8). We measured the longest dimensions of the lesions in three axes from two or more MRI planes to estimate the pre- and post-treatment size of the lesions. Post-treatment size reduction was calculated by comparing the pre- and post-treatment MRI images.
Outcome evaluation
The patients were followed up and asked to fill in a self-developed questionnaire after they agreed to participate in this study. The questionnaire evaluated specific, CFVM-related symptoms before and after percutaneous sclerotherapy, which contained the following different categories: pain; functional impairment; cosmetic deformities; and impairment in daily life. Patients were asked to compare their symptoms before and after sclerotherapy, assigning a grade on a five-point scale, respectively: score of 1 = worsening of symptoms; 2 = no change in symptoms; 3 = minor improvement of symptoms; 4 = major improvement of symptoms; 5 = complete relief of symptoms. Additionally, patients were asked whether any side effects or complications had occurred and if they were satisfied with the treatment.
Percutaneous sclerotherapy
All patients diagnosed with CFVM were treated with percutaneous sclerotherapy. All therapeutic procedures were performed under general anesthesia on a mono- or biplane c-arm angiography system (Siemens Axiom Artis dTA and BA; Siemens Medical Systems, Erlangen, Germany). The CFVM were treated applying the percutaneous sclerotherapy under gravity technique. The sclerosant agent we used was polidocanol at a concentration of 3%. Initially, the lesions were percutaneously punctured with a very small cannula (in the range of 22–27 G) attached to a connecting tube. The correct position of the needle was confirmed by blood return under gravity. Before injecting polidocanol, a phlebography run, using water-soluble iodinated contrast material in DSA technique, was performed. This demonstrated the drainage of the VM and could possibly reveal a risky drainage towards a dangerous intracranial structure such as the cavernous sinus (Figs. 3a, 4a, and 4b). When the needle was positioned correctly in the VM, polidocanol was injected under slow simultaneous subtracted fluoroscopy. Injections were performed after diluting the detergent with additional air into the syringe producing a foam at a ratio of 1:4 volume liquid sclerosant to volumes of air. It displaced the previously injected contrast material and appeared as a negative white contrast on simultaneous fluoroscopic subtraction, similar to the technique described by Agid et al. (4) (Figs. 3b, 4c, and 4d). The volume of the injected sclerosant agent did not exceed 5 mL in children and 10 mL in adults per treatment session. A minimum waiting period of three months between each sclerotherapy session was planned to allow swelling and inflammation of the treated region to decrease. Continuous sclerotherapy sessions were repeated, either until the patient was symptom-free, could tolerate residual symptoms, or until the treating interventionalist was not able to identify any further treatable venous pouches.
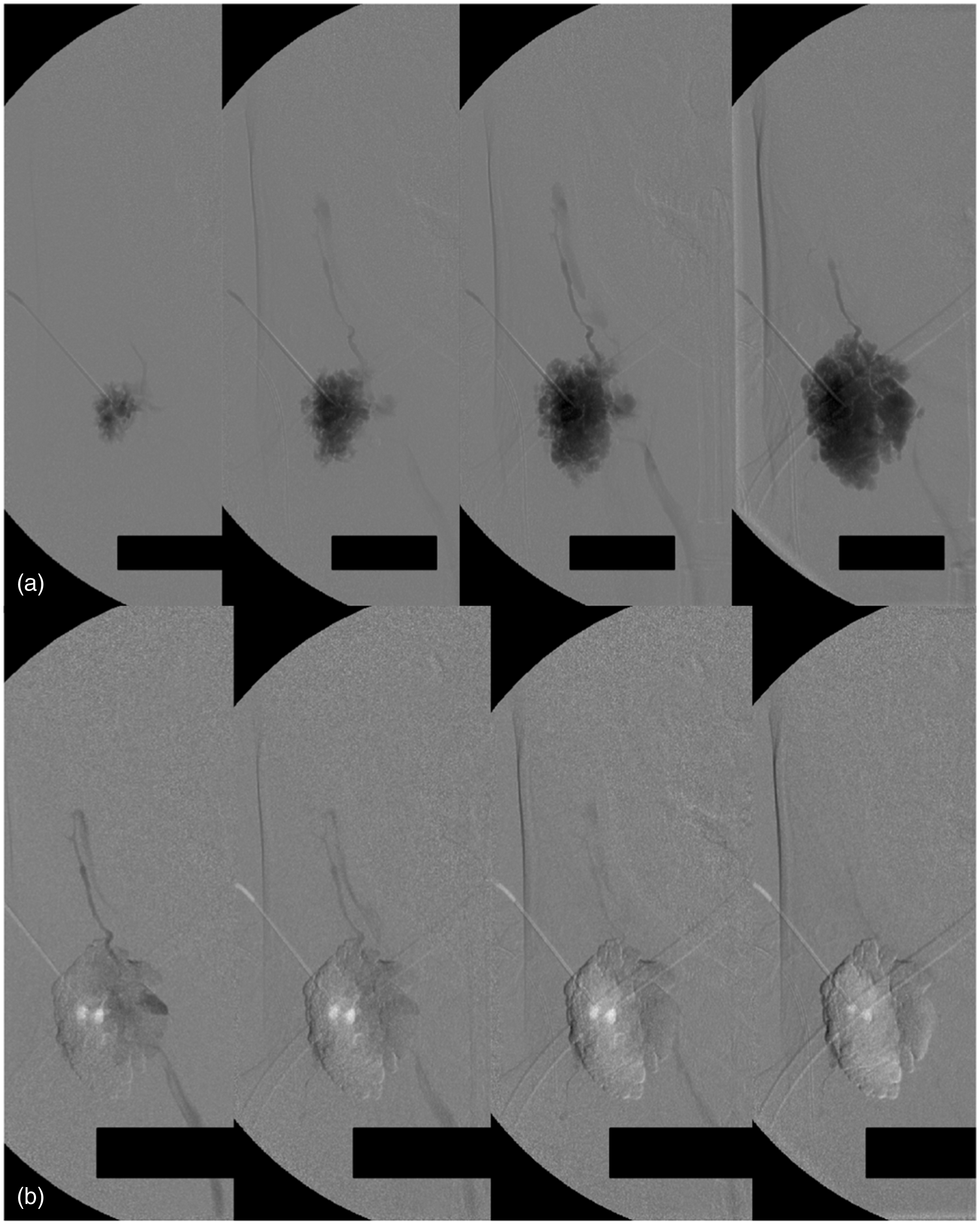
Direct puncture phlebography (anteroposterior [AP] view) of the right submandibular type-II VM (a) demonstrating the venous drainage before sclerotherapy. Percutaneous sclerotherapy (AP view) of the VM with polidocanol (b) showing washout of contrast material and negative white contrast of the sclerosant agent on DSA. Two sessions of percutaneous sclerotherapy with polidocanol were performed over a period of seven months. After treatment, the patient noted a clear improvement of cosmetic aspects with decrease of redness and swelling.
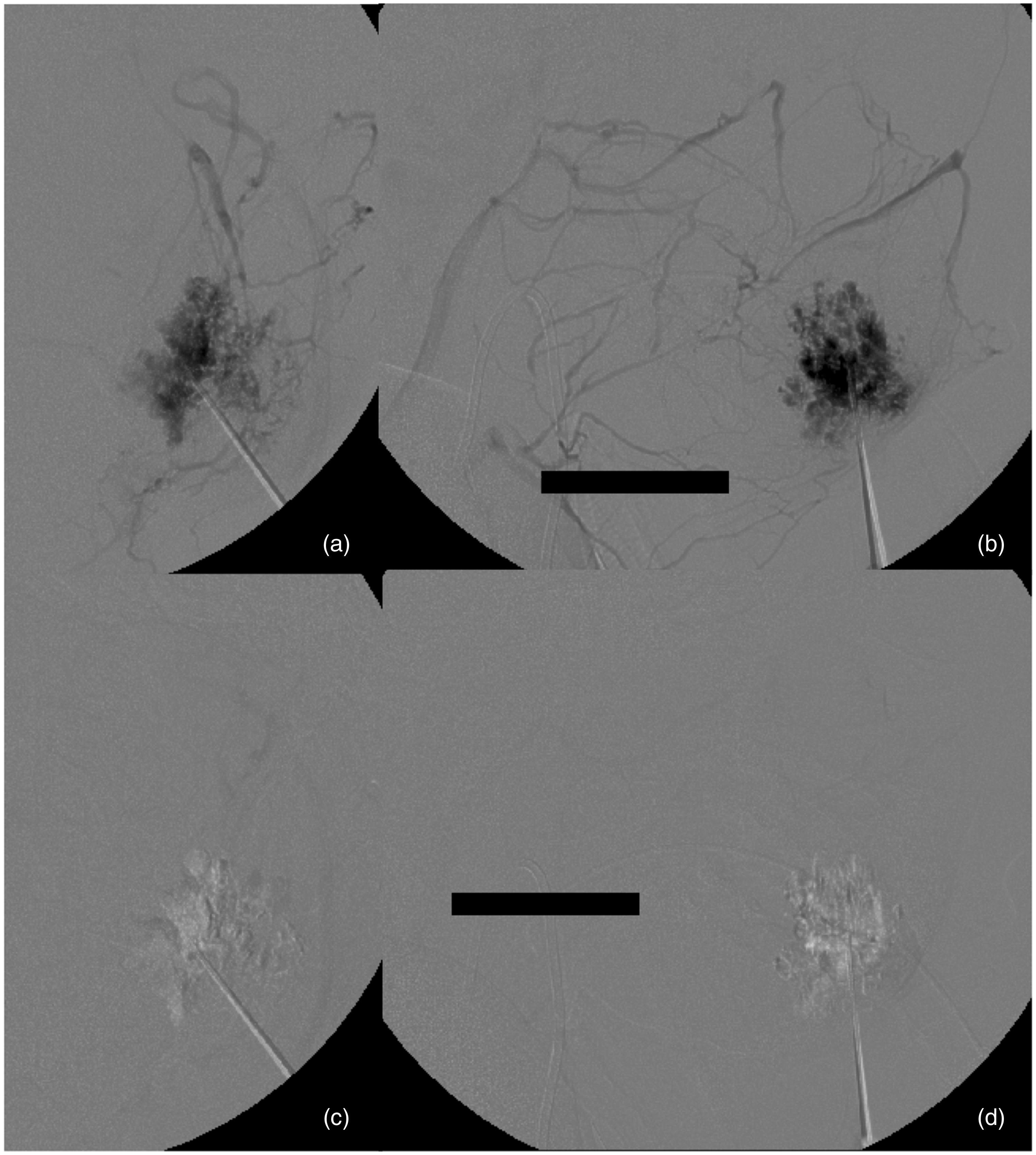
Direct puncture phlebography, AP (a) and lateral (b) projections, of the left type-II buccal VM before sclerotherapy showing the extensive facial venous drainage. Percutaneous sclerotherapy, same projections (c, d) demonstrating typical washout of contrast material after injection of polidocanol. The patient was treated by percutaneous sclerotherapy with polidocanol in five sessions over a period of three years. The patient noted a clearly visible decrease of the lesion. No more psychosocial burden with impairment in daily life was reported.
Statistical analysis
Statistical analyses were performed using SPSS 20.0 (SPSS Inc., Chicago, IL, USA) and SAS 9.2 (SAS Institute, Cary, NC, USA). To assess the significance of the difference between the pre- and post-sclerotherapy clinical results, paired nominal data were matched with the Mc Nemar test. A P value <0.05 was considered statistically significant.
Results
Twenty patients with CFVM were evaluated. Three patients were categorized as type-I VM (15%), nine patients as type-II VM (45%), five patients as type-III VM (25%), and, lastly, three patients as type-IV VM (15%). Most of our patients were treated in multiple staged sessions. The total number of treatment procedures was 56 (mean = 2.8 per patient; range = 1–10 sessions). The follow-up period was defined as time between first treatment and date of response date of the questionnaire. The mean follow-up period was 53 months (range = 7–133 months; median = 39 months) (Suppl. Table 1). Patients were contacted by telephone and asked to complete the questionnaire. Eleven patients presented with symptoms that had begun immediately after birth. Two patients have had symptoms since their early childhood. Six patients developed symptoms during puberty or shortly thereafter and only one patient reported onset of symptoms due to the VM at the beginning of the fourth decade of life. The mean age at the beginning of treatment was 25 years.
Symptoms before and after sclerotherapy.
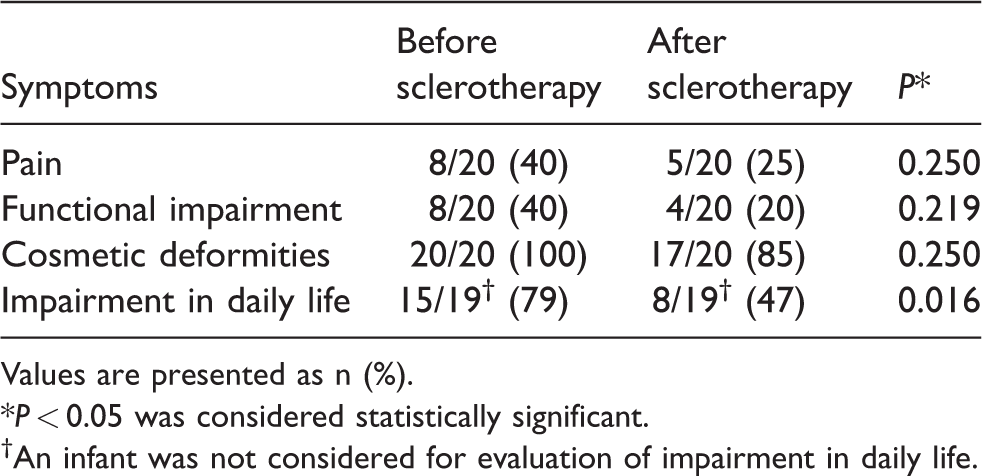
Values are presented as n (%).
*P < 0.05 was considered statistically significant.
†An infant was not considered for evaluation of impairment in daily life.
All patients complained about cosmetic deformities regardless of location or size of the VM. Eight patients specified pain as a leading symptom. Functional impairments were also noticed in eight VM patients. Suppl. Table 1 gives an overview of patients’ presenting symptoms and locations of the VM. Some patients had previously undergone laser therapy or surgical excision that mostly had not improved satisfaction.
All 20 patients completed the questionnaire and were included in this evaluation. Pre- and post-sclerotherapy levels of pain, functional impairment, cosmetic deformities, and impairment in daily life were evaluated. The presence of these CFVM-related symptoms before and after sclerotherapy was statistically compared using the McNemar test (P < 0.05 was considered statistically significant) (Table 1). Changes of patients’ subjective symptoms after sclerotherapy according to the five-point scale are listed in Table 2.
Changes of subjective symptoms after sclerotherapy.
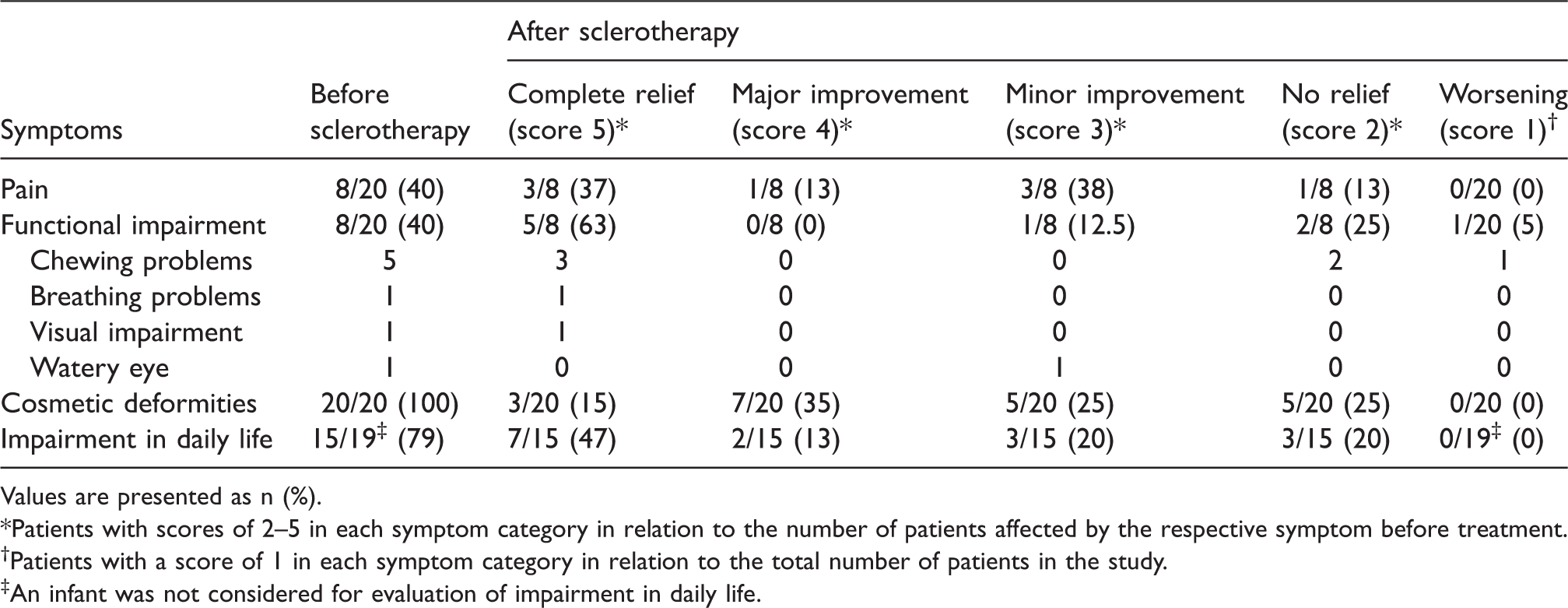
Values are presented as n (%).
*Patients with scores of 2–5 in each symptom category in relation to the number of patients affected by the respective symptom before treatment.
†Patients with a score of 1 in each symptom category in relation to the total number of patients in the study.
‡An infant was not considered for evaluation of impairment in daily life.
Eighteen of 20 patients (90%) experienced a complete relief or improvement of at least one of their respective symptoms after treatment. Two patients (10%) reported no change in any symptoms category. One patient (5%) complained about a post-sclerotherapy worsening of symptoms. She noticed newly emerged chewing problems after sclerotherapy but had a post-sclerotherapy improvement in two other symptoms categories.
Eight out of 20 patients (40%) complained of pain before treatment; seven of them reported a complete relief or improvement after sclerotherapy. Eight out of 20 patients (40%) reported functional impairment before treatment. A post-sclerotherapy complete relief or improvement could be seen in six of them. All 20 patients (100%) presented with cosmetic concerns, 15 of them reported a complete relief or improvement after treatment. Fifteen out of 19 patients (79%) complained about impairment in daily life. After treatment, 12 of them noticed a complete relief or improvement. The difference between pre- and post-sclerotherapy impairment in daily life was statistically significant (P = 0.016). One infant was not considered for evaluation of impairment in daily life.
Thirteen patients showed a > 50% reduction of the CFVM on post-sclerotherapy physical examination and on follow-up MRI (Suppl. Table 1) (Fig. 2). Among them, 11 had a complete relief or improvement of at least one of their presenting symptoms after treatment.
Eighteen of the 20 (90%) patients were satisfied with their percutaneous sclerotherapy. Only one treatment-related complication was noted in 56 treatment sessions (1.8%). One patient with a CFVM of the cheek developed persistent hypertrophic scars after two sessions of percutaneous sclerotherapy with polidocanol.
Discussion
The classification for vascular malformations was recently updated by the International Society for the Study of Vascular Anomalies (ISSVA) (9). Although vascular malformations are already present at birth, they continue to increase in size especially during periods of life with hormonal changes. In some cases, they even grow throughout the patient’s lifetime. The clinical manifestation of CFVM varies considerably. Some patients are asymptomatic, but the majority suffers from cosmetically disfiguring, often discoloring soft tissue masses that are prone to cause pain. CFVM may even obstruct the upper airways and hamper swallowing and speech. The diagnosis is usually based on the clinical manifestation. Both MRI and ultrasound can prove useful to confirm the diagnosis of a VM along with the lesion’s extent identification (10). There are different treatment options for VM in general, such as surgical excision, laser therapy, and percutaneous sclerotherapy. The latter is a well-established treatment option and is a widely accepted treatment for VM.
The goal of sclerotherapy is to shrink the malformed channels, reduce venous insufficiency, and decrease swelling and pain, as stated by other authors (5). Percutaneous sclerotherapy may improve CFVM-related symptoms. However, both patients and operators have to keep in mind that the underlying disease stems from a hereditary condition, which is usually not curable (5). Ethanol, polidocanol, ethanolamine oleate, and sodium tetradecyl sulfate are the four mainstream sclerosants (11–13). Ethanol is the most effective and powerful sclerosant in the treatment of VM. However, unfavorable systemic reactions—such as skin necrosis, severe swelling, and neuropathy—are well-known and feared complications (14). The efficacy of foamed detergents such as sodium tetradecyl sulfate and ethanolamine oleate is comparable to ethanol, with the advantage of significantly reduced occurrence of systemic complications and neuropathy (5). Unlike several other previously published studies on percutaneous sclerotherapy of CFVM (14–17), we used polidocanol as the sclerosant for treatment. Polidocanol has less sclerosant power than ethanol but seems to be better tolerated than ethanol (18). We were able to confirm this observation, given we only experienced one complication in 56 treatment sessions. The injected volume was individually adjusted to the volume and localization of each malformation and never exceeded 5 mL per treatment session for children and 10 mL for adults. Bleomycin is an established sclerosant with promising results and less post-procedural swelling than ethanol. Thus, it is used as a sclerosant especially for oral and orbital VM. However, it requires more treatment sessions compared to ethanol and has a noteworthy rare risk of pulmonary fibrosis (15).
Concerning indication and treatment requirement, meticulous considerations between risk of percutaneous sclerotherapy and risk of natural history have to be made. The therapeutic goal must always be defined by clinical symptoms and not just by angiographic or cross-sectional images. The main objective is the reduction of CFVM-related risks and symptoms. Additionally, it is of utmost importance for the patients to be provided with realistic expectations regarding the subjective therapy outcome. Patients’ subjective perception regarding clinical outcomes often diverges to the objective improvement or change on MRI. In this context, it is noteworthy that 12 of 18 patients with improvement of at least one of their corresponding symptoms had a post-sclerotherapy size reduction of > 50% on MRI and physical examination, while six of these 18 patients had a < 50% size reduction.
We observed heterogeneity of CFVM types in our cohort with 15% type-I, 45% type-II, 25% type-III, and 15% type-IV VM on direct puncture phlebography. This distribution is comparable to the results evidenced by Puig et al. (6). They concluded that sclerotherapeutic interventions can be safely performed in type-I and type-II VM and that careful consideration must be given to sclerotherapy of type-III and type-IV VM. Interestingly, we also encountered no complication with 12 type-I or type-II VM patients and only one minor complication with one out of eight classified type-III and type-IV VM patients. Notably, we did not observe any association between the type of VM and the subjective outcome of the patients after sclerotherapy treatment. Eighteen of 20 patients, exhibiting all four types of VM, specified complete relief or improvement of at least one of their presenting symptoms. One of the patients who did not improve after treatment had a type-II VM, while the other patient was diagnosed with type-III VM. Nevertheless, only two of 13 patients with a > 50% size reduction were type-III or type-IV VM.
In accordance with other authors, we believe that patient satisfaction and improvement of clinical symptoms are the most important outcomes (19,20). We agree with other groups that the therapeutic goal is the improvement or at least stabilization of patients’ physical comfort as well as minimization or elimination of impairments in daily life (16,19–21). Many of our patients already had a long clinical history and suffered from a high psychosocial burden when they presented to our department for percutaneous sclerotherapy. In certain severe cases, further complementing therapeutic options, such as surgical procedures, or laser therapy might be mandatory. Ideally, all therapeutic treatment options should be available at one medical institution. Surgical options of CFVM at our hospital are limited. We mostly treat patients who have been referred to us by different physicians in a multidisciplinary setting. We jointly discuss the cases and subsequently evaluate if percutaneous sclerotherapy with Polidocanol is a promising treatment option. Considering the results of this study, most of the patients noted an improvement or even a complete post-therapy relief of their symptoms. Moreover, we were able to statistically demonstrate percutaneous sclerotherapy significantly reduced impairments in daily life. In our opinion this is one of the most important goals in treatment of CFVM. In this context, we observed that some patients were satisfied to an extent that no continued treatment was requested, even though the VM was clinically still visible and/or radiologically detectable.
It is well established that VM in general have a noteworthy high recurrence rate and tend to regrow during puberty and other times of hormonal changes (1). Nevertheless, in our series of CFVM-affected patients treated by sclerotherapy with polidocanol, we could not observe any recurrent malformation on MRI nor physical examination at the time of follow-up. However, the majority of our CFVM patients were young adults with a mean follow-up period of 53 months. These patients are likely to have a long life expectancy. In this context, it is crucial to regularly see patients clinically and follow them up utilizing MRI. Hence, further investigations are necessary to collate additional data about lifetime recurrence rates of CFVM, including the risk of recurrence in times of hormonal changes.
Our study has several limitations. First, the number of analyzed cases in this retrospective study research is considerably low since CFVM is recognized as a relatively rare disease. Second, we used a self-developed/non-standardized questionnaire to assess the subjective results of our patients. It was hence not validated in terms of reliability and reproducibility. Also, the questionnaire was only answered after treatment. Therefore, patients’ subjective perception of the pre-sclerotherapy status could have been influenced by the final treatment outcomes, limiting the value of the results. However, one aim of this descriptive retrospective evaluation was to highlight specific changes of important CFVM-related symptoms after percutaneous sclerotherapy with polidocanol.
In conclusion, percutaneous sclerotherapy using polidocanol is a well-tolerated treatment for CFVM with a low complication rate. Size reductions and positive results relating to improvement of varying clinical symptoms including impairment in daily life can be achieved. However, certain severe cases might require further therapeutic options.
Footnotes
Acknowledgements
The authors thank Mr. Thomas Schmitz, Mrs. cand. med. Cynthia Schmidt, Dr. Katharina Melber, and Mr. Dominic Eichrodt for their editorial assistance.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.