
Abstract
Background
Assessment of Crohn’s disease (CD) activity is important to identify patients with active inflammation for therapy management. Quantitative analysis can provide objective measurement of disease presence.
Purpose
To evaluate the feasibility of quantitative analysis of contrast-enhanced dual-energy computed tomography (DECT) data in detection of small bowel inflammation in patients with CD with an emphasis on iodine quantification.
Material and Methods
DECT enterography was prospectively performed in 20 patients with active CD and in 20 healthy individuals, as the control group. Iodine overlay images were created. Wall thickness, attenuation, absolute iodine density, relative iodine density, and fat fraction were measured in the terminal ileum of all patients by two radiologists. Intraclass correlation coefficients were calculated to assess inter-rater agreement. Parameters were compared between patient groups using mixed model analysis. Receiver operating characteristic (ROC) analysis was performed.
Results
Both absolute and relative iodine density were significantly higher in active disease than in normal small bowel (all P < 0.001). In contrast, measurement of fat fraction was not significantly different in affected terminal ileal loops compared to normal terminal ileum (P = 0.075). ROC analysis demonstrated a similar excellent diagnostic accuracy of wall thickness, attenuation, and absolute and relative iodine density with area under the ROC curve (AUC) values in the range of 0.96 for attenuation to 1 for relative iodine density.
Conclusion
DECT with iodine quantification can be used in distinguishing normal small bowel from active inflammatory CD. Further research should investigate the value of iodine quantification in grading CD activity and in monitoring therapeutic response.
Introduction
Crohn’s disease (CD) is one of the two major subtypes of inflammatory bowel disease and is characterized pathologically by a transmural granulomatous inflammatory process. Although it can affect any portion of the gastrointestinal tract, CD has a predilection for the small bowel, in particular the terminal ileum. Assessment of inflammatory activity in CD is crucial in the management of patients and in monitoring response to therapy. Historically, activity in CD has been generally evaluated using clinical and biochemical parameters or endoscopy. However, assessment of disease activity solely by endoscopy may be incomplete since CD is a transmural disease which may extend beyond the reach of the endoscope (1). Therefore, cross-sectional imaging has become a vital tool for the global assessment of CD allowing detection of both intestinal and extra-intestinal disease manifestations such as abscesses, fistulas, or bowel obstruction (2–4). Computed tomography (CT) as well as magnetic resonance imaging (MRI) of the small bowel have high diagnostic accuracy in the evaluation of CD (5–8). CT enterography (CTE) differs from routine abdominal CT examination by using large volumes of an oral neutral contrast agent and intravenous administration of spasmolytic medication, thereby improving visualization of the small bowel wall and lumen. CTE findings of mural stratification, mural hyperenhancement, bowel wall thickening, haziness of the surrounding mesenteric fat, and engorged vasa recta (‘comb sign’) have been well described and correlate with active inflammation (7,9,10).
Dual-energy CT (DECT) has been a rapidly progressing modality ever since its introduction into clinical practice in 2006. DECT has a particular advantage compared to conventional single-energy CT (SECT) as it can provide material-specific images. The basic principle of DECT consists of acquisition of two image datasets of differing energies, usually 80 kVp and 140 kVp, within the same study. Tissue characterization with DECT is possible since different materials have different X-ray absorption characteristics when scanned with these high and low X-ray energies. Materials with high atomic numbers, such as iodine, show large differences in attenuation at high and low kVp values, and therefore become potential targets for material characterization with DECT image acquisition (11–14). DECT post-processing techniques can decompose contrast-enhanced images into iodine images and virtual non-contrast (VNC) images. These iodine images represent the amount of iodine present in a tissue. Quantification of iodine content on iodine images may provide a more consistent measurement compared with attenuation measurements in Hounsfield Units (HU) in a SECT acquisition as the latter takes into account both the tissue density and the iodine amount whereas the iodine images give specific information about the iodine content of a tissue (11,13,14). While previous studies using conventional single-energy CTE (SECTE) already validated the ability of quantitative measures of wall thickness and mural attenuation to detect active small bowel inflammation (15–17), the use of dual-energy CTE (DECTE) with iodine quantification for diagnosis of active CD has only been scarcely investigated (18).
The objective of this study was to measure wall thickness, attenuation, relative and absolute iodine density, and fat fraction in small bowel on contrast-enhanced DECTE and to study the ability of these features in distinguishing normal small bowel from active inflammatory CD.
Material and Methods
This prospective study was approved by the institutional ethics committee. Informed consent was obtained from all participants.
Patient population
A case-control study design was used. All 40 CTE examinations were performed at our institution over a 15-month period (October 2015 – December 2016). The study group consisted of 20 patients with endoscopically proven CD involving the terminal ileum and high clinical suspicion of active inflammatory disease based on objective markers of inflammatory activity (CRP > 5 mg/L or fecal calprotectin > 100 mcg/g) and/or symptoms suggestive of active disease (including obstructive symptoms such as colicky abdominal pain, vomiting). The mean duration of disease was 12 years (range = 0–41 years). At the time of CT examination, 17 of the 20 patients were being treated with a variety of medications for CD, including aminosalicylates, immunomodulators, and biologic therapies. These patients had been taking their medication for at least one month before CT examination. All patients were referred to our department for CTE examination to confirm active inflammation, assess the extent of disease, and detect possible extra-enteric complications. The control group consisted of 20 patients without CD confirmed on ileocolonoscopy (n = 17) or colonoscopy and capsule endoscopy (n = 3). These patients underwent CTE examination at our institution for abdominal discomfort and diarrhea (n = 15), unexplained weight loss (n = 1) or iron-deficiency anemia (n = 4) within 60 days of endoscopic examinations. Most of these patients were diagnosed with irritable bowel syndrome by a board-certified gastroenterologist. There were 9 women and 11 men in the study group (mean age = 44 years; age range = 26–65 years) and 12 women and eight men in the control group (mean age = 54 years; age range = 25–75 years) at the time of CT examination.
Dual-energy CTE
All CT examinations were performed with a dual-source DE unit (Somatom Definition Flash, Siemens Healthineers, Erlangen, Germany). The DECT protocol was as follows: tube A was operated at a kilovoltage peak of 80 kVp and tube B at 140 kVp; reference mAs were 230 and 178 mAs, respectively; pitch = 0.6; slice increment = 1 mm; and slice thickness = 3 mm. Examinations were performed with automatic tube current modulation to reduce dose. Before scanning, patients ingested four 250-mL aliquots (1000 mL in total) of a neutral polyethylene glycol electrolyte solution (Moviprep®, Norgine B.V., Amsterdam, The Netherlands) over a 45-min period, with subsequent aliquots given 15, 30, and 45 min after the first intake. CTE examination was performed 60 min after the start of ingestion. Patients were given 20 mg of an intravenous spasmolytic agent (hyoscine butylbromide, Buscopan®, Boehringer Ingelheim, Ingelheim am Rhein, Germany) immediately before scanning to abolish bowel motility. Images were acquired 70 s after administration of 100 mL intravenous iodine contrast material (Visipaque™, GE Healthcare, Princeton, NJ, USA) at a rate of 3.5 mL/s.
Iodine-selective imaging
Primary image reconstruction was performed in real-time at the CT acquisition workstation and resulted in separate low energy (80 kVp), high energy (140 kVp), and weighted average image datasets (120 kVp). These weighted average images are also referred to as “mixed” images and result from combining HU information from the individual 80-kVp and 140-kVp datasets. As they are visually comparable to a SE study, mixed images are usually used for clinical interpretation. Subsequently, material specific imaging was performed with iodine density images being created from the 80-kVp and 140-kVp datasets on a separate workstation with dedicated DE software (Syngo®.via, Siemens Healthineers, Erlangen, Germany) by three-material decomposition analysis. With this technique, the iodine contribution to each voxel is selectively identified from the absorption characteristics of three materials: fat; soft tissue; and iodine. In this way, the iodine contribution can be subtracted from the dataset generating VNC images and iodine images. The iodine content can be displayed as pure iodine maps or as an iodine overlay map that superimposes the iodine content in color on top of the gray-scale VNC image.
Image review
All DECTE images were independently reviewed by two gastrointestinal radiologists (IDK, LD) with six and 19 years of experience, respectively. All measurements were made on a dedicated work station (Syngo®.via, Siemens Healthineers, Erlangen, Germany). The terminal ileum was measured within 5 cm of the ileocecal valve. Wall thickness (mm) was determined on the mixed images using a linear measurement tool. Bowel wall attenuation (HU), absolute iodine density (mg/dL), relative iodine density (%), and fat fraction (%) were obtained from the iodine material density overlay images using a round region of interest (ROI) placed over the bowel wall. In normal terminal ileum, the ROI was placed over the entire bowel wall. In CD patients, ROI placement depended on the terminal ileal wall enhancement pattern. When homogeneous bowel wall enhancement was present (n = 4), the ROI was placed over the entire bowel wall. When a mucosal enhancement pattern (e.g. increased enhancement of the mucosal layer relative to the outer layers) (n = 11) or layered enhancement pattern (e.g. increased enhancement of the mucosa and the serosa relative to the middle layer) (n = 5) was present, measurements were taken in the mucosal layer (Fig. 1). The ROI sizes varied based on the bowel wall thickness. In order to minimize variations among patients, the iodine density in the bowel wall was normalized to the iodine density of the infrarenal aorta by placing a ROI over the center of the vessel to measure the maximum intra-arterial iodine density.
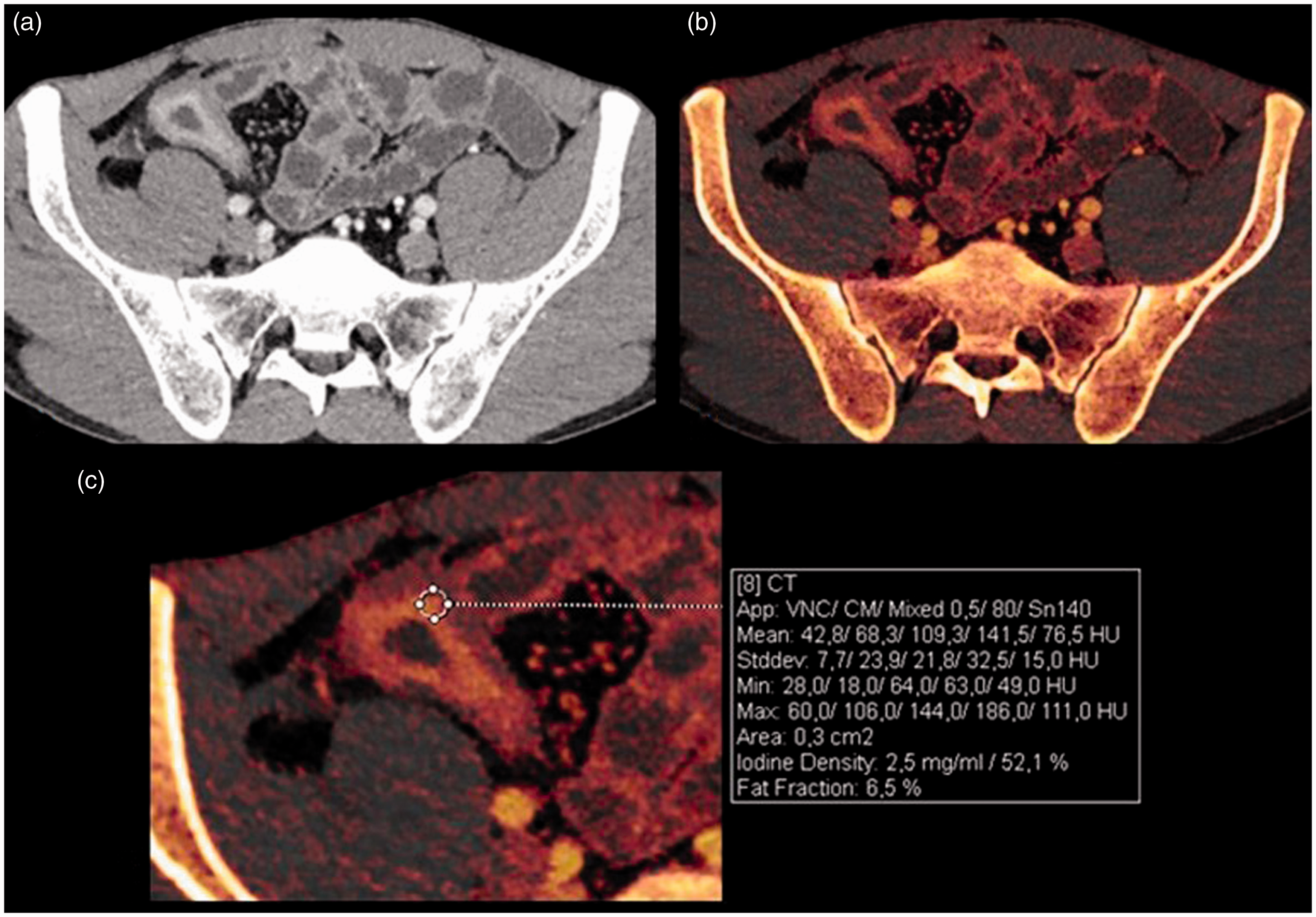
Axial mixed DECTE image (a) and iodine overlay image (b) demonstrating inflammation of the terminal ileum with a mucosal enhancement pattern in a 36-year-old man with CD. A ROI is placed in the intensely enhancing mucosal layer of the thickened terminal ileal wall generating quantitative data (c).
Statistical analysis
Statistical analysis was performed using software package SPSS 24.0 for Windows (SPSS, Chicago, IL, USA). Intraclass correlation coefficients (ICC) were calculated to assess inter-rater agreement. ICC values < 0.40 were considered to represent poor agreement; values of 0.4–0.59, moderate agreement; values of 0.6–0.74, good agreement; and values of 0.75–1.00, excellent agreement. Mixed model analysis was used to assess the ability of each quantitative DECTE parameter (wall thickness, attenuation, absolute and relative iodine density, and fat fraction in the terminal ileum) to discriminate between the mean scores of these parameters of patients with disease and patients without disease. A random intercept for rater was included in these models, as outcome scores of both raters were used in these analyses. Statistical significance was defined as P < 0.05. Receiver operating characteristic (ROC) analysis was performed to evaluate the accuracy of each variable to help identify active inflammation in the terminal ileum. Area under the curve (AUC) estimates with associated 95% confidence intervals (CI) are reported.
Results
The level of agreement between the two readers was excellent for absolute and relative iodine density (ICC = 0.82 and ICC = 0.75, respectively) and good for wall thickness (ICC = 0.70) and attenuation (ICC = 0.69) but only moderate for fat fraction (ICC = 0.49).
Terminal ileal wall thickness was significantly increased in patients with active CD compared with wall thickness in patients without CD (P < 0.001). Similarly, terminal ileal attenuation was significantly higher in patients with active CD than in patients without disease (P < 0.001). Both absolute and relative iodine density measurements were also significantly different among the two groups (P < 0.001), with the highest quantitative measures of iodine density seen in patients with active terminal ileal CD (Fig. 2). Contrarily, no significant difference was observed between fat fraction of the terminal ileum in patients with active CD and patients without CD (P = 0.075). All values are shown in Table 1.
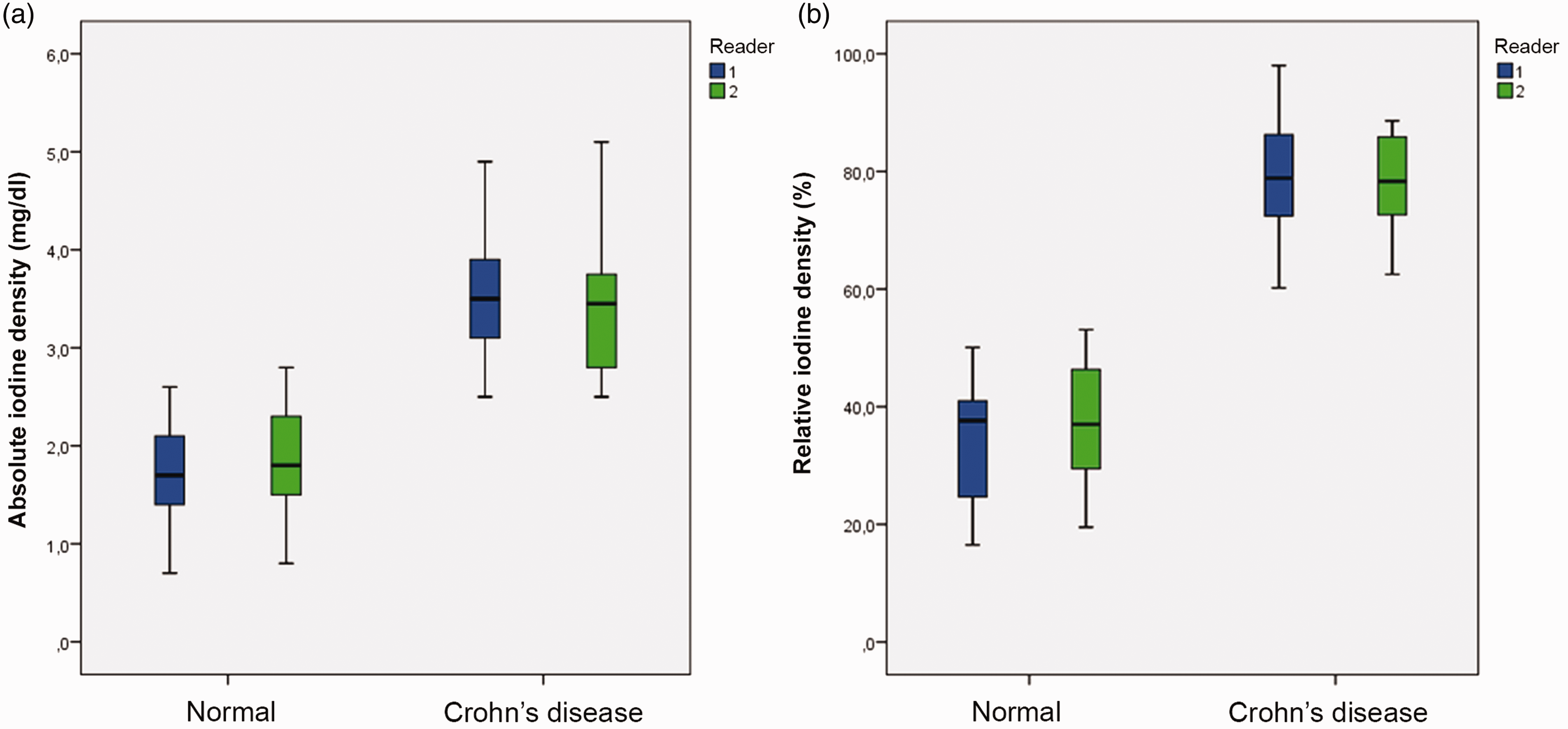
Box and whiskers plots of absolute iodine density (a) and relative iodine density (b) measured in normal terminal ileum and terminal ileum of patients with active CD. Iodine density measurements were significantly increased in patients with active CD compared with normal terminal ileum.
Mean wall thickness, attenuation, absolute iodine density, relative iodine density and fat fraction measured in normal terminal ileum and in the terminal ileum of patients with active Crohn’s disease (CD).
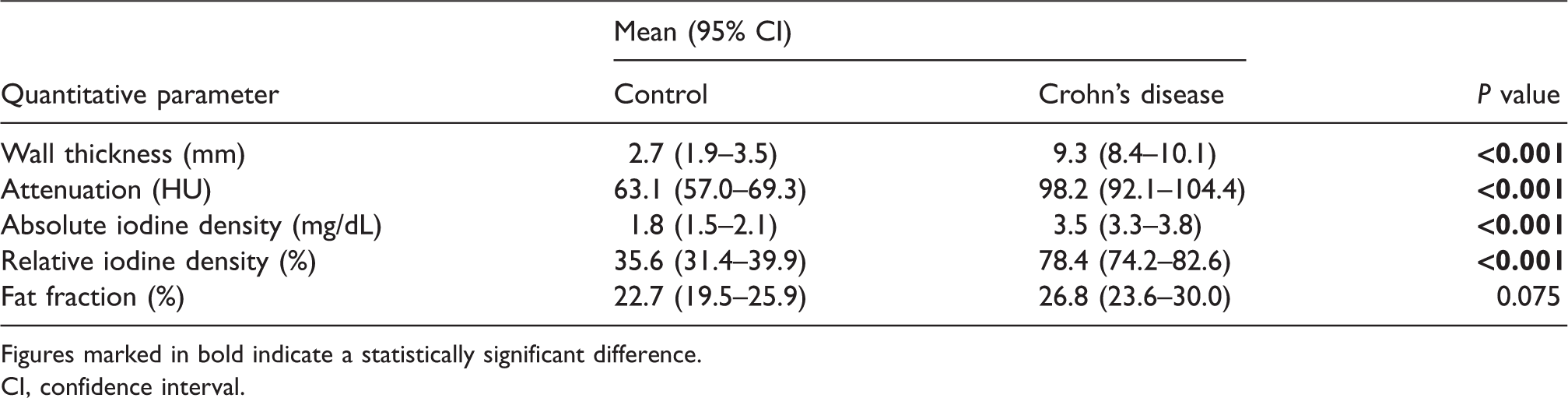
Figures marked in bold indicate a statistically significant difference.
CI, confidence interval.
ROC analysis demonstrated an excellent performance of wall thickness, attenuation, and absolute and relative iodine density in identifying active inflammation in the terminal ileum with AUC values in the range of 0.96 for attenuation to 1.00 for relative iodine density. Fat fraction shows a clearly lesser diagnostic accuracy (reader 1, AUC = 0.68 and reader 2, AUC = 0.60) (Fig. 3, Table 2).
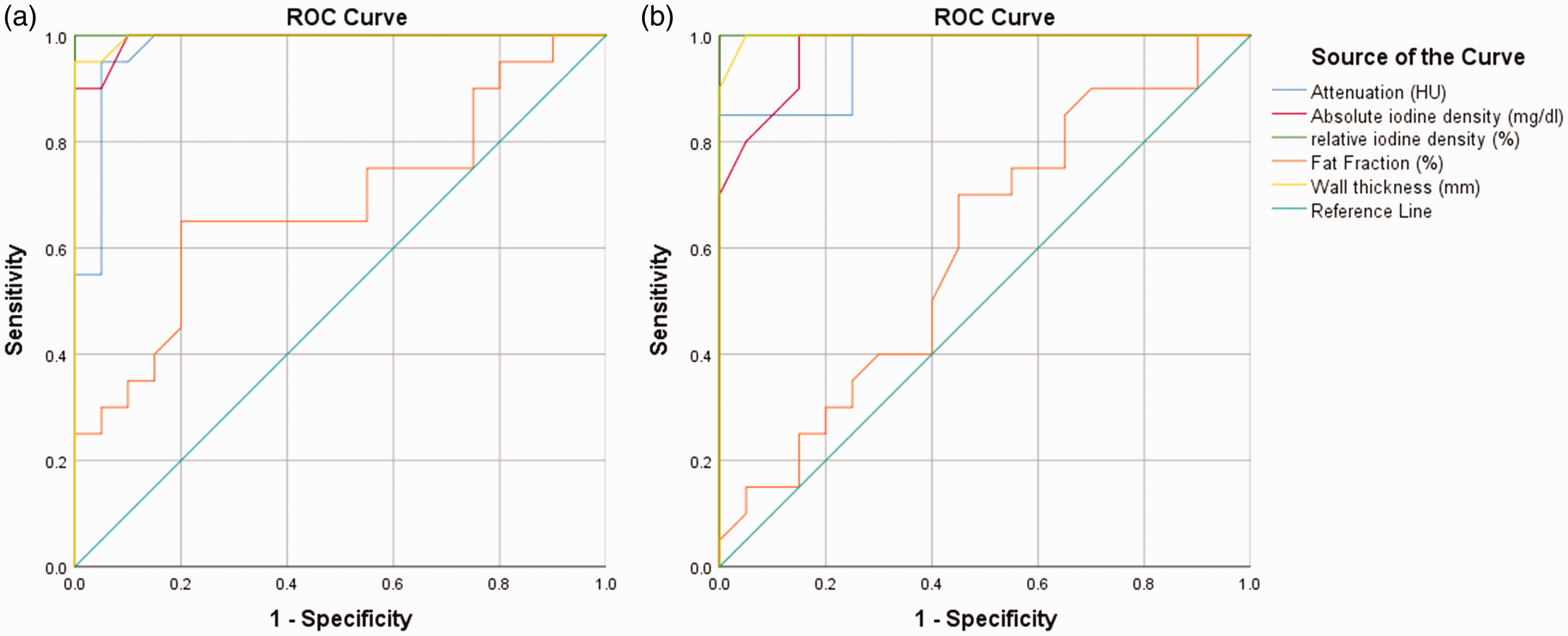
ROC curves reflect capability of attenuation, absolute iodine density, relative iodine density, fat fraction and wall thickness to detect active inflammation in the terminal ileum, as assessed by readers 1 (a) and 2 (b). Fat fraction (orange line) shows a clearly lesser diagnostic performance compared to the other parameters.
ROC analysis with AUC values for terminal ileal wall thickness, attenuation, absolute iodine density, relative iodine density, and fat fraction.
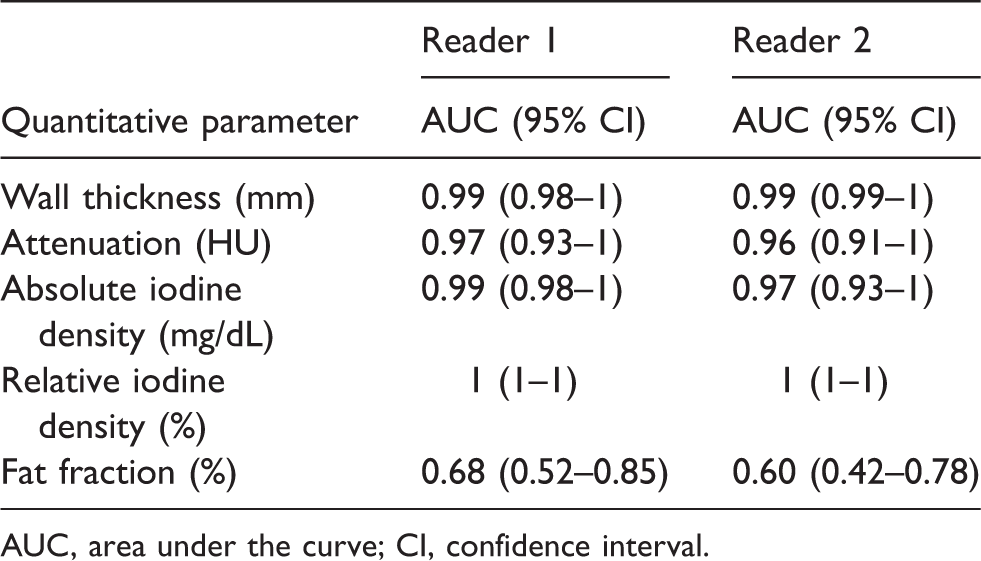
AUC, area under the curve; CI, confidence interval.
Discussion
It is well-known that CTE and MR enterography (MRE) are both valuable imaging modalities in CD as they can depict active disease as well as the presence of extraintestinal complications such as strictures, abscesses, and fistulas. Several studies have shown that CTE and MRE have comparable accuracies for assessing active inflammatory CD (5–8). The imaging modality of choice is largely center-specific, dependent upon local expertise, cost, and access. Nevertheless, with the increasing awareness of radiation exposure, there has been a more global interest in the use of MRI. The recent joint ESGAR/ECCO consensus guidelines on imaging in inflammatory bowel disease also indicated radiation exposure as a major reason to prefer MRE to CTE (2). This is especially important in young patients or patients with chronic diseases, such as CD, who may require repeated imaging over a lifetime. However, CT is the imaging modality of choice in the emergency setting because it is rapidly available, and less time-consuming. Furthermore, CTE consistently provides high-quality diagnostic images, even in frail patients or patients with difficulties breath-holding. Studies comparing image quality between CTE and MRE have preferred CTE to MRE, also stating superior inter-observer agreement (6,7,19). Substantial advances in CT dose reduction techniques have already been made, both for acquisition, such as automatic tube current modulation, as well as for image reconstruction, such as iterative reconstruction, and ongoing research will result in further CT dose reduction (11,20–22). In DECT imaging, there is a common misconception that it implies an increased radiation dose to the patient because of the acquisition of two imaging datasets. However, several studies have shown that abdominal dual-source DECT examinations can be performed without increased radiation dose exposure or impairment of image quality compared to SECT (22–24). Therefore, the quantitative imaging potential of DECT can be utilized without increased radiation dose penalty.
Assessment of inflammatory activity of CD is important to identify patients with active inflammation so that appropriate therapy may be administrated. In routine radiological practice, visual assessment of bowel wall thickness, increased mural attenuation, and peri-enteric inflammatory changes are generally used to diagnose active CD. However, sometimes these visual findings can be subtle or equivocal. In these cases, quantitative analysis can be helpful as it can provide objective measurement of disease presence. Previous studies using SECT have already validated the ability of quantitative measures of wall thickness and mural attenuation to detect active small bowel inflammation (15–17). Bodily et al. found that CTE measurements of mural attenuation and wall thickness of the terminal ileum correlated significantly with histologic and endoscopic findings of inflammatory CD. Also, they found that measurements of terminal ileum attenuation had the highest sensitivity (90%) for predicting the presence of active inflammatory CD, compared with a sensitivity of 80% for visual assessment of mural hyperenhancement (15). Baker et al. investigated the efficacy of absolute and relative mural attenuation on CTE in distinguishing normal small bowel from active CD of the terminal ileum, and also studied the utility of wall thickness. They found that both absolute and relative mural attenuation could discriminate normal small bowel from active terminal ileum CD with statistical significance, and that wall thickness was an important covariable: when wall thickness was taken into account, absolute and relative attenuation measurements were significantly better at depicting active CD than the same measurements without wall thickness (16). In our study, we confirmed the ability of wall thickness and attenuation to detect active CD using DECT imaging. Moreover, we could also distinguish normal small bowel from active terminal ileum CD by quantifying iodine content within the bowel wall. We found that absolute and relative iodine density measurements were significantly higher in patients with active CD than in patients without CD (P < 0.001). Furthermore, ROC analysis revealed a similar excellent diagnostic performance of wall thickness, attenuation, absolute iodine density, and relative iodine density measurement. In a recent retrospective study, Villanueva Campos et al. have measured absolute iodine density (mg/dL) and fat fraction (%) in bowel segments with radiological signs of active inflammation as well as in normal appearing bowel segments in 33 CD patients (18). Similar to our study, they have found that absolute iodine density was significantly higher in affected bowel loops than in normal appearing bowel segments. Furthermore, they could demonstrate a significantly higher fat fraction in normal appearing small bowel as compared to inflammatory bowel segments. Unlike Villanueva Campos et al., we found that measurement of fat fraction is not able to distinguish normal small bowel from active inflammatory CD. Indeed, submucosal fat accumulation in the bowel wall, known as the “fat halo sign” on CT imaging, has been described in patients with longstanding CD but relates to chronic bowel inflammation and is not typical of active disease (25–27). A possible explanation for these contradictory results regarding fat fraction could be that Villanueva Campos et al. did not compare CD patients with a healthy control group, as in our study, but obtained control measurements from normal appearing bowel loops (e.g. lacking radiological signs of inflammation) within the study group. As it is known that more than one subtype of CD may be present in the same patient, especially in longstanding disease, the presumably normal bowel segments in the study by Villanueva Campos et al. could possibly contain a certain degree of chronic inflammatory changes (e.g. submucosal fat deposition) not visible to the human eye.
The level of agreement between readers in this study was good for wall thickness and attenuation, and excellent for absolute and relative iodine density measurements suggesting that disease activity can reproducibly be measured using these quantitative parameters. However, relative measurements are more appropriate in comparisons between examinations performed in different patients or in the same patient at various times as the level of vascular attenuation on subsequent examinations could vary. Therefore, we believe that the use of relative iodine density measurements has a particular benefit and should be further explored.
Although clinically relevant, identifying the presence of active CD is not sufficient to guide therapeutic decisions since disease severity has a key role in most of the current treatment algorithms. Severity indices using MRE have already been proposed and validated (e.g. Magnetic Resonance Index of Activity (MaRIA) score, Crohn’s Disease MRI Index (CDMI) score); however, no CT-based severity score has yet been developed (28). Future research should aim to develop a quantitative scoring system for grading CD activity using DECT and explore the potential use of iodine density measurement as a marker of disease severity. Furthermore, considering the expense and potential side effects of medical treatment, objective and reproducible measures of disease activity are not only needed to improve diagnostic accuracy, but also to justify the use and evaluate the effectiveness of therapy (29–31). Therefore, further trials should also investigate whether iodine density measurements within the bowel wall change during treatment and whether these changes correspond to serum biomarkers or endoscopic or histologic findings.
Several limits exist in this study. First, this investigation reflects our preliminary results in a small sample of patients. Future studies should enroll a larger number of patients to obtain more conclusive results. Second, we did not differentiate between treatment nor disease duration among patients in the study group. However, we believe this reflects daily clinical practice in radiology. Third, further clinical trials need to be performed to confirm our quantitative data since iodine density may be influenced by injection parameters and cardiopulmonary status. In our study, this was in part offset by using the normalized iodine density which minimized individual differences and thereby reduced error. Finally, we had no reference standard for the small bowel other than the terminal ileum.
In conclusion, quantification of iodine density within the bowel wall can be used in distinguishing normal small bowel from active inflammatory CD. To the author’s knowledge, this is the first prospective study to explore the use of DECT in patients with CD. Further studies should focus on investigating the value of iodine density measurement in grading disease activity and in monitoring therapeutic response.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.