
Abstract
Background
Although imaging can be suggestive of the diagnosis of rectal cancer, the primary imaging role is to assist in treatment triage of histologically diagnosed tumors. The possibility of a multimodal approach in the response to the treatment opens the way for the selection of criteria more personalized to the patient.
Purpose
To assess the prognostic factor of morphological and functional magnetic resonance imaging (MRI) in rectal cancer.
Material and Methods
Seventy-seven patients were enrolled and underwent MRI before treatment and 59 patients underwent MRI after treatment. Radiologists evaluated the presence of lesions using a 4-point confidence scale; they recorded anatomical side, extent, and distance from the anorectal junction and distance from the circumferential margin. Tumor location was classified according to the involvement of proximal rectal channel and/or distal rectal channel. Radiologists scored signal intensity on T2-weighted (T2W) images, diffusion-weighted images (DWI), and MRI dynamic enhancement pattern. Tumor regression grade (TRG) and pathological T (pT) were the gold standard.
Results
Lesion vascularization score before treatment showed a predictive value of complete pathological response (sensitivity 88%, specificity 50%) based on pT, while using TRG lymph node number before treatment (sensitivity 83%, specificity 57%) showed a predictive value for response treatment. T2W signal (sensitivity 78%, specificity 30%) and DWI signal after treatment (sensitivity 78%, specificity 61%) showed a good predictive value for local rectal recurrences.
Conclusions
Lesion vascularization and lymph node number had a predictive value for neoadjuvant treatment complete response in rectal cancer. T2W signal intensity and DWI signal showed a good predictive value for local rectal recurrences.
Introduction
Colorectal cancer is the most common gastrointestinal cancer. Rectal cancer comprises one-third of all colorectal cancer cases, and of these, approximately 30% arise within 6 cm from the anal verge (1,2). This cancer is a frequent malignancy in both sexes, accounting for 39,610 new cases in the USA in 2015; after lung cancer, rectal cancer is the second most common cause of cancer mortality in the USA (3). Although imaging can be suggestive of the diagnosis of rectal cancer, the primary imaging role is to assist in treatment triage of histologically diagnosed tumors (4). Magnetic resonance imaging (MRI) is the gold standard in oncological pelvic examination, providing morphological and functional data (4–6). MRI allows an excellent imaging of the rectal wall, so that it can be obtained an accurate evaluation of cancer stage including tumor infiltration degree, involvement of the perirectal fat as well as of mesorectal fascia and anterior peritoneal reflection, and an effective assessment of lymph nodes and extramuscular vascular invasion (EMVI) (4–7). In order to get functional information to guide patient selection versus personalized therapeutic strategies after treatment and for restaging after treatment, diffusion-weighted imaging (DWI) can assess the microstructural organization of a tissue such as cell density, cell membrane integrity, and cell viability and is recommended in clinical practice (8–11). Moreover, dynamic contrast-enhanced MRI (DCE-MRI), again restricted to clinical research, had demonstrated the role of perfusion information to assess neoadjuvant treatment response; currently, this has limited clinical usage in rectal cancer (12,13).
Total mesorectal excision (TME) associated with preoperative radiation and chemotherapy (CRT) is the standard care for locally advanced rectal cancer (LARC) (14,15). However, conservative treatment strategies are being developed for patients with early rectal cancer at diagnosis and patients with significant pathological regression after CRT (16) while a “wait and see” strategy is adopted when a complete clinical response is obtained. These strategies have the advantage of reducing morbidity and provides a “true” organ-sparing approach (17).
The possibility of a multimodal approach opens the way for the selection of criteria more personalized to the patient. Therefore, there is the need to identify prognostic features, which can guide therapeutic strategies. The aim of this prospective study is to assess the functional and morphological prognostic features of MRI which can be of any assistance in the treatment choice for rectal cancer patients.
Material and Methods
Patient population
Seventy-seven consecutive patients (median age = 64 years; age range = 41–79 years) were enrolled in this prospective study from March 2009 to June 2016. All patients had a biopsy-proven rectal adenocarcinoma. Endorectal ultrasonography, pelvic MRI, and whole-body contrast-enhanced CT scans have been used for staging. Inclusion criteria were: patients with clinical stage T3–4 cancer or with nodal involvement. Exclusion criteria were: inability to give informed consent; previous rectal surgery; and contraindications for undergoing MRI or administering MR contrast media. Three patients were not subjected to DCE-MRI before treatment for contrast agent contraindications.
Among the 77 enrolled patients, 59 had an MRI examination before and after CRT treatment since they underwent neoadjuvant therapy; 18 had an MRI examination before surgical treatment only, since they underwent TME directly. The length of time between baseline and preoperative MRI scan was 90 days (± 15). All patients had been enrolled in a prospective trial approved by the local Independent Ethical Committee (14). All patients signed written informed consent to participate to the study.
Neoadjuvant therapy and surgical approach
Fifty-nine patients were subjected to radio-chemotherapy. External radiation therapy was performed using a three-field technique (one posteroanterior and two lateral fields). Standard fractions of 1.8 Gy/day to the reference point were given, five times a week, up to a total dose of 45 Gy. Details of treatment planning have been previously reported (14). These patients received standard treatment with capecitabine at a dose of 825 mg/m2 twice daily, five days a week, for five weeks. Fifty-nine patients underwent TME nine weeks (range = 7–14 weeks) after completing CRT. An anterior or abdominoperineal resection was performed on the basis of the results of restaging.
The follow-up was five years after surgery. In addition to regular physical examinations every 3–6 months, the following tests have been recommended to watch for colorectal cancer recurrence: CEA testing was recommended every 3–6 months for five years; CT scans of the abdomen and chest were recommended every 6–12 months for the first three years; MRI of the pelvis was recommended every 6–12 months for the first three years; colonoscopy was recommended one year after surgery; recto-sigmoidoscopy test was recommended every six months for five years (18). Therefore, our patients underwent CEA testing every 3–6 months for five years and CT scans and MRI of the pelvis every 6–12 months for the first three years. Colonoscopy was performed one year after surgery, while recto-sigmoidoscopy was performed every six months for five years.
According to the follow-up, we reported the number of local recurrences for the studied population. Median follow-up time was 47 months (±11).
MRI data acquisitions
MRI was performed with a 1.5-T scanner (Magnetom Symphony, Siemens Medical System, Erlangen, Germany) equipped with a phased-array body coil. Patients were placed in a supine, head-first position. Mild rectal lumen distension was achieved with 60–90 mL of undiluted ferumoxil (Lumirem, Guerbet, Roissy CdG Cedex, France) suspension introduced per rectum in order to get mild distension of rectal lumen and improve the evaluation of rectal wall involvement, particularly in the post-contrast MR scan. Pre-contrast coronal T1-weighted (T1W) two-dimensional (2D) turbo spin-echo (TSE) images and sagittal and axial T2W 2D TSE images of the pelvis were obtained. Axial DW images were obtained with a single-shot spin-echo diffusion-weighted echo-planar pulse sequence (SE-DW-EPI) at b-values of 0, 50, 100, 150, 300, 600, and 800 s/mm2. Axial dynamic contrast-enhanced T1W FLASH three-dimensional (3D) gradient-echo (GRE) images were obtained: one sequence before and ten sequences after intravenous injection of 0.1 mmol/kg of a positive, gadolinium-based paramagnetic contrast agent (Gd-DOTA, Dotarem, Guerbet, Roissy-CdG-Cedex, France) at 2 mL/s of flow rate, followed by a 10-mL saline flush at the same rate. Sagittal, axial, and coronal post-contrast T1W 2D TSE images, with and without fat saturation, were obtained. The axial images were acquired without any angulation. Axial T1W pre- and post-contrast sequences were acquired at the same position as the T2W sequence. MRI total acquisition time was about 30 min.
Sequence parameters details were reported in Table 1.
Pulse sequence parameters on MR studies.
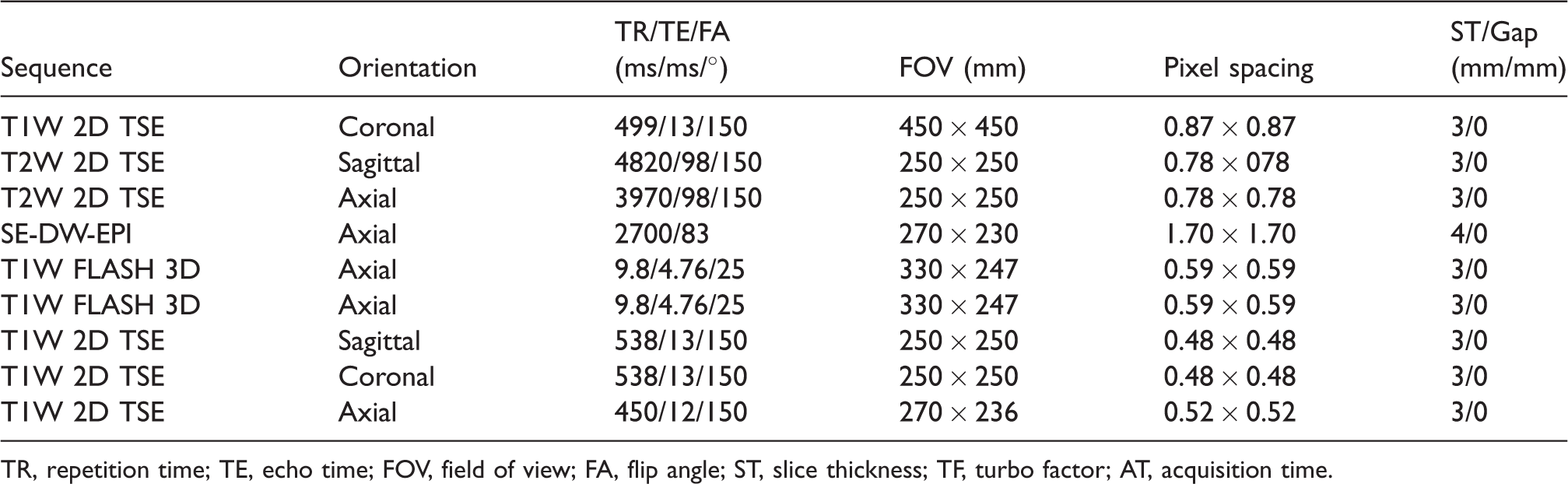
TR, repetition time; TE, echo time; FOV, field of view; FA, flip angle; ST, slice thickness; TF, turbo factor; AT, acquisition time.
MRI image data analysis
MRI analysis was performed prospectively in a single reading session for each patient by consensus of two expert gastrointestinal MR radiologists with at least 10 years of experience in abdominal imaging. MRI readers were blinded to the clinical and pathological outcome.
The radiologists evaluated the presence of lesions, using a 4-point confidence scale (score) (6); 1 = no lesion; 2 = probably no lesion; 3 = probably lesion; 4 = definitely lesion. For each single lesion, the radiologists recorded the anatomical side, extent, and distance from the anorectal junction and the distance from the circumferential margin (CRM). The tumor location was classified according to the involvement of the proximal rectal channel and/or distal rectal channel.
We scored the signal intensity (SI) in T2W imaging and in DWI.
The appearance of the tumor on T2W images was categorized using a 4-point scale (score): 0 = no lesion detected; 1 = hypointense; 2 = isointense; 3 = hyperintense compared to rectal wall.
When the lesion was hyperintense on all b-values, we defined this as restricted diffusion. We used a 2-point scale (score) to assess the diffusion: 1 = no restricted diffusion; 2 = restricted diffusion.
We classified qualitatively the perirectal vascularization according to the number and caliber of hematic vessels into mesorectal fat, using a 3-point confidence scale (score): 1 = no hematic vessels; 2 = few hematic vessels (1–4 detected vessels) with regular caliber; 3 = many hematic vessel (>5) with or without increased caliber.
Qualitative (q) DCE-MRI involves the visual inspection and classification of the time intensity curve (TIC). qDCE-MRI evaluation was performed by radiologists in consensus, placing multiple regions of interest (ROIs) inside the lesions on dynamic contrast FLASH 3D GRE. Each ROI area was of 5 pixels (0.54 × 0.54 mm2 each pixel). We followed the scheme based on qualitative evaluation of TIC shapes proposed by Cheng et al. (19): type 1 = rapid initial and persistent enhancing type; type 2 = rapid initial and stable late enhancement (plateau); type 3 = rapid initial and decreasing late enhancement (wash-out). We classified the tumor vascularization, according to a 3-point scale (score): 1 = type 1 TIC shape; 2 = type 2 TIC shape; 3 = type 3 TIC shape.
Moreover, we reported the number of perirectal nodes.
In patients undergoing neoadjuvant therapy, radiologists re-evaluated the same parameters on post-treatment images.
Histological examination was the gold standard.
Evaluation of pathologic response
Details of how pathologic response assessment was performed have been described (20). Pathological TNM was prospectively evaluated by two expert pathologists who were not aware of the MRI findings according to the American Joint Committee on Cancer. Briefly, surgical specimens containing the tumor were evaluated and scored according to tumor regression grade (TRG), as proposed by Mandard et al. (21): TRG 1 = a complete response with absence of residual cancer and fibrosis extending through the wall; TRG 2 = the presence of residual cancer cells scattered through the fibrosis; TRG 3 = an increased number of residual cancer cells, with predominant fibrosis; TRG 4 = residual cancer outgrowing fibrosis; TRG 5 = the absence of regressive changes. Based on pathological TNM, the patients were divided into three categories: ypT0-1N0 was classified as complete response (CR); ypT2N0 was classified as intermediate response (IR); and ypT3-4N0 or ypTanyN+ was classified as poor response (PR) (19). Based on TRG, the patients with a TRG 1 or 2 score were considered good responders, whereas the remaining patients (TRG 3, 4, or 5) were classified as poor responders. Moreover, patients with TRG 1 were classified as complete responders.
Statistical analysis
Quantitative variables were expressed with median value ± standard deviation. All categorical data values were expressed absolute numbers and percentages. Correlation analysis using Rho Spearman coefficient was performed in order to assess the correlation between all extracted MRI variables with T, N, and grading results. Receiver operating characteristic (ROC) curves were calculated using all extracted MRI variables (perirectal vascularization, T2W signal, lymph nodes number, lesion vascularization, DWI signal). Optimal thresholds were obtained maximizing the Youden index in order to differentiate complete response versus intermediate and poor response based on pathological TNM and to differentiate good responders versus poor responders based on TRG. Sensitivity and specificity were calculated. Moreover, ROC curves, sensitivity, and specificity to differentiate patients with local recurrence by disease-free patients were also obtained. Fisher’s exact test was used to assess if the results were statistically significant.
A P value < 0.05 was considered significant for all tests. All analyses were performed using Statistics Toolbox of Matlab R2007a (The Math-Works Inc., Natick, MA, USA).
Results
All patients in our series had a radical resection with an intact and complete mesorectum. Fifty-nine underwent neoadjuvant therapy and 18 underwent TME directly. Sixty-seven patients had histological grade G2 and 10 had histological grade G3. Three patients were pathologically classified as T0, 13 as T1, 43 as T2, 12 as T3, two as T4, and four as Tx. Sixty-two patients had no lymph node involvement (N0) while 10 patients were pathologically classified as N1 and five as N2. Seven patients were classified as pathological complete responders and 52 as intermediate/poor responders by pT. Six patients had TRG 1, 22 had TRG 2, 18 had TRG 3, and 13 had TRG 4. Twenty-eight patients were then classified as good responders and 31 were classified as poor responders according to TRG.
Nine patients in our series had local recurrence histologically proven while 68 were free of disease at the time of follow-up.
In the staging phase, MRI detected all lesions (median score was 4); 55 tumors (71.4%) involved the distal rectal channel while 22 tumors (28.6%) involved the proximal rectal channel. For distal rectal tumors, 24 out of 55 (43.6%) involved anorectal junction. All lesions were extraperitoneal; 14 lesions (18.2%) were intraperitoneal and extraperitoneal.
Table 2 reports the findings of the extracted MRI variables before and after treatment including CRM, perirectal vascularization (Fig. 1), T2W signal, lymph node number, lesion vascularization, and DWI signal.
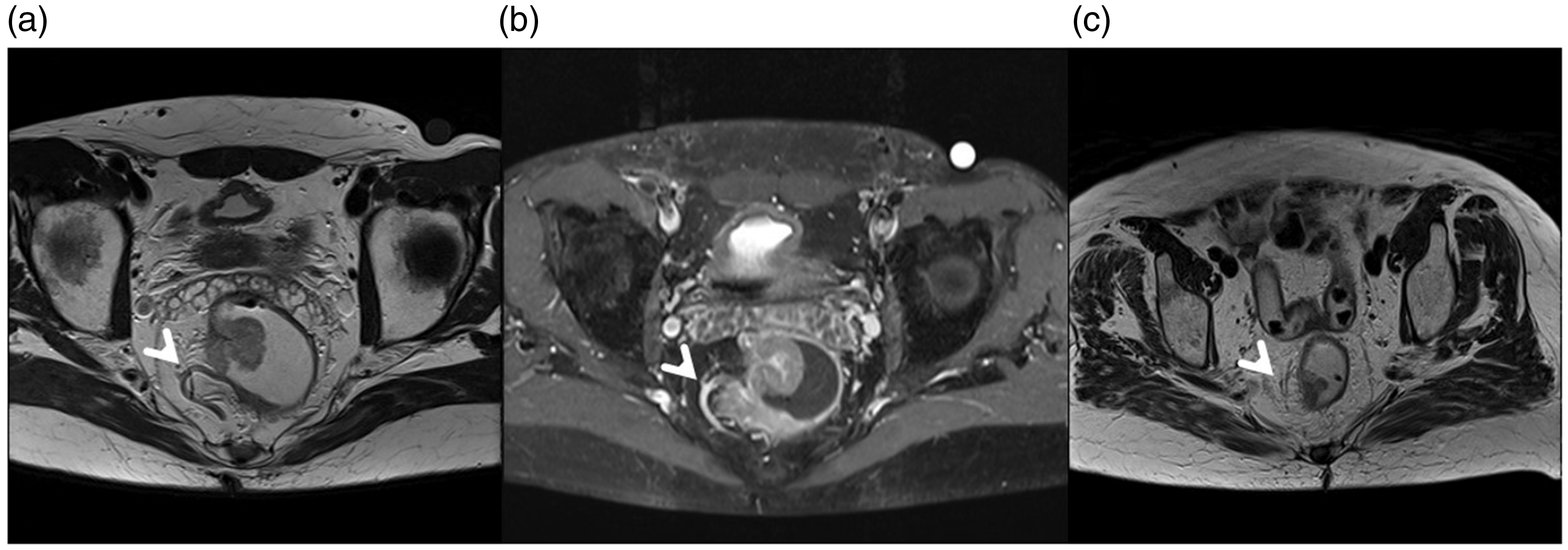
Man aged 45 years. Rectal cancer involves the proximal extraperitoneal channel. (a) T2W TSE sequence in axial plane: T3 lesion appears hyperintense, involving perirectal fat. (b) T1W TSE sequence after contrast medium: grade 3 of perirectal vascularization. (c) T2W TSE sequence in axial plane after neoadjuvant therapy: the lesion appears less evident compared to (a) with a grade 1 of perirectal vascularization. Responder patient.
Findings of the extracted MRI variables before and after treatment including CRM, perirectal vascularization, T2W signal, lymph node number, lesion vascularization, DWI signal.
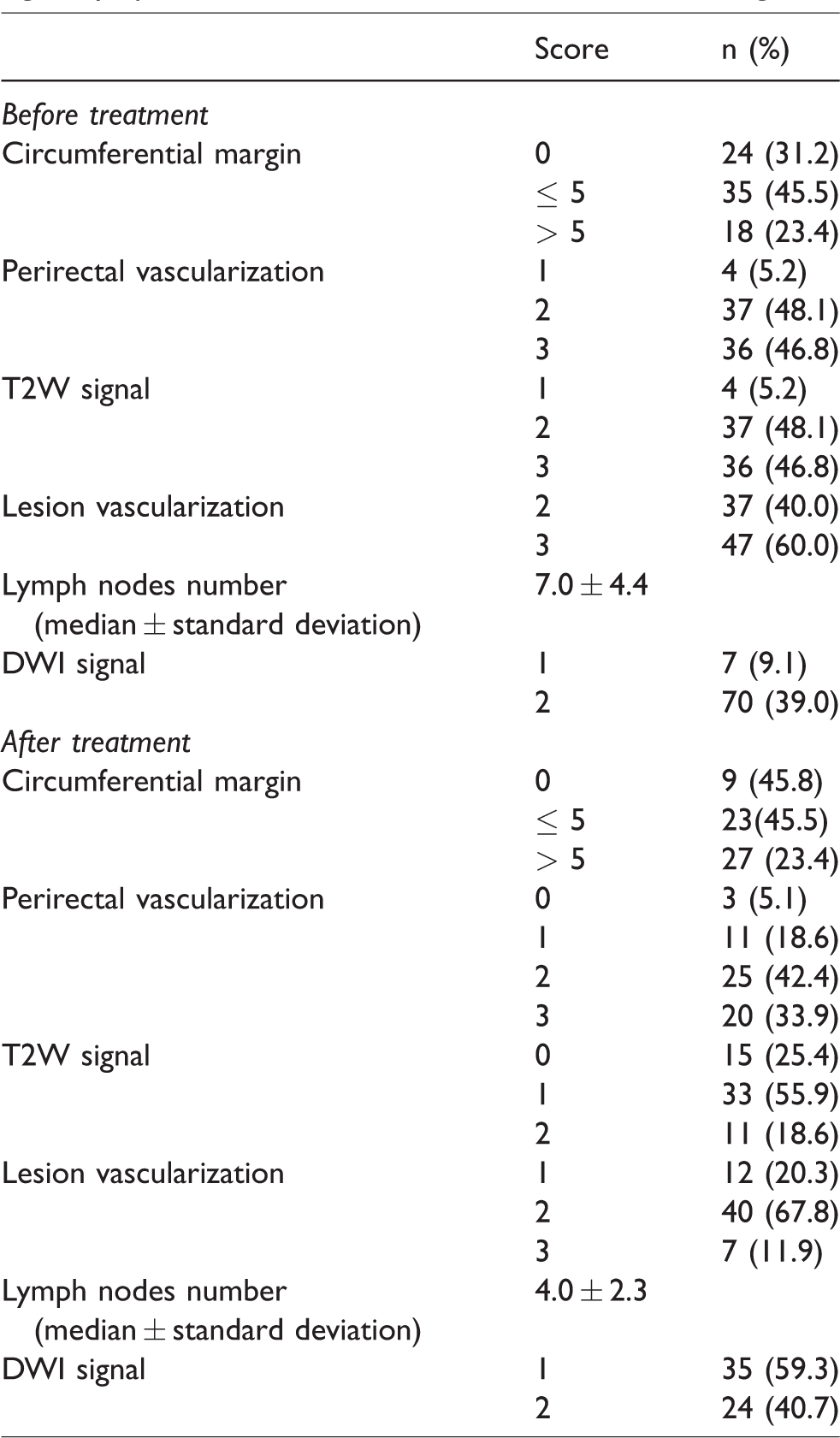
Table 3 reports the correlation coefficients between MRI descriptors before and after treatment with histopathological findings. A low value of correlation statistically significant was observed between T score and lesion vascularization before treatment. Moreover, a low value of correlation that was statistically significant was reported between the N score and perirectal vascularization for the values both before and after treatment (Fig. 2) and between N score and T2W signal before treatment. No correlations were observed between grading score (G) and all extracted MRI variables both before and after treatment.

Woman aged 64 years. Rectal cancer involves the distal channel with involvement of the anorectal junction. (a) T1W FLASH 3D GRE post-contrast medium sequence and (b) TIC in pre-treatment examination; the qualitative assessment shows a type 3 curve with rapid initial and decreasing late enhancement (wash-out). (c) T1W FLASH 3D GRE post-contrast medium sequence and (d) TIC in post-treatment examination; TIC shape is a type 1 with rapid initial and persistent enhancing. Responder patient.
Correlation finding using Rho Spearman coefficient.
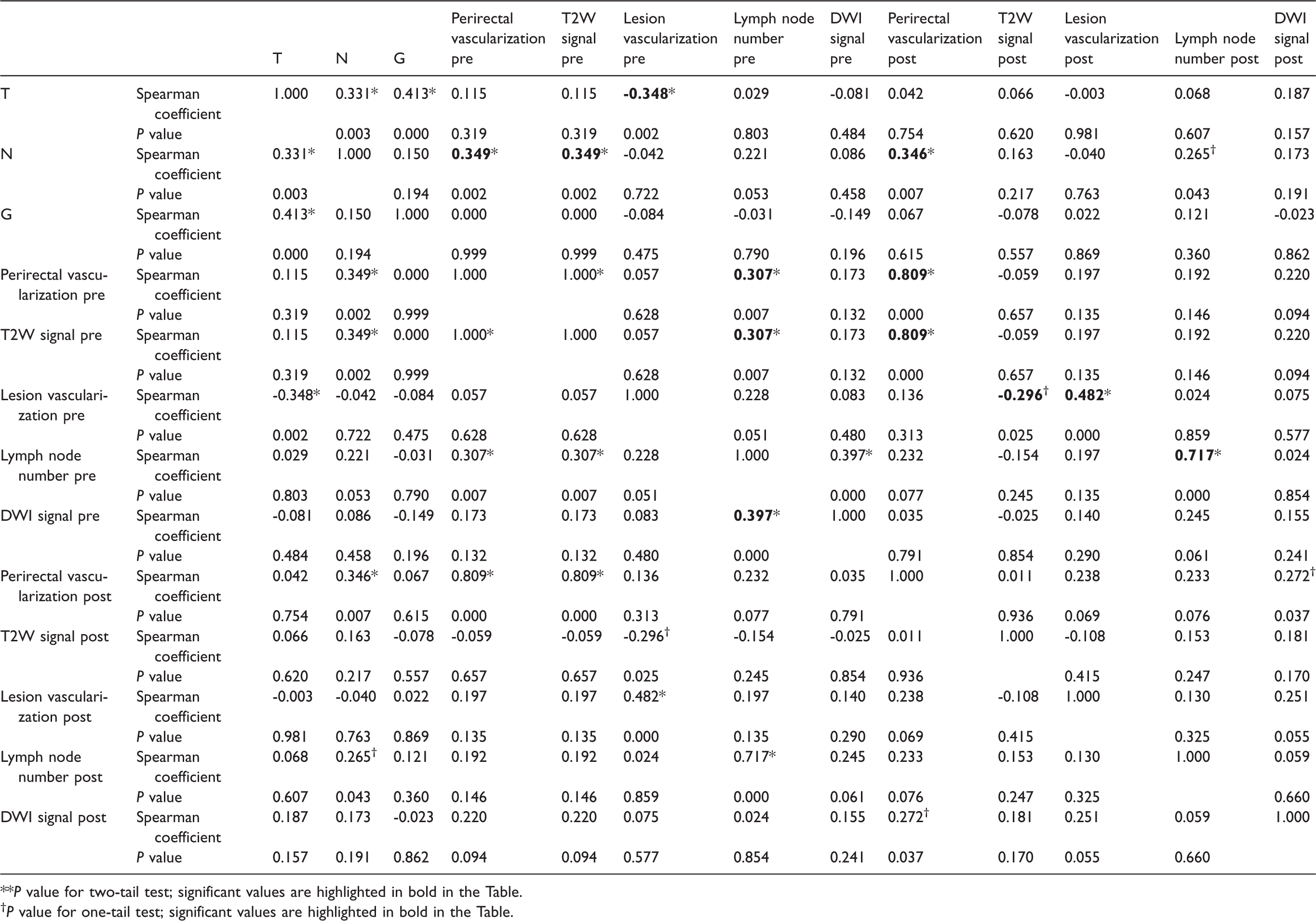
**P value for two-tail test; significant values are highlighted in bold in the Table.
†P value for one-tail test; significant values are highlighted in bold in the Table.
Table 4 reports the diagnostic performance of the best MRI descriptors to predict tumor response after neoadjuvant therapy and to predict local recurrence. Lesion vascularization before treatment (score value ≤2) showed a predictive value of complete pathological response based on pT having an area under the ROC curve (AUC) of 0.65 (95% confidence interval [CI] = 0.51–0.79) with a sensitivity of 88% and a specificity of 50% (Fig. 3a). The results were statistically significant with a P value = 0.04 at Fisher’s exact test (Table 4). Based on TRG, the lymph node number (≤7) before treatment also showed a predictive value of complete treatment response having an AUC of 0.75 (95% CI = 0.59–0.91) with a sensitivity of 83% and a specificity of 57% (Fig. 3b). The results were statistically significant with a P value = 0.04 at Fisher’s exact test (Table 4). Based on TRG, no MR variables with the score system showed significant results in order to differentiate good responder versus poor responder patients .
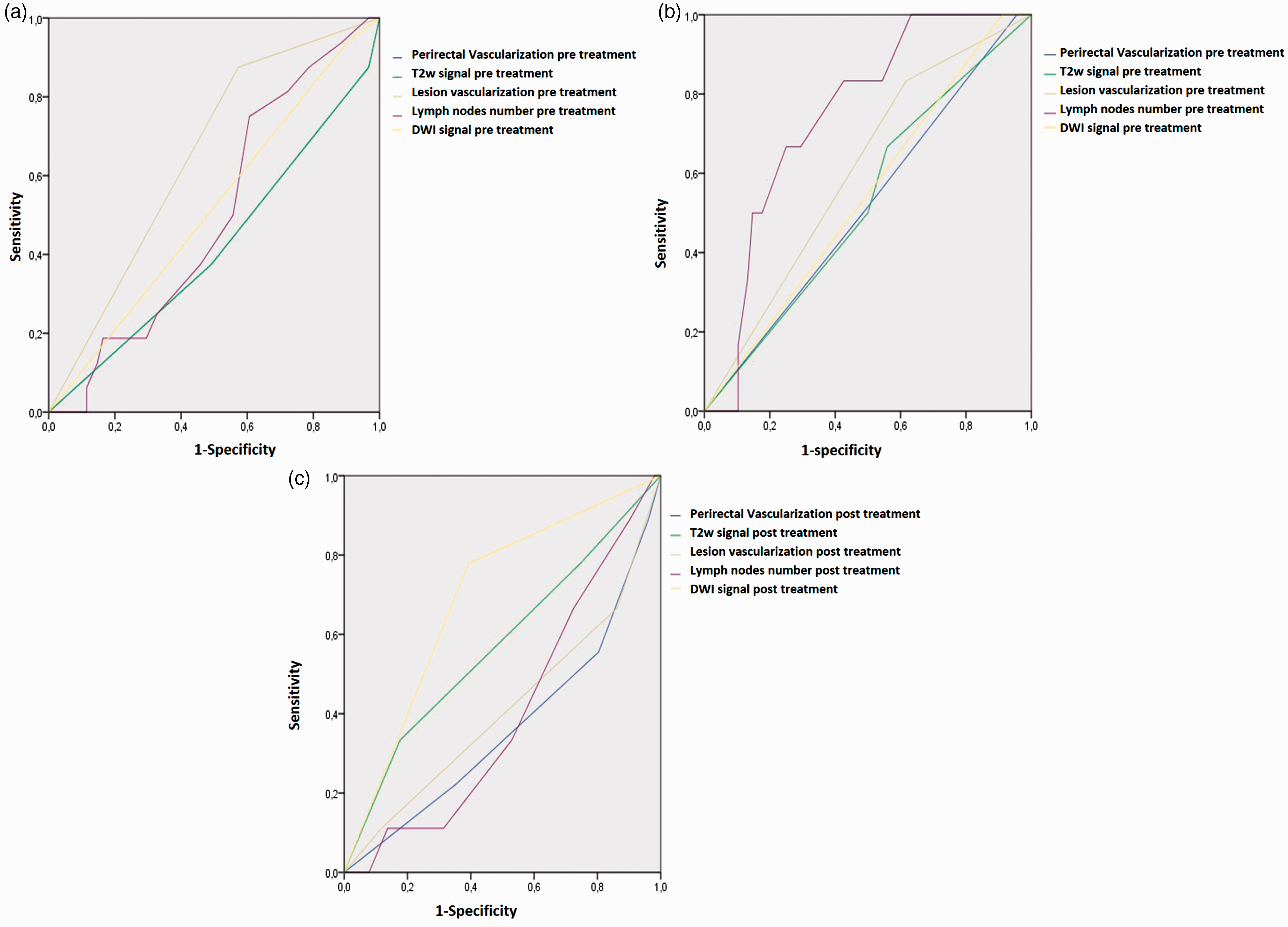
(a) ROC curve to assess predictive value of extracted MRI variables score before treatment to predict pathological complete response based on pT; (b) ROC curve to assess predictive value of extracted MRI variables score before treatment to predict pathological complete response based on TRG; (c) ROC curve to assess predictive value of extracted MRI variables score after treatment to predict local recurrence.
Diagnostic performance of the best MRI descriptors to predict tumor response after neoadjuvant therapy and to predict local recurrence.

T2W SI (score value = 2) and DWI signal (Fig. 4) (score value = 2) after treatment showed a good predictive value for local recurrence (Table 4). The first showed an AUC of 0.57 (95% CI = 0.36–0.79) with a sensitivity of 78% and a specificity of 30%. The second showed an AUC of 0.69 (95% CI = 0.51–0.87) with a sensitivity of 78% and a specificity of 61% (Fig. 3c). However, the results are not statistically significant (P value > 0.05 at Fisher’s exact test) due to the sample size of local rectal recurrences in our series. Moreover, there was the involvement of the CRM in 7/9 (77.8%) patients that had recurrence; all of these patients were subjected to neoadjuvant therapy before TME.
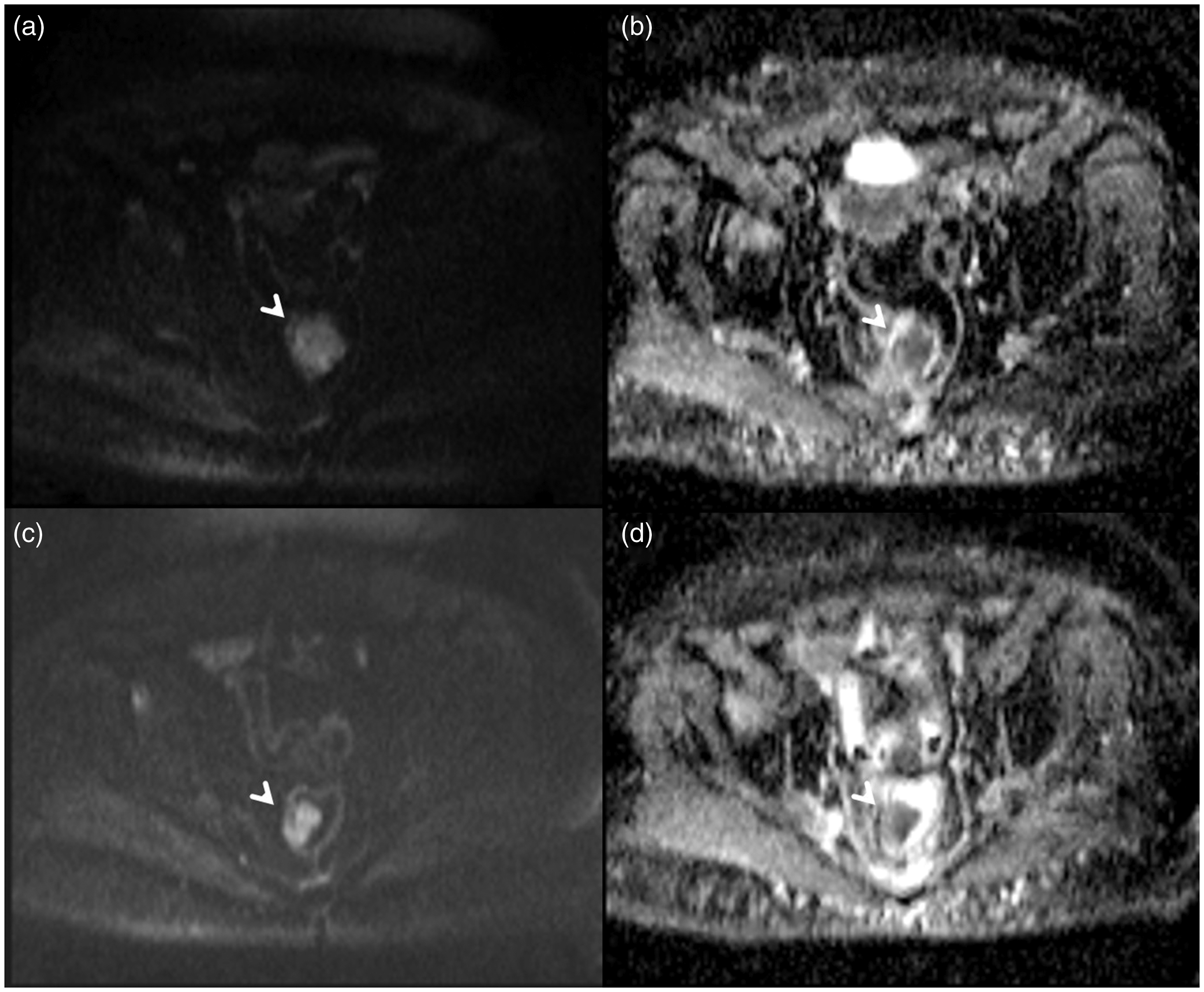
Man aged 62 years. Rectal cancer involves proximal intra–extraperitoneal channel. (a) DWI sequence (b-value 800 s/mm2) and (b) ADC maps: pre-treatment examination; the lesion appears hyperintense with a score of 2: restricted diffusion. (c) DWI sequence (b-value 800 s/mm2) and (b) ADC maps: after CRT treatment, the lesion is hyperintense with a score of 2 similar to pre-treatment examination. Non-responder patient.
Discussion
The therapeutic management of rectal cancers should provide two elements: the first related to oncological radicalism, targeting the local control of the disease and long-term survival; and the second, the preserving of the functional result, preserving the anal sphincter function, and conserving the sexual and urinary function. The assessment of the best therapeutic approach for each patient is considered essential for the evaluation of some prognostic factors (22). In this regard, a primary role has the evaluation of the pathological characteristics of the resected specimen. The pathological stages (TNM stages) and other independent pathological prognostic factors (histological grade, vascular and lymphatic invasion, perineural invasion, and tumor resection margin features) are considered very important predictors of the postoperative outcome (23–26). These prognostic factors could be evaluated in the pre-therapeutic stage by MRI, allowing decision-making in the therapeutic management of patients (27,28). Also, in the post-therapy assessment morphological and functional features on MR study were evaluated to obtain criteria in order to stratify patients into therapy responders, non-responders and incomplete responders (10,11). Many authors described the DWI technique as potentially able to overcome part of morphological MRI limits, being capable of showing viable neoplastic tissue due to its reliability in detecting the restricted proton diffusion in hypercellular tissues with high nucleocytoplasmic ratio. Moreover, researchers investigated the DCE-MRI potential advantages in prediction and in assessment of response to therapy in different tumors (29,30), where neoformed tumor capillaries, being leaky, can determine a rapid gadolinium uptake, an early wash-out, and overall shorter first pass, especially if compared with healthy tissues. In our study, we evaluated some morphological and functional features of MRI that can be of any assistance in the treatment choice for rectal cancer patients to stratify the patients into good responders and poor responders and to predict patients with higher risk for local recurrence.
According to our results, only few extracted MR parameters allow us to stratify the patients into good or poor responders, as the lesion vascularization before treatment showed a predictive value of complete pathological response based on pT. As based on TRG, lymph node number before treatment also had a predictive value of complete treatment response. Moreover, T2W SI and DWI signal after treatment showed a good predictive value for local recurrence. A low statistically significant correlation was observed between T score and lesion vascularization before treatment and between T score and perirectal vascularization. Moreover, a low statistically significant correlation was reported between N score and perirectal vascularization before and after treatment and between N score and T2W signal before treatment. No correlations were observed between grading score and all extracted MRI variables both before and after treatment. Conversely, lesion vascularization before treatment showed a predictive value of complete pathological response based on pT having AUC of 0.65, with a sensitivity of 88% and a specificity of 50%. Based on TRG, lymph node number before treatment was also a predictive value of complete treatment response having an AUC of 0.75, with a sensitivity of 83% and a specificity of 57%. Based on TRG, no score system for each MR variables showed significant results in order to differentiate good responders versus poor responders. To the best of our knowledge, this is the first study that evaluated these parameters in terms of score system to predict pathological treatment response. T2W SI and DWI signal after treatment showed a good predictive value for local recurrence. The first showed an AUC of 0.572, with a sensitivity of 78% and a specificity of 30%. The second showed an AUC of 0.693, with a sensitivity of 78% and a specificity of 61%. Nevertheless, the results are not statistically significant due to the sample size of local rectal recurrences in our series.
However, the potential of our results is that a scoring system could be easier to understand for the radiologist. In fact, it is possible to predict the treatment response looking not at the percentage change but at the categorical value of a parameter .
Different from our results, Choi et al. (31) demonstrated that the apparent diffusion coefficient (ADC) low percentile values have a significant difference between pathological complete response and not pathological complete response groups, demonstrating the utility of the ADC value as a quantitative and objective marker to evaluate complete pathological response to preoperative CRT in rectal cancer. A limit of the study is that we have not assessed quantitatively the ADC parameter to evaluate complete pathological response to preoperative CRT in rectal cancer. Sathyakumar et al. (32) studied the MRI parameters which best predict complete response to neoadjuvant CRT in patients with LARC. The study cohort comprised 64 patients (11 with pathological complete response). The following factors predicted complete response on univariate analysis: low initial tumor volume on T2W high-resolution images and DWI; tumor volume-reduction rate (TVRR) of > 95% on DWI; and complete response on post-CRT DWI as assessed by the radiologist. However, the best MRI predictors were complete response on post-CRT DWI as assessed by the radiologist and TVRR of > 95% on DWI, and these parameters had AUC of 0.881 (95% CI = 0.74–1.0) and 0.843 (95% CI = 0.7–0.98), respectively. The sensitivity, specificity, positive predictive value, negative predictive value, and accuracy of DWI in predicting complete response were 81.8%, 94.3%, 75%, 96.1%, and 76%, respectively; the sensitivity, specificity, and accuracy of TVRR of > 95% as a predictor of CR were 80%, 84.1%, and 64.1%, respectively. However, this difference was not statistically significant.
In our study, we found the involvement of CRM in 7/9 patients that had recurrence (77.8%). All these patients were subjected to neoadjuvant therapy before TME. Ma et al. (33) studied the characteristics and prognostic significance of preoperative MRI-assessed CRM (mrCRM) in rectal cancer. In their study, the relationship between MRI-assessed CRM and pathological CRM (pCRM) was assessed, and survival analysis was used to determine the prognostic significance of mrCRM. Of all the 203 patients, the total accuracy of mrCRM for predicting involvement of pCRM was 84.2%, sensitivity was 50%, and specificity was 86.8%. The three-year local recurrence, disease-free survival, and overall survival rates were 35.6%, 58.1%, and 85.2%, respectively, in patients with involved mrCRM, compared with 8.9%, 78.9%, and 92.3%, respectively, in patients with clear mrCRM. In multivariate analysis, mrCRM found an independent risk factor for local recurrence, with a hazard ratio of 3.49. With these results, the authors concluded that the involvement of mrCRM was significantly associated with local recurrence regardless of pCRM status.
Some potential limitations deserve special consideration: two radiologists evaluated the MR images by consensus and in a single session per patient so that the intra-observer variability was not assessed. We had not assessed the EMVI, which is known be a prognostic indicator for disease recurrence, since patients who show little fibrosis of EMVI following CRT are more likely to develop metastatic disease (34).
In conclusion, according to our results, a proper recognition of some prognostic morphological and functional features such as lesion vascularization and lymph node number before treatment, and T2W SI and DWI signal after treatment could be advantageous during MR examination since these parameters could help to stratify the patients into complete responders and could be useful to identify the local recurrence as soon as possible. However, it is necessary that more studies on morphological and functional MR prognostic parameters are carried out to make the results more robust.
Footnotes
Acknowledgments
The authors thank Alessandra Trocino, librarian at the National Cancer Institute of Naples, Italy. The authors also thank Margherita Foggia for the collaboration.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.