
Abstract
Background
Sentinel lymph node biopsy (SLNB) has been accepted as the standard treatment for axillary evaluation for invasive breast cancer with a clinically negative axilla and the low rate of recurrence after SLNB was reported.
Purpose
To evaluate the performance of screening ultrasound (US) for breast and axillary recurrence detection in breast cancer patients who underwent SLNB.
Material and Methods
We identified 2807 examinations of 562 breast cancer patients who underwent SLNB and received annual screening US combined with mammography (MG) for five years. The cancer detection rate, recall rate, and positive predictive value (PPV3) of biopsies in breasts and breast plus axillae were calculated separately.
Results
During the five-year follow-up period, 21 patients had recurrences of breast cancer (9.8 per 1000 person-year; 95% confidence interval [CI] = 6.0–14.9), including three axillary recurrences (1.4 per 1000 person-year; 95% CI = 0.3–4.1). Screening breast US detected 12 breast cancers. The axillary scanning detected none of the axillary recurrences, but yielded 11.8 recalls per 1000 US screenings; the PPV3 for the breast and breast plus axillae were 18.3% and 15.1%, respectively.
Conclusion
Axillary recurrence was very rare in patient who underwent SLNB; additional axillary scanning did not provide axillary recurrence detection, but only increased the number of false-positive recalls and biopsies.
Introduction
After initial treatment of breast cancer, there remains a risk of subsequent locoregional recurrence in breasts or axillae, or a new primary lesion in the conserved and contralateral breast (1,2). As the number of breast cancer survivors increases, patient management and surveillance strategies after primary treatment are gaining importance (3).
According to previous studies, ultrasound (US) surveillance increased early invasive breast cancer detection in women who had undergone surgery. US detects ipsilateral recurrent or contralateral metachronous breast cancers with higher sensitivity (91–97%) than that of palpation or mammography (MG), which have sensitivities of 45.5–79% and 45–87%, respectively (4–7). In the American College of Radiology Imaging Network (ACRIN) 6666 trial, addition of a single breast US examination to MG increased the detection of small node-negative cancers in women with an elevated risk of breast cancer (8). The supplemental cancer detection yield of US was 4.2 per 1000 women screened (8), and in annual supplemental incidence screening, US identified an additional 3.7 cancers per 1000 screens (9). In the ACRIN 6666 protocol, the axillary scanning was optional, and recording a representative negative imaging was not a requirement. The American College of Radiology (ACR) Breast Imaging Reporting and Data System (BI-RADS) Atlas, 5th edition, also suggests that the axillae could be optionally scanned during screening by whole-breast US examination (10); however, there is no specific guideline for the inclusion of axillary scanning in screening US.
Currently, sentinel lymph node biopsy (SLNB) is known as a standard surgical technique for nodal staging in patients with clinically negative axillae, and its false-negative rate is reported to be as low as 5–7% (11–14). While performing postoperative screening US, the role of US surveillance for axillary recurrence in patients with breast cancer who underwent SLNB or ALND is unclear, and few studies evaluating axillary US scanning for regional lymph node recurrence (LNR) after SLNB. Because SLNB has been accepted as the standard of care for axillary evaluation for invasive breast cancer with a clinically negative axilla, and the low rate of recurrence after SLNB—as reported in several recent studies (15–17)—we hypothesized that inclusion of axillary scanning in whole-breast US screening might not be essential.
Therefore, the purpose of this study is to retrospectively evaluate the performance of screening breast US for breast and axillary recurrence detection in breast cancer patients who underwent SLNB.
Material and Methods
Study population
The institutional review board of our institution approved the review of images and medical records and waived the requirement for informed consent. Since 2002, our outpatient department has offered radiologist-performed whole-breast screening—including the both axillae—with handheld US units, supplementary to MG for women with a personal history of breast cancer regardless of their breast density. We identified 760 consecutive patients who underwent SLNB alone, regardless of mastectomy or breast-conserving surgery (BCS), at our hospital between July 2010 and June 2011. Patients who underwent ALND after SLNB result (n = 180) or who had not received annual follow-up screening during the five-year period (n = 18) were excluded. Finally, postoperative screening examinations during the five-year follow-up period (US examinations [n = 2807] and MG [n = 2359]) which had reference biopsy or at least 12-month follow-up in 562 patients were included in this study (Table 1). Among these women, 65.7% had heterogeneously or extremely dense breasts.
Characteristics of included patients and excluded patients.
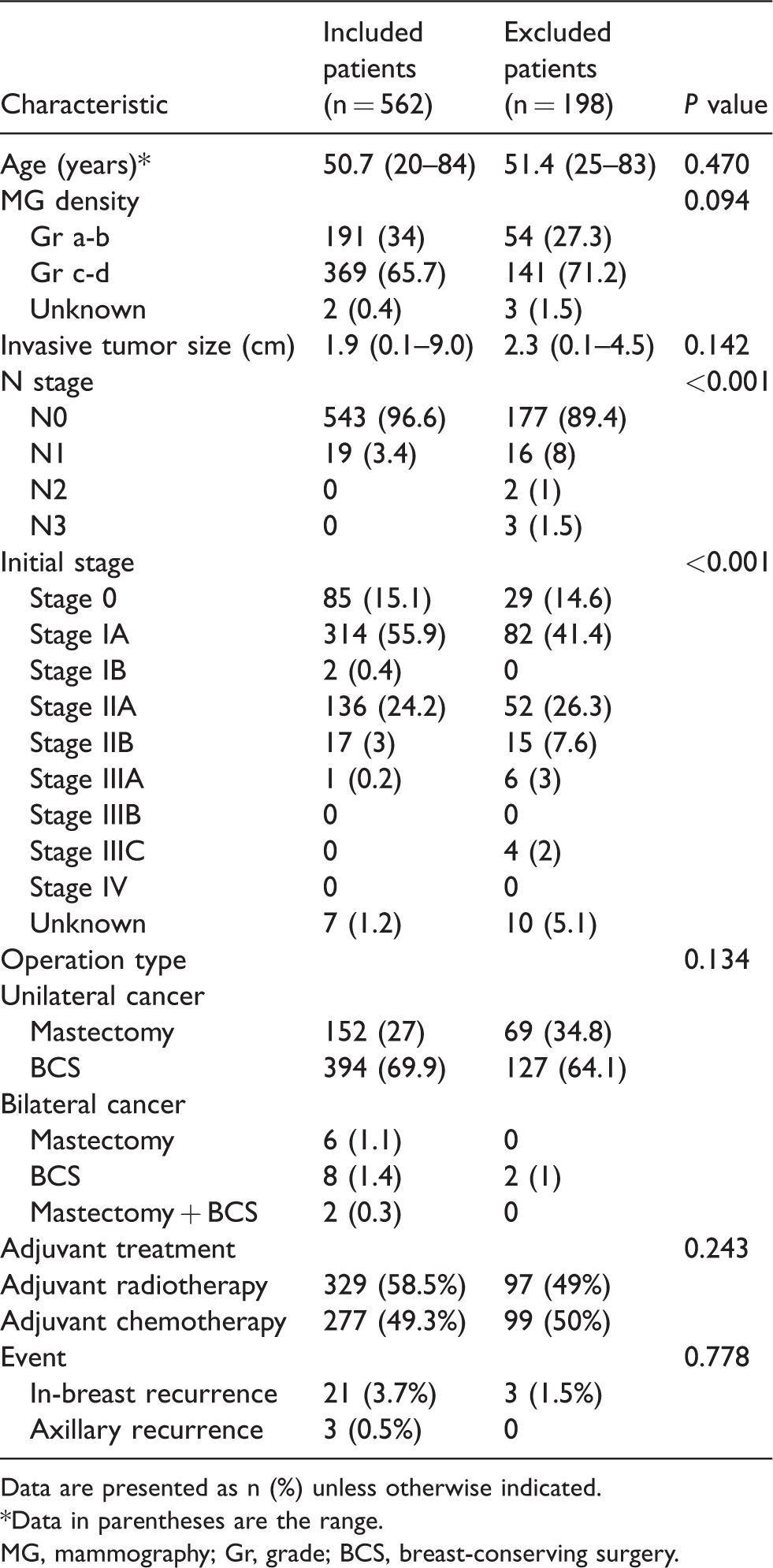
Data are presented as n (%) unless otherwise indicated.
*Data in parentheses are the range.
MG, mammography; Gr, grade; BCS, breast-conserving surgery.
Postoperative imaging surveillance
Every patient underwent clinical examination and regular imaging follow-up after breast cancer surgery. A clinical examination was performed by a surgeon every six months or annually, and MG plus US screening was simultaneously performed for all patients after the clinical examination. Other imaging modalities—such as breast magnetic resonance imaging (MRI), chest computed tomography (CT), and positron emission tomography-CT (PET-CT)—were conducted when clinically indicated according to a clinician’s decision. Mammograms were obtained using dedicated MG units (Senographic2000 DS units [GE Healthcare, Milwaukee, WI, USA]; Selenia Dimensions [Hologic, Bedford, MA, USA]). Routine MG included standard craniocaudal and mediolateral oblique views. Mammographic breast density was determined using the BI-RADS breast density grading system (18). Whole-breast US examinations were performed by the same radiologists who reviewed or interpreted the MGs, using high-resolution US units with a 15–4 MHz linear transducer (EUB-8500 [Hitachi Medical, Tokyo, Japan]; Supersonic [Aix plorer, Aix-en-Provence, France]) and evaluated remaining breast tissue, chest wall, and bilateral axillary area. Symptoms such as palpability of patients were gathered either from previous medical records or direct interview during US examination. Lymph node (LN) US examination of the axillary area from the lower axilla to the junction of the axilla and upper arm was performed; the LNs were evaluated in two orthogonal planes. Suspicious US features of LN recurrence included marked hypoechogenicity, round or irregular shape, cortical thickness >2.5 mm, eccentric cortical thickening, and replaced fatty hilum (19–22). After US image scanning, the radiologist who performed the US examination reported the results of breasts and axillae using BI-RADS final assessment for the MG plus US or US-only screening examination (10).
Outcome measurements and statistical analysis
Clinical, pathological findings of the surgical biopsy and radiologic findings of postoperative screening examinations during the five-year follow-up period were reviewed. Each MG and US report was retrospectively reviewed by two radiologists in consensus. The BI-RADS final assessment category was determined and recorded for the presence or absence of cysts, solid masses, and suspicious LNs. In addition, other image modalities—such as breast MRI, chest CT, or PET-CT—occasionally performed during the follow-up period were reviewed simultaneously.
Outcomes for newly detected abnormal lesions were assessed based on pathology results or follow-up data. Biopsy or surgical pathology reports that indicated cancer were considered the gold standard for malignancy. In participants without history of biopsy or surgery, the reference standard was clinical follow-up at 12 months or later after the last imaging date. Follow-up examinations performed 9–15 months after the last imaging date were considered to be 12-month follow-ups; these were scheduled as per the preference of the participants.
The recurrence rate (patients per 1000 person-years) and cumulative cancer detection rate (patients per 1000 person-years) were presented with a 95% confidence interval (CI) assuming a Poisson distribution. Recall rate and positive predictive value (PPV3) of biopsies in breasts and breast plus axillae were calculated separately on the basis of pathology or follow-up data. The recall rate was defined as the percentage of examinations assessed as categories of 3, 4, or 5. PPV3 was calculated as the number of detected cancers per examination with biopsy performed (23).
To evaluate the effect of axillary scanning, we calculated sensitivity and specificity of the screening strategies using only breast US and breast US with axillary scanning, respectively, and compared the two screening strategies using McNemar tests for clustered data, after categorizing screening results of BI-RADS 1, 2, and 3 into negative, and BI-RADS 4 and 5 into positive. To evaluate sensitivity and specificity considering the clustering of examinations within a patient, we adopted the methods for binary outcome data with cluster by Obuchowski et al. (24). Comparison of sensitivity and specificity was also based on methods that considered the clustering of observations. All statistical analyses were performed using SAS software (version 9.4; SAS, Institute, Inc., Cary, NC, USA).
Results
Postoperative screening examinations and characteristics of study participants
To evaluate the diagnostic performance of the screening strategy with or without axillary scan, we excluded examinations that did not have pathology reports or one-year follow-up results. This resulted in the inclusion of 2807 examinations from 562 patients. Mean follow-up time was 45.9 months (standard deviation [SD] = 6.0), and total follow-up time was 2150.3 person-years. The mean number of screenings per person-year was 1.1 for MG and 1.4 for US examinations, respectively. The mean age was 50.7 years (SD = 10.3) and all participants were women. Unilateral mastectomy had been performed in 152 patients, unilateral BCS in 394, bilateral mastectomy in six, bilateral BCS in eight, and unilateral mastectomy with contralateral BCS in two. After the final pathologic diagnosis, the patients were confirmed to have invasive ductal carcinoma (IDC; n = 437), ductal carcinoma in situ (DCIS; n = 82), invasive lobular carcinoma (ILC; n = 12), mucinous carcinoma (n = 18), papillary carcinoma (n = 4), tubular carcinoma (n = 3), adenoid cystic carcinoma (n = 2), metaplastic carcinoma (n = 1), malignant phyllodes tumor (n = 1), clear cell carcinoma (n = 1), or apocrine carcinoma (n = 1). The mean number of SLNs excised per axilla was six (range = 1–20). Among them, 19 patients were positive for malignancy in SLNB: 16 with N1 breast cancer and three with micrometastases (N1mi). These 19 patients did not undergo ALND and follow-up was done.
Recurrence rates, cancer detection rates, recall rates, and PPV3
The study population had 21 pathologically confirmed cases of recurrence, three of which were diagnosed as axillary recurrence in pathological evaluation of surgical specimens, as well as breast recurrence. Among all cases of recurrence, five cases occurred within two years, and 16 occurred 3–5 years after initial treatment surgery. Thirteen cases were contralateral breast cancer and eight cases were ipsilateral breast tumor recurrence. The initial pathologic diagnosis was confirmed as IDC in 16 patients, DCIS in three patients, ILC in one patient, and tubular carcinoma in one patient. Based on initial surgical results, the mean size of invasive tumors was 2.1 cm (range = 0.1–5.6 cm) after initial surgery, two cases were in the N1 stage, and each case had one positive LN after SLNB.
Among 21 recurrence cases, 12 patients were diagnosed during screening tests (eight cases were detected by combined MG and US, four cases were detected by screening US only); thus, the cumulative detection rate by breast US was 5.6 patients per 1000 person-years (95% CI = 2.9–9.8). However, none of the axillary recurrences were found by axillary US scanning. Specifically, each US breast screening performed with or without MG detected 0 women per 1000 person-year in the first year (95% CI = 0.0−7.3), 3.7 women per 1000 person-year in the second year (95% CI = 0.5−13.5), 3.8 women per 1000 person-year in the third year (95% CI = 0.5−13.9), and 16.5 women per 1000 person-year after the fourth year (95% CI = 7.2−32.6). Among patients with recurrences, nine women received false-negative results. Five cases were detected as interval cancers with palpable symptoms and two chest wall recurrences were detected by chest CT, not by US or MG. The remaining two cases were detected only with breast MRI, and their pathologic confirmations were performed by MR-guided biopsies. Among all cases of recurrence, 10 cases underwent total mastectomy, nine cases were treated with BCS, and the remaining two cases received radiotherapy and chemotherapy after incomplete resection due to the chest wall invasion. In the three cases of axillary LNR, none were detected by screening US examination, but incidentally detected during follow-up surgery (mastectomy with ipsilateral ALND) for in-breast recurrences.
Out of 2807 US examinations, recalls by breast US examination totaled 363, for a recall rate of 12.9% (95% CI = 11.6–14.3). We found 44 recalls by US examination of the axillae (recall rate = 1.6%; 95% CI = 1.1–2.1), which added 33 recalls to recalls by breast US and yielded a 1.2% increase (P < 0.0001 by clustered McNemar test) in the total recall rate (14.1%; 95% CI = 12.8–15.6) without increasing the sensitivity for detection of axillary recurrences when added to the recalls by breast US. Biopsy was performed on 79 breast lesions from 75 patients and on 17 axillary lesions from 17 patients who were reported as BI-RADS categories 4 or 5, having suspicious findings and the remaining 27 axillary lesions were determined as category 3 and short-term follow-up was done. In the 17 axillary lesions that were considered suspicious on US, there were no recurrences (Fig. 1). Among 79 breast lesions, 12 lesions were malignancy that the PPV3 of biopsy was 18.31% in the breast and 15.12% in the breast plus axillae over five consecutive years.
Quantification of the incremental gain by adding US scanning of the axillae to breast US to detect recurrence of cancer
Breast US with or without axillary scanning exhibited very high agreement in binary decisions on cancer recurrence. Table 2 shows the effect of axillae US addition to breast US screening with axillary scanning on the detection of cancer recurrence. Since five additional negative or benign screening US examinations were performed within 12 months before the pathological confirmation, we treated them as false-negative studies using the definition of the reference standard. Therefore, a total of 26 studies had a positive reference standard. While axillary US was not able to detect additional recurrence lesions, it added a small fraction of false-positive decisions for some lesions. Thus, there was no improvement in the detection of cancer recurrence by adding the axillary US to breast US. Although false negatives were dominant in the early follow-up period, true-positive tests became more frequent as the follow-up period lengthened.
Effect on the detection of cancer recurrence by the adding axillae scanning to breast ultrasound screening in terms of the correct classification to diagnosis group.
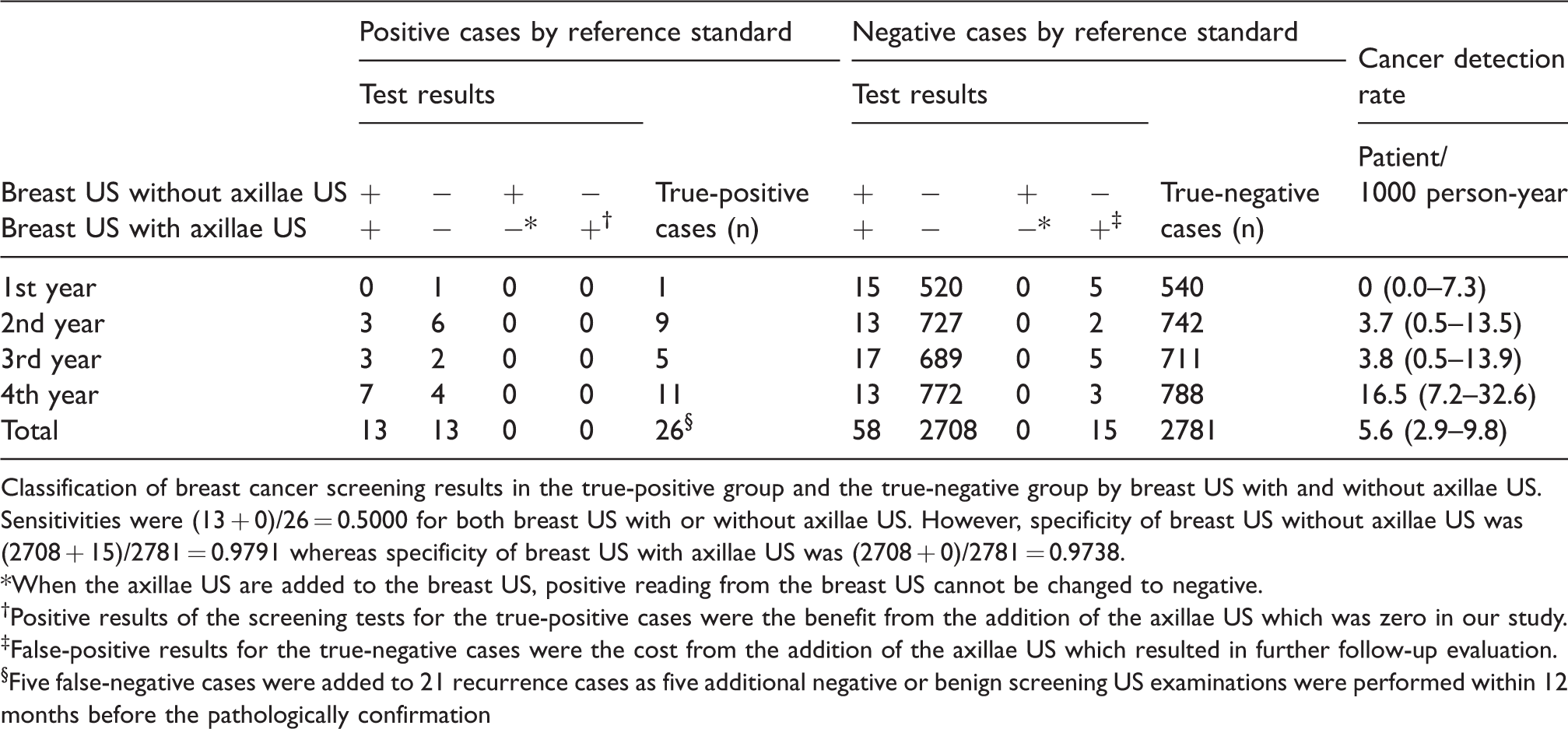
Classification of breast cancer screening results in the true-positive group and the true-negative group by breast US with and without axillae US. Sensitivities were (13 + 0)/26 = 0.5000 for both breast US with or without axillae US. However, specificity of breast US without axillae US was (2708 + 15)/2781 = 0.9791 whereas specificity of breast US with axillae US was (2708 + 0)/2781 = 0.9738.
*When the axillae US are added to the breast US, positive reading from the breast US cannot be changed to negative.
†Positive results of the screening tests for the true-positive cases were the benefit from the addition of the axillae US which was zero in our study.
‡False-positive results for the true-negative cases were the cost from the addition of the axillae US which resulted in further follow-up evaluation.
§Five false-negative cases were added to 21 recurrence cases as five additional negative or benign screening US examinations were performed within 12 months before the pathologically confirmation
Due to the inability to detect any recurrence in the axillae by US, the sensitivity of breast US without axillary scanning was the same as that of the breast US with axillary US. In terms of specificity, however, breast US with axillary US strategy showed significantly lower specificity than breast US without axillary scanning in the McNemar test (P = 0.0001). The false-positive cases made the breast US with axillary US strategy inferior to the breast-only US strategy (Table 3). While the negative test predictive value was the same for both strategies, breast US without axillary US exhibited a higher point estimate in terms of PPV3 (18.31%, 95% CI = 9.33–27.29) than breast US with US scanning of the axillae, in which the 95% CIs mostly overlapped.
Sensitivity, specificity, and predictive values of breast US, axillae US, and breast US with axillae US considering the correlation of the observations due to clustering within the patient.
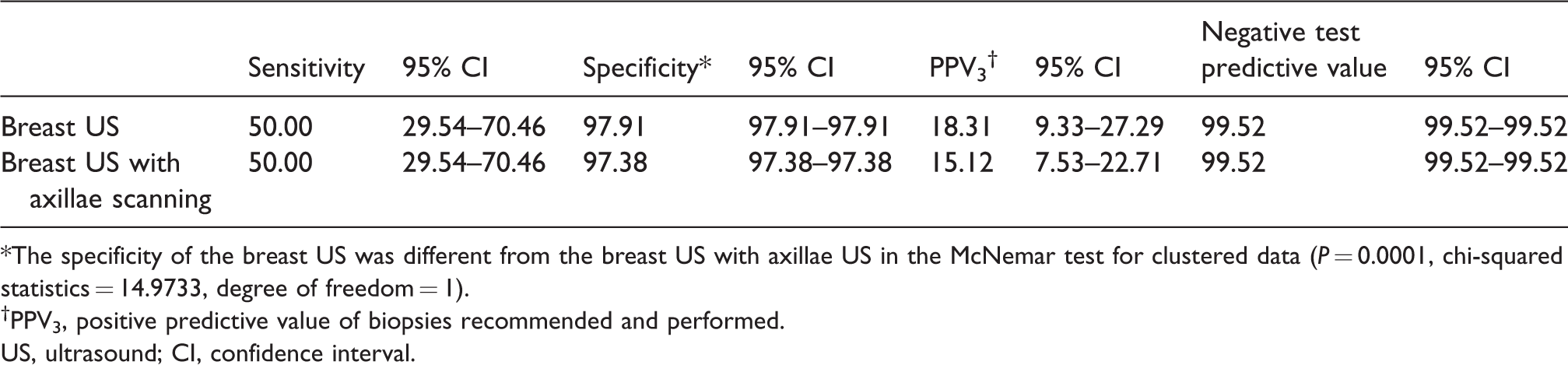
*The specificity of the breast US was different from the breast US with axillae US in the McNemar test for clustered data (P = 0.0001, chi-squared statistics = 14.9733, degree of freedom = 1).
†PPV3, positive predictive value of biopsies recommended and performed.
US, ultrasound; CI, confidence interval.
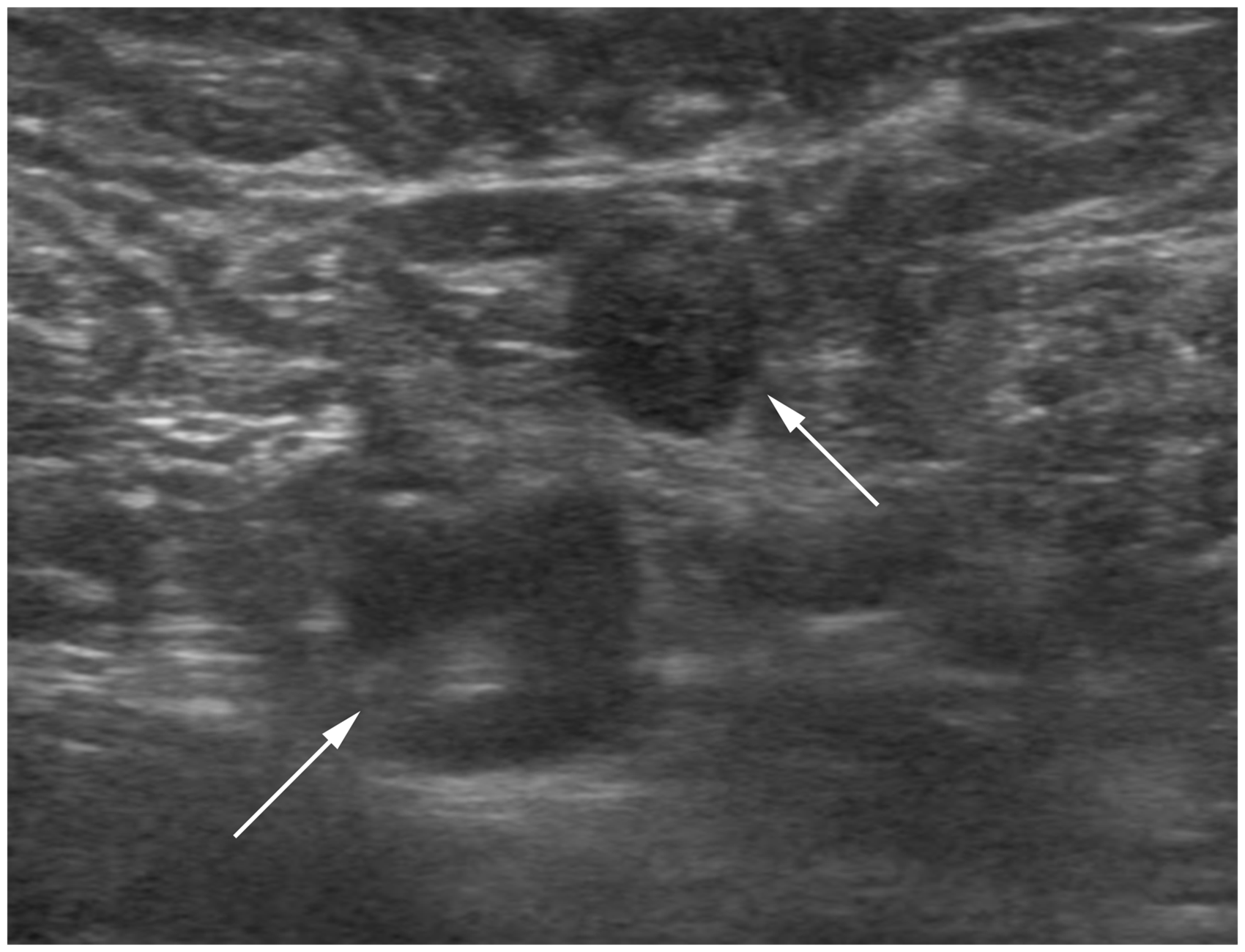
A 55-year-old woman with a history of a right BCS due to IDC 3 years ago. Postoperative US screening shows enlarged lymph nodes (arrows) in the right axilla newly developed when compared to the previous examinations including axilla US and chest CT. The maximal cortical thickness was 3.5 mm (>2.5 mm). US-guided core needle biopsy was done for the lymph node and the pathologic result was reactive lymph node with no tumor. After one year, the size of the lymph node was decreased without any suspicious finding.
Discussion
In this study, we found that, compared with in-breast recurrence, axillary recurrence after SLNB was very rare, and US screenings including the axillae were not helpful in detecting axillary recurrence.
There have been no reliable screening or diagnostic tools to evaluate the axilla; scanning of both axillae with US could be valuable for clinically node-negative patients. The diagnostic performance of US as a tool to evaluate LN metastases has been variable in previous studies. High PPV3 s (69% and 73%) were noted in the preoperative setting (25,26). In patients with known malignancy, when either eccentric nodal cortical thickening or a loss of fatty hilum was considered suspicious, sensitivity was 77% and specificity was 80% (21). In terms of screening, while some reported high sensitivity and accuracy in detecting LNR after ALND or SLNB (27,28), in the ACRIN 6666 trial which included high-risk women, axillary screening US detected only one malignancy among 2498 examinations (33.43% of the 7473 examinations; 0.4 per 1000) (29). In addition, Lee et al. reported that axillary scanning during breast US had no effect on additional cancer detection, but rather increased the number of false-positive results in dense breast women without mammographic abnormality (30). In our study, there was no additional cancer detection when the axillary scan was added and no evidence of axillary recurrence in screening US examinations even in retrospect. In addition to the unsatisfactory diagnostic yield of axillary US, axillary recurrence in patients who underwent SLNB has been reported to be as rare as 0.3–0.7% (15–17), which was similar to our study findings (0.5%, 3 of 562 patients). Thus, the results should be interpreted differently for individual study populations with different treatment methods and follow-up periods (27,28).
Even though recall rates were not high in comparison with the rates for breast lesions on screening US, the high false-positive rate on axillary US screening was undesirable (29). In our study, the recall rate for axillary LNs was only 1.6%; the addition of axillary scanning decreased specificity and PPV3 due to the number of false-positive cases. Although it is not difficult to include axillary scanning in the screening regimen, additional axillary scanning may lengthen the examination time, affecting workflow. In addition, whether to include the axillary region with US screening could be a main factor in utilizing automated breast ultrasound (ABUS) as a screening method. Our data confirming low axillary recurrence detection by US could lead to wider implementation of ABUS, even though more studies with larger data are warranted.
Our study has several limitations. First, this is a retrospective, single-center study. Second, we did not provide incremental data for screening US compared with MG. Our primary aim was to decide whether to add axillary region scanning to breast US. Thus, it was not necessary to provide incremental US data for detecting axillary recurrence in comparison with MG. Third, adjuvant treatment after surgery was not considered. Finally, due to the small number of tumor recurrences, especially in the axillae, the correlation between immunohistochemical subtypes and locoregional recurrence could not be evaluated. To generalize these results, and to confirm the characteristics of locoregional tumor recurrence, a large number of postoperative breast cancer screening populations from multiple institutions are required.
In conclusion, screening US combined with axillary scanning detected in-breast recurrences but did not provide additional axillary recurrence detection in patients who underwent SLNB. The addition of axillary US scanning only increased the number of false-positive recalls and biopsies in these patients. Our study suggests that axillary scanning during postoperative supplemental US screening in breast cancer patients who underwent SLNB is unnecessary.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant from the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (grant no. HI15C1532)