
Abstract
Background
Percutaneous transluminal angioplasty (PTA) is an established treatment of arteriovenous fistula (AVF) stenosis. Drug-coated balloons (DCB) are coated with an antiproliferative drug intended to decrease neointimal hyperplasia and restenosis.
Purpose
To investigate the patency after treatment of restenosis in radiocephalic AVFs with PTA versus DCB.
Material and Methods
A retrospective study comprising 26 patients, recruited from treatment registers, receiving at least one previous PTA and a re-intervention (13 PTAs and 13 DCBs) at the same anatomic location, were observed for 24 months. Patency after re-intervention was compared between the two cohorts. Furthermore, an intra-subject analysis, comparing patency before and after DCB, was performed in the DCB cohort. The Kaplan–Meier method was used to estimate the proportion of stenosis-free patients at different time points after treatment.
Results
After 12 and 24 months, the estimated proportions of stenosis-free patients were 61% and 31%, respectively, in the DCB cohort, compared to 40% and 15% in the PTA cohort. In the intra-subject analysis, 15% and 8% of the patients treated with PTA remained stenosis-free after 12 and 24 months, respectively. Patients treated with DCB had significantly longer patency than patients in the PTA cohort (median 16 vs. 5 months, respectively; P = 0.05). Additionally, in the intra-subject analysis, patency after DCB treatment exceeded PTA (median 16 vs. 5 months, respectively; P = 0.01).
Conclusion
Our results indicate that DCB angioplasty is associated with significantly improved patency in the treatment of restenosis in radiocephalic AVFs. A longer follow-up or randomized controlled trial is warranted.
Introduction
The prevalence of end-stage renal disease (ESRD) has increased over the last 40 years and is still rising (1). Radiocephalic arteriovenous fistulas (AVFs) are well established as the preferred vascular access for patients in need of permanent hemodialysis (2–4), but stenosis is a common cause of dysfunction (5). Percutaneous transluminal angioplasty (PTA) is the preferred treatment for AVF stenosis (6,7). Restenosis is relatively common and the angioplasty itself probably plays an important role in this process (8,9).
Drug-coated balloons (DCB) are coated with paclitaxel, an anti-proliferative drug that inhibits mitosis and cell-proliferation (10). In the arterial bed, DCB has proven to be effective in the treatment of neo-intimal hyperplasia in the superficial femoral artery (11); it is an established treatment for in-stent stenosis in the coronary arteries (12) and it has potential benefits compared with bare metal stents in de novo coronary lesions (13). Some studies seem to indicate improved primary patency of AVFs after DCB (14–20), but the evidence regarding the effect of DCB angioplasty is still limited.
Since 2011, our institution has performed DCB angioplasty in patients with restenosis of AVFs. The aim of this study was to assess and compare the patency of radiocephalic AVFs after restenosis treatment with PTA versus DCB angioplasty.
Material and Methods
This retrospective observational study comprised two cohorts. Both cohorts experienced after previous PTA a restenosis at the same anatomic location, but the following angioplasty (index procedure) was performed using a repeated PTA in one cohort and DCB in the other. The patency (time to restenosis) after the index procedure was compared between the two cohorts. In addition, an intra-subject analysis was performed including all patients in the DCB cohort; in this analysis, the patency of the index procedure was compared to the patency of the previous PTA. The study design is illustrated in Fig. 1. The observation time was 24 months after the index operation for both cohorts. The regional committee for medical and health research ethics approved the study and informed consent was obtained.
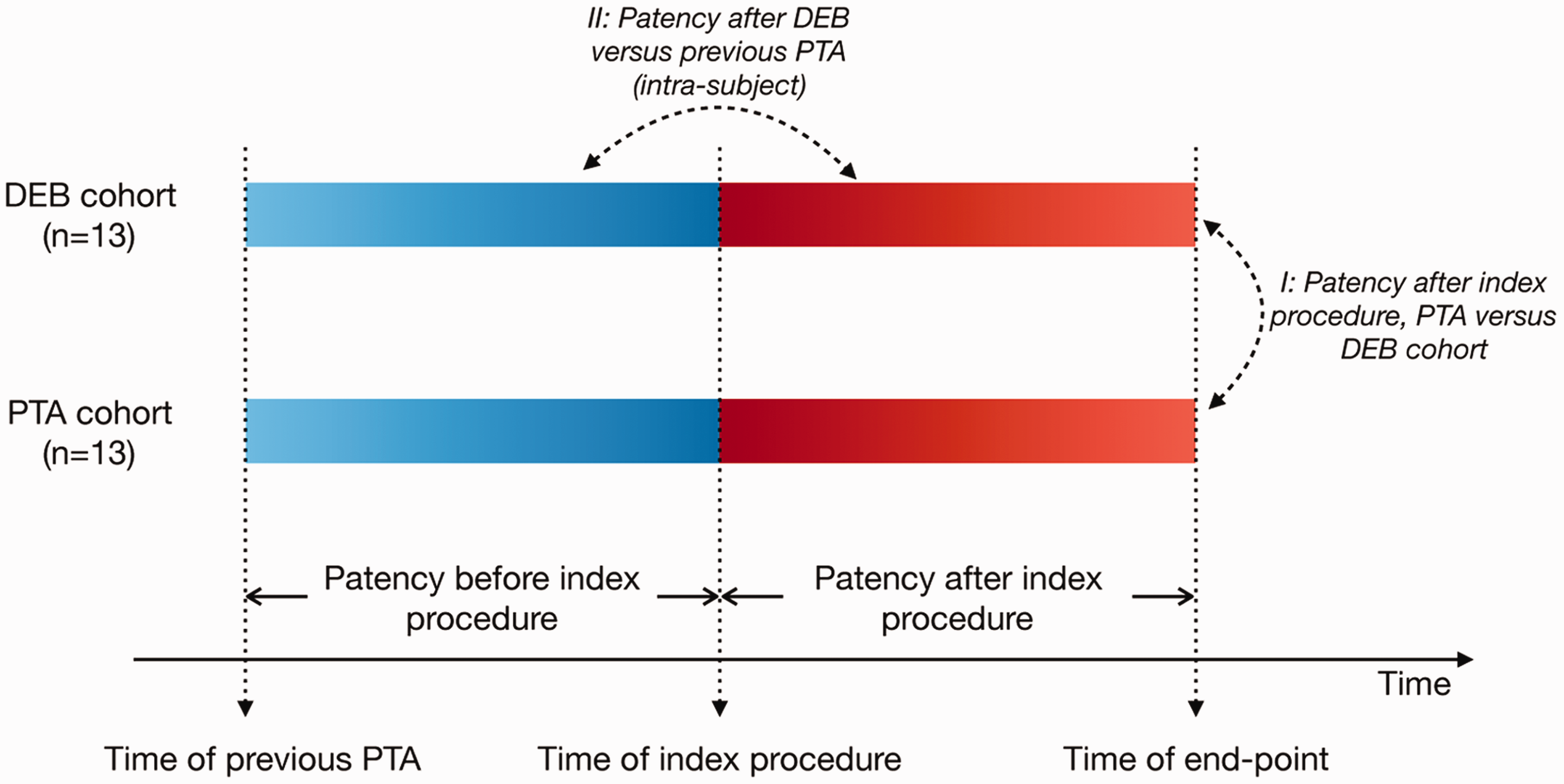
Study design. Two cohorts, each comprising 13 patients. All patients had experienced restenosis after at least one previous PTA. In the following treatment (index procedure), one cohort received angioplasty with DCB, the other cohort with a repeated PTA. Patency was compared between the two groups after the index procedure (I). Additionally, within the DCB cohort, patency after DCB was compared to patency after the previous PTA treatment (II). The endpoints included a stenosis-free period exceeding the observation time (24 months), restenosis, death, kidney transplantation, or loss to follow-up.
All chronic kidney failure patients with a radiocephalic AVFs restenosis who had received at least one PTA at the same anatomic location before the index procedure, from October 2008 to December 2015, were eligible for inclusion. The AVF must have been used for at least one dialysis session before the first PTA. Exclusion criteria were stent treatment of the investigated stenosis and kidney transplantation or death within six months of the index procedure. Patients treated with high-pressure balloon or cutting balloon were not included. The patients were retrospectively recruited based on treatment registers from the Department of Radiology.
Demographic and clinical parameters, characteristics of the stenosis at the time of the index procedure, and the patency of the PTA before the index procedure were investigated to assess potential confounders. Details are shown in Table 1.
Demographic and clinical characteristics of each treatment group.
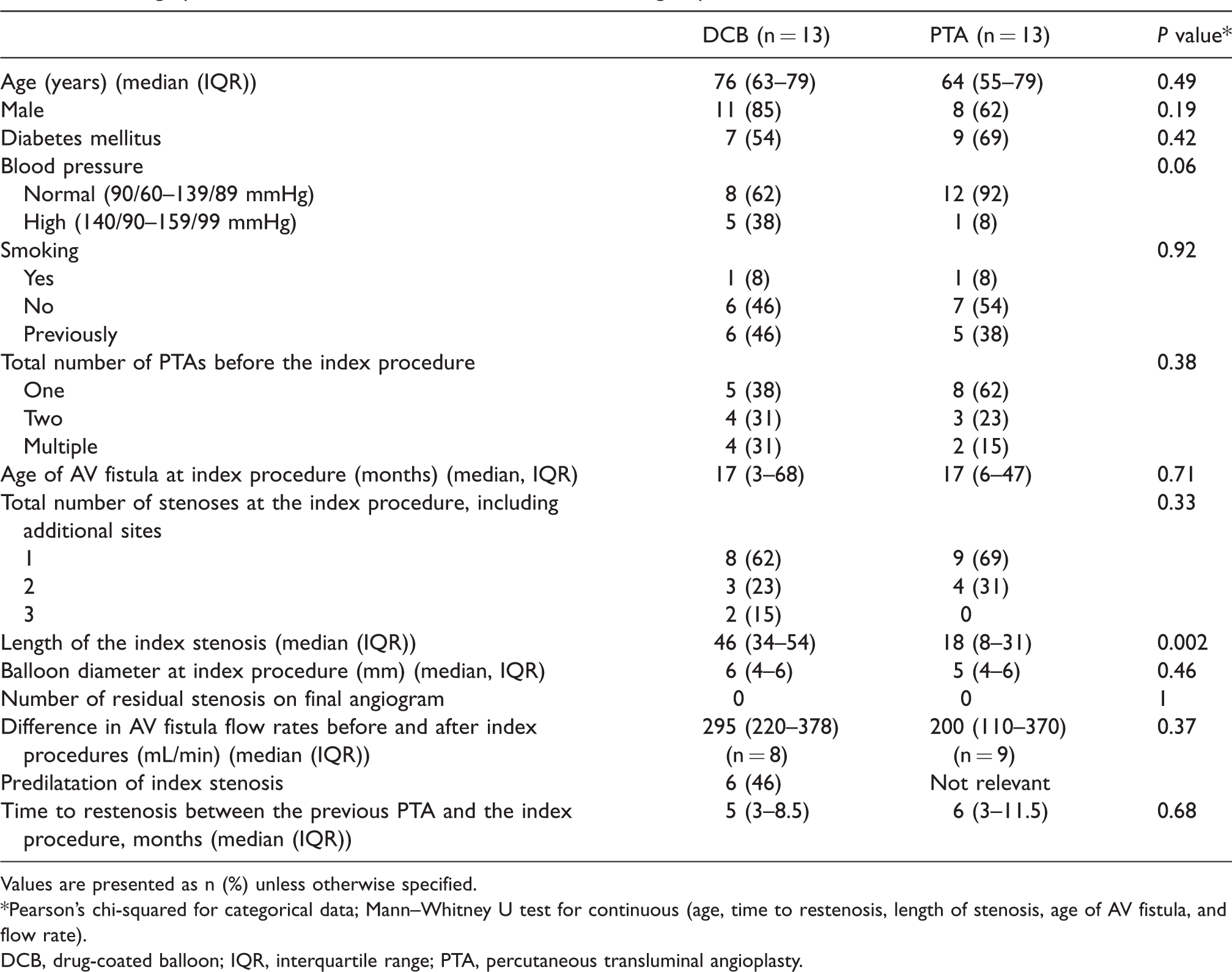
Values are presented as n (%) unless otherwise specified.
*Pearson’s chi-squared for categorical data; Mann–Whitney U test for continuous (age, time to restenosis, length of stenosis, age of AV fistula, and flow rate).
DCB, drug-coated balloon; IQR, interquartile range; PTA, percutaneous transluminal angioplasty.
All data were collected from the patient journals and the local radiological information system.
Observations and devices
All included patients were subject to a dialysis control with a nephrologist every fifth week. The control encompassed an intra-access flow measurement with ultrasound dilution according to the Kidney Disease Outcomes Quality Initiative Guidelines. Decreased flow was individually evaluated based on the patient’s previous flow chart. When a symptomatic stenosis was suspected, the AVF underwent sonographic evaluation by an interventional radiologist and immediate angioplasty was offered for all significant stenosis. Velocity measurements were used to calculate the degree of stenosis and four times increase in peak systolic velocity was considered significant. Each stenosis was also evaluated on digital subtraction angiography. This applied for all patients; hence, the same criteria were used for referrals in both cohorts.
The IN.PACT Admiral (Invatec-Medtronic, Brescia, Italy) was used for all DCB procedures and the balloon was left inflated at nominal pressure for at least 2 min according to the instructions for use. Pre-dilatation of the stenosis could be performed at the discretion of the operator. The Armada 0.035 PTA catheter (Abbot Laboratories, Abbot Park, IL, USA) was used for all PTA procedures. Inflation times for this procedure were not recorded. All patients received i.v. 5000 IU of heparin intraoperatively to prevent thrombosis.
Statistical analysis
The Kaplan–Meier method was used to estimate the proportion of stenosis-free patients at different time points after treatment. The estimated median time to restenosis was reported. The log-rank test was used to compare the stenosis-free time period between the two cohorts; the Wilcoxon test for paired samples was applied for intra-subject analyses comparing the two types of angioplasty within the DCB cohort. A Pearson’s chi-squared test and Mann–Whitney U test were applied to compare the two cohorts with respect to demographic and clinical characteristics. A P value ≤0.05 was considered statistically significant. Analyses were performed with SPSS 25.0 (IBM, Armonk, NY, USA).
Results
A total of 31 patients were identified; 16 were treated with DCB angioplasty and 15 were treated with PTA. Three patients who received DCB angioplasty were excluded (one stent implantation in the investigated stenosis, one kidney transplantation, and one death within six months of the index procedure), whereas two patients who received PTA only were excluded (one stent implantation in the investigated stenosis and one kidney transplantation within six months of the index procedure). Thus, each cohort comprised 13 patients.
The proportion of stenosis-free patients after 12 months was 61% for the DCB cohort versus 31% for the PTA cohort. After 24 months, the numbers were 40% for DCB versus 15% for PTA. In the intra-subject analysis, the proportion of stenosis-free patients after the previous PTA was 15% after 12 months and 8% after 24 months. The number of censored patients during the observation period was three in the PTA cohort (one death, one kidney transplantation, and one rejecting further treatment) and three in the DCB cohort (one death and two kidney transplantations). Patients treated with DCB angioplasty had a significantly longer stenosis-free time period than patients in the PTA cohort (median = 16 vs. 5 months, P = 0.05). DCB angioplasty was also associated with a longer stenosis-free time period than PTA in the intra-subject analysis (median = 16 vs. 5 months, P = 0.01). The survival curves are included in Fig. 2.
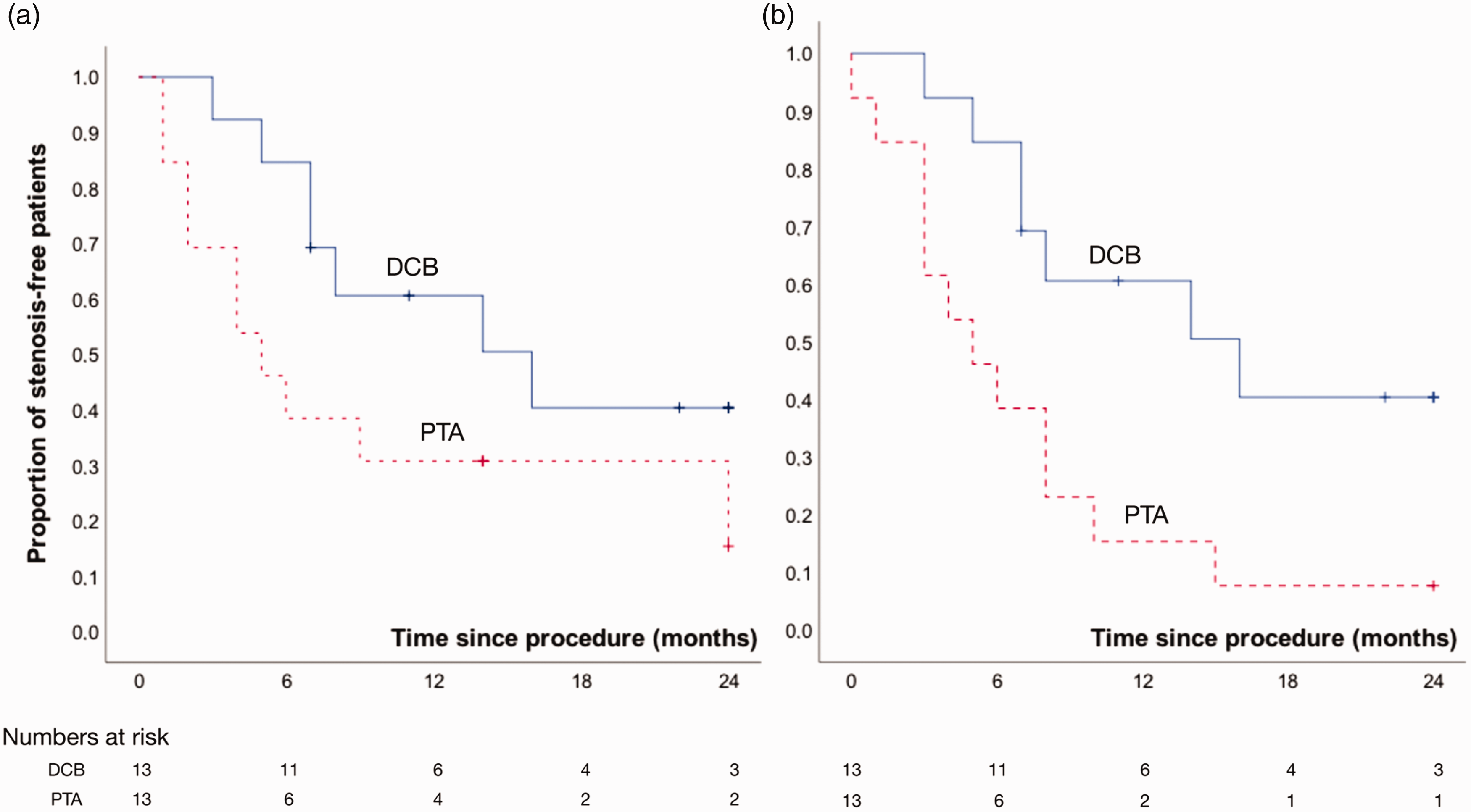
Kaplan–Meier curves showing the expected proportion of patients remaining stenosis-free and the number of patients at risk. (a) Patency after the index procedure in the DCB cohort versus the PTA cohort. In the DCB cohort, patients were censored at date of death (n = 1), date of kidney transplantation (n = 2) and patency exceeding 24 months (n = 3). In the PTA group, patients were censored at date of death (n = 1), date of kidney transplantation (n = 1), and date of rejecting further treatment (n = 1). (b) Intra-subject comparison of patency after DCB versus previous PTA. In this PTA cohort, one patient was censored because the patency exceeded 24 months.
Demographic and clinical characteristics are summarized in Table 1. Patients treated with DCB had a significantly longer index stenosis, but the remaining parameters showed no statistically significant differences. No adverse events were reported and there was no AVF thrombosis.
Discussion
In this study, DCB angioplasty exhibited significantly longer patency both compared to previous PTA treatment in the same patients and compared to a control group receiving only PTA treatment.
The results are consistent with previous studies (14–20) showing that DCB angioplasty is associated with improved patency compared with PTA. Relatively few studies have examined the use of DCB angioplasty in AVFs and sample sizes have, in general, been small. In a randomized control trial (RCT) with 20 patients in each group, Katsanos et al. reported a significantly higher proportion of stenosis-free patients six months after DCB treatment than for PTA (70% vs. 25%, P < 0.01) (14). Irani et al. reported similar results in a prospective RCT, with a target lesion primary patency of 0.81 versus 0.61 (P = 0.03) in the DCB and PTA, respectively, at six months and 0.51 versus 0.34 (P = 0.04) at 12 months (15). In contrast, in another two-cohort study with 26 patients in each cohort, Çildağ et al. found no significant difference in the six-month patency rate (77% vs. 65%, P = 0.45) (16). The 12-month primary patency was reported to be significantly higher in the DCB group than in the PTA group (65% vs. 35%, P < 0.05). These 12-month results corresponded well with the values reported in our current study. Recently, Trerotola et al. published the 180-day results of a prospective multicenter RCT, including 285 patients, finding no significant difference in the 180-day primary patency (71% vs. 63%, P = 0.06) (18). However, according to their discussion, many patients were censured because of the strict 180-day endpoint and when using the common six-month primary patency, a significant benefit of DCB was detected. Both Khawaja et al. and Boitet et al. have published systematic reviews concluding that DCB angioplasty might convey some benefits compared with PTA in terms of improved patency of AVFs (19,20). However, they noted that the studies had numerous limitations: all studies were single-center-based with a small sample size; none were blinded; some included both AVFs and AV grafts in the same results; and some did not separate a new stenosis from a recurrent stenosis.
In contrast to the majority of other studies, our study focused only on a recurring stenosis at a given anatomic location in a radiocephalic AVF. This was done to reduce the effect of potential confounding factors that could influence the comparison of patency following PTA versus DCB treatment. Furthermore, our study did not include patients with AV grafts; patients with stents in their AVF were excluded. This ensured a more homogenous group of AVFs.
Although the effect of DCB is well proven, the optimal DCB design remains uncertain. This has led to an increased attention towards further development and refining of drug-coated balloons. Parameters such as type of drug, drug concentration, delivery time, excipient, solubility characteristics, and more are all of importance, and there are many questions yet to be answered before we have the optimal DCB (21).
Limitations of the study
The index stenosis was significantly longer in the DCB cohort than in the PTA cohort. In addition, although not significant, some demographic data may indicate that a potential bias seems to be in favor of the PTA cohort (e.g. the DCB cohort was slightly older, had higher blood pressures, and more stenosis than the PTA cohort). The overall low number of differences in demographic and clinical characteristics reflects the equitable basis, but underlying differences could be undetected due to small sample size.
A further limitation in our study was that the balloon inflation time at index procedure was not available in the PTA cohort. Additionally, pre-dilatation was used in only six patients before the DCB procedure. Today all operators predilates before the DCB procedure. However, no patients had a significant residual stenosis at the final angiogram. The difference in flow rates before and after the index procedure could be calculated in only eight patients in the DCB cohort and nine patients in the PTA cohort.
This is a retrospective observational study and hence blinded randomization was not possible. Since our institution is the only one performing this type of hemodialysis access maintenance in the region, it is reasonable to assume that the study encompassed all treatments of the included patients, which limits the possibility of selection bias. The population of chronic kidney failure patients in the region is relatively small; hence, the number of patients eligible for inclusion was low. Still, a significant difference in stenosis-free times was observed, indicating a clear difference in treatment efficacy.
In conclusion, this study showed that compared to PTA, DCB angioplasty significantly improves the patency of radiocephalic AVFs treated for restenosis. A longer follow-up or an RCT trial is warranted.
Footnotes
Acknowledgements
The authors wish to thank senior consultant Asbjørn Ødegård at the Department of Radiology, St Olavs Hospital for help with the treatment registers.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Norwegian University of Science and Technology (NTNU) and The Norwegian National Advisory Unit on Ultrasound and Image-guided Therapy funded the study.