
Abstract
Background
The existence of contrast-induced nephropathy is widely accepted. Recent studies suggest its incidence has been overestimated.
Purpose
To determine the effect of intravenous iodinated contrast agents on renal function in patients with chronic renal failure without acute disease that can interfere with the assessment of renal function.
Material and Methods
We prospectively analyzed changes in serum creatinine levels after intravenous administration of iodinated contrast agents in all patients with chronic renal failure (creatinine clearance < 60 mL/min by the CKD-EPI Equation) without acute disease referred for computed tomography (CT) follow-up of aortic aneurysm. Between March 2010 and December 2016, a total of 108 patients met the inclusion criteria. The first 35 patients randomly underwent both contrast-enhanced and unenhanced CT examinations six months apart; the 73 following patients underwent only contrast-enhanced CT examinations. Serum creatinine levels were recorded immediately before and 48–72 h after CT examinations. Contrast-induced nephropathy was defined as an increase of ≥25% in serum creatinine from baseline levels.
Results
In the first 35 patients, mean changes in creatinine levels after unenhanced and enhanced CT examinations were similar. From the total of 108 patients who underwent contrast-enhanced CT, serum creatinine increased > 25% with respect to baseline in only two patients, in one case after contrast-enhanced CT examination and in the other after unenhanced CT examination; in a third patient, serum creatinine decreased >25% after contrast-enhanced CT examination.
Conclusion
No relevant contrast-induced nephrotoxicity was detected in this group of patients with chronic renal failure without acute disease.
Keywords
Introduction
Contrast-induced nephrotoxicity (CIN) is defined as acute kidney injury attributed to the intravascular administration of iodinated contrast material. The existence of CIN has been widely accepted in the literature, although its incidence has been controversial due to the wide range of findings published (up to 30%) (1).
In a retrospective study to determine the incidence of CIN after computed tomography (CT) examinations, Davenport et al. (2) found that intravenous iodinated contrast material was nephrotoxic only in patients with creatinine clearance < 30 mL/min/1.73 m2, with a trend toward significance at 30–44 mL/min/1.73 m2. Some authors have claimed that the real incidence of CIN is much lower than previously thought (3–8). Two factors can lead to overestimating the real incidence of CIN: spontaneous fluctuations in serum creatinine (SCr) levels (9–11) and the presence of acute disease that may affect kidney function (12).
In order to assess the effect of these two factors, recent studies have included control groups of patients not administered iodinated contrast material and many found no differences in the incidence of nephrotoxicity between patients administered contrast material and controls (7,13–17). Similarly, after adjusting for presumed risk factors for acute kidney injury, some retrospective studies found no differences in nephrotoxicity between cohorts exposed versus those unexposed to iodinated contrast material (18–23).
We aimed to determine the incidence of CIN in patients with chronic renal failure without acute conditions that may interfere with kidney function.
Material and Methods
Our institutional review board approved this prospective observational study and all patients provided written informed consent.
Inclusion criteria: all outpatients referred for CT follow-up of aortic aneurysm who had chronic renal failure, defined as creatinine clearance <60 mL/min by the CKD-EPI equation. Exclusion criteria: patients on hemodialysis and those with acute conditions that may affect kidney function. The following data were obtained from electronic medical records: age; sex; medical history (including diabetes, hypertension, dyslipidemia, ischemic heart disease, cerebrovascular accident, and peripheral vascular disease); and medical treatments administered.
To avoid CIN in patients with chronic renal failure undergoing CT for aortic aneurysms, our center’s protocol alternated between contrast-enhanced CT and unenhanced CT studies every six months. For contrast-enhanced examinations, all patients received 1.2 mL/kg of iopromide 300 mg/mL (Ultravist®, Berlimed S.A.; Alcalá de Henares, Spain). Patients received no nephroprotective treatment or special hydration before the examination but were advised to drink plenty of fluids after the examination.
SCr levels were recorded immediately before the CT examination (baseline) and 48–72 h after CT examination (post-examination). The difference between the baseline and post-examination SCr values were calculated. CIN was defined as a ≥25% increase in SCr from baseline.
In the descriptive statistical analysis, categorical variables are reported as absolute and relative frequencies; continuous variables are expressed as means and standard deviations.
To compare baseline and post-examination SCr, we used Student’s dependent t-test for paired samples and Pearson correlation coefficients; significance was set at P < 0.05. SPSS version 18.0 (SPSS, Chicago, IL, USA) was used for all analyses.
Results
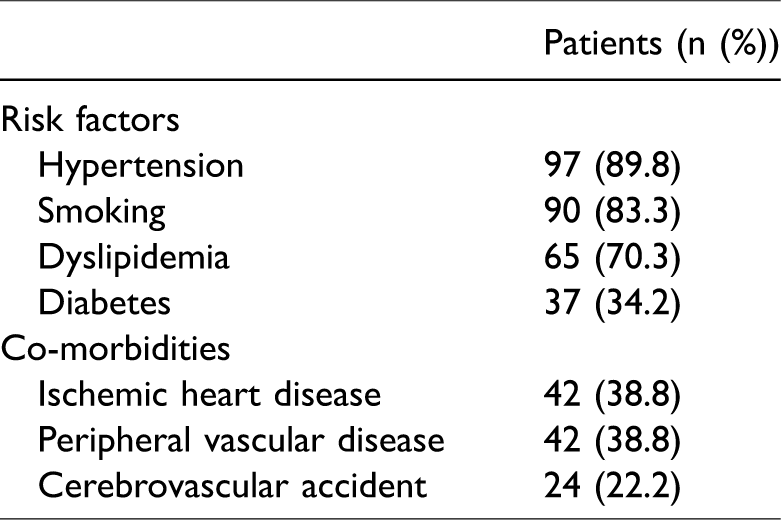
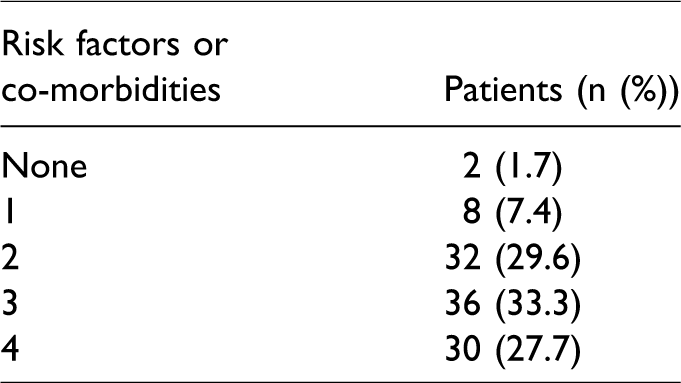
Between March 2010 and December 2016, a total of 420 patients underwent CT examinations to follow up aortic aneurysms. Of these, 162 (38%) had chronic renal failure, but 54 were excluded (39 refused to participate in the study, 13 were on hemodialysis, and two had acute conditions that could affect kidney function). Thus, the data from 108 patients (107 men; mean age = 77.4 years, age range = 59–95 years) were analyzed. Table 1 summarizes patients’ risk factors and co-morbidities. All but two patients had risk factors and 90.6% had two or more risk factors (Table 2). Table 3 reports patients’ stage of chronic kidney disease.
Patients’ risk factors and co-morbidities.
Risk factors and co-morbidities per patient.
The stages of chronic kidney disease.
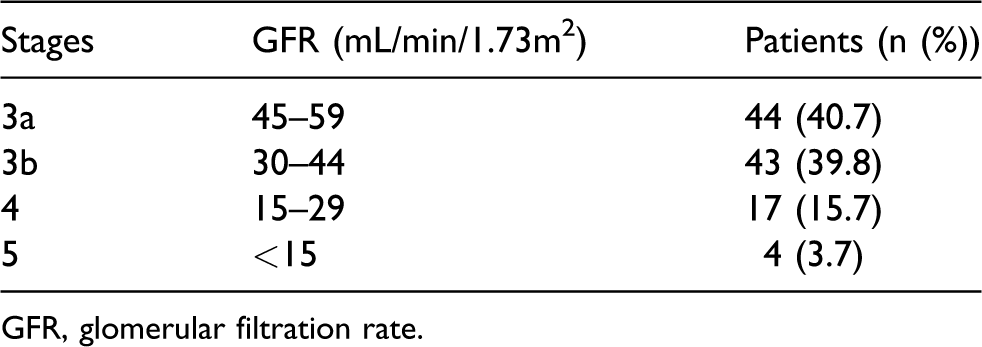
GFR, glomerular filtration rate.
The first 35 patients underwent both contrast-enhanced and unenhanced CT examinations in accordance with the protocol in force. However, as no statistically significant differences were observed between the mean changes between baseline and post-examination SCr, we decided to use contrast material for all examinations in the remaining 73 patients.
In the 35 patients who underwent both unenhanced and contrast-enhanced CT, mean baseline SCr was 1.56 mg/dL before unenhanced and 1.60 mg/dL before contrast-enhanced examinations (paired-sample correlation = 0.89). After both examinations, mean SCr increased slightly with respect to baseline levels 0.049 mg/dL after unenhanced versus 0.026 mg/dL after enhanced studies (P = ns).
The graph in Fig. 1 plots the difference in each patient between the SCr level before (baseline SCr) and after contrast-enhanced CT (deviation from baseline) for each of the 108 patients. Importantly, SCr levels fluctuations depended on the degree of renal function: the worse the renal function, the greater the differences in SCr.
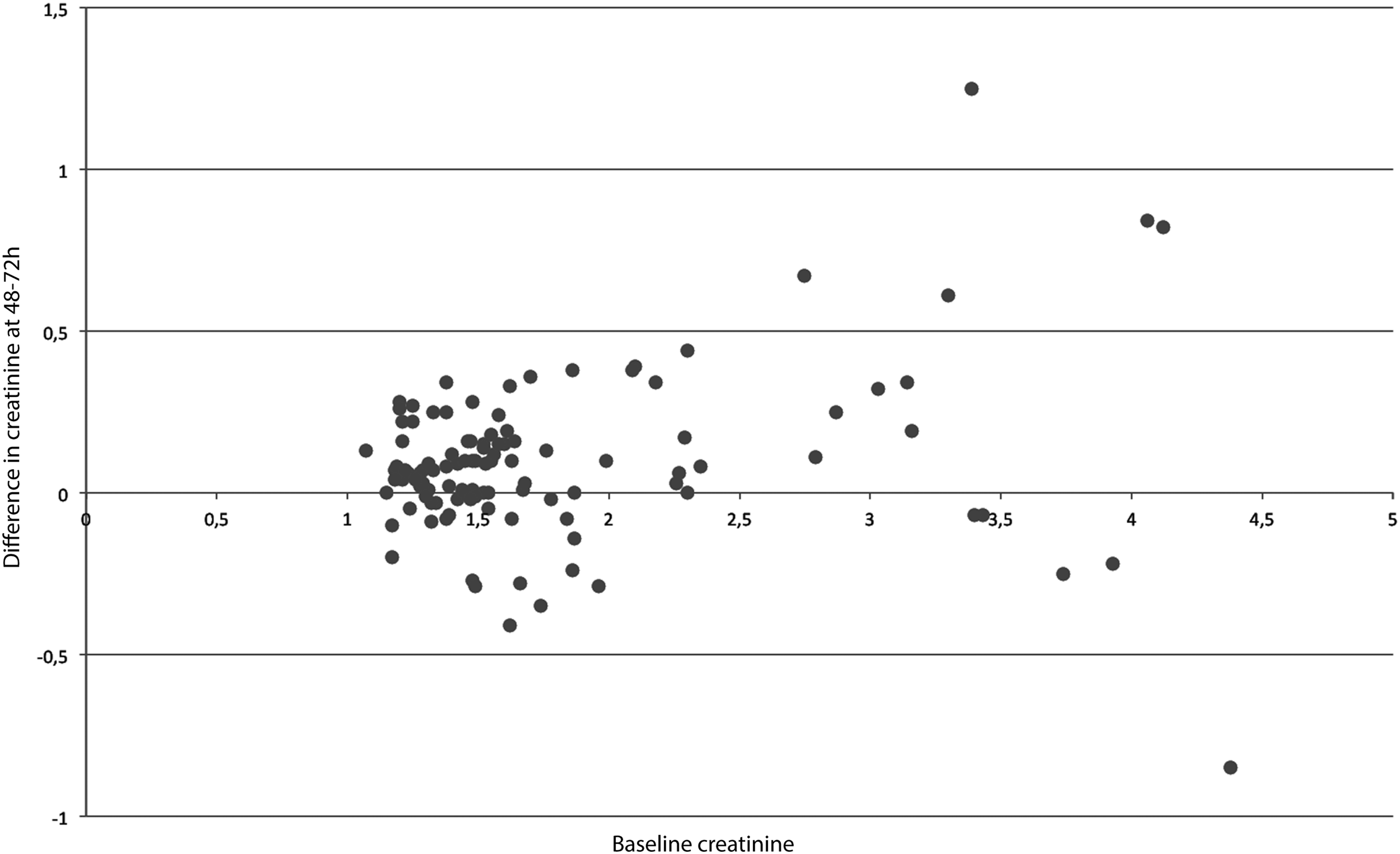
Difference in each patient in the SCr level before (baseline SCr) and after contrast-enhanced CT (deviation from the baseline).
In two patients, SCr levels after the examination were >25% higher than at baseline, in one after a contrast-enhanced examination and in the other after an unenhanced examination. In a third patient, SCr after contrast-enhanced CT was > 25% lower than baseline. In the two patients in whom SCr increased > 25%, SCr had returned to baseline levels at a follow-up 10 days later; in the patient in whom SCr decreased > 25%, SCr had returned to baseline level at a follow-up 21 days later.
Discussion
In our sample of patients with chronic renal failure, we found no evidence that the administration of contrast material affected kidney function. In the group of 35 patients who underwent both unenhanced and enhanced CT, variations in SCr from baseline did not differ with administration of contrast material; SCr increased slightly after both unenhanced and contrast-enhanced CT examinations (0.049 mg/dL after unenhanced versus 0.026 mg/dL after enhanced studies; P = ns).
Furthermore, in the 108 patients who underwent contrast-enhanced examinations, changes in SCr values >25% were observed in only three. One case occurred after an unenhanced CT while the other two occurred after contrast-enhanced examinations. Interestingly, SCr actually decreased in one of these patients after contrast-enhanced CT. Thus, SCr increased by >25% in only one of the 108 patients who underwent CT after intravenous contrast administration.
The increase in SCr > 25% observed in the patient who did not receive contrast material can clearly not be attributed to intravenous contrast administration. Likewise, it would be nonsensical to attribute the > 25% decrease in SCr to intravenous contrast administration. Therefore, why should we attribute the > 25% increase in SCr in the other patient to intravenous contrast administration?
These isolated cases probably reflect variations in SCr due to asymptomatic conditions or undetectable clinical circumstances that are unrelated to the use of iodinated contrast material. A review of the electronic medical records revealed that SCr values in these three patients returned to baseline levels within 21 days after CT examination.
These findings are especially relevant because our patients were particularly fragile. All had chronic renal failure, were elderly (mean age = 77.4 years), and had significant co-morbidities: 90% were hypertensive and 34.2% were diabetic, all considered at high risk (24–26).
Our results also reflect spontaneous fluctuations in SCr, which increased in some cases and decreased in others. Our results corroborate those of other studies that found that the magnitude of these fluctuations increases with higher baseline SCr (9–11,19). This is the reason why our definition of CIN did not include the criteria of an absolute increase in SCr ≥ 0.5 mg/dL, used in some studies. In patients with high baseline SCr, an increase of 0.5 mg/dL may represent normal fluctuations in baseline SCr rather than CIN (10). This may explain why studies that considered an absolute increase of ≥0.5 mg/dL CIN not only found a higher incidence in patients with high baseline levels, but also found a higher proportion of controls who met the criteria for CIN even though they had not received iodinated contrast material (11,19,23).
The main limitation of the present study is the small sample and larger prospective studies would be necessary to strengthen our conclusions. However, given the low incidence of CIN, large prospective studies would be difficult to organize. Moreover, large retrospective studies using propensity-matched cohort analysis have found that the incidence of CIN is very low or non-existent (2,8,19,21,23). Nevertheless, to avoid the risk of CIN clinicians, studies often opt for unenhanced CT examinations; thus, the findings of our prospective study in this series of patients with specific conditions may help convince clinicians that the risk of CIN is often negligible.
In conclusion, in our group of patients with chronic renal failure without acute disease that may affect kidney function, intravenous administration of iodinated contrast material had no relevant effect on SCr. Many cases of acute kidney dysfunction attributed to CIN may actually be due to the effects of intercurrent disease or normal fluctuations in SCr. There is no need to avoid the administration of iodinated contrast in patients with chronic renal failure. Not performing enhanced CT when necessary to gain valuable information is probably worse for the patient than the risk of CIN.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.