
Abstract
Background
Retention of conception products is a common complication following delivery and remains a diagnostic and management challenge due to non-specific symptoms and ultrasound findings.
Purpose
To introduce a clinical approach for managing patients with suspected retained products of conception following delivery.
Material and Methods
The ultrasound examination included gray-scale and Doppler parameters which classified the patients into three groups: high, moderate, or low probability for retained products of conception. The same classification was used both to stratify individual risk for retained products of conception, as well as for counseling the appropriate management.
Results
The study included 66 patients. Retained products of conception was confirmed in 62%, 32% and 0% of the high, moderate and low probability groups, respectively. Additionally, each group was further divided according to the timing of the ultrasound examination: before or after 42 postpartum days. A significant increase, from 12% to 64%, in the positive predictive value was observed in the moderate probability group when the ultrasound was performed ≥ 42 days postpartum.
Conclusions
In the low probability group, no surgical intervention is recommended. When ultrasound findings are classified as high probability for retained products of conception, surgical evacuation of the uterine content is recommended. For clinically stable women with ultrasound findings consistent with moderate probability, ultrasound follow-up at the end of the puerperal period (42 days) is recommended. This approach may improve the sonographic prediction of retained products of conception and prevent unnecessary interventions.
Introduction
Retention of conception products is a common and treatable complication of labor and delivery. The incidence of retained products of conception (RPOC) after routine vaginal delivery is thought to be 3–5% (1) and it may also occur after cesarean delivery (2). Symptoms are not specific and may include prolonged postpartum hemorrhage, fever, and abdominal pain. When diagnosis of RPOC is confirmed, the common practice is a surgical uterine evacuation, which might lead to other complications, such as: uterine perforation; cervical laceration; and long-term intrauterine adhesion (3). Pre-procedure accurate assessment is therefore crucial to avoid unnecessary intervention. Ultrasound (US) is usually the first-line imaging modality in the evaluation of suspected RPOC, due to its non-invasive nature, high availability, and high reproducibility. However, occasionally, the US diagnosis of RPOC might be non-specific due to overlapping findings with other conditions such as blood clots or necrotic decidua (4). Gray-scale US findings, which were found to be suggestive of RPOC, include an endometrial echogenic mass, thick endometrium, or complex endometrial fluid.
Of these findings, endometrial mass was the most sensitive and specific finding, with a positive predictive value (PPV) of 59% (5). Recent studies have indicated the important contribution of color Doppler US in order to enhance RPOC diagnostic accuracy. Detection of vascularity in a thickened endometrium or endometrial mass has increased the PPV for the diagnosis of RPOC to 65%–100% (6–8). Demonstrating intrinsic vascularity is helpful to distinguish simple clots and decidua, which may resemble RPOC on gray-scale imaging, from true RPOC.
We developed a clinical approach suggestion to managing cases with suspected RPOC based on gray-scale and color Doppler US findings.
The aim of the present study was to check the efficiency of this approach in terms of RPOC predictability and counseling for the appropriate management.
Material and Methods
In the present study, we reviewed the files of women who were referred for suspected RPOC to our Prenatal Ultrasound Unit during 2015 and 2016. Inclusion criteria were women after third trimester delivery, having risk factors for RPOC, such as: manual lysis, suspicious appearance of the placenta following delivery, or an adherent placenta. Women with symptoms (such as vaginal bleeding, abdominal pain, or fever) and abnormal intrauterine US findings were also included in the study. Scans were performed with either a 2–4-MHz curvilinear abdominal transducer or a 5–9-MHz transvaginal probe using either a General Electric Voluson 730 Expert Professional US or E8 systems or E10 (GE Medical Systems, Milwaukee, WI, USA). All scans included gray-scale and Doppler imaging. Sonographic images and patients’ reports were stored electronically in the hospital’s archive.
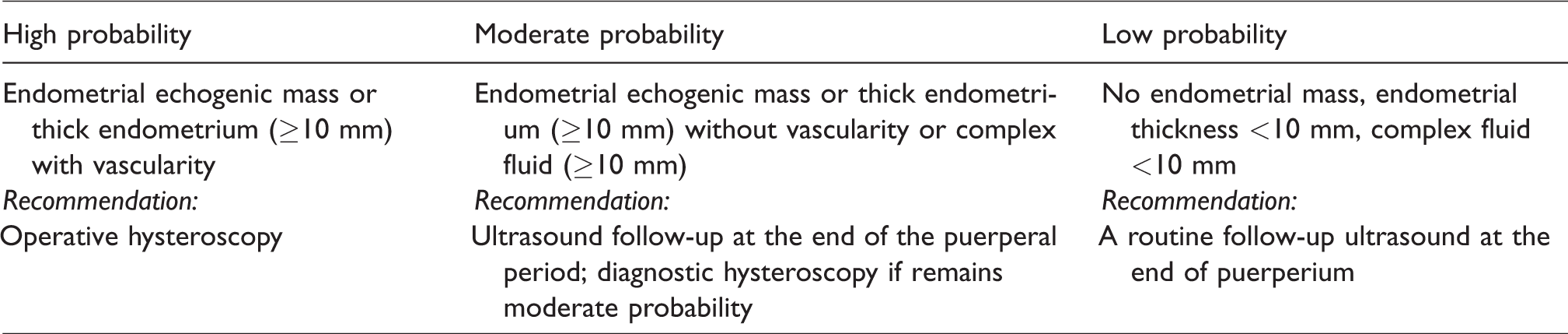
The US evaluation was based on categorization of the findings in the uterine cavity into three groups, determining the probability for RPOC. These categories, which are routinely used in our department, were determined based on our previous experience from analyzing US reports compared to histopathological results derived from women with suspected RPOC who underwent surgical evacuation. Accordingly, the presence of an intrauterine echogenic mass or a thick endometrium (≥10 mm) comprising detectible vascularity, were classified as high probability while the same findings without vascularity or the presence of complex fluid (fluid with avascular echogenic echoes ≥10 mm) were classified as moderate probability. Negative findings (no endometrial mass, endometrial thickness <10 mm, or complex fluid <10 mm) were classified as low probability.
The same classification was used both to stratify individual risk of RPOC as well as to advise the appropriate management (Table 1). Images documenting the different categories are presented in Fig. 1. The images were evaluated by a single expert sonographer (OL) using the above classification table.
Sonographic classification and management recommendations for patients with suspected RPOC following delivery that were routinely used in our department.
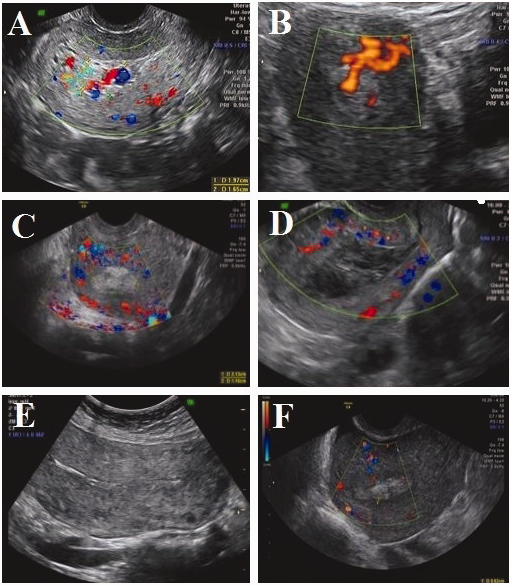
Images of the uterine cavity in patients with suspected RPOC following delivery. (a, b) High probability: an echogenic mass with vascularity. (c, d) Moderate probability: (c) an echogenic mass without vascularity; (d) complex fluid >10 mm. (e, f) low probability: no echogenic mass, endometrial thickness < 10 mm.
As part of our routine work procedures, sonographic findings were reported to the patients and the surgical team. The diagnosis of RPOC was confirmed following endoscopic surgery with positive histopathological results.
The study was approved by the Institutional review board. Information including demographics, obstetrical history, recent delivery, operative procedures, and pathology reports when available, were obtained. In cases where no operative intervention was performed in our unit, a telephone interview with the patient was conducted after a period of 6–12 months. The purpose was to investigate the ambulatory follow-up and whether any surgical intervention had been performed elsewhere. If surgical intervention was reported, histopathological results were obtained.
Statistical analysis was conducted in the statistical laboratory at the University using SPSS Statistics version 24 software (Chicago, IL, USA). Continuous variables are presented as the mean ± standard deviation or as median (range). Frequencies are presented as percentages. Means and medians were compared with the student’s t-test. The PPV and negative predictive value of the various criteria in predicting RPOC was examined. A two-tailed Fisher’s exact test or Pearson’s chi-square test were used to determine the association of various sonographic criteria with the presence of RPOC.
A P value < 0.05 was considered statistically significant.
Results
Our study included 66 patients. The mean maternal age was 31 years (range = 20–43 years). Vaginal delivery and cesarean delivery were recorded in 59 (89%) and 7 (11%) patients, respectively. US scan was performed at a mean of 33 days postpartum (range = 1–135 days). Twenty-nine patients (44%) were asymptomatic and 37 (56%) had symptoms presenting as vaginal bleeding (70%), abdominal pain (16%), or fever (14%).
Based on US examination 26 (39.4%), 28 (42.4%), and 12 (18.2%) patients were classified as high, moderate, and low probability for RPOC, respectively (Fig. 2). Upon grouping the women according to this sonographic scoring system, a statistically significant difference in the prevalence of RPOC was observed, with rates of 62% in the high, 32% in the moderate, and 0% in the low probability categories (Fig. 2).
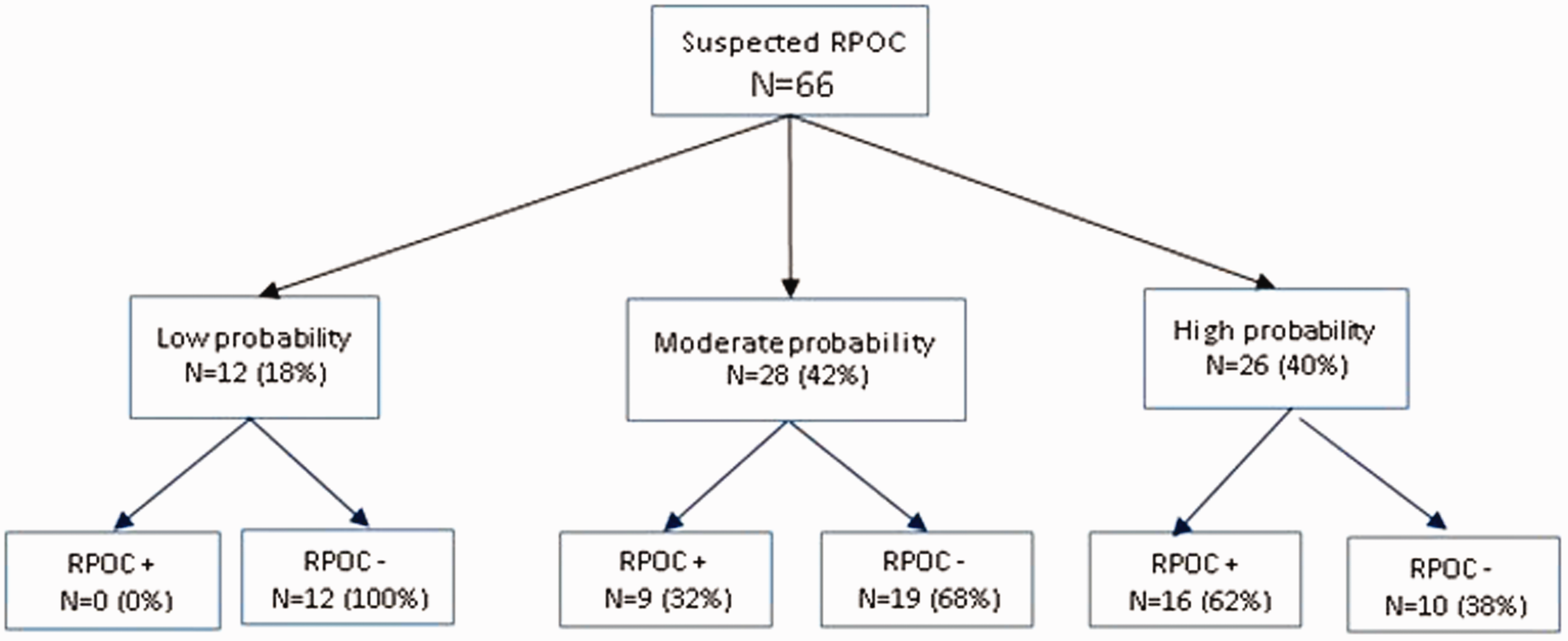
Flow chart summarizing the detection rate of RPOC in low, moderate, and high probability groups. P < 0.0001, Pearson’s Chi-square test.
Additionally, each group was further subdivided based on the timing of the US examination: <42 days postpartum (during puerperium) or ≥ 42 days. In the high probability group, confirmation of RPOC increased from 56% to 75% when the sonogram was conducted ≥ 42 days postpartum as compared to exam conducted <42 days postpartum. The increase was more prominent in the moderate probability group: from 12% to 64% (Table 2). In the low probability group, there was no case of RPOC regardless of the time range of the US assessment.
RPOC prevalence in the different subgroups according to time interval from labor to US examination.
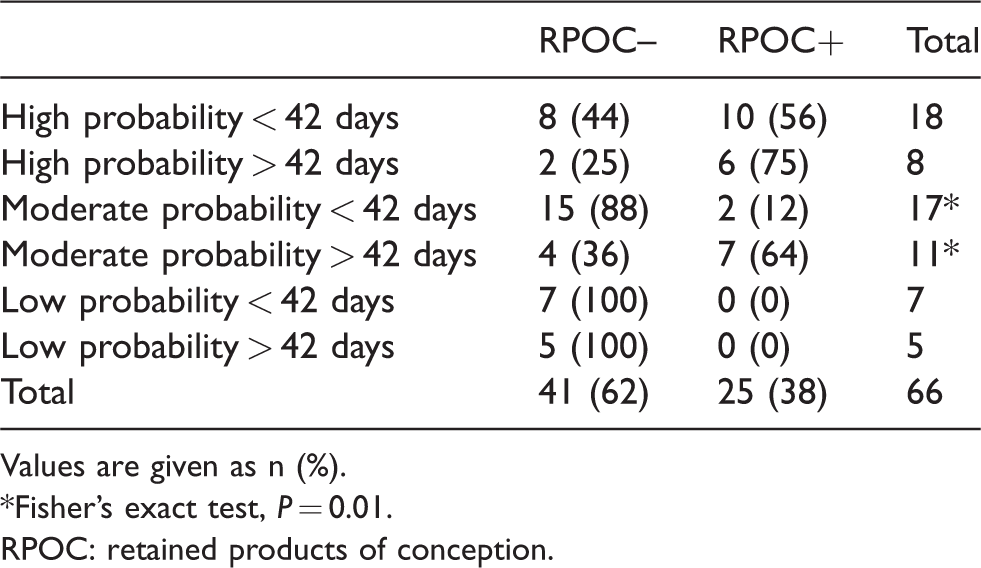
Values are given as n (%).
*Fisher’s exact test, P = 0.01.RPOC: retained products of conception.
Surgical procedure for uterine evacuation was conducted in 40/66 study patients (60%), including three patients in the low probability group, 14 in the moderate probability group, and 23 in the high probability group. In total, 25 patients (38%) had histopathological confirmation of RPOC, 16 from the high-risk group and nine from the moderate-risk group. No case of RPOC was recorded in the low-risk group.
Discussion
Accurate sonographic diagnosis of RPOC is challenging due to non-specific findings and variable appearance. The presence of blood clots, necrotic decidua, and placental tissue leads to overlap findings in patients with and without RPOC (4). Various studies have shown that the false-positive diagnosis of retained products on sonography is high, in the range of 17%–51% of the cases (4,9–11).
Our study shows that in the low probability group, in which US findings are negative, the negative predictive value for RPOC was 100%. Although some of the patients in the low-risk group were referred for endoscopic surgery due to clinical considerations (prolonged vaginal bleeding), pathology was negative for RPOC in all. The absence of US findings suggestive of retained products accurately excluded RPOC. Our results are in agreement with Durfee et al. (5) who found no RPOC in 64 patients with normal findings according to similar criteria. The low probability group is relatively small in our study (12 cases) because our cohort included women who were referred to our unit for further US evaluation after RPOC was suspected. It is assumed that most women who belong to the low probability subgroup had an ambulatory US, with no suspicious findings for RPOC, and were therefore not referred for further evaluation.
The timing of the examination is crucial since normal US appearance of the uterine cavity changes during puerperium. US finding indicating contents in the uterine cavity is most common at 7–14 days upon delivery and it diminishes gradually until the end of puerperium (12). As Edwards et al. showed in women with uncomplicated postpartum recovery, 51% had an echogenic mass within the uterine cavity at seven days postpartum, decreasing to 6% at day 21 (13). Postponing the US evaluation to the end of the puerperal period is worthwhile since the presence of fluid, debris, or blood clots appearing as echogenic masses in the uterine cavity disappear by that time (12,13).
The moderate probability group, which includes avascular content in the uterine cavity, is the most prone to false-positive results and its consequence, due to the overlap of sonographic findings between avascular RPOC and blood clots. The overall PPV in this group was 32%. Our study suggests that US performed ≥ 42 days postpartum increases the PPV dramatically in the moderate probability subgroup from 12% when performed <42 days, to 64%. There are few data regarding the optimal time frame of surgical intervention in cases of RPOC. A recent study from our center (14) demonstrated no difference between early or late surgical intervention in the reproductive outcome in women with pathologically confirmed RPOC. Therefore, our current recommendation is that conservative follow-up of suspected cases in the moderate probability group should be maintained until the end of the puerperium. This approach seems to be both effective in avoiding unnecessary surgical interventions, as well as safe regarding future reproductive outcomes. However, it is only possible when the clinical condition enables expectant management as in asymptomatic or mildly bleeding patient.
In the high probability group (which includes sonographic findings in the uterine cavity with vascularity), the overall PPV was 62%; although increase in PPV was observed after 42 days, it did not reach any statistical significance.
The data of the current study are in accordance with previous studies demonstrating that the presence of blood flow on color Doppler imaging improves sonographic prediction of RPOC (7,8,15). An interesting question is the possible explanation for the non-RPOC cases in the high probability group. One explanation could be the possible spontaneous expulsion of the retained products during the time interval between the US scan and the surgical procedure or the follow-up examination. Another explanation could be the sub-involution of the placental site. Namely, if a blood clot is adjacent to the involution site, color Doppler flow might erroneously appear to be within the endometrium. Therefore, when utilizing Doppler sonography, it is important to distinguish Doppler signals arising from tissue within the endometrial cavity from those signals which occur within the adjacent myometrium and may represent the implantation site.
A previous study from our center (16) proposed a new approach for the early diagnosis of RPOC. A routine US evaluation was performed on the second or third postpartum day. This initial postpartum scan was found to be abnormal in 271 women, while 230 (85%) of them had a normal scan on US follow-up 2–4 weeks later. Hence, US evaluation for RPOC is not advisable for routine screening in the first postpartum days. In the present study, the mean time of the US scan from delivery was 33 days, a fact which probably prevented many unnecessary tests. The current study confirmed that imaging of the postpartum uterus in order to detect RPOC has improved accuracy when performed at the end of puerperium. In addition, this approach is also practical and easily implemented, since routine follow-up after delivery is usually recommended at this session. Certainly, if symptoms such as vaginal bleeding, abdominal pain, or fever occur during this time, US should be conducted based on clinical indications.
This study has a few limitations, which need to be addressed. The first is its retrospective nature. However, all scans were performed using a strict uniform method which combined gray-scale and Doppler imaging and were reviewed by a single physician. A second limitation is that not all patients underwent surgical procedure; therefore, there were patients we regard as RPOC-negative, but lack pathological confirmation. However, this shortcoming is comparable to most published studies dealing with this issue. It is conceivable that some of these patients had RPOC. However, if retained products were indeed present, they were not clinically important and were spontaneously expelled without involving any complication. A third limitation is the small number of our cohort. Still, there were no losses on follow-up and all our patients were monitored until the end of this study.
In conclusion, this study presents a sonographic classification combined with a working protocol for the diagnosis and management of patients with suspected RPOC after delivery. In the low probability group with normal sonographic findings, no surgical intervention is recommended. In the high probability group, surgical evacuation of the uterine content is indicated and our recommendation for operative hysteroscopy remains. When sonographic findings are within the moderate probability category, and the patient is clinically stable, expectant management with follow-up scan at the end of the puerperal period (42 days) is recommended. This approach may increase the PPV of the US examination and avoid unnecessary interventions. Larger prospective studies are required to confirm our results.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.