
Abstract
Background
Measurement of iodine concentration from dual-energy or spectral computed tomography (CT) provides useful diagnostic information especially in patients suffering from malignant tumors of various origins.
Purpose
The purpose of this study was to systematically investigate the accuracy of the measurement of iodine concentration, focusing on potential influencing factors and assessing its suitability for routine clinical use.
Material and Methods
First, a 3D-printed cylindrical phantom was used to assess reliability of dual-energy CT-based iodine concentration measurement. Second, a semi-anthropomorphic phantom was used to evaluate the potential impact of positional variation of the target volume as typically seen in clinical scans. Finally, a reference vial was placed on the body surface of 38 patients undergoing abdominal dual-energy CT to analyze correlations between applied doses and patient diameters.
Results
The position of the target volume within the cylindrical phantom and the applied dose level significantly influenced the magnitude of measured iodine concentrations (P < 0.001). We also found a significant difference in accuracy depending on target volume position in the semi-anthropomorphic phantom (P = 0.028). In patient scans, we observed an error of 19.6 ± 5.6% in iodine concentration measurements of a reference and significant, moderate to strong, negative correlations between measured iodine concentration, maximum patient diameter, and applied dose (maximum sagittal diameter: r = −0.455, P = 0.004; maximum coronal diameter: r=−0.517, P = 0.001; CTDIvol: r = −0.385, P = 0.017)
Conclusion
Dual-energy CT-based iodine concentration measurement should be interpreted with caution. In clinical examinations, placement of a reference vial could be a potential solution to relativize errors.
Introduction
In single-kilovoltage-peak (kVp) computed tomography (CT) examinations, tissue attenuation at the average energy of photons emitted by the X-ray tube is measured using the Hounsfield unit (HU) scale (1). The HU values measured in these scans vary with the chemical composition and density of biological tissues. Tissues or materials of different chemical composition therefore may appear the same on single-kVp images because they have the same underlying HU number. If more than one tissue/material is present in a given image pixel, the resulting HU value represents the total attenuation resulting from different materials in the beam path within the pixel. For this reason, no separate quantitative measurements can be derived for different overlaying materials in single-kVp scans (1).
In dual-energy CT (DECT), two datasets of the same region are acquired at two different kilovoltage peaks with two photon energy spectra. Different options to accomplish DECT have been developed by manufacturers (2). In our study, we used fast kVp-switching. When two different datasets (or up to 11 datasets in spectral CT) are acquired, it is possible to differentiate known components of chemical compounds based on their attenuation spectra. These datasets can be used to reconstruct component maps and make quantitative concentration measurements. The accuracy of such concentration measurements can theoretically be affected by several factors (1,3,4).
For various clinical indications, CT examinations are performed with an iodine-containing contrast agent (CA). In oncologic patients, CA distribution or enhancement can help identify and follow up malignant lesions through focal enhancement with higher HU values on contrast-enhanced CT scans. This information also allows estimation of the vital activity of malignant tissue (5–9). However, correct interpretation can be challenging because it is not possible to differentiate the origin of increased HU values in single-kVp CT scans. These limitations can be overcome by DECT with generation of iodine maps and measurement of iodine concentration (IC). DECT has been reported to improve detection and characterization of malignant tumors of various origins; moreover, it may have predictive value in these patients and can be used to monitor the response to oncologic treatments (5–7,9–12). Before IC measurement can be used to derive diagnostic information in deciding about patient management in clinical routine, factors affecting IC measurement and potential errors should be known. First studies investigating the accuracy of IC measurement report differences between vendors and scanner models as well as significant errors (4,13).
The purpose of this study was to systematically investigate the accuracy of IC measurement in DECT, focusing on potential influencing factors, such as positioning/location of the target volume within the field of view (FOV), other structures within the FOV, applied dose, and assessing its suitability for routine clinical use.
Material and Methods
A stepwise study design was chosen to systematically evaluate the reliability of IC measurement. In a first step, we investigated the effects of different concentrations, applied dose, and slight positional variation in a simple phantom. In the second step, we used a semi-anthropomorphic phantom to further investigate reliability introducing larger variations in position within the FOV and taking effects of other structures within the FOV into account. In the third step, IC measurement errors were recorded in patients undergoing routine clinical CT scans. Here we analyzed patients’ body diameters as potential influencing factors. Furthermore, placement of a reference vial was evaluated as a possible simple solution to enable standardization of IC values in clinical routine. Measurements of absolute IC values are given in 100 μg/cm3 as vendor’s standard. Deviations and errors are expressed as percentages of the reference concentrations.
Phantom measurements: cylindrical 3D print
First, we evaluated the reliability of IC measurements over several scans at two different ICs (124 [100 μg/cm3] and 336 [100 μg/cm3]); the unit of 100 μg/cm3 was chosen due to default vendor setting for better comparability to other studies. The two ICs were derived from our experiences with anthropomorphic 3D-printed phantoms. To analyze errors related to dose, we set the applied dose to the available minimum and maximum (6.36/23.5 mGy) and investigated small position variations within the phantom/FOV (see below).
We used a 3D-printed phantom which was produced using a technique described by Jahnke et al. (14,15). The dimensions of the printed phantom were equal to a commercially available, well-established phantom (Multi-Energy CT Phantom®, Gammex Inc, Middleton, WI, USA). Printed, solid cylinders with two different concentrations of potassium iodide were used for measurement. After CT measurement, exact iodine concentrations of the cylinders were verified by dissolving the cylinder material and analyzing iodine content of the resulting solution by means of a redox titration. The position of the cylinders within the phantom was varied between the center and the outer ring (Fig. 1; for exact dimensions/distances see commercial phantom).
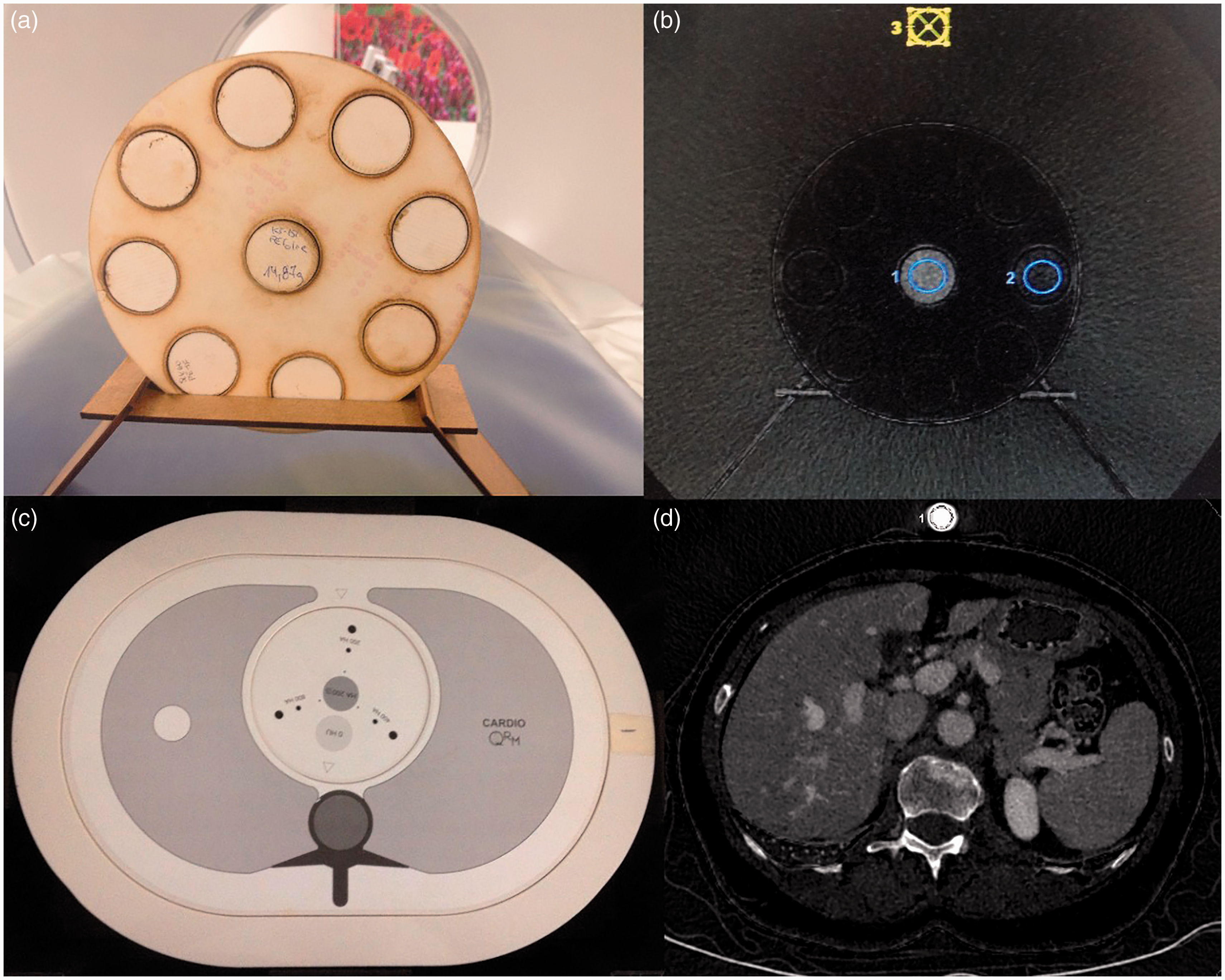
Experimental set-up. (a) 3D-printed phantom with the same dimensions as a well-established, commercially available phantom. Printed, solid cylinders with two different concentrations of potassium iodine were used for measuring ICs (b), which were subsequently verified. The position of the cylinders within the phantom varied between the center and the outer ring. In the second step, CT scans were acquired with liquid dilutions of a commercially available contrast agent and sodium chloride in plastic vials utilizing a semi-anthropomorphic phantom (Cardio CT Phantom®). This phantom simulates the thorax of a medium-sized patient containing artificial lungs, spine and soft tissue material with respect to density and attenuation characteristics (c). The vial was placed anterior to and lateral to the phantom. In the third step, the liquid dilution of contrast agent (Ultravist 370®) and sodium chloride (1:10) in a plastic vial was placed on the body of 38 patients who underwent abdominal DECT scans (d). Blue circles: positions of ROIs for IC measurement.
Phantom measurements: Cardio CT Phantom®
Second, we evaluated the influence of larger position variations and the effect of other structures within the FOV on IC measurement.
For this purpose, DECT scans were performed with a liquid dilution of a commercially available contrast agent (Ultravist 370®, Bayer Vital GmbH, Leverkusen, Germany) and sodium chloride (1:10) in a plastic vial using a semi-anthropomorphic phantom (Cardio CT Phantom®, QRM, Forchheim, Germany). This phantom simulates the thorax of a medium-sized patient containing artificial lungs, spine, and soft-tissue material with respect to density and attenuation characteristics (Fig. 1). For the dilution, we deliberately chose a concentration that does not occur within the body in clinical routine. The reason for this is the known increase in measurement errors in low iodine concentrations, which should not affect this measurement (3). The vial was placed anterior to and lateral to the phantom.
Patient measurements
Third, we evaluated possible IC measurement errors in a clinical setting focusing on the effect of different body diameters in order to quantify methodological deviations in IC that must be taken into account in the routine application of the technique. Furthermore, we evaluated the placement of an IC reference as a simple solution for standardizing IC measurement in the routine clinical setting.
For this purpose, we used the above-described liquid dilution of contrast agent (Ultravist 370) and sodium chloride (1:10) in a vial, which was placed in a standardized anterior, median position on the body of 38 oncologic patients who underwent abdominal DECT scans for lesion detection/characterization or therapy monitoring. Therefore, written informed consent was waived.
CT technique
Examinations were performed on a 64-multislice CT scanner (Revolution HD®, GE Healthcare Milwaukee, WI, USA) following acquisition of a posterior-anterior scout. Phantom scans were repeated 10 times to minimize random measurement errors. As our study was performed on a GE scanner, we used GE’s dual-energy-based spectral mode, known as Gemstone® spectral imaging (GSI). Except for applied dose levels in cylindric phantom measurements, which were set either to minimum (6.36 mGy) or maximum (23.5 mGy), all further parameters (noise index, pitch, collimation, rotation time, slice thickness, iterative reconstruction level) were kept constant across all scans; images were reconstructed using a soft-tissue kernel (Table 1).
Scan parameters.
Except for applied dose levels in cylindrical phantom measurements, CT acquisition parameters were kept constant across all scans, and images were reconstructed using a soft-tissue kernel.
ASIR, adaptive statistical iterative reconstruction; DFOV, display field of view; SFOV, scan field of view.
Quantitative image analysis
All analyses were performed using a commercially available server/client solution (Advantage Workstation® Server, GE Healthcare Milwaukee, WI, USA). Iodine map datasets of the DECT scans were calculated using GE’s GSI Volume Viewer® application at 0.625-mm slice thickness. In one slice, circular regions of interest (ROIs) were manually placed in the printed iodine cylinders and the plastic vials with the contrast agent dilution. In patient scans, maximum patient diameters in sagittal and coronal orientation were recorded by manual measurement.
Radiation dose
The volume computed tomography dose index (CTDIvol) as defined by the U.S. Department of Health and Human Services is a standard parameter for determining CT radiation dose based on phantom measurements. It is independent of both sample size and scan length; therefore, it was used in this study and taken from the dose report of each scan.
Statistical analysis
All statistical analyses were performed with commercially available software (SPSS 24.0®, IBM, Armonk, NY, USA). Values of P ≤ 0.05 were considered statistically significant. Graphics were created with GraphPad Prism v.5® (GraphPad Software, San Diego, CA, USA). Normal distribution of data was analyzed with the Kolmogorov–Smirnov (KS) test. Two-way ANOVA was used to analyze the data from the measurements in the cylindrical phantom and a two-tailed t-test was used for the results obtained in the Cardio CT Phantom®. The patient data were tested by determining Pearson correlations between measured ICs, applied doses, and body diameters.
Results
Phantom measurements: cylindrical 3D print
In the cylindrical phantom scanned with the minimum dose setting of 6.36 mGy, we measured mean ICs of –2.9 ± 1.1 [100 μg/cm3] (central position) and –0.7 ± 1 [100 μg/cm3] (peripheral position) in the cylinder containing a proven concentration of 124 [100 μg/cm3]. When this cylinder was scanned with the maximum dose setting of 23.5 mGy, we measured means of 0.7 ± 1 [100 μg/cm3] (central position) and –0.8 ± 0.6 [100 μg/cm3] (peripheral position). For the cylinder with the higher iodine concentration of 336 [100 μg/cm3], we measured means of 18.9 ± 1.8 [100 μg/cm3] (central position) and 22.5 ± 0.5 [100 μg/cm3] (peripheral position) with the minimum dose setting (6.36 mGy) and 22.2 ± 1.3 [100 μg/cm3] (central position) and 21.8 ± 0.8 [100 μg/cm3] (periphery position) with the maximum dose setting (23.5 mGy) (Fig. 2). These results prove that IC measurements are reliable. Furthermore, small variations in positioning the cylinder/target volume within the phantom/FOV and the used dose level significantly influenced the measured ICs (P < 0.001) (Fig. 2).
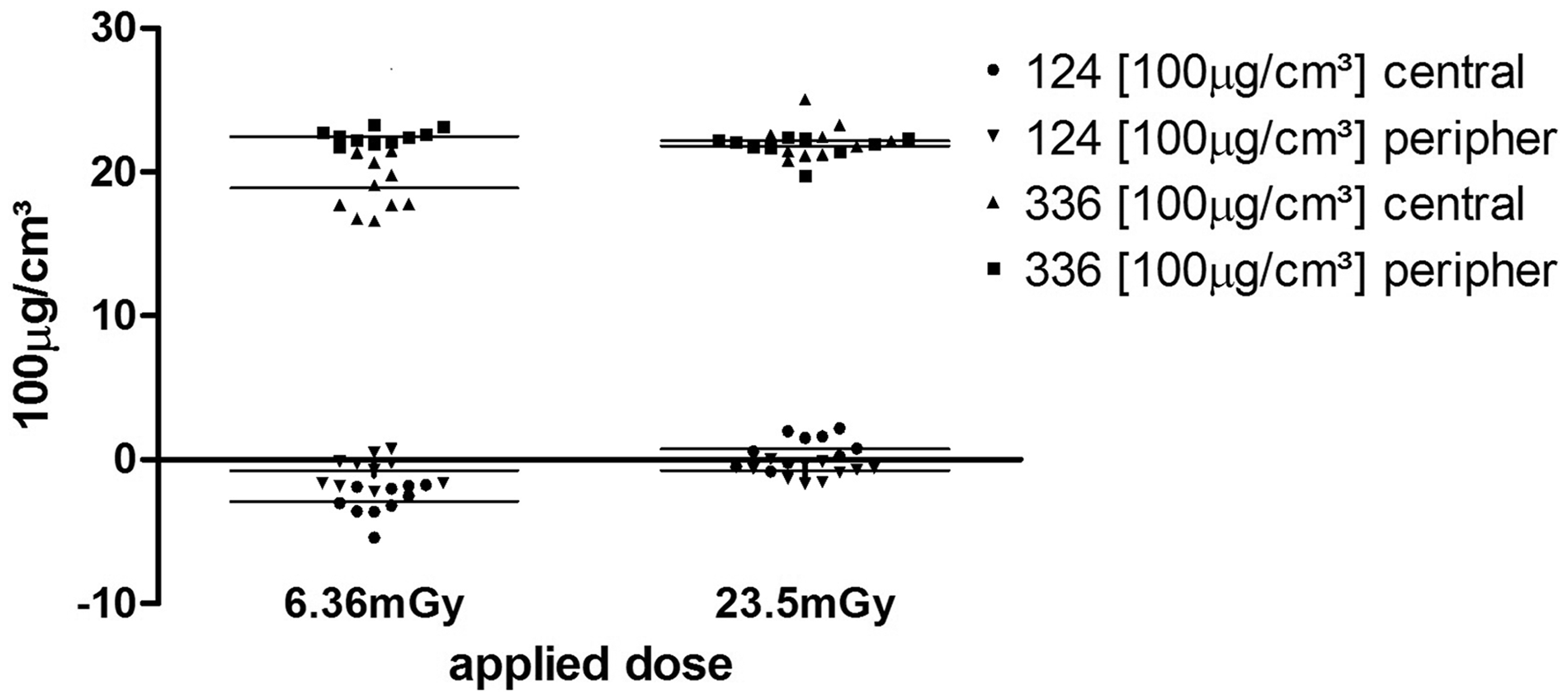
ICS in cylindrical phantom. Absolute errors in terms of deviations between measured and actual ICs were relatively large in our experiments while deviations between serial measurements were small. Our results confirm that cylinder positioning within the phantom and applied dose levels significantly influence measured ICs (p < 0.001). The carrier material of the phantom has negative HU values, which probably explains the negative IC values measured in our study.
Phantom measurements: Cardio CT Phantom®
In the experiments using the semi-anthropomorphic phantom, different vial positions did not significantly affect absolute mean ICs, which were 282.3 ± 1.3 [100 μg/cm3] (anterior position) and 279.7 ± 2.9 [100 μg/cm3] (lateral position). However, the relative IC measurement error compared to the reference concentration was significantly influenced by the vial position (anterior position: 23.7 ± 0.1%; lateral position: 24.4 ± 0.2%; P = 0.028) (Fig. 3). These results again corroborate the reliability of IC measurement and reveal an influence of positioning on IC measurement errors, which may be larger when other structures are present within the FOV.
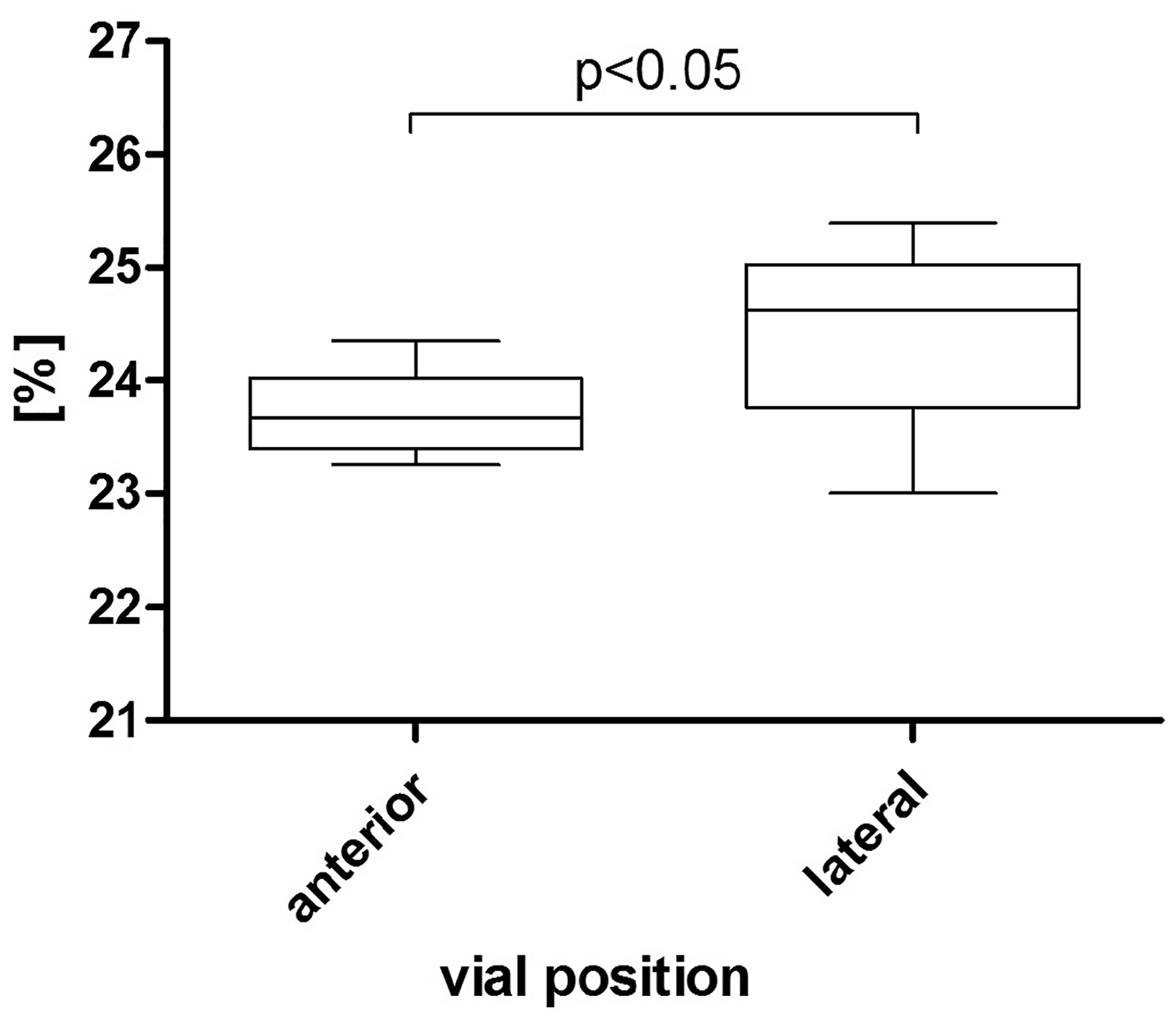
IC deviation from reference in semi-anthropomorphic phantom. Our results in this experiment show that positioning of the vial influences the relative measurement error. The results also show that repeated measurements are robust if the target volume remains in the same region of the FOV and that position-dependent accuracy differences are small.
Patient measurements
The mean measured iodine concentration of the reference vial (370 [100 μg/cm3]) in patient scans was 297.4 ± 13.5 [100 μg/cm3] for a mean applied dose of 10.26 ± 4.1 mGy. This corresponds to a 19.6 ± 5.6% deviation from the reference in patient scans. Patients’ maximum body diameters in sagittal (262.9 ± 46.9 mm) and coronal (362.8 ± 54.4 mm) orientations matched with previous observations in oncologic patients in our department. We also observed significant, moderate to strong, negative correlations between measured iodine concentrations, maximum diameters, and applied doses (maximum sagittal diameter: r = –0.455, P = 0.004; maximum coronal diameter: r = –0.517, P = 0.001; CTDIvol: r = –0.385, P = 0.017) (Fig. 4).
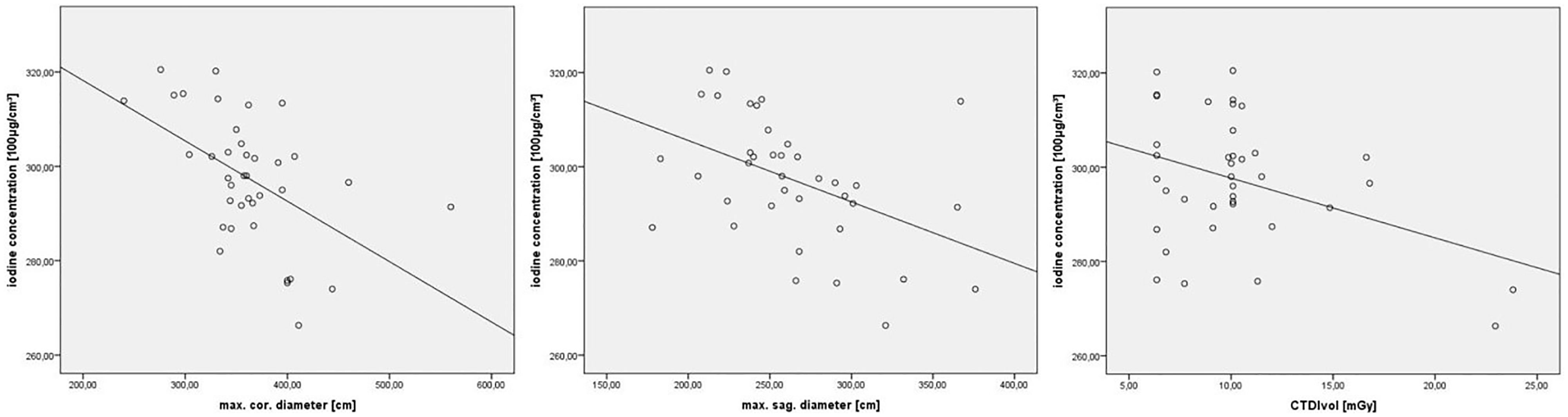
Correlations between measured iodine concentrations, patients’ body diameters, and applied doses. We observed significant, moderate to strong, negative correlations between measured ICs, maximum body diameters, and applied doses. Maximum body diameters in sagittal and coronal orientations are consistent with previous observations in oncologic patients examined at our department.
Discussion
Contrast-enhanced CT is widely available and relatively inexpensive, making it one of the most widely used medical imaging modalities, especially in oncologic patients. Additional diagnostic information is provided by DECT, which is increasingly being used with the advent of dose optimization techniques. While every improvement in terms of diagnostic value is of great importance due to the broad application of CT, a novel technique should also be viewed critically. DECT-based IC measurement has already been used in cancer patients for lesion differentiation or grading (8,9,12). But there are also initial reports describing intrinsic relevant measurement errors, depending on vendor and CT scanner model (4,13). This is an important concern that radiologists must be aware of. Furthermore, it is important to know other factors potentially affecting IC measurement in order to find a way for dealing with them and standardizing IC measurement before the information can be used in routine clinical decision making.
The purpose of this study therefore was to assess the accuracy of IC measurement focusing on potentially clinically relevant influencing factors and its feasibility in clinical routine.
We used a stepwise design to separately evaluate these different aspects. In the first step, IC measurement reliability was determined for different concentrations and possible effects of the applied radiation dose and slight positional variation inside the CT scanner.
In terms of reliability, our results reveal relatively large absolute errors between measured and actual ICs. Nevertheless, deviations in serial measurements were small, indicating that the measurements themselves are degraded by relatively small errors. Therefore, absolute deviations of the concentrations are presumably attributable to the analysis algorithms, which are probably not optimized for measurement in small phantoms.
Slight positional variation within the FOV and use of different doses significantly influenced measured ICs in our experiments (P < 0.001) (Fig. 2). This is consistent with a study reporting a decrease in measurement errors at higher dose (1). In that study a standard phantom covered with other materials and liquid samples were used (1). Such a phantom can lead to inaccuracies, since artifacts can occur at interfaces between materials of different attenuation, e.g. in covering, and the homogeneity of liquid solutions cannot be guaranteed over a longer measuring period. To avoid these problems, we used a completely homogeneous and solid phantom; however, this comes with the disadvantage that the carrier material of the phantom has negative HU values, which probably caused some negative IC values in our experiments.
Our second step aimed at determining potential effects of larger position variations within the FOV as well as any influence of other structures present in the FOV in a semi-anthropomorphic phantom. Furthermore, the target volume was changed to liquid dilutions of a commercially available contrast agent to more closely simulate routine patient examinations. The results show that repeated measurements are robust if a constant position of the target volume within the FOV is maintained. In addition, our results indicate that position-dependent variation is small.
Nevertheless, positioning does have an influence on the absolute measurement error. Since absolute IC values are used as diagnostic markers, these differences are relevant when interpreting findings in patients with different indications for CT such as lesion detection/characterization, differentiation, tumor grading, and therapy monitoring (8–11,16–21). Therefore, to avoid this error, a standardized, anterior, median position of the vial was chosen for the following measurements in the patient cohort.
In the third step, we investigated routine patient examinations to analyze potential errors and influencing factors focusing on patients’ body diameters. In addition, we placed a reference vial, which might provide a simple solution for standardization of IC measurement in patients.
We observed a 19.6 ± 5.6% error of IC measurements of the reference vial in patient scans, where patients’ maximum diameters matched with previous observations in oncologic patients examined at our department. We also observed significant, moderate to strong, negative correlations between measured IC, maximum diameters, and applied doses. The increasing underestimation of ICs with increasing body diameters is consistent with published phantom results (1). However, we also observed a correlation between the applied dose and underestimation of IC in clinical routine, which did not agree with our phantom results and reported data, e.g. by Papadakis et al. (1).
Overall, these findings confirm that IC measurement is subject to significant errors in routine clinical CT examinations, which has to be kept in mind when interpreting ICs for clinical decision-making. With a magnitude of 19.6%, absolute errors in our patient scans are in the range to be expected from phantom measurements. This magnitude may be lowered when a third-generation CT scanner is used (4,13).
A limitation of our study is that all experiments were performed on the same CT scanner because our center has no newer-generation CT system with dual-energy capability. Furthermore, we did not analyze potential effects of other factors such as the reconstruction algorithm used, as described by Euler et al. and others; however, since we kept these parameters constant across all measurements, no relevant error should have occurred (3). Phantoms were used for assessing dose- and position-dependent effects on measured ICs, since reliable, dose-dependent serial measurements are not feasible in a patient population, and position-dependent measurements (e.g. with several vials) were considered to be too complex, time-consuming, and unreliable for clinical routine. Finally, the patient cohort (n = 38) is relatively small and the results should be verified in a larger group.
In conclusion, our results confirm that DECT-based quantitative IC measurement is affected by scanner-dependent technical parameters such as the applied dose, procedural variables such as the positioning of the target volume in the FOV, and patient-related factors such as body dimensions. The observed errors of approximately 20% in the clinical setting probably rule out the use of IC measurement for characterizing and grading malignant tumors or monitoring treatment responses in these patients. However, our results can be used to consider the deviations in interpreting ICs for clinical decision-making. For patient examinations, we furthermore recommend the use of a reference body (e.g. vial with known contrast agent dilution) placed in a standardized position. This would be a straightforward, widely available, and cost-effective way of accounting for differences in IC measurements and making them more comparable.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.