
Abstract
Background
Magnetic resonance imaging (MRI) with hepatocyte specific contrast has the highest sensitivity for colorectal liver metastases but comes at high costs and long examination times.
Purpose
To evaluate if preoperative detection of colorectal liver metastases with less resource-consuming diffusion-weighted imaging (DWI) alone or in combination with multidetector computed tomography (MDCT) can compete with gadolinium-etoxybenzyl-diethylenetriaminepentaacetic acid (Gd-EOB-DTPA)-enhanced MRI.
Material and Methods
Forty-four patients with 123 colorectal liver metastases received MDCT and Gd-EOB-DTPA-enhanced MRI including DWI before liver resection for colorectal liver metastases. Five image sets were evaluated by two radiologists. The DWI set consisted of DWI, ADC map, coronal, axial T2-weighted single-shot sequences. The DWI-T2F set contained additionally respiratory-triggered T2-weighted TSE-SPIR sequences. The MDCT set consisted of four-phase MDCT, the MDCT-DWI set also contained DWI. The CE-MRI set contained all MRI sequences including Gd-EOB-DTPA. Reference standards was histopathology and follow-up.
Results
CE-MRI set had highest sensitivity (P ≤ 0.013) with 95% compared to 72%, 73%, 73%, and 87% the for DWI set, DWI-T2W-FS set, MDCT set, and MDCT-DWI set, respectively. The CE-MRI set had the highest sensitivity (P≤0.012) for colorectal liver metastases <10 mm with 87% compared to 55%, 52%, 23%, and 58% for the DWI set, DWI-T2W-FS set, MDCT set, and MDCT-DWI set, respectively. The MDCT-DWI set improved sensitivity overall and in size-dependent subgroup analyses compared to the MDCT set (P ≤ 0.031). The MDCT-DWI set showed the highest specificity of 98% followed by 98%, 98%, 95%, and 88% for the DWI set, DWI-T2W-FS set, MDCT set, and CE-MRI set, respectively.
Conclusion
The less resource and time-consuming DWI sets are inferior to Gd-EOB-DTPA-enhanced MRI for the detection of colorectal liver metastases. Gd-EOB-DTPA-enhanced MRI with its excellent sensitivity should be the preferred preoperative modality when meticulous lesion identification is essential. Combination of DWI with MDCT improved significantly sensitivity compared to each modality alone.
Keywords
Introduction
Colorectal cancer (CRC) is the third most common cancer and the fourth leading cause of death with about 700,000 deaths worldwide (1). After the lymph nodes, the liver is the organ most commonly infiltrated by metastases (2). At the time of diagnosis with CRC, approximately 20–30% of patients have synchronous colorectal liver metastases (CRLM) and up to 50% will develop CRLM during the course of their disease (3).
The only potential curative treatment for patients with CRLM is surgical resection (3). Complete resection in combination with chemotherapy has resulted in a five-year survival approaching 50% (4). Whether liver resection is applicable is a multidisciplinary decision, where the identification and precise localization of all liver metastases is essentially important (3). Detection of CRLM is based on multiple imaging modalities including multidetector computed tomography (MDCT), magnetic resonance imaging (MRI), and fluorine-18 fluorodeoxyglucose (18F-FDG) positron emission tomography combined with MDCT (PET/CT) (5). Intraoperative ultrasound (IOUS) as the last imaging modality before liver resection may provide additional information (6).
MDCT is the most common imaging modality for staging and follow-up of patients with CRLM, even though several newer studies have shown that contrast-enhanced MRI (CE-MRI) is superior to MDCT for the detection and characterization of CRLM (7–9). This applies especially for small lesions < 10 mm and, ideally, MRI should be the first line modality in evaluating the liver (7,9). On the other hand, criticism has been directed towards MRI with liver-specific contrast media as a mandatory imaging modality for patients with CRLM because the cost and treatment delay outweigh any potential benefits in terms of improved sensitivity compared to MDCT (10). CE-MRI is a time-consuming and expensive technique and a more efficient and less expensive imaging procedure would be appreciated. In the light of recent findings of gadolinium deposits in brain and bone, the need of a non-gadolinium dependent imaging protocol has been even more underlined (11). Promising results about the potential of a shortened MRI protocol, based on diffusion-weighted imaging (DWI) for the identification and follow-up of CRLM, have been reported (12,13).
The aim of this study was to evaluate, in the preoperative setting, whether three different DWI approaches could match the diagnostic performance of gadolinium-etoxybenzyl-diethylenetriamine pentaacetic acid (Gd-EOB-DTPA) MRI including DWI. The three different DWI approaches were DWI with and without time-consuming additional T2-weighted (T2W) fat-saturated (FS) images and DWI in combination with multiphasic MDCT.
Material and Methods
This prospective single center study was approved by the regional ethics committee. All patients gave written consent. Data collection was done prospectively during 2011–2013.
Patients
In total, 44 patients with histologically confirmed CRC and suspected CRLM (synchronous or metachronous) referred for liver resection to our institution were consecutively included. The CRLM had to be preliminarily resectable, defined as feasible R0 or R1-resection with a sufficient liver remnant. Preliminary treatment strategy and resectability were evaluated by a multidisciplinary team (liver surgeon, oncologist, and radiologist) based on MDCT findings in portal venous phase from referral institutions. Exclusion criteria were: metachronous CRLM <6-month interval between last cycle of chemotherapy for the primary CRC; Eastern Cooperative Oncology Group performance status >2; incapability to carry out breath-hold instructions; previous liver resection; other malignancy; pregnancy; known contrast media intolerances; reduced renal function; and severe claustrophobia (Fig. 1 and Table 1).
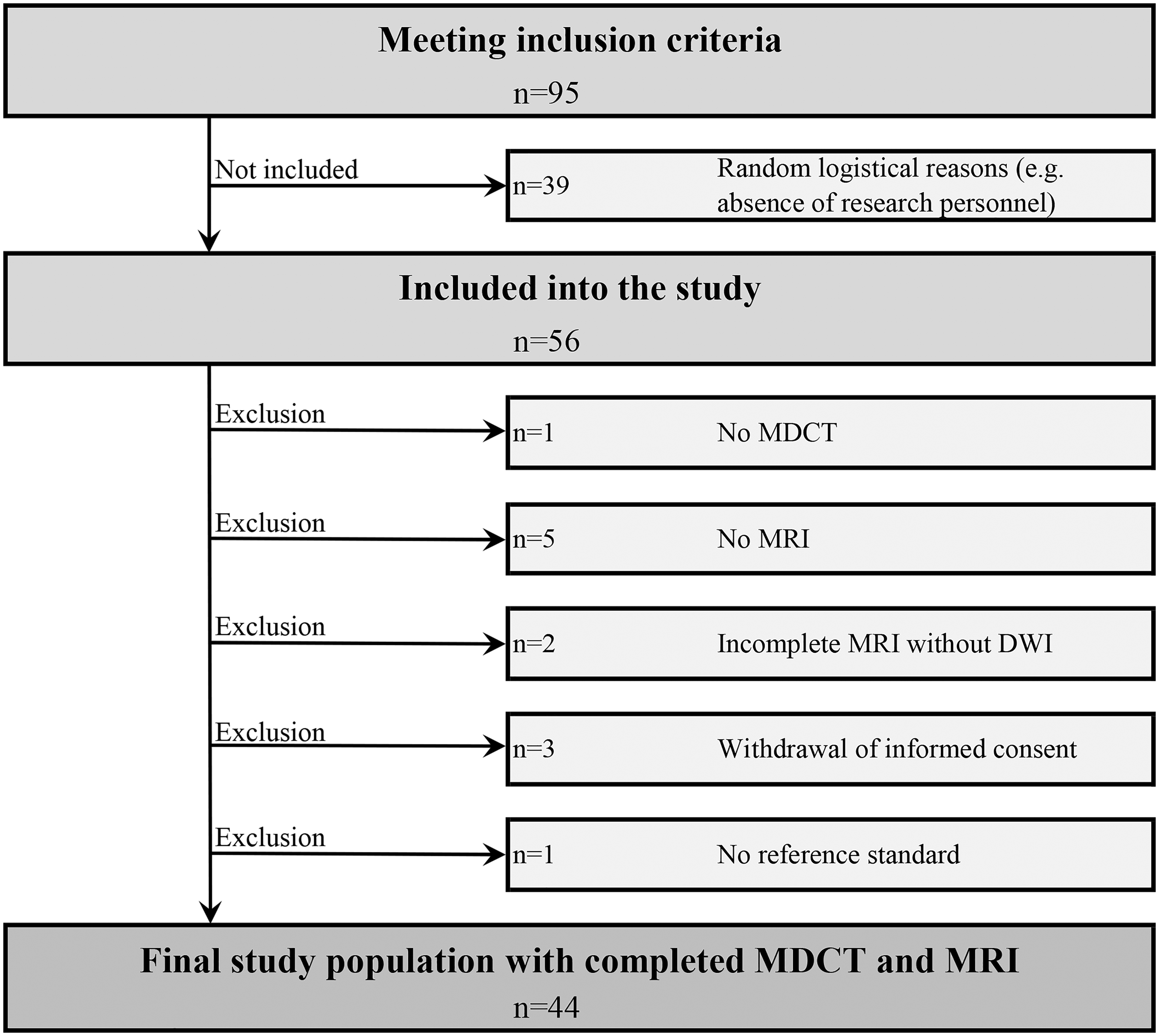
Flow chart of patient inclusion.
Patient characteristics.

Values are given as n (%) unless otherwise specified.
Staging at diagnosis of CRC according to the American Joint Committee on Cancer (AJCC) 7th edition.
Imaging protocols
All patients underwent examinations on 1.5-T MRI (Achieva, Philips) with either SENSE cardiac 32-channels coil or SENSE XL Torso 16-channels, Table 2. The patients received 1 mL Gd-EOB-DTPA (Primovist 0.25 mmol/mL, Bayer Schering Pharma AG) per 10 kg bodyweight. The contrast media was injected in a cephalic vein at an injection speed of 1 mL/s by a power injector (Spectris Solaris EP, Medrad Inc.), followed by 20 mL saline flush at 2 mL/s (bolus tracking). Axial T1-weighted (T1W) three-dimensional (3D) FFE THRIVE images were obtained before contrast and after 20–30 s, 70 s, 180 s, and 20 min in the hepatocyte phase with additional coronal images. Apparent diffusion coefficient (ADC) maps were provided, based on b-values of 50 s/mm2 and 800 s/mm2.
MRI protocol.
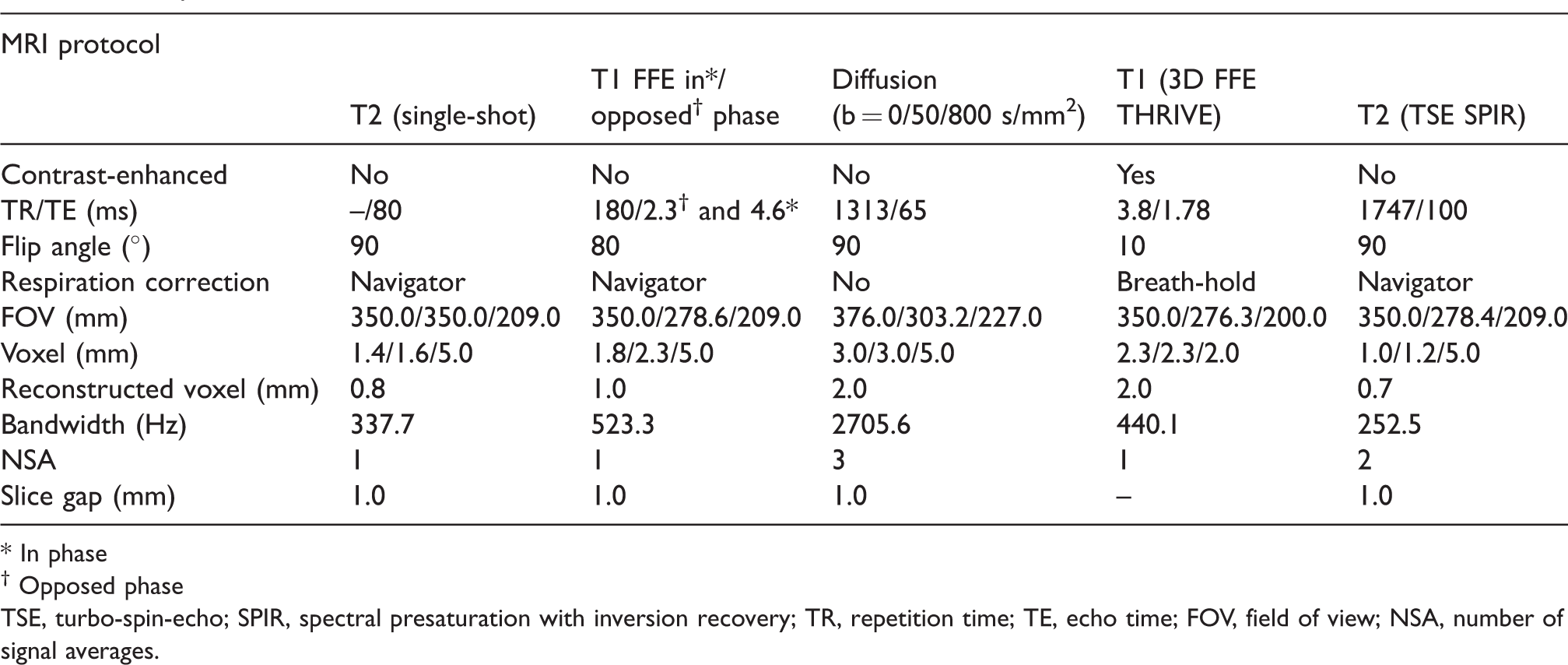
* In phase
† Opposed phase
TSE, turbo-spin-echo; SPIR, spectral presaturation with inversion recovery; TR, repetition time; TE, echo time; FOV, field of view; NSA, number of signal averages.
CT scans of the liver were performed on a Biograph mCT (Siemens AG) (Table 3). A total of 150 mL Imeron, 350 mg/mL (Bracco) were administered by a power injector (Stellant, Medrad Inc.) via a cubital vein at 5 mL/s.
MDCT protocol.
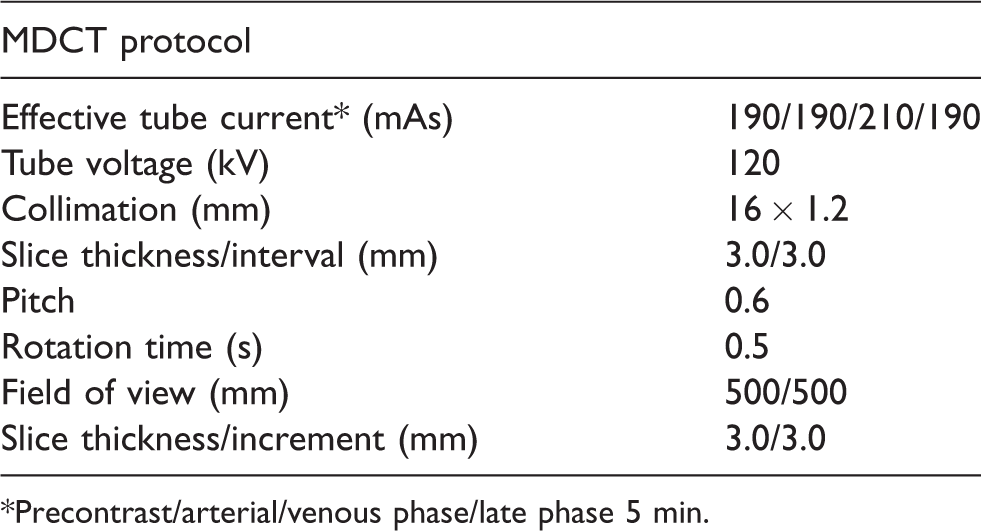
*Precontrast/arterial/venous phase/late phase 5 min.
Imaging evaluation
Five different imaging sets were provided. Image set 1 (DWI set) and 2 (DWI-T2W-FS set) consisted of both DWI, ADC map, T1W survey, coronal and axial T2W single-shot sequences (SSH). The DWI-T2W-FS set contained, in addition, a respiratory triggered T2W TSE sequence with SPIR (T2F). Imaging set 3 was MDCT only (MDCT set) and imaging set 4 combined MDCT with DWI-T2W-FS set (MDCT-DWI set). Image set 5 (CE-MRI set) contained all acquired MRI sequences, including Gd-EOB-DTPA enhanced sequences.
For the CE-MRI set, the diagnostic criteria for CRLM were defined as hypointense lesions on T1W images and moderately hyperintense lesions on T2W images. During the early dynamic phase, they showed poor enhancement centrally and increased peripheral rim enhancement and were hypointense on Gd-EOB-DTPA enhanced images in the hepatobiliary phase (HBP) (1). On DWI, CRLM were defined as hyperintense lesions at b = 50 s/mm2, which remained hyperintense at b = 800 s/mm2 and with ADC values that were less or equal to that of the adjacent liver parenchyma. Furthermore, an equivalent lesion had to be present on contrast-enhanced images (especially in the case of lesions <10 mm). Lesions identified on DWI had to be present on at least one additional image series.
On CT, hypovascular CRLM were defined as hypoattenuating lesions with less enhancement than normal liver in the portal-venous phase and with washout and/or remaining hypoattenuating on delayed phase.
The imaging sets were evaluated by B.H./K.A. (DWI set/DWI-T2W-FS set), C.J./A.S. (MDCT set), and E.V./A.S. (CE-MRI set). The MDCT-DWI set was based on the findings from the DWI-T2W-FS set and MDCT set; for deviating findings, a consensus was provided by A.S./J.B.D. For the consensus, positive findings from at least one of the imaging sets was regarded as CRLM, unless MDCT showed typical contrast enhancement for hemangiomas/CRLM or cysts were found on DWI/SSH with equivocal findings on MDCT. A.S. had >7 years of experience with CT and MRI liver imaging, the other four radiologists had >10 years. All were aware of the study aims and that the patients were under evaluation for CRLM but were blinded for all other information. To prevent recognition, the minimal time between evaluations was four weeks. The two reports for each exam were compared and the two readers agreed to a final consensus that was used for further evaluations. All images were reviewed using a local picture archiving and communication system (PACS) (Syngo Studio V36, Siemens AG, Erlangen, Germany).
Reference standard
The liver was intraoperatively inspected and during open procedures bimanually palpated. IOUS was used, if requested, by the surgeon for anatomical orientation or detection of not palpable CRLM identified on preoperative imaging.
The resected liver specimens were sent to histopathological examinations. The specimens were formalin fixated and cut into parallel slices in the axial plane, if possible. The slice thickness was 3 mm, if possible, depending on the shape of the specimen. Hematoxylin and eosin staining was performed for further examinations. Lesion type (CRLM, hemangioma, cyst, etc.), location, size, and minimal tumor-free margin to resection surface were registered. Clinical data and operation report were available to the pathologist, but report from radiological imaging was usually not given.
If no histopathological examination was available, follow-up exams were used. Lesions were classified as CRLM if the lesion increased in size or decreased in size/disappeared after receiving chemotherapy. Five-year follow-up data were available for all patients.
CRLM not identified by preoperative imaging but identified intraoperatively or by histopathological examination of the operation specimen were defined as false-negative (FN) CRLM. For size-dependent subgroup analyses, those CRLM were considered <10 mm.
Statistical analyses
The image findings were recorded manually by the readers and compared with the reference standard (RS). Statistical analyses were performed in SPSS (version 22.0.0.1; SPSS Inc., Chicago, IL, USA) and MedCalc (version 18.9, MedCalc Software, Ostend, Belgium).
The diagnostic performance was calculated based on the number of statistical units (lesions). Indeterminate lesions (no definite confirmation by RS) were excluded from the per-lesion analysis.
Kappa statistics were used to estimate inter-observer agreement for CRLM: <0.20 = poor; 0.21–0.40 = fair; 0.41–0.60 = moderate; 0.61–0.80 = substantial; and 0.81–1.00 = almost perfect.
95% confidence intervals (CI) were used for statistical interference. McNemar test was used to determine differences in sensitivity and specificity. P < 0.05 was considered to indicate a significant difference.
Results
Liver lesions
Nine (20%) of the patients had histopathologically confirmed mucinous CRLM. Four patients had benign lesions only. The preliminary suspected CRLM in these patients were characterized by imaging as hemangiomas in three patients. One patient was operated and histopathological examination reviled a sclerotic hemangioma (Table 4). None of the patients had significant liver steatosis or cirrhosis. Four patients were found inoperable.
Liver lesions.
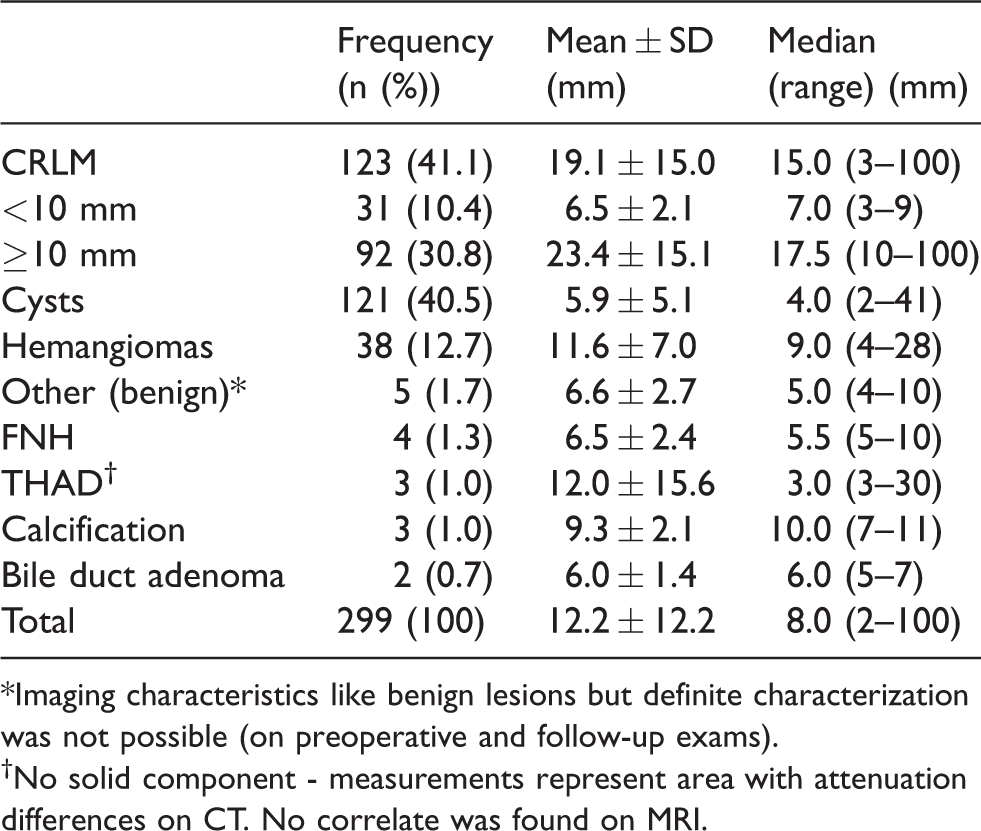
*Imaging characteristics like benign lesions but definite characterization was not possible (on preoperative and follow-up exams).
†No solid component - measurements represent area with attenuation differences on CT. No correlate was found on MRI.
Diagnostic performance
Inter-observer agreement for CRLM was high for all imaging sets with almost perfect agreement (kappa ≥0.81) for the DWI set, the DWI-T2-FS set, MDCT set, and MDCT-DWI set, and a substantial inter-observer agreement for the CE-MRI set (kappa = 0.72).
The diagnostic performance of all imaging sets is given in Table 5. The overall receiver operating characteristics (ROC) and corresponding areas under the curves (AUC) are given in Fig. 2. The AUC of the CE-MRI set and MDCT-DWI set were significantly higher than for the DWI set, the DWI-T2-FS set, and the MDCT set (P ≤ 0.014). The differences between the CE-MRI set and MDCT-DWI set did not reach significance. The CE-MRI set had the significantly highest sensitivity for CRLM overall (P ≤ 0.013) and for CRLM < 10 mm (P ≤ 0.012). No significant differences were found between the DWI set and the DWI-T2W-FS set overall or in subgroup analysis. Compared with the MDCT set, the MDCT-DWI set improved sensitivity significantly overall and in size-dependent subgroup analyses (P ≤ 0.031). Compared to the DWI set and DWI-T2W-FS set, the MDCT-DWI set improved sensitivity significantly overall, but in the size-dependent analysis this was only significant for CRLM ≥ 10 mm (P < 0.001). Only few CRLM < 10 mm were identified by the MDCT set (sensitivity = 22.6%) and sensitivity of the MDCT-DWI set was not significantly improved, remaining low (58.1%) compared to the CE-MRI set (87.1%).
Diagnostic performance.
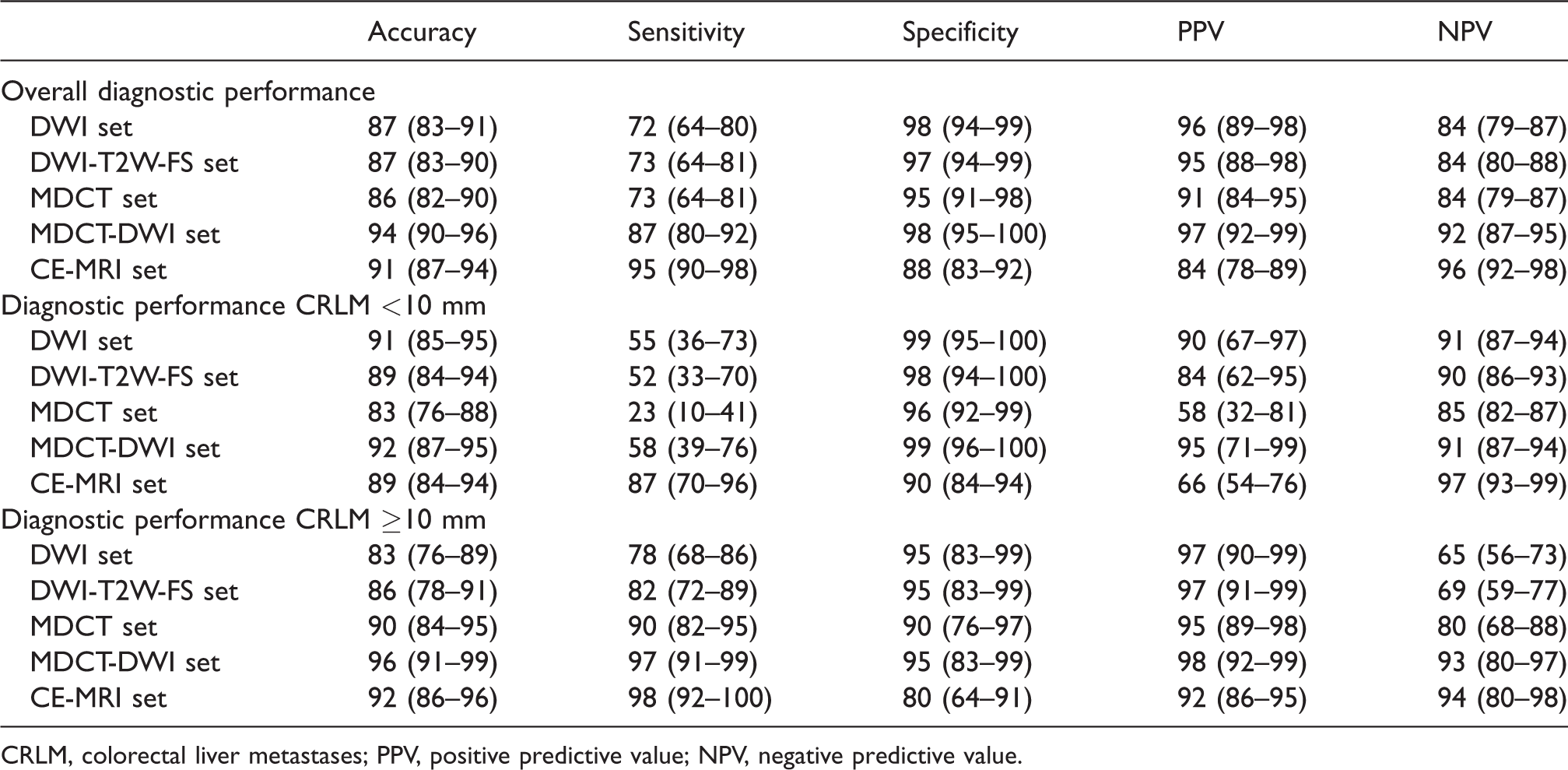
CRLM, colorectal liver metastases; PPV, positive predictive value; NPV, negative predictive value.
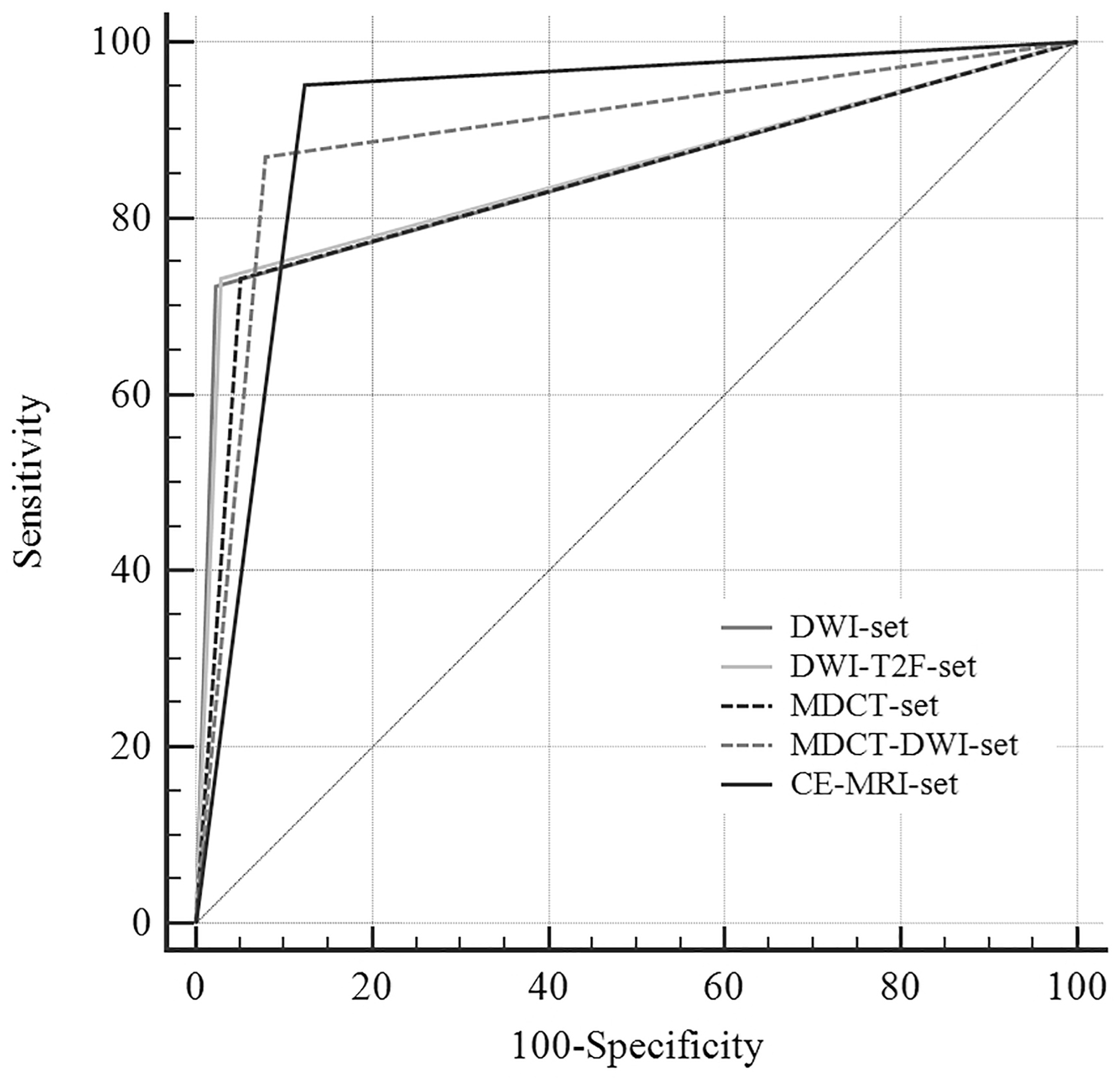
Receiver operating characteristics (ROC) for all imaging sets and overall performance with area under the ROC (AUC) curve.
Three CRLM were missed on all preoperative imaging and identified by histopathological examination of the operation specimen only. CRLM were most often misread as hemangiomas. This accounted for FN findings in 47.1% of the DWI set, in 33.3% of the DWI-T2W-FS set, in 21.2% of the MDCT set, and in 25.0% of the MDCT-DWI set. No CRLM were misread as hemangiomas by the CE-MRI set. The remaining FN findings were confounded with other benign lesions, mainly small cysts, or the CRLM were completely missed.
There were four false-positive (FP) findings for the DWI set and five for the DWI-T2W-FS set. Four benign lesions were mistaken as CRLM by both sets, with three of them occurring in one patient, representing small focal nodular hyperplasia with a size of 5, 6, and 10 mm. The fourth lesion was a hemangioma of 11 mm. One 4-mm hemangioma was misread as CRLM only by the DWI-T2W-FS set.
Nine FP findings were registered for the MDCT set, of which six were small cysts, one represented no lesion, and two were atypical hemangiomas of 19 and 20 mm. The cysts and the finding representing no lesion were correctly characterized as negative/benign after combining DWI and MDCT in the MDCT-DWI set.
The CE-MRI set registered 22 FP findings; 18 were hemangiomas, two were benign lesions (no further characterization available), one was a cyst, and one was a calcified lesion. The median size of these lesions was 7.5 mm (range = 4–18 mm). Due to the high number of FP hemangiomas, the CE-MRI set had overall the significantly lowest specificity of 87.6% (P ≤ 0.024). For lesions < 10 mm, the CE-MRI set had a significantly lower specificity than the DWI set, DWI-T2W-FS set, and MDCT-DWI set (P ≤ 0.007). By combining DWI for the identification of small cysts with MDCT with contrast for lesion characterization, the number of FP findings was reduced to three in the MDCT-DWI set and all represented atypical hemangiomas.
The MDCT-DWI set had the highest specificity. This was significant, compared to the CE-MRI set (P < 0.001). No other significant differences in specificity were found between the imaging sets.
Discussion
Advances in MRI technology have led to the development of DWI as an important supplement and/or alternative to Gd-EOB-DTPA-enhanced MRI in the diagnostic and staging of CRLM (13,14). The results of our study showed that the combination of DWI and Gd-EOB-DTPA has the highest sensitivity, thereby confirming earlier findings (15–17). As such, our study stands in contrast to a recent study by Hwang et al. who presented a non-contrast enhanced DWI protocol as a possible alternative to Gd-EOB-DTPA-enhanced MRI with DWI (13). In that study, Gd-EOB-DTPA-enhanced MRI did not improve sensitivity significantly. The characteristics of our study population differ in several ways from Hwang et al. First, in our study, the number of hemangiomas per patient was 6.9-fold higher. Second, the incidence of mucinous CRLM was much higher in our study, 20.5% vs. 2.9% on a patient basis. Third, our study was performed on a 1.5-T MRI system compared to 3.0-T. This might, to some degree, explain the differences in diagnostic performance between the studies since both hemangiomas and mucinous CRLM can make lesion characterization challenging and DWI might benefit from the application of a 3.0-T MRI system (15).
We found the CE-MRI set to be highly accurate with the significantly highest sensitivity while at the same time providing precise anatomical imaging, which makes it the preferred stand-alone preoperative modality (3,8,18–20). Our results are comparable to earlier findings where sensitivities of 60.4–98.8% were found for DWI and 80.3–99.0% for the combination of DWI and Gd-EOB-DTPA-enhanced MRI (7,18,21). The lower sensitivity for CRLM by DWI alone might be due to problems with distinguishing small vascular and biliary structures from small metastases, since both might appear as lesions with diffusion restriction. Gd-EOB-DTPA-enhanced images can help to overcome these issues. Other factors hindering detection of CRLM are subscapular lesion location and motion artefacts, especially if located close to the heart (Fig. 3).
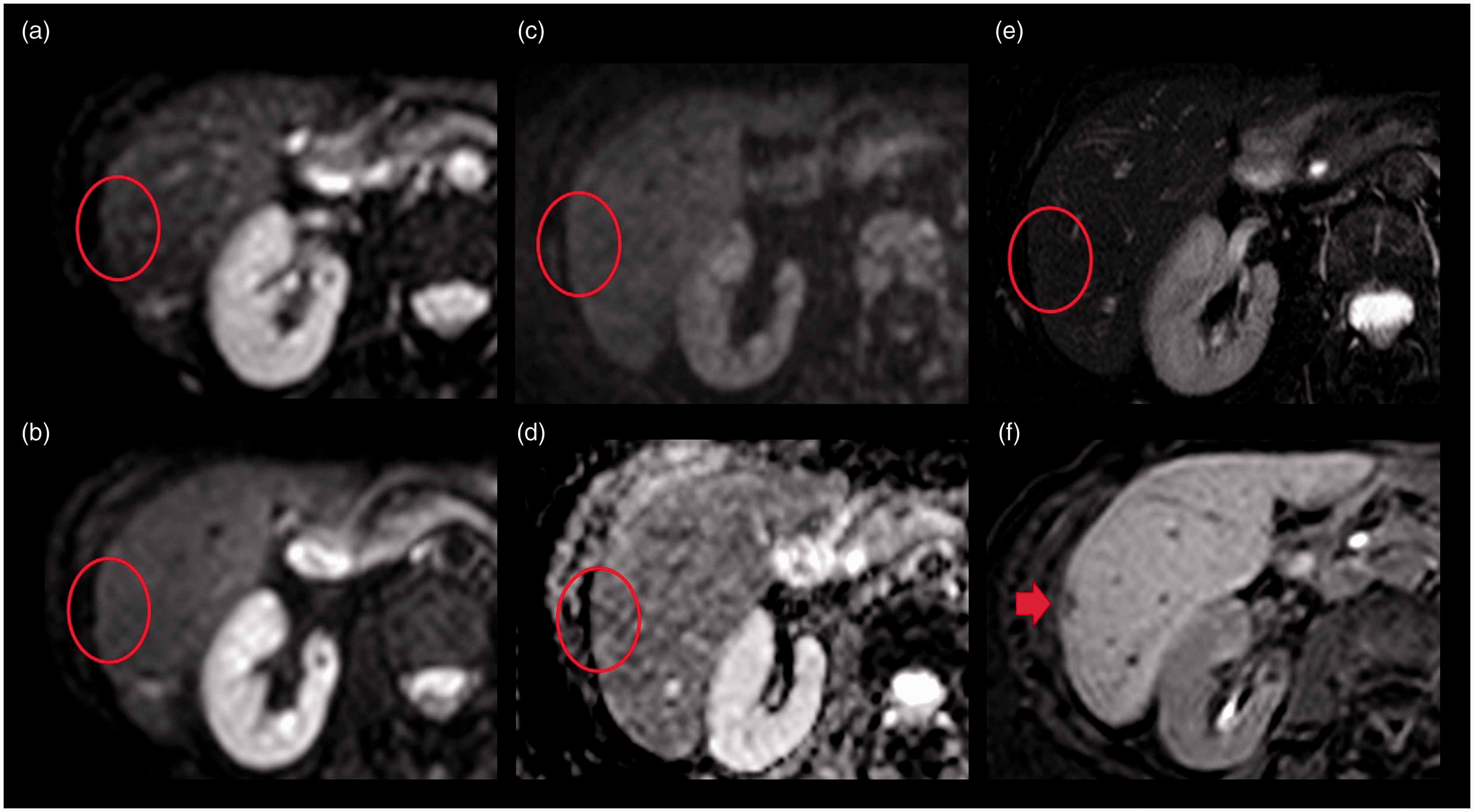
Example of one colorectal liver metastases (CRLM) missed by diffusion-weighted imaging (DWI). CRLM (red arrow) in subcapsular location that was clearly identified by Gd-EOB-DTPA MRI while it was missed by DWI (red circles). (a) DWI b0, (b) DWI b50, (c) DWI b800, (d) ADC map, (e) DWI-T2W-FS, (f) hepatobiliary phase with Gd-EOB-DTPA.
The overall performance of the DWI set, DWI-T2W-FS set, and MDCT set was comparable without significant differences. The investigation of the FN findings that occurred both on the DWI set and the DWI-T2W-FS set showed that 18 CRLM were classified as benign lesions while seven were completely missed. Of these FN findings, 52% were correctly identified as CRLM by the MDCT-set and MDCT-DWI set and 96% by the CE-MRI set. This demonstrates clearly the beneficial effect of contrast media for lesion identification and characterization. In the subgroup analysis for lesions <10 mm, the sensitivity for the DWI set and DWI-T2W-FS set was significantly higher than for the MDCT set (P = 0.002 and P = 0.039). This is in accordance with the literature with the greatest improvement of sensitivity being expected for small lesions <10 mm (2,9,22,23). The lower sensitivity of DWI and DWI-T2W-FS for lesions ≥10 mm was caused by the known difficulties of T2/DWI-based imaging for lesion characterization (24).
Our finding that the CE-MRI set had the significantly lowest specificity was surprising; however, with specificity reaching almost 90%, it was still considerably high but worth further investigation. This was also the reason why the AUC of CE-MRI set was not significantly higher than for the MDCT-DWI set in ROC analysis. The relatively high FP rate for the CE-MRI set was most often caused by difficulties in differentiating CRLM from hemangiomas in 18/22 FP findings. That was especially difficult when mucinous CRLM and hemangiomas were present in the same patient. All six hemangiomas which concurred with mucinous CRLM were interpreted as CRLM while none was FP in the MDCT set. The reason for the difficulties of MRI to correctly characterize hemangiomas in general is probably related to a false washout in hemangiomas that appear iso- or hypo-intense compared to the surrounding hepatocytes which already show a considerable uptake of Gd-EOB-DTPA (25,26). In the DWI sets, where this problem does not occur because no Gd-EOB-DTPA is applied, fewer FP findings were observed. The most often correct assumption of the readers to classify bright lesions on the ADC map as benign is the reason for a higher specificity in these cases, however at the price of reduced sensitivity (17). FP findings are of high importance for optimal patient treatment and might be crucial when evaluating eligibility for liver resection, the only potential curative treatment option for those patients (27–31). In patient groups with high incidence of hemangiomas and mucinous CRLM, accurate characterization of hemangiomas is important. In our study, the incidence of mucinous cancer and hemangiomas was 20.5% and 29.5%, which is higher than expected from the literature with 10–15% and <1–20%, respectively (32,33).
In the usual clinical setting for patients with CRLM under evaluation for liver resection, a MDCT is available, either for primary staging or follow-up. When MDCT does not exclude operability, MRI is often requested; this is especially due to the poor sensitivity of MDCT for small CRLM. Our results support application of MRI including both DWI and Gd-EOB-DTPA for best preoperative identification of all CRLM. By contrast, the much less time-consuming, not Gd-EOB-DTPA-dependent, and therefore cheaper DWI-only protocols could not provide sufficient sensitivity. Additional T2W-FS did not provide any additional value and should therefore not be included into the imaging protocol.
Nevertheless, in the postoperative setting where follow-up is usually based on MDCT, additional DWI might help to identify recurrent disease earlier. In addition, during the primary staging of CRC where MRI is usually not applied, DWI might be an option in case of negative MDCT to improve early detection of small CRLM at reasonable additional costs and increase of examination duration. These applications might improve patient outcome and should be investigated in future studies.
There were limitations to our study. All patients had CRC with suspicious findings for CRLM on a MDCT performed at the referral institution. The high prevalence of CRLM might give bias towards higher sensitivity and transferring our results to a screening situation must be done with caution. On the other hand, the study population was representative for patients under evaluation for liver resection where meticulous identification of all CRLM is crucial. Some small CRLM might have been missed since 21 patients received neoadjuvant chemotherapy after imaging and no systematic contrast-enhanced IOUS of the liver was performed. These biases might cause an overestimation of sensitivity.
In conclusion, the less resource- and time-consuming DWI sets are inferior to Gd-EOB-DTPA-enhanced MRI in patients with CRLM. Gd-EOB-DTPA-enhanced MRI, with its excellent sensitivity, should be the preferred preoperative modality when meticulous lesion identification is essential. Combination of DWI with MDCT improved significantly sensitivity and lesion characterization compared to each modality alone. In case of negative MDCT, DWI could therefore be used as additional screening examination at relatively low costs for staging of primary CRC or as follow-up examination after surgery. T2W-FS, in addition to DWI, did not improve the diagnostic performance and should therefore not be included in DWI protocols for the detection of CRLM.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.