
Abstract
Background
Carotid-cavernous fistulas (CCFs) are commonly misdiagnosed on computed tomography angiography (CTA).
Purpose
This study sought to identify the most sensitive and specific imaging features of CCFs on CTA.
Material and Methods
A retrospective review identified 18 consecutive patients suspected of having a CCF on CTA and subsequently underwent digital subtraction angiography (DSA). Two blinded reviewers assessed multiple findings on CTA: cavernous sinus asymmetry/enlargement; arterial-phase contrast in the cavernous sinus; proptosis; pre- or post-septal orbital edema; and dilated regional vasculature. Each was graded as positive, possible, and negative; “possible” was counted as positive. A third blinded reviewer served as a tiebreaker.
Results
Of 18 patients, nine were true-positive and nine were false-positive. Superior ophthalmic vein early enhancement and dilatation had 100.0% sensitivity (95% confidence interval [CI] 40.0–100.0) and 77.8% specificity (95% CI 44.4–100.0); arterial-phase contrast in the cavernous sinus had 88.9% sensitivity (95% CI 44.4–100.0) and 66.7% specificity (95% CI 18.5–90.1); peri-orbital edema had 88.9% sensitivity (95% CI 35.5–100.0) and 77.8% specificity (95% CI 22.2–100.0). The most specific markers of CCF were superior petrosal sinus and inferior ophthalmic vein dilatation/enhancement (100.0%, 95% CI 88.8–100.0 and 88.9%, 95% CI 44.4–100.0, respectively); the specificity of asymmetric cavernous enlargement was 44.4% (95% CI 11.1–77.7).
Conclusions
Among patients in whom a CCF is suspected on CTA, superior ophthalmic vein dilatation/enhancement and arterial-phase contrast within the cavernous sinus are the most sensitive findings. Asymmetric cavernous sinus enlargement has poor specificity and may result in false-positive diagnoses of CCFs. False positive cases were less likely to have an optimally timed contrast bolus.
Introduction
Carotid-cavernous fistulas (CCFs) are vascular shunts between an internal carotid artery (ICA) and/or external carotid artery (ECA) and the adjacent cavernous sinus (1–3). CCFs have traditionally been categorized based on etiologic (spontaneous versus traumatic), hemodynamic (high versus low flow), and anatomic (direct versus indirect) characteristics (1). Direct CCFs are typically secondary to trauma and are less commonly caused by rupture of an ICA aneurysm or an iatrogenic cause; indirect, or dural, CCFs tend to be idiopathic (4). The classic clinical presentation of affected patients is acute onset of Dandy’s triad: bruit, exophthalmos, and conjunctival chemosis (5). However, palpebral swelling, diplopia, vision loss, headache, pulsatile tinnitus, and facial pain may also be reported (3,6,7).
The gold standard modality for the diagnosis of CCFs is digital subtraction angiography (DSA) (4,8). Nevertheless, the initial diagnosis and characterization of such vascular shunts often rely on non-invasive modalities such as computed tomography angiography (CTA) and magnetic resonance angiography (MRA). Of these, CTA has been shown to be the superior modality in the detection of CCFs (9). Diagnosis of a CCF on CTA has been reported to depend on the observation of arterial enhancement within the cavernous sinus (3). A number of additional imaging features of CCFs have been described and include superior ophthalmic vein engorgement and exophthalmos (10–12).
Despite the well-known imaging characteristics of CCFs, they remain a common pitfall of CTA interpretation. Normal anatomic variants, suboptimal contrast bolus timing, and unrelated pathology may all cause a radiologist to falsely raise the suspicion for a CCF that is ultimately found to not exist on DSA. Hence, this study set out to retrospectively compare the CTA imaging findings of patients with CCFs to patients in whom CCFs were incorrectly suspected to be present. The purpose of this study is to establish the imaging characteristics of CCFs that could act as a diagnostic roadmap during image interpretation.
Material and Methods
Patient selection
Institutional review board approval was obtained for the purposes of this study. A retrospective review was completed of consecutively imaged patients who had CTA findings read as being suspicious for a CCF and subsequently underwent cerebral angiography (1 October 2009 to 31 January 2019); DSA was considered the gold standard for diagnosis (13,14). Included patients were divided into two cohorts: (i) patients that had a CCF confirmed on DSA (“true positive”); and (ii) patients whose follow-up DSA was negative for CCF despite the CTA findings (“false positive”).
Imaging review and interpretation
Two neuroradiologists, blinded to results of cerebral angiography, completed a retrospective review of the CTA images; a third neuroradiologist, also blinded, served as tiebreaker for discordant results. For each examination, both reviewers assessed the quality of contrast bolus timing, graded on a scale based on the differentiation between arterial and venous opacification: 1 = extremely poor (venous opacification greater than arterial opacification); 2 = some differentiation, though sub-optimal; and 3 = excellent (all contrast is within the arterial vasculature; no venous opacification present).
Cavernous sinuses were assessed for symmetry in size and opacification (graded as definite asymmetry, possible asymmetry, no asymmetry). Reviewers also noted the presence or absence of multiple findings, all of which were independently assessed on both sides: (i) cavernous sinus enlargement (in which one or both cavernous sinus was considered abnormally increased in size); (ii) arterial-phase contrast with the cavernous sinus (defined as being higher density than the transverse and/or sigmoid sinus); (iii) proptosis; (iv) pre-septal periorbital edema; (v) post-septal orbital edema; (vi) acute fracture adjacent to the cavernous sinus; and (vii) aneurysm of the cavernous segment of the ICA. Additionally, reviewers assessed a number of arterial and venous structures for abnormal enlargement and/or opacification: (i) superior ophthalmic vein; (ii) inferior ophthalmic vein; (iii) superior petrosal sinus; (iv) inferior petrosal sinus; (v) sphenoparietal sinus; (vi) basal vein of Rosenthal; and (vii) facial veins. Finally, reviewers noted whether a CCF was thought to exist.
All variables were rated on a semi-quantified confidence scale of how likely reviewers felt the findings were to exist: 1 = absent; 2 = possibly present; or 3 = definitely present. All “possible” cases were considered positive. Any noted pertinent findings were considered positive regardless of laterality of true-positive CCFs, e.g. a dilated right facial vein was considered positive even if the fistula was located on the left side.
Statistical analysis
Diagnostic performance to detect CCF for each characteristic was evaluated by calculating the sensitivity and specificity. Inter-observer agreement was assessed between the two readers by Cohen’s Kappa. Sensitivity and specificity were calculated using R version 3.4.2 (Vienna, Austria) and Cohen’s Kappa was calculated using SAS statistical software version 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
Baseline patient characteristics
Eighteen patients were included in the cohort: nine true-positive (4 women; average age 34.8 ± 17.2 years); and nine false-positive (5 women; average age = 62.4 ± 12.9 years). Of the true-positive patients, 5/9 (55.6%) were located on the right side. Of the nine true-positive cases, 3 (33.3%) were direct CCFs; all other cases were indirect. Three of the true-positive cases were secondary to blunt trauma, all of which resulted in direct fistulas.
Imaging review
For all patients, the quality of contrast bolus was deemed excellent in 5/18 (27.8%), moderate in 10/18 (55.6%), and poor in 3/18 (16.7%) patients. Of the contrast bolus timings of the false-positive patients, 1/9 was excellent, 7/9 were moderate, and 1/9 was poor; of the true-positive patients, 4/9 were excellent, 3/9 were moderate, and 2/9 were poor. Asymmetrical cavernous sinus size was seen in 14/18 (77.8%) of the entire patient cohort; 6/9 (66.7%) of the true-positive cases and 8/9 (88.9%) of the false-positive cases (Figs. 1 and 2). Of all patients, 14/36 (38.9%) had enlargement of either the right or left cavernous sinus: 9/18 (50.0%) of true-positive cases (either right or left cavernous sinus) and 5/18 (27.8%) of false-positive cases.
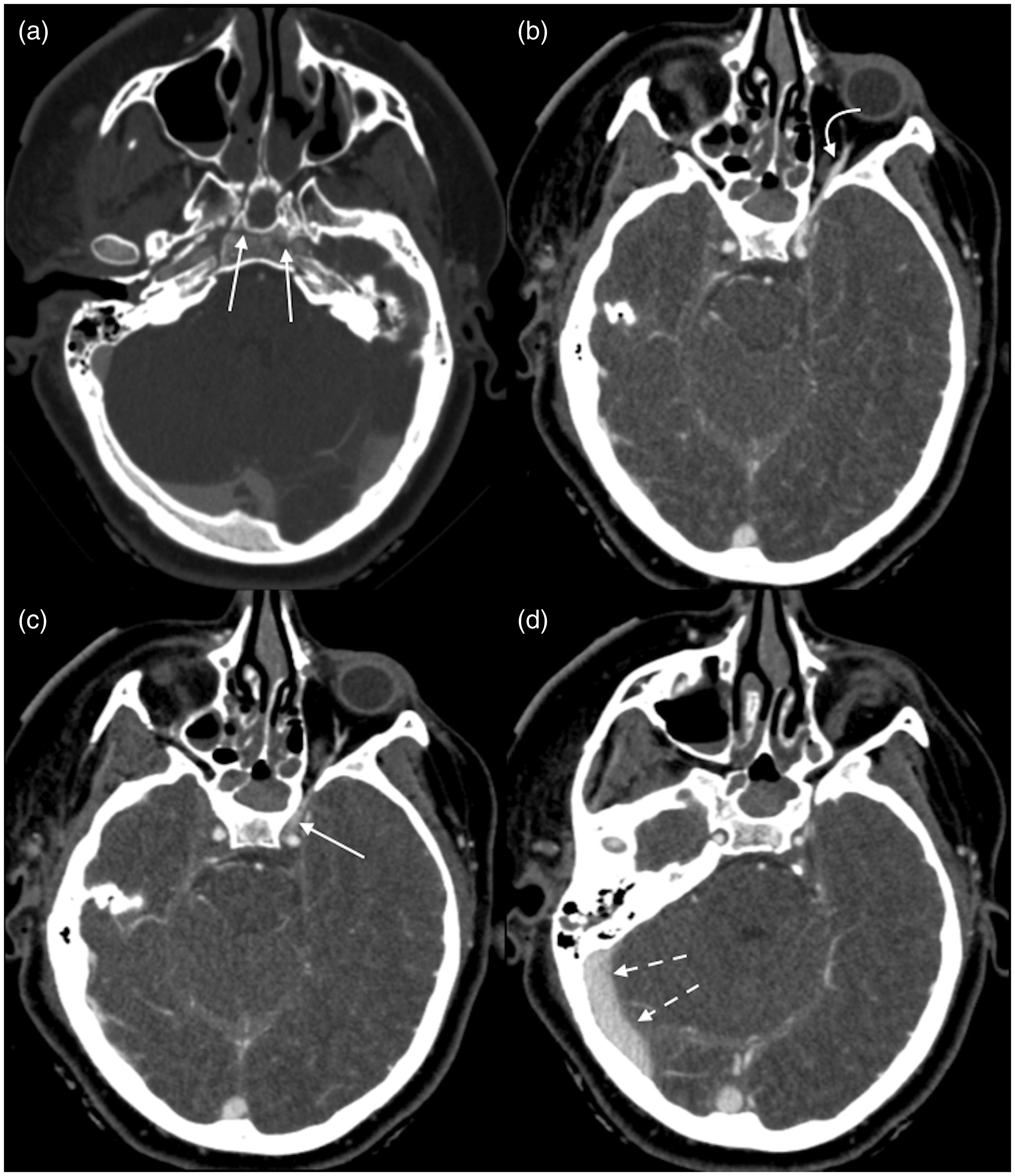
A 16-year-old girl presented after sustaining a traumatic injury to her head during a water skiing accident. (a) CTA demonstrated an acute horizontal fracture through her clivus (arrows). (b) The left superior ophthalmic vein was asymmetrically dilated compared to the contralateral side (curved arrow). (c) Slight asymmetric prominence of the left cavernous sinus was noted, although it was not enlarged (straight arrow). (d) However, the contrast phase within the cavernous sinus was equal to the right transverse sinus, indicating venous phase of the contrast bolus (dashed arrows). No CCF was identified on subsequent DSA.
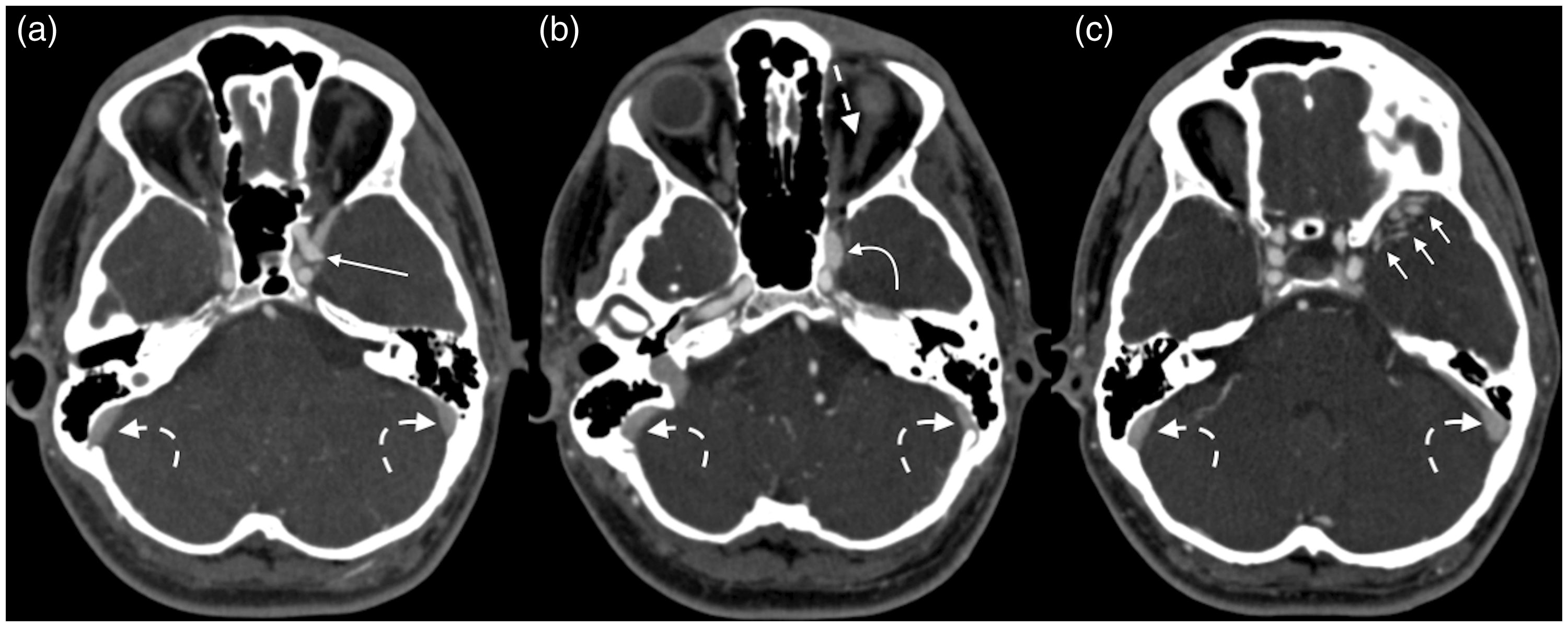
A 25-year-old man presented with diplopia. (a) CTA demonstrated a 2 × 2 mm aneurysm arising from the lateral aspect of the left cavernous ICA (straight arrow). (b) The left cavernous sinus appeared asymmetrically prominent and enlarged (curved arrow) and (c) the left sphenoparietal sinus and adjacent vasculature were engorged (short arrows). (b) The left superior ophthalmic vein was neither enlarged nor opacified with contrast (straight dash arrow) and contrast density in the distal transverse and sigmoid sinuses (curved dash arrows) was similar to that seen in the cavernous sinus. Findings were overall concerning for a direct CCF secondary to rupture of an aneurysm. However, no fistula was seen on the subsequent DSA.
Sensitivities and specificities of all studied parameters are shown in Table 1. The most sensitive markers of CCFs were superior ophthalmic vein enlargement/early enhancement (100.0%; 95% confidence interval [CI] = 40.0–100.0), arterial-phase enhancement of the cavernous sinus (88.9%; 95% CI = 44.4–100.0), and periorbital edema (88.9%; 95% CI = 35.5–100.0) (Figs. 3 and 4). The most specific findings were superior petrosal sinus enlargement/early enhancement (100.0%; 95% CI = 88.9–100.0) and proptosis (100.0%; 95% CI = 40.0–100.0). The specificity of an enlarged cavernous sinus was 44.4% (95% CI = 11.1–77.7). Fractures adjacent to the cavernous sinus were identified four times (three patients, one bilateral), all of which were among false-positive cases. No cases (neither true-positive nor false-positive) noted abnormal enhancement and/or dilatation of the basal vein of Rosenthal.
Sensitivity and specificity of findings associated with CCFs.*
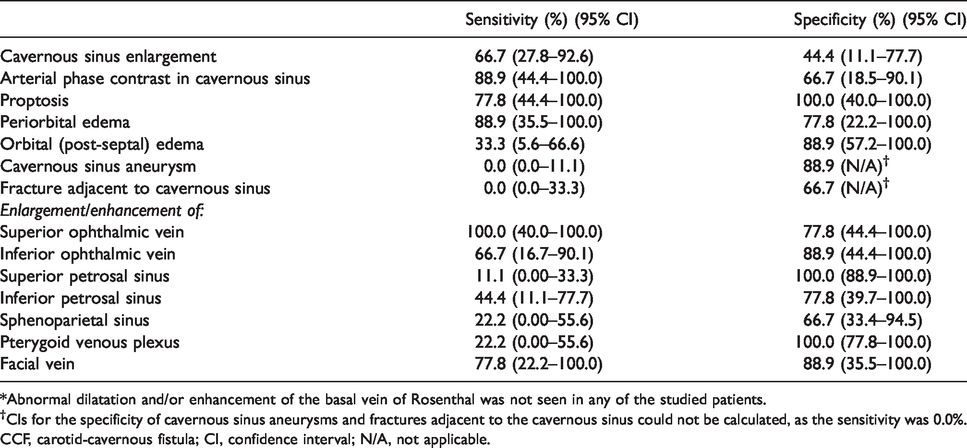
*Abnormal dilatation and/or enhancement of the basal vein of Rosenthal was not seen in any of the studied patients.
†CIs for the specificity of cavernous sinus aneurysms and fractures adjacent to the cavernous sinus could not be calculated, as the sensitivity was 0.0%.
CCF, carotid-cavernous fistula; CI, confidence interval; N/A, not applicable.
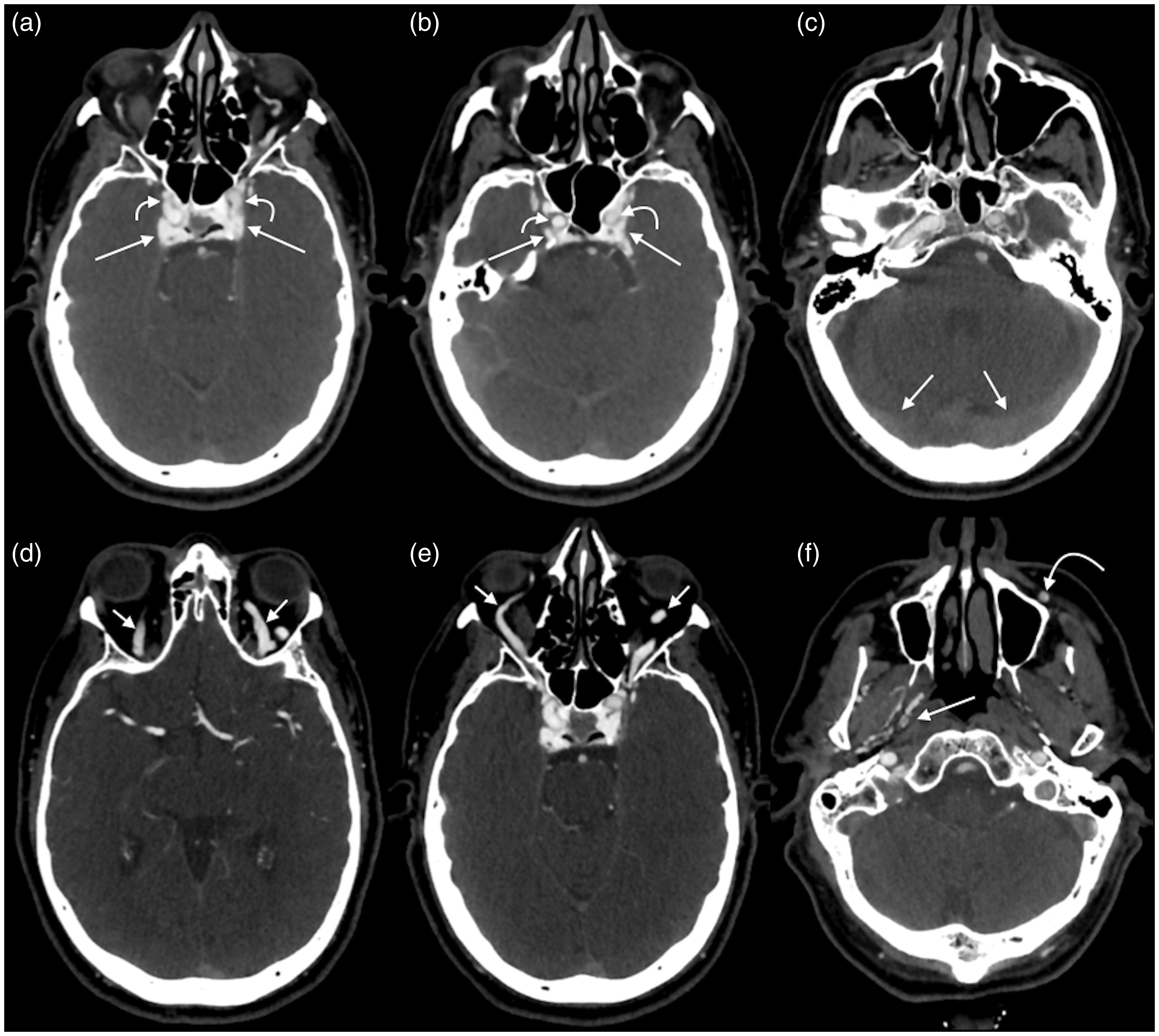
A 60-year-old man presented with progressive visual acuity decline following blunt trauma to the face. (a, b) CTA demonstrated marked opacification of both cavernous sinuses (straight arrows), with contrast density similar to that of the adjacent ICAs (curved arrows). (c) The density of contrast material within the cavernous sinuses was significantly higher than the transverse sinuses (arrows). (d) Both superior ophthalmic veins (short arrows) and (e) inferior ophthalmic veins (short arrows) were dilated and opacified. (f) The right pterygoid plexus was asymmetrically prominent on the right (dashed arrow) and the left facial vein was asymmetrically enlarged on the left (curved arrow). Subsequent DSA showed a direct right-sided CCF.
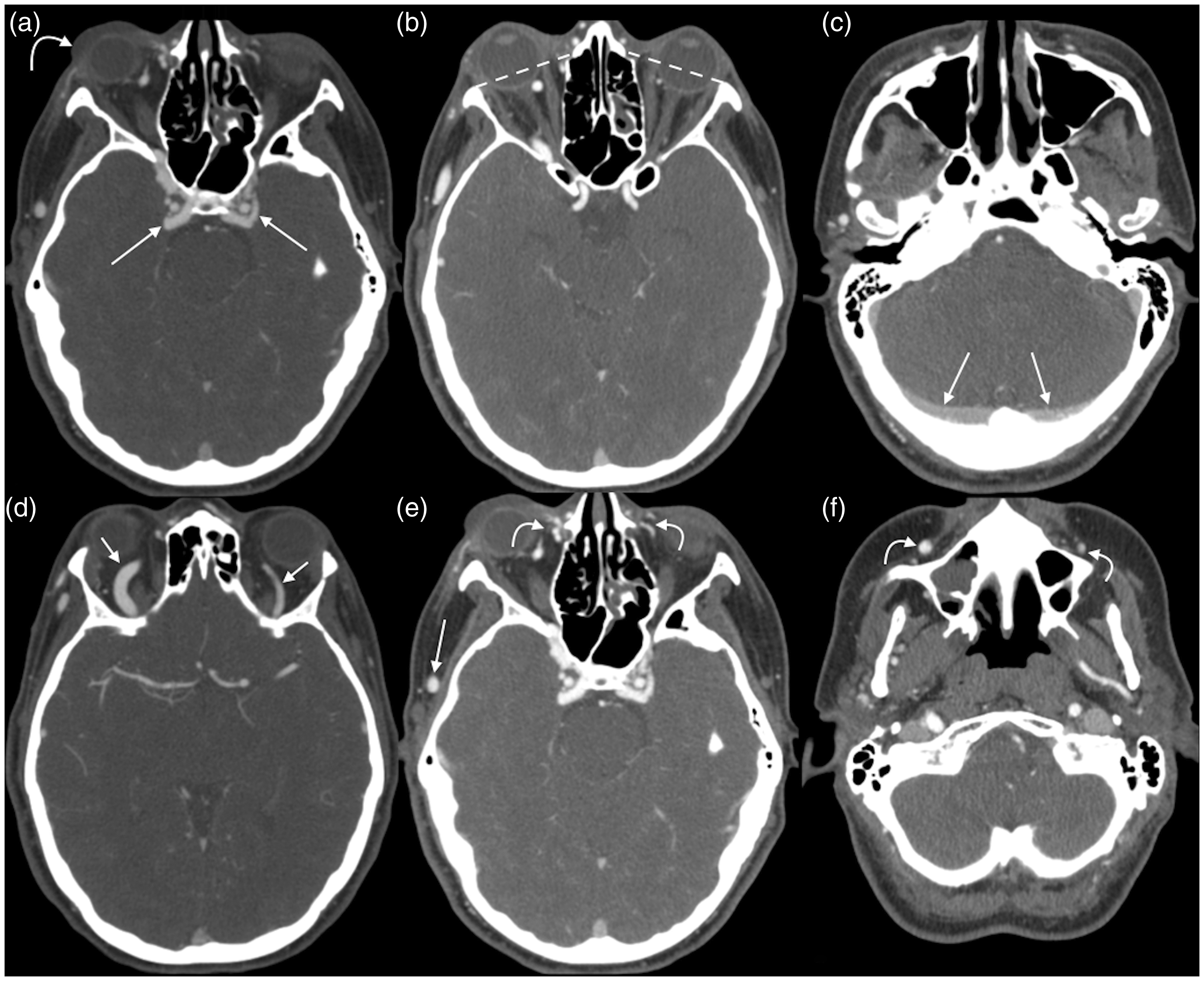
A 34-year-old woman presented with a 10-day history of right proptosis, periorbital swelling, and blurry vision; she reportedly had a physical altercation with her ex-boyfriend one month before presentation. (a) CTA showed right greater than left opacifiation of the cavernous sinuses (straight arrows) as well as right-sided periorbital edema (curved arrow) and (b) proptosis (dashed lines). (c) Density of contrast within the cavernous sinuses was greater than that of the transverse sinuses (arrows), confirming arterial to venous shunting. (d) Both superior ophthalmic veins were opacified and distended, right larger than left (short arrows). (e, f) Similarly, there was right greater than left opacification and distention of the facial veins (curved arrows), as well as the right superficial temporal vein (e, arrow). A follow-up DSA demonstrated a direct right CCF.
Inter-observer agreement
Inter-observer agreements of each parameter are detailed in Table 2. Findings with the highest inter-observer agreements were fracture adjacent to the cavernous sinus (κ = 1.00; 95% CI = 1.00–1.00), cavernous sinus aneurysm (κ = 1.00; 95% CI = 1.00–1.00), superior ophthalmic vein enlargement and early enhancement (κ = 0.77; 95% CI = 0.48–1.00), and facial vein enlargement and early enhancement (κ = 0.77; 95% CI = 0.48–1.00).
Inter-observer agreement for all studied imaging findings.
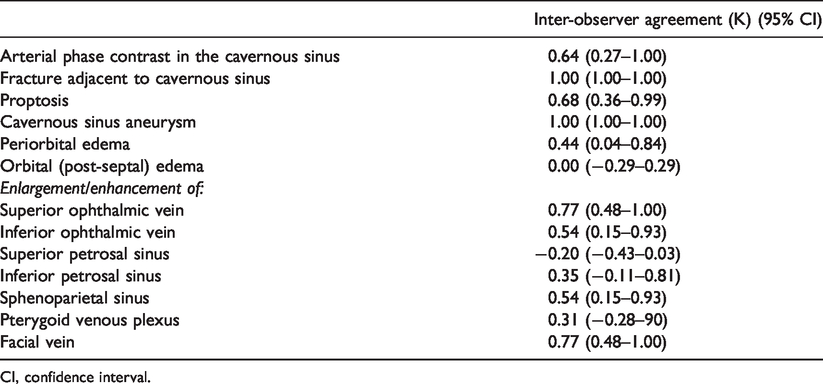
CI, confidence interval.
Discussion
This study sought to assess the sensitivity and specificity of multiple CTA findings for CCFs. The results demonstrated wide variability in the degree to which such findings are able to accurately diagnose CCFs. Superior ophthalmic vein enlargement with early enhancement was highly sensitive, while enlargement/enhancement of the superior petrosal sinus and pterygoid venous plexus and proptosis were highly specific. To the knowledge of the authors of this study, this is the first such comparison of findings among true- and false-positive cases of CCFs suspected on CTA.
Multiple prior studies have described the use of CTA in the diagnosis CCFs (9,15–18). Nevertheless, as this study shows, diagnosing CCFs on CTA can be made difficult by normal anatomic variants, suboptimal timing of the contrast bolus, and asymmetry of structures that are often implicated as imaging evidence of CCFs. Furthermore, patients may present with a wide range of symptoms, which can also confound the diagnosis; nerve palsies, headaches associated with conjunctivitis, painful ophthalmoplegia, symptoms in the contralateral eye, and other non-specific symptoms have all been linked to CCFs (19–23).
The current study assessed both cavernous sinus symmetry (similarity between sides) and size (subjective opinion of size, regardless of symmetry). The majority of patients had cavernous sinus asymmetry. However, this was more frequently observed in false-positive cases, in which an asymmetric appearance of the cavernous sinuses was noted in all but one case. This suggests that the presence of cavernous sinus asymmetry contributed to the false-positive cases within the cohort, whereas CCFs were correctly diagnosed when the radiologist relied more on other related findings. “Enlarged” cavernous sinuses were less commonly seen among false-positive cases than true-positive cases, although its poor specificity also made this finding a potential source of falsely identified CCFs. These results underscore the importance of noting the quality of the contrast bolus timing when suspecting CCFs. A CCF often appears as early enhancement of the cavernous sinus on the side of the CCF, but not within the contralateral cavernous sinus (11). Unfortunately, suboptimal timing of the contrast bolus has been reported to occur in up to 17% of examinations (24).
The largest prior study that focused on the utility of CTA imaging findings in CCFs was performed by Lee et al. (3). The authors reported sensitivities in the range of 81–100% of ophthalmic vein engorgement, cavernous sinus engorgement, similar enhancement of the ICA and cavernous sinus, or greater enhancement in the cavernous sinus than the transverse sinus. However, the superior sensitivities reported by Lee et al. were likely related to differences in the research methodology; the authors of that study compared true-positive cases with normal controls. In addition, the study by Lee et al. only assessed the cavernous sinus and superior ophthalmic vein. The larger scope of the current study was able to demonstrate that periorbital edema, proptosis, and facial vein engorgement are also sensitive imaging features of CCFs.
All retrospective studies have limitations. The current study was limited by a small sample size. In addition, the study had inherent selection bias, as patients were included only if their initial CTA examination was suspected to have a CCF. This could lead to over-representation of imaging features that often mislead radiologists. However, this bias was unavoidable, as the study’s purpose was to compare imaging findings among patient with true- and false-positive examinations. Next, both indirect and direct fistulas were included in the same true-positive group; differences between the groups were not assessed. Future research may be useful to distinguish between imaging features of these entities on CTA.
In conclusion, accurately diagnosing CCFs on CTA requires close examination of multiple findings. Arterial-phase contrast in the cavernous sinus and superior ophthalmic vein dilatation/enhancement are the most sensitive findings for CCFs; proptosis and enlargement/enhancement of the superior petrosal sinus and pterygoid venous plexus are the most specific. Asymmetric cavernous sinus enlargement has poor specificity and is a potential diagnostic pitfall that may result in false-positive diagnoses.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.