
Abstract
Background
Hemorrhagic transformation increases mortality and morbidity in patients with acute ischemic stroke.
Purpose
The purpose of this study is to evaluate the diagnostic performance of magnetic resonance imaging (MRI) for prediction of hemorrhagic transformation in acute ischemic stroke.
Material and Methods
A systematic literature search of MEDLINE and EMBASE was performed up to 27 July 2018, including the search terms “acute ischemic stroke,” “hemorrhagic transformation,” and “MRI.” Studies evaluating the diagnostic performance of MRI for prediction of hemorrhagic transformation in acute ischemic stroke were included. Diagnostic meta-analysis was conducted with a bivariate random-effects model to calculate the pooled sensitivity and specificity. Subgroup analysis was performed including studies using advanced MRI techniques including perfusion-weighted imaging, diffusion-weighted imaging, and susceptibility-weighted imaging.
Results
Nine original articles with 665 patients were included. Hemorrhagic transformation is associated with high permeability, hypoperfusion, low apparent diffusion coefficient (ADC), and FLAIR hyperintensity. The pooled sensitivity was 82% (95% confidence interval [CI] 61–93) and the pooled specificity was 79% (95% CI 71–85). The area under the hierarchical summary receiver operating characteristic curve was 0.85 (95% CI 0.82–0.88). Although study heterogeneity was present in both sensitivity (I2=67.96%) and specificity (I2=78.93%), a threshold effect was confirmed. Studies using advanced MRI showed sensitivity of 92% (95% CI 70–98) and specificity of 78% (95% CI 65–87) to conventional MRI.
Conclusion
MRI may show moderate diagnostic performance for predicting hemorrhage in acute ischemic stroke although the clinical significance of this hemorrhage is somewhat uncertain.
Introduction
Hemorrhagic transformation increases mortality and morbidity in patients with acute ischemic stroke (1). Several factors are known to be associated with hemorrhagic transformation, including age, National Institutes of Health Stroke Scale (NIHSS) score, the etiology of stroke, and use of recombinant tissue plasminogen activator (2–4). In addition to these factors, the abilities of various imaging modalities to predict hemorrhagic transformation have also been evaluated, based on the fact that disruption of the blood–brain barrier may be associated with hemorrhagic transformation (5).
Multiple studies have reported the diagnostic performance of magnetic resonance imaging (MRI) for prediction of hemorrhagic transformation in acute ischemic stroke (5–13). Conventional MRI using FLAIR sequences, as well as advanced MRI protocols including perfusion-weighted imaging (PWI) (dynamic susceptibility-weighted [T2*-weighted (T2*W)] imaging and dynamic contrast-enhanced [T1-weighted] imaging) and diffusion-weighted imaging (DWI) have shown promising results. In particular, T2*W imaging can sensitively reveal hemorrhagic events of a mild degree in ischemic stroke. If MRI can provide imaging parameters predicting hemorrhagic transformation, it could be used to identify appropriate candidates for thrombolytic therapy and would therefore be a valuable modality for clinical decision-making.
However, the diagnostic performance of MRI for prediction of hemorrhagic transformation in acute ischemic stroke has not yet been systematically evaluated. Therefore, this study aimed to evaluate the diagnostic performance of MRI for prediction of hemorrhagic transformation in acute ischemic stroke.
Material and Methods
This study was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (14). Institutional Review Board approval was waived in this meta-analysis, but the included studies had informed consent obtained from all individual participants in each study.
Literature search
A systematic literature search of MEDLINE and EMBASE was performed to find original articles evaluating the diagnostic performance of MRI for prediction of hemorrhagic transformation in acute ischemic stroke published up to 27 July 2018. The literature search, literature selection, data extraction, and quality assessment were performed independently by two reviewers (CHS and SCJ). The search terms were: ((acute ischemic stroke)) AND ((“hemorrhagic transformation”) OR (“haemorrhagic transformation”)) AND ((“magnetic resonance imaging”) OR (“MR imaging”) OR (MRI)). The search was not restricted by language, starting date, or whether articles were animal- or human-based. Any additional manually identified articles were included to expand the search.
Eligibility criteria
The following eligibility criteria were applied: (i) patients presented with stroke symptoms; (ii) patients underwent emergency MRI before treatment; (iii) patients underwent follow-up MRI or CT to detect hemorrhagic transformation; and (iv) articles had sufficient information for the reconstruction of two by two tables for determination of the diagnostic performance of MRI for prediction of hemorrhagic transformation in acute ischemic stroke.
Articles were excluded because of any of the following: (i) review articles; (ii) conference abstracts; (iii) animal studies; (iv) case reports with a sample size ≤10 patients; (v) insufficient data to reconstruct a 2 × 2 table; and (vi) studies with a partially overlapping patient cohort. In the case of an article not providing sufficient information for the reconstruction of 2 × 2 tables, an author of the article was contacted for the provision of further information.
Data extraction and quality assessment
The following information was extracted from the included studies using a standardized form: (i) Demographic characteristics: institution, study period, study design, consecutive or non-consecutive enrollment, reference standard, the interval between MRI and follow-up MRI or CT, sample size, number and percentage of patients with hemorrhagic transformation, male-to-female ratio, mean age, and inclusion criteria after symptom onsets; and (ii) MRI characteristics: the strength of the magnet, vendor, machine, MRI protocol, number of readers, reader experience, blindness of readers to clinical or reference standard, MRI parameters, and corresponding cut-off values for diagnosis of hemorrhagic transformation. Quality assessment of the included studies was performed according to the Quality Assessment of Diagnostic Accuracy Studies-2 (QUADAS-2) tool (15).
Data synthesis and analysis
The primary outcome was to evaluate the diagnostic performance of MRI for predicting hemorrhagic transformation in patients with acute ischemic stroke, with various MRI parameters being used. The individual sensitivities and specificities of each study were evaluated. If diagnostic performance was provided for several MRI parameters within a single study, the highest diagnostic performance was selected to represent the results of that study.
Study heterogeneity was investigated using the following methods: (i) Cochran’s Q-test with P < 0.05 indicating the presence of study heterogeneity; (ii) Higgins inconsistency index (I2) test with I2 > 50% indicating the presence of study heterogeneity (16); (iii) visual assessment of the difference between the 95% confidence and prediction regions in the HSROC curve with a large difference indicating heterogeneity; (iv) visual assessment of a coupled forest plot to determine the presence of a threshold effect with a threshold effect indicating a positive correlation between sensitivity and false-positive rate among the selected studies (17); and (v) a Spearman correlation with a coefficient > 0.6 indicating a threshold effect (18).
A bivariate random-effects model was used to obtain the pooled sensitivity and pooled specificity, and their 95% confidence intervals (CIs) (17,19–22). The diagnostic odds ratio (DOR) defined as the odds of having a positive MRI result in patients with hemorrhagic transformation compared to the odds of having a positive MRI result in patients without hemorrhagic transformation was also obtained. A coupled forest plot and a hierarchical summary receiver operating characteristic (HSROC) curve with 95% confidence and prediction regions were plotted. A Deeks’ funnel plot was also constructed to verify publication bias, with statistical significance being evaluated using Deeks’ asymmetry test (23). Subgroup analyses were performed on studies using advanced MRI techniques, including PWI and DWI, studies using PWI parameters, and studies using conventional MRI parameters. In addition, studies predicting symptomatic hemorrhagic transformation were also analyzed.
All statistical analyses were conducted by one of the authors (CHS, with five years of statistical experience in performing systematic reviews and meta-analysis) using the “Metandi” and “Midas” modules in Stata 15.0 (StataCorp, College Station, TX, USA) and the “Mada” package in R 3.4.1 (R Foundation for Statistical Computing, Vienna, Austria). A P value < 0.05 was considered to indicate statistical significance.
Results
Literature search
The literature selection process is illustrated in Fig. 1. The systematic literature search identified 202 articles. After removing 10 duplicate articles, screening of the titles and abstracts of the 192 remaining articles was conducted. A total of 152 articles were excluded as follows: 106 articles that were not in the field of interest; 18 reviews; 11 conference abstracts; nine animal studies; and eight case reports. Full-text reviews were then conducted on the remaining 40 articles; a further 31 articles were excluded as follows: 23 articles with insufficient data to reconstruct 2 × 2 tables; five with a partially overlapping cohort; two that were not in the field of interest; and one case report. Finally, nine original articles evaluating the diagnostic performance of MRI for prediction of hemorrhagic transformation in acute ischemic stroke and with a total of 665 patients were included in this study (5–13).
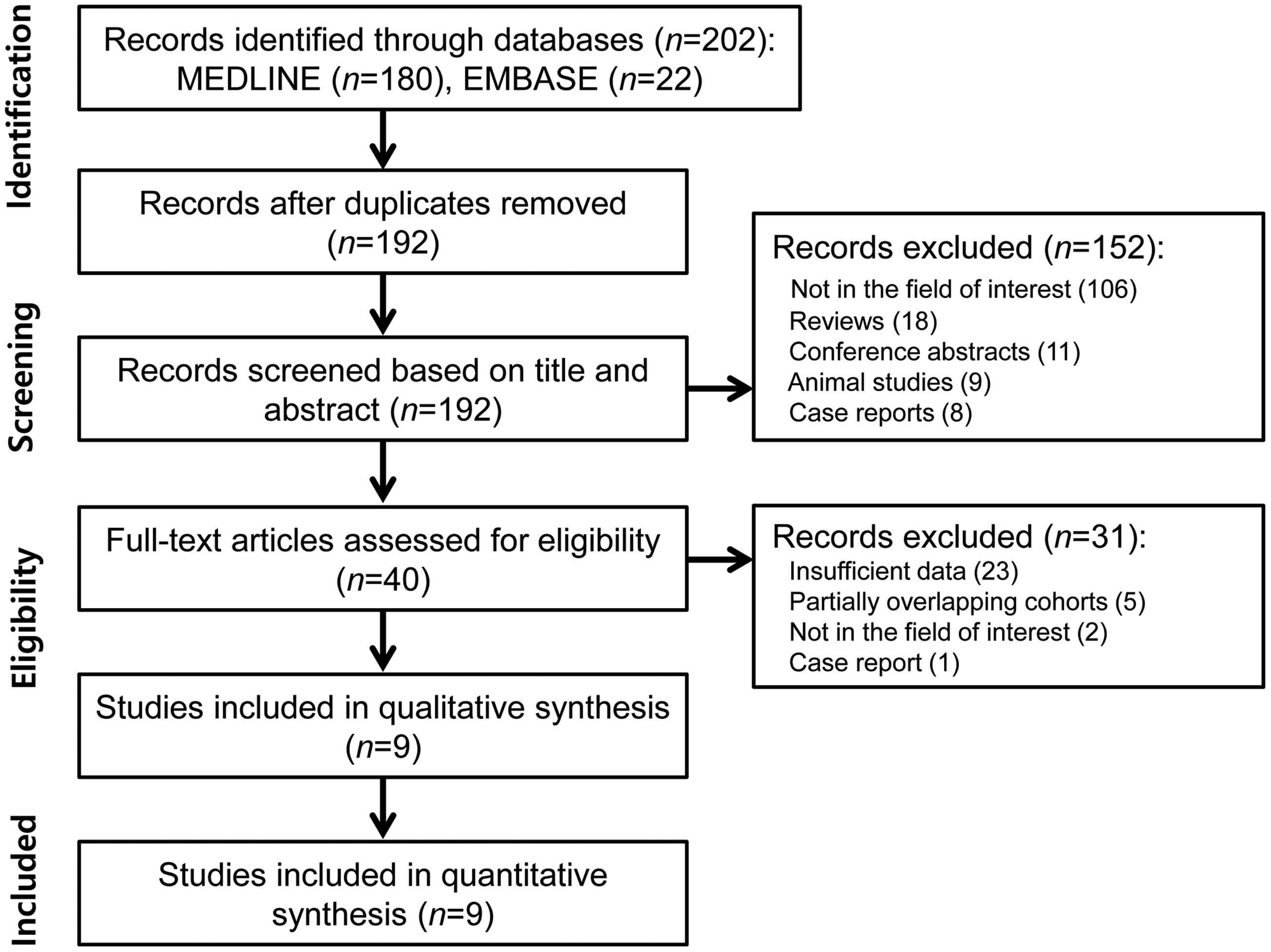
Flow diagram of the literature selection process.
Characteristics of the included studies and quality assessment
The demographic characteristics are listed in Table 1. One study was a randomized controlled trial (91 patients) (6), two studies were of a prospective design (7,9), and five were retrospective (5,8,11–13). Hemorrhagic transformation categorized as hemorrhagic infarction and parenchymal hematoma was evaluated according to the European Cooperative Acute Stroke Study (4). In 7/9 studies, hemorrhagic transformation was assessed using all types of hemorrhagic transformation (5,8–13), whereas two studies used parenchymal hematoma (6,7). In 8/9 studies, patients underwent thrombolysis; among them (5–8,10–13), only one study included patients underwent mechanical thrombectomy (5). For the reference standard, seven studies used follow-up MRI (gradient-echo T2*W image) or CT (5–10,13), one study used follow-up CT (12), and one study used MRI (11).
Demographic characteristics of the included studies.
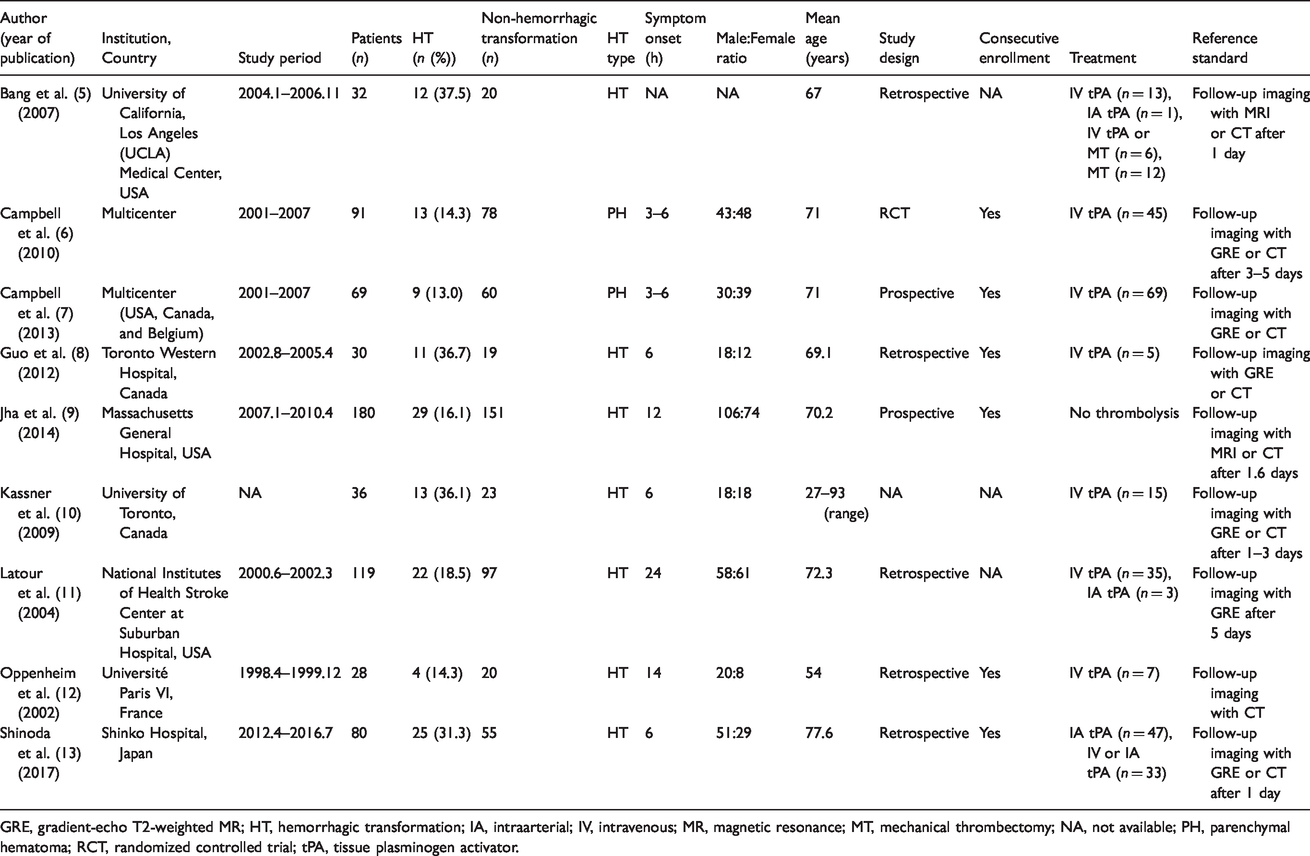
GRE, gradient-echo T2-weighted MR; HT, hemorrhagic transformation; IA, intraarterial; IV, intravenous; MR, magnetic resonance; MT, mechanical thrombectomy; NA, not available; PH, parenchymal hematoma; RCT, randomized controlled trial; tPA, tissue plasminogen activator.
The quality assessment results are shown in Suppl. Fig. 1. The quality of the included studies was considered moderate, with all nine studies scoring >4 out of 7 in the QUADAS-2 domains. In the patient selection domain, three studies were considered as having an unclear risk of bias due to non-consecutive enrollment (5,10,11). In the index test domain, four studies were considered to have an unclear risk of bias because it was unclear whether MRI was interpreted blindly to the reference standard (6,7,10,13). In the reference standard domain, four studies were again considered as having an unclear risk of bias as it was unclear whether the reference standard was evaluated blindly to the MRI (6,7,10,13). In the flow and timing domain, three studies were regarded as having an unclear risk of bias because the time intervals between MRI and the reference standard were not described (7,8,12).
MRI parameters predicting hemorrhagic transformation: a systematic review
The detailed MRI characteristics are described in Table 2. Seven studies used 1.5-T scanners (5,7,8,10–13). Various MRI protocols and corresponding parameters were used to predict hemorrhagic transformation in acute ischemic stroke, with 6/9 (67%) studies using advanced MRI parameters (PWI (5–7,10) and DWI (12,13)) and three studies using conventional MRI (8,9,11).
MRI characteristics of the included studies.
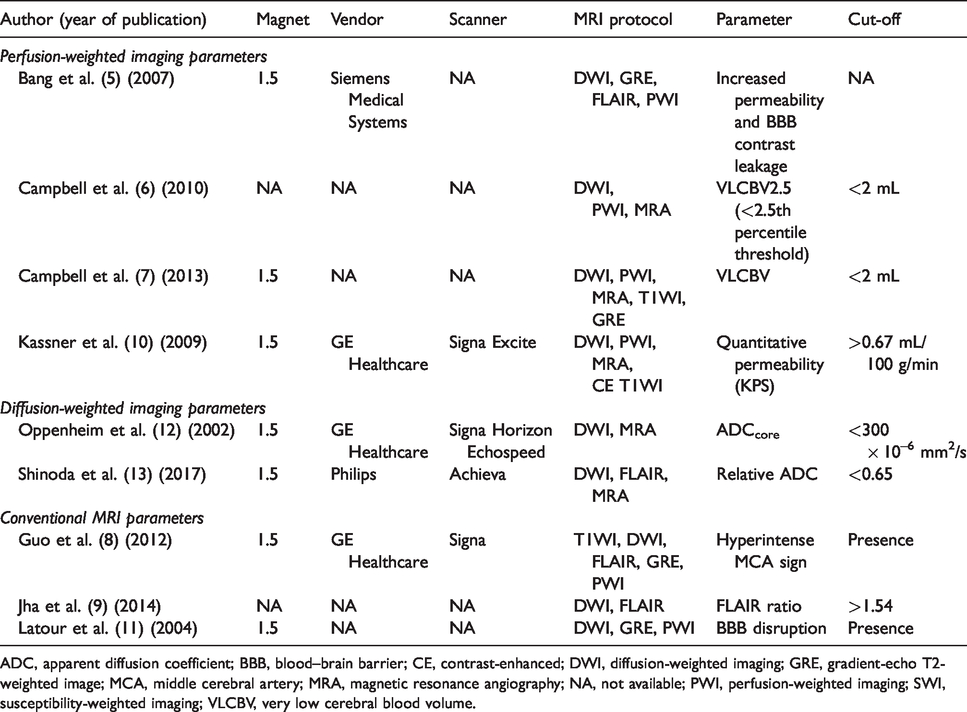
ADC, apparent diffusion coefficient; BBB, blood–brain barrier; CE, contrast-enhanced; DWI, diffusion-weighted imaging; GRE, gradient-echo T2-weighted image; MCA, middle cerebral artery; MRA, magnetic resonance angiography; NA, not available; PWI, perfusion-weighted imaging; SWI, susceptibility-weighted imaging; VLCBV, very low cerebral blood volume.
Among the four studies using PWI, two used permeability-related parameters (6,7), and both showed significantly higher blood–brain barrier permeability in a hemorrhagic transformation group compared with a non-hemorrhagic transformation group. The other two studies used cerebral blood volume (CBV) (5,10) and showed significantly lower CBV in hemorrhagic transformation groups compared with non-hemorrhagic transformation groups. Two studies used the apparent diffusion coefficient (ADC) as a parameter (12,13), and these showed significantly lower ADCcore (12) and relative ADC (13) in hemorrhagic transformation groups compared with non-hemorrhagic transformation groups.
In terms of conventional MRI, all studies used FLAIR signal intensity (8,9,11), including hyperintense middle cerebral artery sign (8) and FLAIR ratio (9), and identified the appearance of hyperintense signal in the sulci or ventricles in comparison with previous or subsequent examinations as disruption of the blood–brain barrier (11).
Diagnostic performance of MRI for prediction of hemorrhagic transformation: a meta-analysis
The sensitivities and specificities of the individual studies showed wide variation, in the range of 48–100% and 58–100%, respectively (Fig. 2). The Q-test revealed the presence of study heterogeneity across the included studies (Q = 30.070, P < 0.001), with the Higgins I2 statistic also revealing that study heterogeneity was present in both sensitivity (I2 = 67.96%) and specificity (I2 = 78.93%). There was a relatively small difference between the 95% confidence region and 95% prediction region in the HSROC curve, which indicated that the possibility of study heterogeneity was low (Fig. 3). Visual assessment of the coupled forest plot demonstrated the presence of a threshold effect (Fig. 2), as did the Spearman correlation coefficient between the sensitivity and false positive rate (0.831, 95% CI = 0.372–0.963).
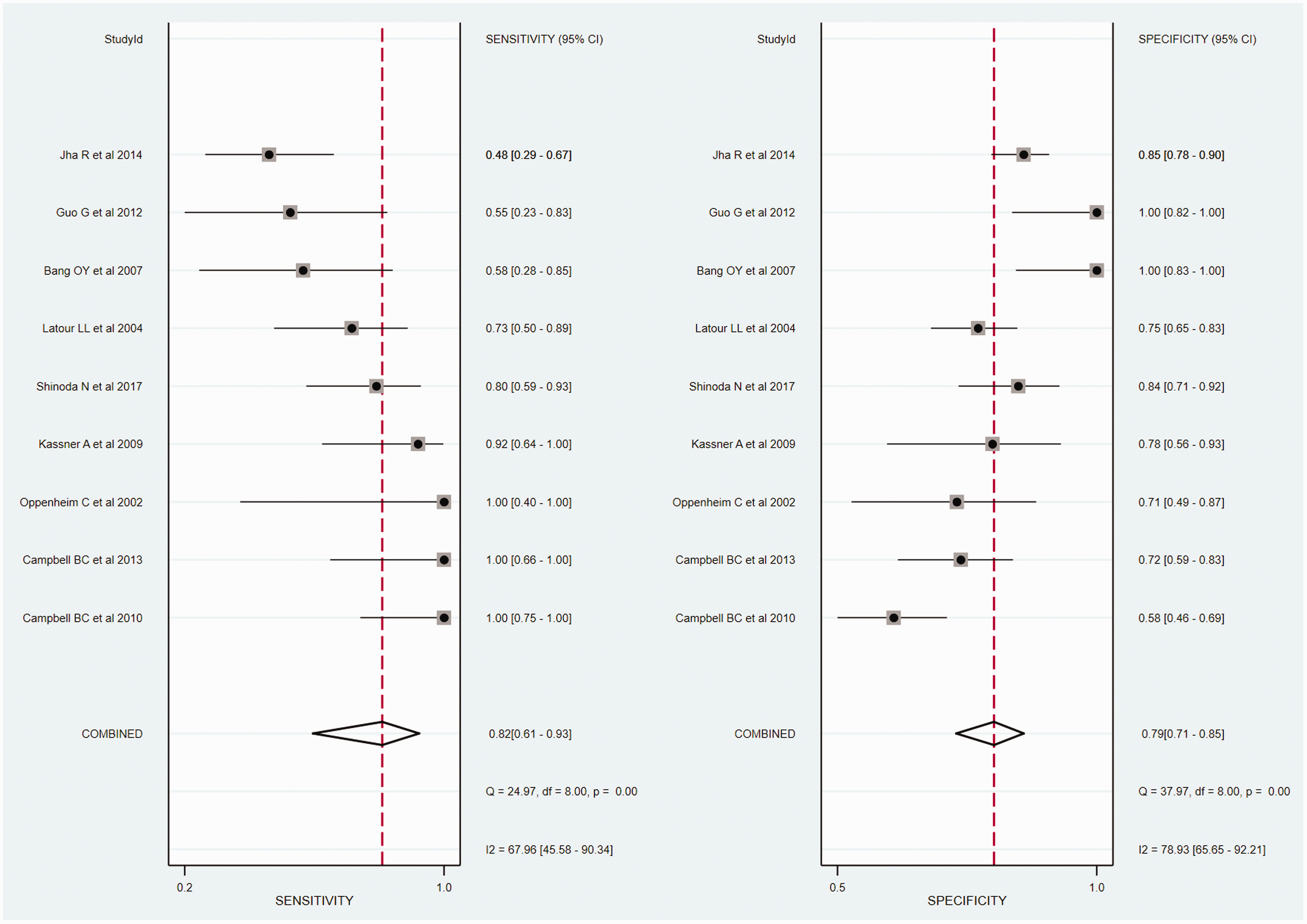
Coupled forest plots of the pooled sensitivity and pooled specificity of MRI for the prediction of hemorrhagic transformation in acute ischemic stroke. Squares indicate pooled estimates and horizontal lines indicate 95% CIs.
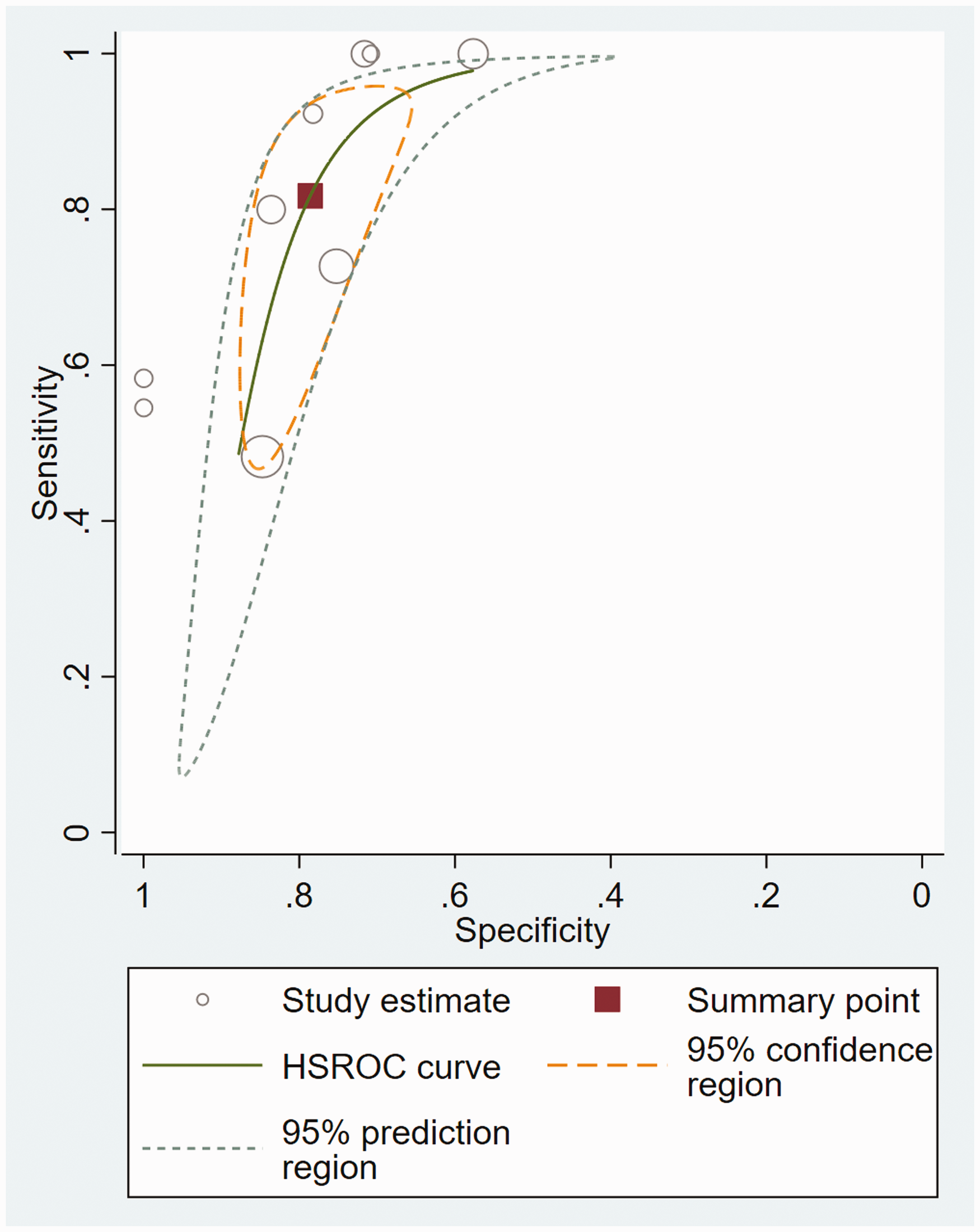
Hierarchical summary receiver operating characteristic curve of the diagnostic performance of MRI for prediction of hemorrhagic transformation in acute ischemic stroke.
The pooled sensitivity and pooled specificity for the diagnostic performance of MRI for prediction of hemorrhagic transformation were 82% (95% CI = 61–93) and 79% (95% CI = 71–85; Fig. 2), respectively. The DOR was 16 (95% CI = 7–37) and the area under the HSROC curve was 0.85 (95% CI = 0.82–0.88; Fig. 3). The Deeks’ funnel plot demonstrated a high possibility of publication bias (P = 0.02; Suppl. Fig. 2).
Subgroup analysis
Six studies used advanced MRI for the diagnosis of hemorrhagic transformation in acute ischemic stroke (5–7,10,12,13). The subgroup analysis of these six studies showed a sensitivity of 92% (95% CI = 70–98) and a specificity of 78% (95% CI = 65–87), with the area under the HSROC curve being 0.90 (95% CI = 0.87–0.93). Heterogeneity in the sensitivity (I2 = 60.57%) and specificity (I2 = 76.16%) was lower than for the total nine studies. Four studies using PWI parameters showed a sensitivity of 92% (95% CI = 80–100) and a specificity of 80% (95% CI = 64–95) (5–7,10). Three studies using conventional MRI parameters showed a sensitivity of 57% (95% CI = 27–86) and a specificity of 85% (95% CI = 72–98) (8,9,11).
Three studies used MRI for the diagnosis of symptomatic hemorrhagic transformation in acute ischemic stroke (5,7,12). The subgroup analysis of these three studies showed sensitivity of 96% (95% CI = 84–100) and specificity of 81% (95% CI = 66–96).
Discussion
Our study revealed that hemorrhagic transformation is associated with high permeability, hypoperfusion, low ADC, and FLAIR hyperintensity. MRI showed a moderate diagnostic performance in the prediction of hemorrhagic transformation in acute ischemic stroke, with a pooled sensitivity of 82% (95% CI = 61–93) and a pooled specificity that was also 79% (95% CI =71–85). Although study heterogeneity was present, a threshold effect was confirmed. In the subgroup analysis, studies using advanced MRI showed sensitivity of 92% (95% CI = 70–98) and specificity of 78% (95% CI = 65–87). MRI may show moderate diagnostic performance for predicting hemorrhage in acute ischemic stroke although the clinical significance of this hemorrhage is somewhat uncertain.
Although hemorrhagic transformation may significantly affect the prognosis in patients with acute ischemic stroke (1), the exact pathophysiology of hemorrhagic transformation is still unclear (13). Disruption of the blood–brain barrier is suggested as one of the possible mechanisms of hemorrhagic transformation. Cerebral endothelial cells are known to be more resistant to ischemic insult than neurons or glia (24). Loss of blood–brain barrier integrity implies that severe ischemic insult has occurred in a region, resulting in the increased likelihood of full vessel-wall failure (5). Disruption of the blood–brain barrier may be an essential condition for hemorrhagic transformation. Multiple MRI techniques are based on this concept of disruption of the blood–brain barrier.
Our study demonstrates that high blood–brain barrier permeability and low CBV derived from PWI are associated with hemorrhagic transformation. Blood–brain barrier permeability imaging has been introduced for the prediction of hemorrhagic transformation in acute ischemic stroke, including recent examples of perfusion CT (25–28). Although perfusion CT is a fast and widely available modality, MRI PWI offers several advantages, including a high contrast-to-noise ratio, the ability to capture the entire spectrum of acute ischemic stroke from multiple small foci to the larger vascular territory, and no ionizing radiation. In terms of hypoperfusion, it has been postulated that hemorrhagic transformation is a consequence of severe ischemic damage to vessel walls, damage which then proceeds to blood–brain barrier disruption and leakage (29). In connection with this, the value of DWI for evaluating the degree of ischemia is well known, and our study demonstrated that low ADC values were associated with hemorrhagic transformation (12,13).
For conventional MRI, all the studies used FLAIR hyperintensity as an indication of hemorrhagic transformation (8,9,11). FLAIR hyperintensity might be a consequence of net increased water content in pathological tissue following severe ischemia, cytotoxic edema, or increased blood–brain barrier permeability (30,31). We found that studies using conventional MRI showed a relatively low sensitivity (48–73%), while, in contrast, advanced MRI revealed a sensitivity of 92% and a specificity of 79% for predicting hemorrhagic transformation. Therefore, advanced MRI techniques should be used to determine the presence of hemorrhagic transformation.
A previous meta-analysis demonstrated that presence of cerebral microbleeds and high cerebral microbleeds burden on pretreatment MRI were independently associated with symptomatic intracerebral hemorrhage in patients with acute ischemic stroke treated with intravenous thrombolysis (32). Another study reported that microbleeds on susceptibility-weighted imaging (SWI) showed a significant association with hemorrhagic transformation (33). Therefore, hemorrhagic transformation is also probably associated with the presence of cerebral microbleed and high cerebral microbleeds burden.
Recently, several studies have used a classifier-based framework or machine learning to predict hemorrhagic transformation in acute ischemic stroke (34,35). Scalzo et al. exploited a classifier-based framework to automatically identify predictive patterns in permeability maps and demonstrated an average accuracy > 85% (34). Yu et al. developed machine learning models to predict the spatial occurrence of hemorrhagic transformation on PWI and DWI, and found that a kernel spectral regression model showed an accuracy of 84% (35). These models should be validated using a larger dataset.
Several limitations to this study are of note. First, the number of included studies is small. Second, heterogeneity was present in both the sensitivity (I2 = 67.96%) and specificity (I2 = 78.93%), while the presence of a threshold effect was observable on visual assessment of the coupled forest plot and indicated by the Spearman correlation coefficient between the sensitivity and false-positive rate (0. 831, 95% CI = 0.372–0.963). This threshold effect was one of the causes of the heterogeneity, but although it may have explained a large portion of the study heterogeneity, some remained unexplained. It has been postulated that one of the possible reasons for heterogeneity across MRI studies is variation in MRI techniques and corresponding parameters. If MRI were to be used to determine the risk of hemorrhagic transformation in clinical trials, standardization of MRI techniques, especially for quantitative analysis, and development of imaging biomarkers and determination of the optimal cut-off values for predicting hemorrhagic transformation would be paramount. Third, publication bias was noted among the included studies (P = 0.02). This publication bias may be related to the fact that studies with more positive results are more likely to be published. Therefore, it is possible that the diagnostic performance of MRI for predicting hemorrhagic transformation may have been overestimated. Caution is required when applying these results to daily clinical practice. Fourth, there was no adjustment for confounders because we could not obtain individual patient data.
In conclusion, hemorrhagic transformation is associated with high permeability, hypoperfusion, low ADC, and FLAIR hyperintensity. MRI may show moderate diagnostic performance for predicting hemorrhage in acute ischemic stroke although the clinical significance of this hemorrhage is somewhat uncertain.
Supplemental Material
ACR887593 Supplemetal Material1 - Supplemental material for MRI for prediction of hemorrhagic transformation in acute ischemic stroke: a systematic review and meta-analysis
Supplemental material, ACR887593 Supplemetal Material1 for MRI for prediction of hemorrhagic transformation in acute ischemic stroke: a systematic review and meta-analysis by Chong Hyun Suh, Seung Chai Jung, Se Jin Cho, Dong-Cheol Woo, Woo Yong Oh, Jong Gu Lee and Kyung Won Kim in Acta Radiologica
Supplemental Material
ACR887593 Supplemetal Material2 - Supplemental material for MRI for prediction of hemorrhagic transformation in acute ischemic stroke: a systematic review and meta-analysis
Supplemental material, ACR887593 Supplemetal Material2 for MRI for prediction of hemorrhagic transformation in acute ischemic stroke: a systematic review and meta-analysis by Chong Hyun Suh, Seung Chai Jung, Se Jin Cho, Dong-Cheol Woo, Woo Yong Oh, Jong Gu Lee and Kyung Won Kim in Acta Radiologica
Supplemental Material
ACR887593 Supplemetal Material3 - Supplemental material for MRI for prediction of hemorrhagic transformation in acute ischemic stroke: a systematic review and meta-analysis
Supplemental material, ACR887593 Supplemetal Material3 for MRI for prediction of hemorrhagic transformation in acute ischemic stroke: a systematic review and meta-analysis by Chong Hyun Suh, Seung Chai Jung, Se Jin Cho, Dong-Cheol Woo, Woo Yong Oh, Jong Gu Lee and Kyung Won Kim in Acta Radiologica
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was supported by a grant from the Ministry of Food and Drug Safety in 2018 (No. 18182MFDS402).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.