
Abstract
Background
The anatomical features of the thoracic nerve roots in connection with intervertebral discs may prevent surgery-related complications and improve patients’ neurological functional status during thoracic spine surgery. There is limited literature evidence regarding this concept using cadavers.
Purpose
To elucidate the qualitative anatomical features of the thoracic nerve roots in connection with intervertebral discs.
Material and Methods
Fifteen formalin-preserved spine specimens were used in this study. Small pieces of stainless-steel wires were placed along the root sleeves from their points of origin, after exposing the dural sac and bilateral nerve roots. The standard anteroposterior and lateral radiographs were taken after the placement of the wires. Measurements were done on radiographs using the picture archiving communication system.
Results
Take-off angles of the nerve roots at the coronal plane gradually increased from the level of T2 (36.1°±2.72°) to T9 (84.1°±1.84°) and from T9, it decreased to T12 (46.3° ± 2.67°). Similar variation tendency was discovered in take-off angles of the nerve roots at the sagittal plane. No consistent tendency was found both in the distance from the origin of the root sleeve to its superior and inferior vertebral endplate. Distance from the origin of the root sleeve to the posterior midline (DM) exponentially decreased from T1 (8.2 ± 0.87 mm) to T4 (6.0 ± 0.93 mm). It slowly increased from T5 (5.5 ± 0.68 mm) to T12 (10.9 ± 1.79 mm), with T5 having the smallest DM. Distance between the origins of neighboring nerve roots showed an obvious increase from the T1–T2 interval (23.1 ± 2.22 mm) to T7–T8 interval (30.9 ± 2.68 mm). However, it progressively decreased at the T10–T11 interval (26.0 ± 2.40 mm).
Conclusion
The dimensions of the thoracic nerve roots vary greatly from T1 to T12 intervertebral discs. Sound knowledge of these anatomical features of the thoracic nerve is mandatory for the thoracic spine surgery, especially in the posterolateral approach and transforaminal endoscopic surgery.
Introduction
Thoracic disc herniations (TDH) are relatively rare in comparison with cervical or lumbar disc herniations. They mainly occur between the T8 and L1 intervertebral discs (1,2). Recent studies reported that the incidence of TDH occurs in approximately 12%–37% of the population (3). Surgical treatment is often recommended for patients with radiculopathy or myelopathy symptoms that do not respond to conservative treatments (1,4). Currently, there are three types of surgical approaches used for TDH which include the following: anterior trans-thoracic; lateral; and posterolateral (2,5,6). Due to the advancement of surgical technology, few invasive techniques have been optimized for the management of thoracic disc protrusions. Smaller incisions and precise dissections in surgeries lead to excellent clinical efficacy and acceptable complication rates (7,8). Recently, transforaminal endoscopic thoracic spine surgery was reported as a new surgical approach for the treatment of TDH (9,10). This technique is less invasive, allowing sufficient decompression of the spinal cord. Intra-operative neurological monitoring and intra-operative optical magnification are usually used to enhance the safety of TDH surgery and decrease the surgical complications and mortality rates (2,11). In spite of these strategies being implemented, surgical complications can still occur to some extent, such as vertebral column instability, neurologic injury, and thoracic complications (1,12,13). The bone structure and nerves should be anatomically clear to reduce the occurrence of surgical complications. The anatomical features of the thoracic spine are crucial to ascertain the accurate decompressing areas of lamina and avoid the unnecessary bony resection. A previous study (14) explored the detailed anatomy of the posterior ramus and its branches of the thoracic spinal nerve using cadaver dissections. Leng et al. (15) identified the thoracic anatomic parameters of the spinal roots and dorsal root ganglia; however, they did not study the anatomic relationship between the surrounding structures. A study by Awwad et al. (16) measured the distance of adjacent thoracic spinal nerves and those between the inferior endplate of superior vertebrae and thoracic spinal nerve on MRI scans. Their study was an MRI radiological study; therefore, they did not provide information such as take-off angles of the nerve roots at the coronal (CA), sagittal planes (SA), and so forth. There is limited evidence in the literature concerning the thoracic nerve root and its relationship with adjacent structures on cadavers.
The aim of the present study was to analyze the qualitative anatomical features of the thoracic nerve root in relation to the intervertebral discs. This study also took into consideration the take-off angles of the thoracic nerve root at the coronal and sagittal planes which may provide some guidelines for the TDH surgery especially in the posterolateral approach and transforaminal endoscopic surgery.
Material and Methods
The present study involving human body specimens was approved by the Ethics Committee of our institution and followed the guidelines of the Declaration of Helsinki (17). Informed consent was received from the next of kin of the human cadavers involved in this study.
A selection of 15 formalin-preserved male cadavers (age range = 20–68 years; mean age = 43 years) were used for this study. All specimens with previous surgery or severe deformities were excluded. The cadaveric specimens of the spine were dissected using the prone position and all soft tissues were detached from level T1 to T12. Thereafter, bilateral pedicles were cut by a T saw. The vertebral plate and the spinous process was removed exposing the dural sac and bilateral nerve roots. Small pieces of stainless-steel wires were placed along the root sleeves from their points of origin (Fig. 1). The standard anteroposterior (AP) and lateral radiographs were taken shortly after the placement of wires (Fig. 2). To avoid overlapping of the steel wires, one side of the wires was removed while taking the lateral radiograph. All the radiographs were transmitted to the picture archiving communication system (PACS; INFINITT, Seoul, Republic of Korea) and parameters were measured directly on the AP and lateral radiographs using the PACS. The measurements were listed as follows (Figs. 3 and 4):
Take-off angle of nerve root at the coronal plane (on AP radiograph): angle between midline and the axis of the root sleeve (CA); Intraspinal take-off angle of nerve root at the sagittal plane (on the lateral radiograph): angle between the corresponding posterior vertebral body line and axis of the root sleeve (SA); Distance from the origin of the root sleeve to the posterior midline (DM); Distance from the origin of the root sleeve to its superior (DS) and inferior (DI) vertebral endplate; Root-to-root distance (DR): distance between the origins of neighboring nerve roots at the coronal plane.

Photograph of the specimen. The vertebral plate and the spinous process were removed showing the dural sac and bilateral nerve roots. Small pieces of stainless-steel wires were placed along the root sleeves from their points of origin.
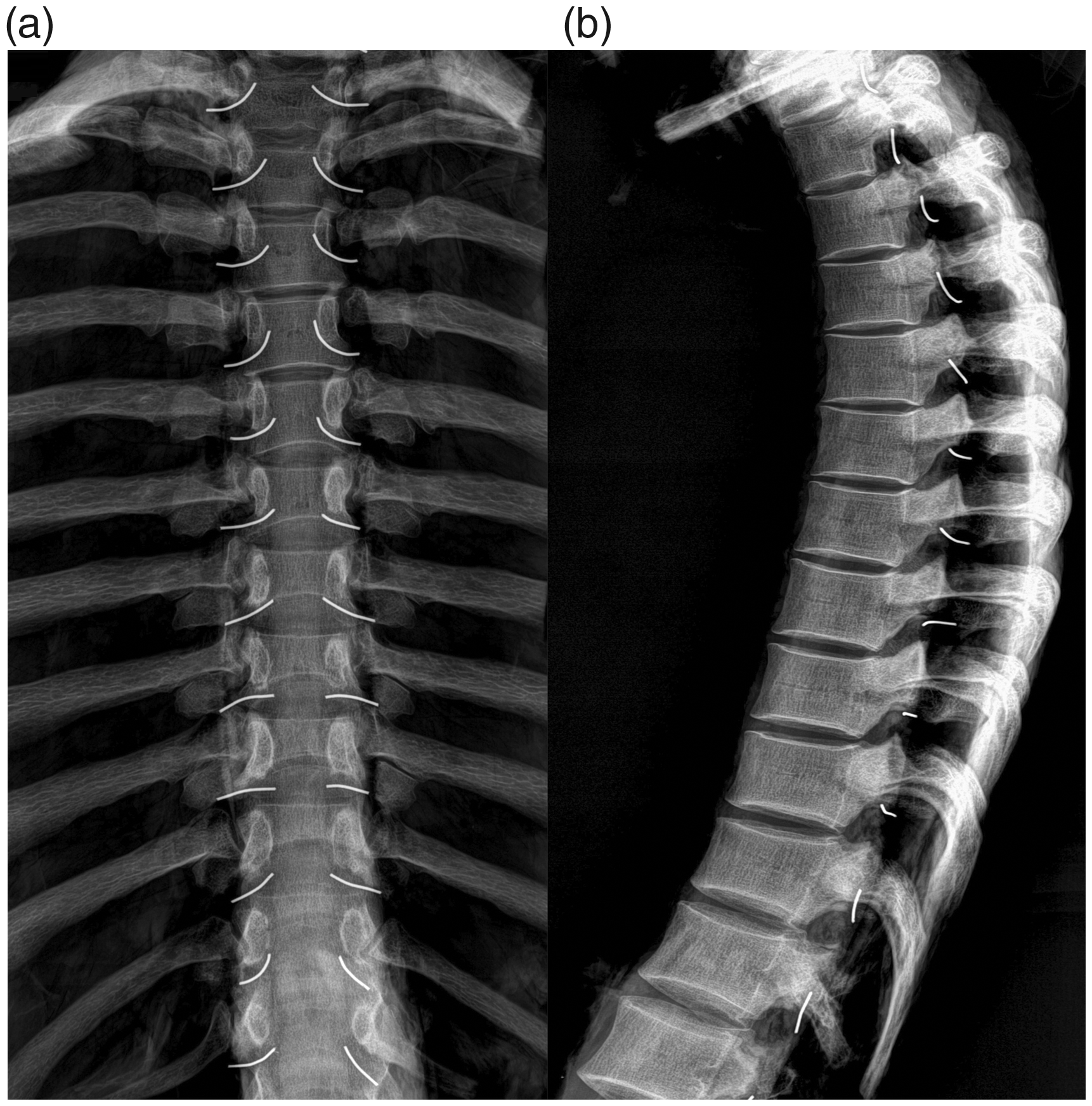
Anteroposterior (a) and lateral radiograph (b) showing the anatomical location of the nerve root, the stainless-steel wire represents the T1–T12 spinal root.
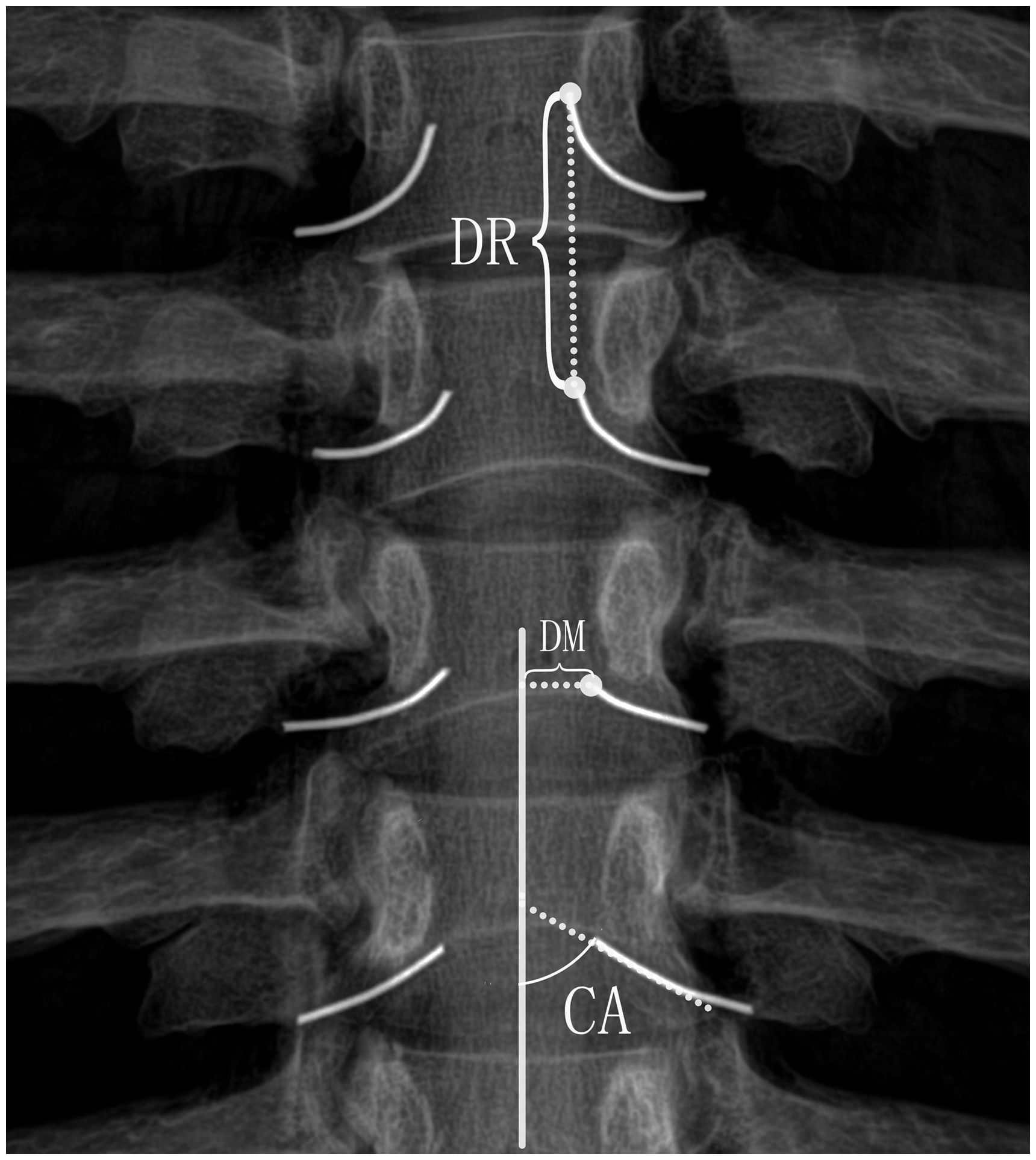
The anteroposterior radiograph showing: (i) the take-off angles of the nerve roots at the coronal plane (CA); (ii) the distance from the origin of the root sleeve to the posterior midline (DM); and (iii) the distance between the origins of neighboring nerve roots (DR).
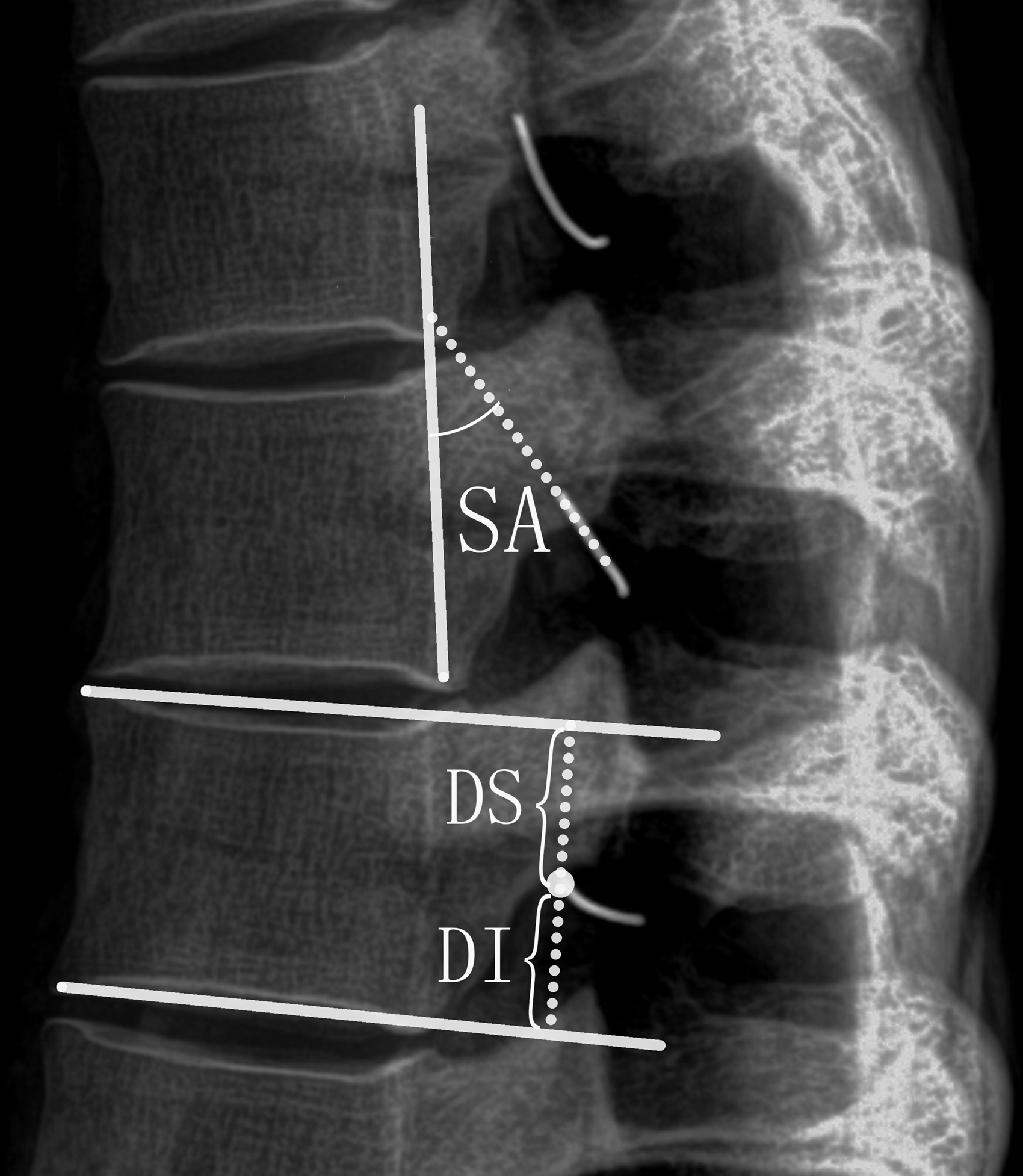
The lateral radiograph showing: (i) the take-off angles of the nerve roots at the sagittal plane (SA); and (ii) the distance from the origin of the root sleeve to its superior (DS) and inferior (DI) vertebral endplate.
All symmetric structures were measured bilaterally. Each parameter was measured by two independent orthopedists. The statistical analysis was done using SPSS software (ver. 19.0; SPSS Inc., Chicago, IL, USA). Paired t-tests were performed comparing mean right-sided with mean left-sided measurements. The level of statistical significance was set to P < 0.05.
Results
There were no statistically significant differences in right-sided versus left-sided measurements for any of the anatomical parameters (P > 0.05). Therefore, we pooled the right-sided and left-sided data together. The results of the measurements are shown in Tables 1 and 2.
Pooled right-sided and left-sided data for CA, SA, DS, DI, and DM.

Values are given as mean ± SD.
*The nerve root is on the left of corresponding posterior cortical plate of the lamina.
CA, take-off angle of nerve root at the coronal plane; DI, distance from the origin of the root sleeve to the its inferior vertebral endplate; DM, distance from the origin of the root sleeve to the posterior midline; DS, distance from the origin of the root sleeve to its superior vertebral endplate; SA, intraspinal take-off angle of nerve root at the sagittal plane.
Distance between the origins of neighboring nerve roots (DR).
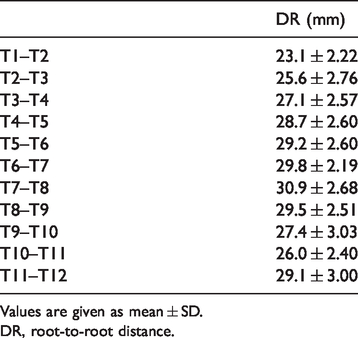
Values are given as mean ± SD.
DR, root-to-root distance.
Take-off angle of the nerve root
From the level of T2 to T9, the CA gradually increased from 36.1° ± 2.72° to 84.1° ± 1.84°, and then decreased to 46.3° ± 2.67° from the level of T9 to T12 discs. The largest angle of CA was found at the level of the T9 disc (84.1° ± 1.84°). A similar variation tendency was also discovered in SA whereas the nerve roots of T1 and T2 were on the left of corresponding posterior cortical plate of the lamina, with T9 (100.4° ± 2.98°) having the largest angle.
Distance from the origin of the root sleeve to the corresponding and lower vertebral endplate
There was no consistent change in either DS or DI measurements. The greatest distance of DS and DI was 16.2 ± 2.65 mm at T9 and 16.39 ± 2.47 mm at T4, respectively, while the smallest distance was found at T4 (8.0 ± 1.78 mm) and T1 (7.8 ± 1.57 mm), respectively.
Distance from the origin of the root sleeve to the posterior midline
There was no consistent variation of DM found from the level of T1 to T12. But DM gradually decreased from 8.2 ± 0.87 mm at T1 to 6.0 ± 0.93 mm at T4. However, it progressively increased from 5.5 ± 0.68 mm at T5 to 10.9 ± 1.79 mm at T12, with T5 having the smallest DM.
Root-to-root distance
The DR showed a significant increase from the T1–T2 interval (23.1 ± 2.22 mm) to the T7–T8 interval (30.9 ± 2.68 mm) and then progressively decreased to 26.0 ± 2.40 mm at the T10–T11 interval. The DR of the T11–T12 interval was 29.1 ± 3.00 mm.
Discussion
Transforaminal endoscopic thoracic spine surgery is less invasive and safe because it involves the removal of a small, lateral part of the facet joint rather than resection of the unilateral facet joint and the caudal pedicle (9,10,18). This technique is currently used in many hospitals across the world. Epidural hematoma and deterioration of nerve roots/spinal cord are some of the rare postoperative complications that come with this method of surgery (19–22). A study by Sivakumaran et al. (23) reported 24 cases with TDH treated by trans-facet approach discectomy with two patients sustaining a small inadvertent durotomy at the root axilla caused by root traction. Another study by Ruetten et al. (22) showed that the total rate of complications was 19% and the rate of serious complications, such as epidural hematoma and deterioration of myelopathy, was 5.8% during the process of full-endoscopic uniportal decompression in 55 patients with TDH. With the advancement of surgical techniques, it is also necessary to have the knowledge of the anatomical structures of the thoracic nerve root.
Although the anatomy of spinal nerves has gained increased attention in recent years, most published articles were mainly focused on the lumbar spine (24–26). The relationship of origin of the thoracic nerve root to the corresponding disc is vital. Knowledge of the anatomic features of thoracic nerve roots will facilitate the thoracic disc surgery and enable patients’ safety during the surgical procedures.
Analyzing the angulation of the nerve roots to the thecal sac at their origin is necessary in order to judge their mobility during intraoperative retraction. Unfortunately, few studies focused on the exact angulation of the nerve roots in the thoracic spine. A study by Leng et al. (15) measured the CA of thoracic spine, an inconsistent change, with the largest angle at T1 (84.6° ± 24.4°) and the smallest angle at T12 (46.7° ± 10.0°), with no further analysis. However, they managed to measure the angle between the midline of the thecal sac and the axis of the nerve roots directly on cadavers (15). The findings of the present study are inconsistent with theirs because in this study, the take-off angle of nerve root was measured between the corresponding posterior vertebral body line and axis of the root sleeve at the coronal and sagittal plane, respectively, via radiograph. This further revealed the exact relationship of the nerve root to its corresponding disc. From the present study’s results with specific regard to the CA and SA of thoracic nerve root, it was discovered that both features constantly increased from the levels of T2 to T9 and decreased from levels T9 to T12. Another interesting finding was that the direction of thoracic nerve was inclined to go backward, particularly from the levels of T6 to T10. The inclination of the thoracic nerve roots may contribute to its special anatomy. The thoracic nerve moves along the middle of the two ribs, contributing to its specific anatomic route. The findings from the present study may contribute to the comprehension of the orientation of thoracic nerve root in posterolateral direction. Therefore, surgical interventions of posterolateral approaches under transforaminal endoscopic thoracic spine surgery may benefit from this information with specific regards to the anatomy.
DS and DI represent the distance from the origin of the root sleeve to its superior and inferior vertebral endplate. There is a certain distance from the origin of the root sleeve to the exit point of the neuroforamen under each pedicle. In addition, the path from the origin of the root sleeve to the exit point of the neuroforamen under each pedicle is not parallel to its corresponding intervertebral space. Therefore, DS and DI are different from measuring the exit point of the neuroforamen under each pedicle. The DS and DI was not clearly identified because of the overlapping of the lower thoracic lamina and the existence of the physiological curvature of the thoracic spine. This was the reason why it was challenging to view the origin of the root sleeve on the AP radiograph. Instead, its length was measured using the sagittal plane. The results from this study indicated that the origin of the root sleeve seems to be between the adjacent intervertebral disc at the sagittal plane in most specimens. This further identifies the exact position of thoracic nerve root origin. A study by Awwad et al. measured the distance between the origin of the root sleeve and posterior edge of the inferior endplate of the overlying vertebrae (16). Their study showed a progressive increase from T4 to T12, with the longest length at T12 and shortest length at T1 (16). From this study, there was no concordant variation in DS and DI. The present study only estimated the distance from the origin of the root sleeve to its corresponding and lower vertebral endplate, which may attribute to the variation of disc height of the thoracic spine. From their study, the DR constantly increased which is not consistent with this study because of the sectional match and larger measurements recorded (16). This could have been due to the different methods of measurements because their study was based on MRI measurements. From the findings of the present study, it can be proved that DM has the rewarding clinical significance, providing the suitable surgical incision during thoracic spine surgery and avoiding the unnecessary nerve injury.
The strength of this study is that it can be easily reproducible because all the measurements are calculated from scanner radiographs using the computer program which limits unnecessary manual errors. Suh et al. have measured the distance between the origin of the bulge on the dural sac and the origin of the root sleeve on the cadaver, and explained lower root compression symptoms (24). This provided further evidence on the pathophysiology of disc prolapses. Future nerve root studies can derive information from this study or Suh et al.’s study to provide more detailed information about the nerve-root angle, its relationship with the root origins and its connections with the corresponding/inferior discs. In addition, the basic anatomy of thoracic spinal nerves could help avoid unnecessary tissue resection and save operating time; more importantly, help avoid surgical complication and ensure patients’ safety during thoracic spine surgery, especially in the posterolateral approach and transforaminal endoscopic surgery.
This study has several limitations. First, the use of formalin-preserved cadavers which are different from fresh cadavers further influencing the results (24). Further studies might attempt to use fresh cadavers using similar methods from this study. Second, the sample size was small and the cadavers were all male. Though Xu et al. (27) and Scoles et al. (28) have demonstrated that most of the parameters of the spine showed no significant difference between male and female, gender-based differences still need to be considered in future studies.
In conclusion, this study concludes that the dimensions of the thoracic nerve roots vary greatly from the level of T1 to T12 intervertebral discs. Sound knowledge of these anatomical features of the thoracic nerve is mandatory for the thoracic spine surgery especially in the posterolateral approach and transforaminal endoscopic surgery.
Footnotes
Acknowledgements
The authors thank all their colleagues for their invaluable assistance during the execution of this study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Science and Technology Department of Zhejiang Province (2020358020), and Wenzhou Municipal Science and Technology Bureau (Y20150063).