
Abstract
The modern-day radiologist must be adept at image interpretation, and the one who most successfully leverages new technologies may provide the highest value to patients, clinicians, and trainees. Applications of virtual reality (VR) and augmented reality (AR) have the potential to revolutionize how imaging information is applied in clinical practice and how radiologists practice. This review provides an overview of VR and AR, highlights current applications, future developments, and limitations hindering adoption.
Keywords
Introduction
Applications of virtual reality (VR) and augmented reality (AR) have the potential to revolutionize how imaging information is applied in clinical practice and how radiologists practice (1,2). In this review, we performed a targeted literature search (PubMed, Google Scholar) related to use of AR and VR in medicine, medical education, and radiology. References within manuscripts including other manuscripts and news media are included. Articles containing specific interventions were prioritized by study quality and publication date. This review provides an overview of VR and AR, highlights current applications, future developments, and limitations hindering adoption.
Definition of VR and AR
Both VR and AR, although distinct from each other, refer to simulations in which virtual elements are used to replace or supplement native sensory input. VR is an immersive simulation which creates the perception of being present within a non-physical virtual world. This is typically accomplished with a head-mounted display (HMD) in which a user receives sensory input from the display rather than their native surroundings (3). AR differs from VR in that the real world is not eliminated from the user’s view. Instead, virtual objects are superimposed onto the real world through a HMD or other display system, so that the user is able to interact simultaneously with the real world as well as with virtual objects (3–5). Users may interact with graphics and virtual objects through the use of voice commands, hand gestures, or with a controller (3,6).
Technology development
VR and AR concepts have existed for several decades. Perhaps the earliest application of virtual reality was pioneered by cinematographer Morton Heilig, who in 1962 designed and patented a “sensorama,” a wide-angled video booth in which viewers were able to watch a film while having their sensory systems engaged through the use of fans, odor-emitters, stereoscopic sound, and motional chairs (7). An early version of the HMD, attached to large sensors and a mechanical arm suspended from the ceiling, was later developed by Ivan Sutherland in 1968 (8).
VR and AR applications were initially costly and had limited capabilities (9). However, advances in technology, such as decreased costs of smartphone display technology, graphics processing, and motion tracking (3), have led to a boom of VR and AR gaming applications and a renewed interest in medical imaging applications. The “miniaturization” of technology has resulted in the development of high-performance wireless HMDs (10). Immersive reality has been further popularized by increased web connectivity and open source software, which has facilitated exploration, collaboration, and development of VR and AR applications. Such advances have enabled innumerable applications within medicine, including in medical education, procedural planning, and therapeutic intervention. Total spending in VR and AR is expected to rise dramatically, from $11.4 billion in 2017 to nearly $215 billion in 2021, with spending in healthcare applications projected to reach $5.1 billion in 2025 (11,12).
Current and future applications
Alternative to 3D printing
In the last decade, physicians have increasingly utilized 3D-printing technology, in which reconstructions are printed into models that can be interactively explored (13,14). Use of 3D-printed models has improved procedural planning (15–32), medical research, and medical education (26,33–37). Despite the benefits of 3D printing, there are several limitations which hinder its widespread adoption, including cost, turnaround time, and size constraints of printed models (14). VR and AR technologies provide several advantages over 3D printing (Table 1). Reconstructions can be generated at comparatively low costs and turnaround times. Specialized software allows models to be viewed at different sizes and manipulated in dynamic ways that may improve an understanding of complex anatomy (Fig. 1). The ease of use, lower cost, shorter turnaround time, and customizability are appealing features of VR and AR that can supplement or substitute 3D printing in specific applications (38). While controlled data comparing the two modalities are limited, some studies report advantages over 3D printing. For example, when evaluating cerebrovascular anatomy for neurosurgical training, users reported greater resolution and educational potential with VR over 3D printing (39).
Comparison between 3D printing to VR and AR.*
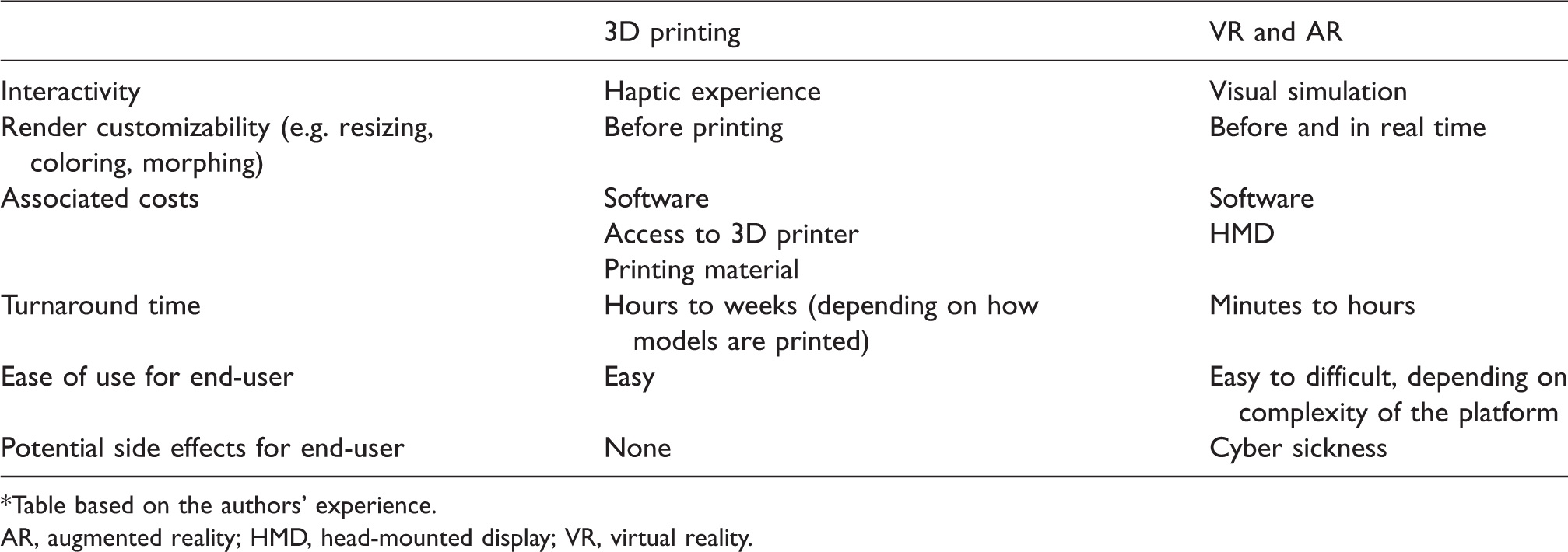
*Table based on the authors’ experience.
AR, augmented reality; HMD, head-mounted display; VR, virtual reality.
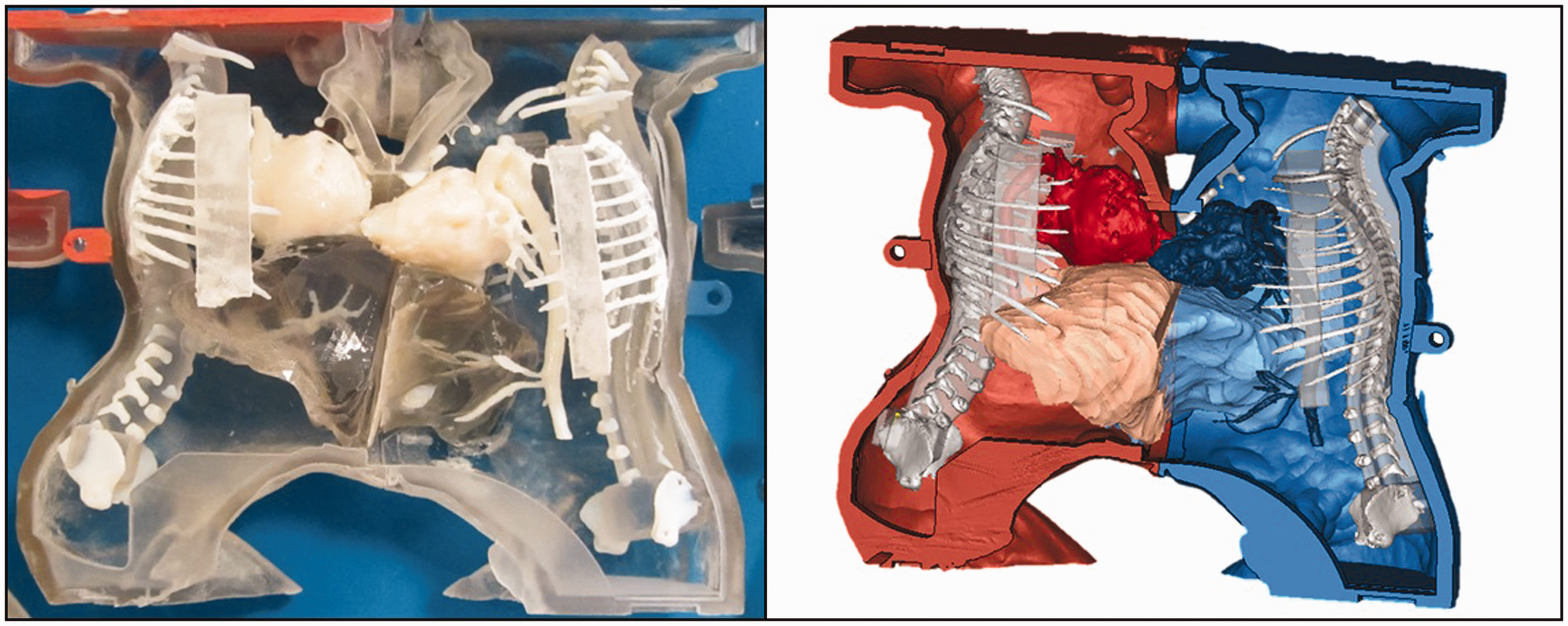
3D-printed model and virtual reconstruction of conjoined twins for surgical planning.
Diagnosis and surgical planning
VR and AR can aid in the understanding of complex anatomical relationships. For example, AR models of kidneys have been generated for surgical planning and decision-making before robotic-assisted partial nephrectomy (40). In the setting of camera-assisted surgery in which the operator is limited by the endoscope’s internal field of view, AR applications can transpose the endoscopic view onto the patient, aiding the surgeon’s ability to navigate (41). Successful use of this technology has been described for nephrectomy, nephrolithotomy, adrenalectomy, brain tumor resection, cerebral aneurysm clipping, splenectomy, and abdominal tumor resection (42–53). In mammography, viewing images of the breast in AR allows for stereoscopic depth perception, 3D cursor use, and joystick navigation (54,55). Joystick navigation involves the use of a handheld controller, which can be used to “fly” throughout an image to better visualize target areas. These tools may ultimately improve detection and localization of abnormal microcalcifications and tumors (54,55). VR reconstructions of the breast have also been introduced for the assessment of tumor response after neoadjuvant chemotherapy and for aiding in surgical planning (55,56).
Interventional radiology
VR and AR have the potential to revolutionize image-guided interventions and improve patient outcomes. Real-time AR reconstructions superimposed onto patients for percutaneous and endovascular interventions may provide benefits over conventional localization techniques. A pilot study showed that viewing VR reconstructions of splenic artery aneurysms before endovascular embolization improved operator confidence (57). In one model, AR reconstructions of the aorta and its major branches were transposed onto a phantom and, with the use of electromagnetic markers, an endovascular catheter was tracked within the virtually generated vascular tree (58). This type of application could theoretically reduce procedure time and radiation exposure (58). AR also has growing promise in percutaneous interventions, such as biopsies and ablations (59). Although there are challenges associated with patient movement and image mismatch when using AR, advances in image reconstruction have significantly improved accurate lesion localization with AR, achieving a difference of <5 mm between virtual and real distances (60). Currently, however, studies evaluating objective benefits of AR over conventional localization techniques in interventional radiology (such as “road-mapping with fluoroscopy”) are limited and will require more robust research than “proof-of-concept” demonstrations to validate clinical utility.
The reading room
Attempts are underway to redesign the conventional reading room with virtual reality. Typical reading rooms require highly specialized equipment and specific lighting conditions to ensure accurate image interpretation. A novel virtual reality reading room has been introduced, where images can be interpreted using a commercially available HMD (61). Optimal image conditions can be reconstructed in a virtual environment, precluding the need for controlled external lighting conditions and specialized monitors (61). In this specific application, image navigation is performed with the use of hand gestures, which allows for dynamic visualization, such as real-time object rotation and tilting. Users found the platform to have sufficient ease of use and interpretability without reporting any discomfort (61). Use of VR reading rooms could cut equipment and maintenance costs, and by eliminating effects of ambient lighting conditions could potentially improve diagnostic accuracy.
Relaxation/Distraction therapy
Distraction or relaxation therapies aim to reduce patient pain and anxiety by using sensory stimuli in lieu of pharmacological substances. Common distraction methods include listening to music or viewing scenes on a standard digital screen (62–64). A distinct benefit of using VR for distraction/relaxation therapy is due to its completely immersive nature. Multiple studies have shown that VR can help reduce the use of sedation during MR imaging (65–67). VR has also benefited pediatric patients aged 4–6 years by decreasing pain and anxiety during dental procedures (68), intravenous line placement (69), and other procedural interventions (70). In adult burn victims, the use of VR distraction therapy during dressing changes reduced pain, anxiety, and length of hospitalization (71). Reductions in pain were more notable with higher quality headsets that covered a wider field of view, suggesting that more immersive VR experiences are more effective (72). In a separate pilot study, VR relaxation therapy was safely used during orthopedic surgery under regional anesthesia (73). Distraction therapy also decreased intravenous sedation and procedure related pain during preoperative adductor canal catheter placement before total knee arthroplasty (74). The efficacy of VR relaxation therapy has been validated by functional magnetic resonance imaging (fMRI) (75). Users exposed to painful thermal stimuli during fMRI scans reported less subjective pain and had statistically significant reductions in pain-related brain activity while using VR relaxation therapy (75). The reported successes of using VR for distraction therapy, during invasive surgical procedures warrants adoption in interventional radiology as well. Patients prone to anxiety, claustrophobia, or high analgesic requirements during interventional radiology procedures may find this therapy especially beneficial.
Informed consent process
Informed consent, generally speaking, is a process of communicating the purposes, risks, and benefits of procedures between a patient and provider (76). There has been a shift toward a more patient-centered model in which visual aids are used in an effort to overcome lower levels of patient health literacy and ultimately achieve a greater sense of autonomy in patients (77). Improving the informed consent process can result in decreased anxiety, higher patient satisfaction, and an improved understanding of procedures (78–80). Part of the consent process is an explanation of the procedure, which could be accomplished by using VR. For example, patients who were primed with what to experience during the recovery process also experienced lower postoperative pain, a shorter length of stay, and less negative affect (81,82). Based on such positive effects, the use of VR to enhance patient education and consent for radiology procedures should be further explored.
Education and training
Advances in diagnostic and interventional radiology have increased the scope of procedures performed by radiologists. Despite the growing breadth of radiology procedures, time constraints in busy clinical services have made it challenging to provide standardized teaching for trainees. Trainees and faculty would favor implementation of standardized procedural training during radiology residency (83), and VR lends itself to creating such curricula. Current simulations based on phantoms do not provide an experience that accurately portrays a live situation, while VR simulations, such as for cardiopulmonary resuscitation, can provide an extremely high fidelity and customizable experience (84). VR and AR simulations may also be used to more accurately assess trainee performance, such as knowledge and skill levels in neurosurgery (1).
Patients may also prefer that trainees undergo procedural training in a simulated environment before performing procedures on patients. By using VR, trainees can be transported into a procedure room where they may observe and even participate in virtual procedures before performing them on patients. This allows educators to provide standardized and curated educational training material to all trainees. In a pilot program implemented by McCarthy et al. (10), radiology faculty and trainees were able to watch interventional radiology tutorials in VR. This program allowed trainees to experience the process of learning with an instructor in a procedure room. The majority of pilot participants reported that the module they watched was excellent or good and had the potential to contribute to the future of interventional radiology training (10). VR can also fill gaps in procedural experience by providing simulations of procedures that a trainee rarely encounters during their graduate medical training (85,86).
Teaching challenging anatomical concepts can be made simpler with VR and AR. 3D reconstructions of images and post-processing software can be used to generate high quality interactive VR and AR simulations. Such simulations will enable the user to manipulate and edit objects in ways that are not possible using other modalities, such as 3D printing (3). For example, virtual reality has been used to teach anatomy to medical students with “virtual dissections” (87).
Advances in HMDs and decreasing costs have enabled the “VR classroom.” For example, teaching modules recorded with specialized 360° cameras can be viewed in VR, which may provide more engagement than conventional teaching methods. Certain applications also enable users to convene in a virtual location (88). This technology can be used to enhance radiology collaboration and education, including in underserved locations. As commercial medical virtual reality applications continue to emerge, new interactive methods to teach radiology will be developed (3).
Overall, the advent of VR simulations in medical education can increase opportunities for providing high-quality standardized educational simulations and assessments at scale, while minimizing the need for dedicated physical space, costly simulation manikins, or need for human cadavers.
Limitations and ethical considerations in VR and AR
One of the most notable side effects of immersive reality is “cyber sickness.” In essence, this describes sensations of discomfort including nausea, headache, and dizziness when using VR and AR applications (89–91). It is posited that cyber sickness is due to vestibular mismatch, in which there is the visual perception of motion in a simulation without matching input from the vestibular system (3). Multiple strategies aimed at reducing cyber sickness have been explored, such as developing VR simulations which only shows movement when there is actual movement of the user’s head (3). Advanced VR HMDs can track nuanced head movements to reduce vestibular mismatch (3). Eye strain may also contribute to discomfort with VR, which can be caused by low frame-rates and HMDs which do not properly accommodate the user’s eyes (3,91). Developers must anticipate potential discomfort with VR and find ways to mitigate unwanted side effects when creating applications.
AR must overcome several limitations to become useful during image-guided procedures. For example, when virtually reconstructed anatomy is transposed over a patient in real time with AR HMDs, the image location must be accurate. Inaccurate localization may result in a less efficient procedure or unnecessary patient harm. Techniques are being developed to optimize AR image reconstruction, including overcoming respiratory motion and organ deformation (60,92–94). In addition to accurate image localization, the device must feel like a “natural extension” of the operator’s senses (95). The image must move smoothly and accurately while the operator’s head position changes. The HMD must also be light, comfortable, and mobile enough for the operator to use during potentially long image-guided interventions (95).
VR and AR technology are still limited with regards to accurately portraying reality. Creating a realistic virtual experience, while feasible using current technology, can require significant time, financial resources, and expertise. Therefore, developing simulations that do not require high levels of accuracy, such as those simulating the performance of simple tasks may provide the highest initial value (86). In addition, more high-quality research is necessary to understand whether VR and AR educational and training applications in radiology provide a significant advantage over conventional methods to justify costs.
Caution should be taken when implementing this technology in medicine. Numerous VR and AR applications have already been cleared by the FDA using the 510(k) pathway, where safety and effectiveness are demonstrated by showing “substantial equivalence” to pre-existing 3D modeling software (96,97). However, more research is required to ensure that the introduction of this technology in specific use-cases confers a benefit to the radiologist workflow and patient care.
Ethical concerns have been raised regarding any unintended consequences when VR and AR supplement or replace existing methods (98). For example, inaccuracies in simulations may contribute to improper training. An analogy to this is flight training of military pilots, where a virtual simulation may not accurately replicate certain scenarios, leading to a distorted perception of real-time flight (98). In addition, trainees may not receive the same level of scrutiny as they would during live interventions, potentially fostering the development of flawed techniques.
As VR and AR technology evolves, thorough consideration should be given on how it is introduced into medicine. Special attention should be placed on major participants and their motivations in this arena. Oversight from a combination of professions including radiologist and non-radiologist physicians, informatics specialists, developers, artists, and other industry professionals are required to adequately test, facilitate, and record changes in this field. Cautious introduction of VR and AR will ensure that it is incorporated in a safe and effective manner.
Conclusion
Advances in VR and AR have enabled novel applications in education, training, and patient care in radiology. We are currently exploring the utility of VR for visualization of complex anatomy and procedural training in interventional radiology. We believe that further exploration and thorough research is warranted to better understand how to best utilize this technology to optimize radiology training and improve patient care.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.