
Abstract
Background
Uterine fibroid embolization (UFE) is an effective treatment for uterine leiomyomata. Optimizing the choice of embolic agents is imperative to achieve better patient outcomes with maximum resource utilization.
Purpose
To evaluate the efficacy and cost-effectiveness of trisacryl gelatin microspheres (TAGM) versus combined TAGM and gelatin sponge (GS) embolization in the treatment of symptomatic uterine leiomyomata.
Material and Methods
Between July 2007 and December 2010, 106 consecutive patients underwent UFE with TAGM. Between January 2011 and December 2016, 123 consecutive patients underwent UFE with a combination of TAGM/GS. The primary outcomes were successful infarction rate (≥90% infarction) of the dominant leiomyoma and percentage reduction in uterine and dominant leiomyoma volume on MRI at six months. Secondary outcomes included adverse event rates, pain scores, and change in clinical symptoms at six months. The embolic agents utilized per procedure were recorded and a cost-effectiveness analysis was performed.
Results
Baseline characteristics of both groups were similar. Successful infarction was achieved in 93.2% of the TAGM group and 94.6% of the TAGM/GS group (P = 0.52). Reduction in uterine volume (TAGM 40.7%, TAGM/GS 44.4%, P = 0.16) and dominant leiomyoma volume (TAGM 47.6%, TAGM/GS 50.1%, P = 0.29) at six months was similar. No significant difference was observed in symptom improvement at six months (P = 0.8). The mean number of TAGM vials utilized and cost per procedure was 6.3 and $1688.40 for TAGM embolization and 3.6 and $979.50 for TAGM/GS embolization, respectively.
Conclusion
Primary and secondary outcomes were comparable when performing UFE with TAGM versus combined TAGM/GS. The combined use of TAGM/GS reduced the mean cost of embolic agents by 42%.
Introduction
Uterine fibroid embolization (UFE) is an effective, minimally invasive treatment strategy for the management of symptomatic uterine leiomyomata supported by an extensive evidence base (1–5).
Excellent results have been achieved using multiple different embolic agents. There is a substantial cost differential for the multiple embolic agents available. A recent meta-analysis demonstrated comparable clinical and radiological outcomes for multiple embolic agents with no single agent demonstrating superior results (6).
It is the responsibility of healthcare practitioners to strive to achieve the best possible outcomes for patients in the setting of optimal resource utilization. An aging population, increased prevalence of chronic diseases, and the rapid pace of healthcare innovation with its associated costs are all significant obstacles to improving healthcare outcomes. In order to tackle this, healthcare systems are shifting toward a value-based model of reimbursement with value defined as health outcomes achieved relative to the associated cost (7).
The study of cost-effectiveness or value in interventional radiology is important as it provides useful data in the development, adoption, and justification of a procedure. Before 2010, UFE was predominantly performed in our institute using trisacryl gelatin microspheres (TAGM) (Embosphere, Merit Medical Inc., South Jordan, UT, USA) as a single embolic agent. TAGM are calibrated microspheres made from microporous cross-linked acrylic beads embedded with gelatin and have been demonstrated to be a highly effective uterine embolic agent (8,9). The economic recession of 2008 had a substantial impact on healthcare funding in our country with a cumulative 27% reduction (€4 billion) in the healthcare budget between 2008 and 2014 (10). This accentuated the need for a review of practices in the UFE program in our institute to try and identify alternative procedural techniques or novel treatment strategies to reduce expenditure and increase value while minimizing the impact on patient care and outcomes. The single costliest element of the UFE procedure in our institute was the embolic agent. Therefore, an approach utilizing a combination of a reduced quantity of TAGM followed by gelatin sponge (GS) (Lyostypt, B. Braun, Rubí, Spain) was introduced as a cost-reduction strategy after initial anecdotal evidence suggested that there was a similar radiological and clinical outcome compared to using TAGM alone. GS is a water-insoluble hemostatic material with biodegradable properties which has been demonstrated as an effective embolic agent in UFE (11–16).
The aim of the present study is to compare the radiological and clinical outcomes of UFE in our institute with TAGM alone versus a combination of TAGM and GS and to perform a cost-effectiveness analysis of the two procedural techniques, focusing on the cost of the embolic agents utilized as the primary difference between the two techniques.
Material and Methods
This was an institutional review board, waived, retrospective, single-institute study to compare the outcomes of UFE with TAGM as a single embolic agent versus combined TAGM and GS particles for the treatment of symptomatic uterine leiomyomata.
Consecutive patients who underwent UFE with TAGM between July 2007 and December 2010 as well as consecutive patients who underwent UFE with combined TAGM and GS between January 2011 and December 2016 were included in the study.
The inclusion criteria included premenopausal patients with symptomatic uterine leiomyomata (menorrhagia, dysmenorrhea, and bulk-related symptoms) who underwent contrast-enhanced magnetic resonance imaging (CE-MRI) before embolization and a subsequent CE-MRI approximately six months after embolization. No limit was applied to patient age or uterine or dominant leiomyoma volume. Exclusion criteria included incomplete imaging, pregnancy, and previous UFE. Patients with perivaginal passage of their leiomyoma after embolization or who underwent myomectomy after embolization were also excluded as this precluded the evaluation of the degree of infarction and changes in leiomyoma volume.
MRI
All patients underwent unenhanced and CE-MRI (Multihance™ [gadobenate dimeglumine], Bracco, High Wycombe, UK) of the pelvis before and six months after embolization on a 1.5-T MRI scanner (Achieva, Philips Medical Systems, Best, the Netherlands) with standard departmental protocols including coronal T2-weighted (T2W) spin echo (TR/TE = 3000/90 ms, slice thickness = 4 mm), sagittal T2W spin echo (TR/TE = 3081/90 ms, slice thickness = 5 mm), sagittal T1-weighted (T1W) spin echo (TR/TE = 598/10 ms, slice thickness = 5 mm), and post-contrast sagittal T1W spin echo (TR/TE = 550/10 ms, slice thickness = 5 mm).
Procedure
Before embolization, patients completed an institute-specific, standardized, departmental questionnaire similar to the uterine fibroid symptom and quality of life questionnaire (UFS-QOL) (17) and were reviewed at the UFE clinic by the lead consultant interventional radiologist to assess for suitability for UFE.
All procedures were performed by three experienced operators with >10 years of experience performing UFE. A standardized technique was utilized for both UFE performed with TAGM and UFE using TAGM/GS as the embolic agent with the two procedures differing only in the administration of embolic agents. A unilateral right femoral artery approach was employed in all cases. An aortogram was performed to evaluate the arterial supply. A variety of 4-Fr and 5-Fr catheters were utilized to sequentially access the orifice of both uterine arteries and a 3-Fr microcatheter was then advanced coaxially into the uterine arteries. In all TAGM and combined TAGM/GS cases, 500–700 μg TAGM microsphere suspensions were administered for the first four vials with 700–900 μg microsphere suspensions administered subsequently as required.
In cases where TAGM was used as the single embolic agent, the endpoint for embolization was near-stasis of flow within the ascending uterine artery for a period of five heartbeats (18). In combined TAGM/GS embolization cases, TAGM was initially utilized until forward flow was reduced within the ascending uterine artery. GS in the form of a slurry was prepared by hand from Lyostypt sheets® manually cut into approximately 1-mm squares and mixed with iodinated contrast (Omnipaque 300) to a volume of 10 mL using two 10-cc syringes connected via a three-way tap. Embolization with GS was performed to achieve stasis of forward flow in the ascending uterine artery for five consecutive heartbeats (18).
Following embolization, all patients were admitted to a post-surgical gynecology unit with a standardized post-UFE management pathway including patient-controlled analgesia (PCA). All patients were admitted overnight following the procedure and were reviewed daily by the interventional radiology consultant and/or fellow who undertook the procedure. Pain scores at 24 h were recorded on a standardized visual analogue scale ranging from 0 (no pain) to 10 (worst pain).
Follow-up
All patients were routinely reviewed in the UFE clinic by the lead consultant interventional radiologist at one and six months after embolization. A transabdominal pelvic ultrasound was performed by the lead consultant interventional radiologist at one month. As above, all patients underwent a repeat unenhanced and contrast-enhanced MRI six months after embolization on the same day as their UFE clinic review. For the purpose of this study, all pre-and post-embolization MRI scans were retrospectively reviewed independently by the lead consultant interventional radiologist performing UFE in our institute and a radiology fellow in their fifth year of training.
Data analysis
Post-contrast T1W imaging was used to identify the dominant enhancing leiomyoma. The volume of the uterus and dominant leiomyoma were calculated before and after embolization using the formula for a prolate ellipse: craniocaudal × anteroposterior × transverse dimension × 0.5233 (Fig. 1). The percentage infarction was estimated on post-procedure MRI by measuring and subtracting the volume of perfusing non-infarcted tissue from the volume of the entire leiomyoma (Fig. 2). When residual enhancement was patchy or irregular in shape, the percentage infarction was estimated by visual assessment to the nearest percentage. Differences in recorded infarction rates between the two readers were resolved by consensus in a subsequent discussion.
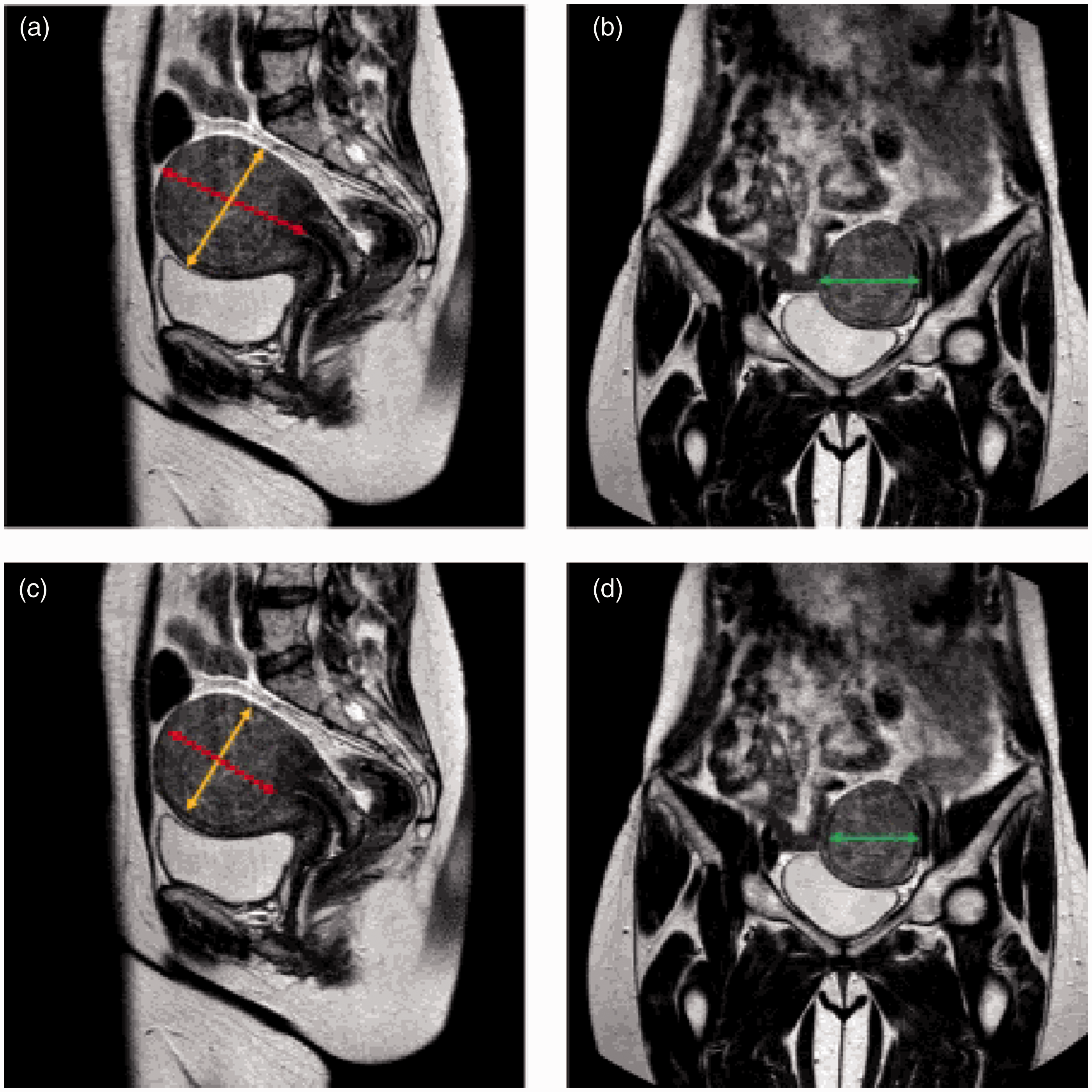
Calculating uterine (a, b) and dominant (c, d) leiomyoma volume.
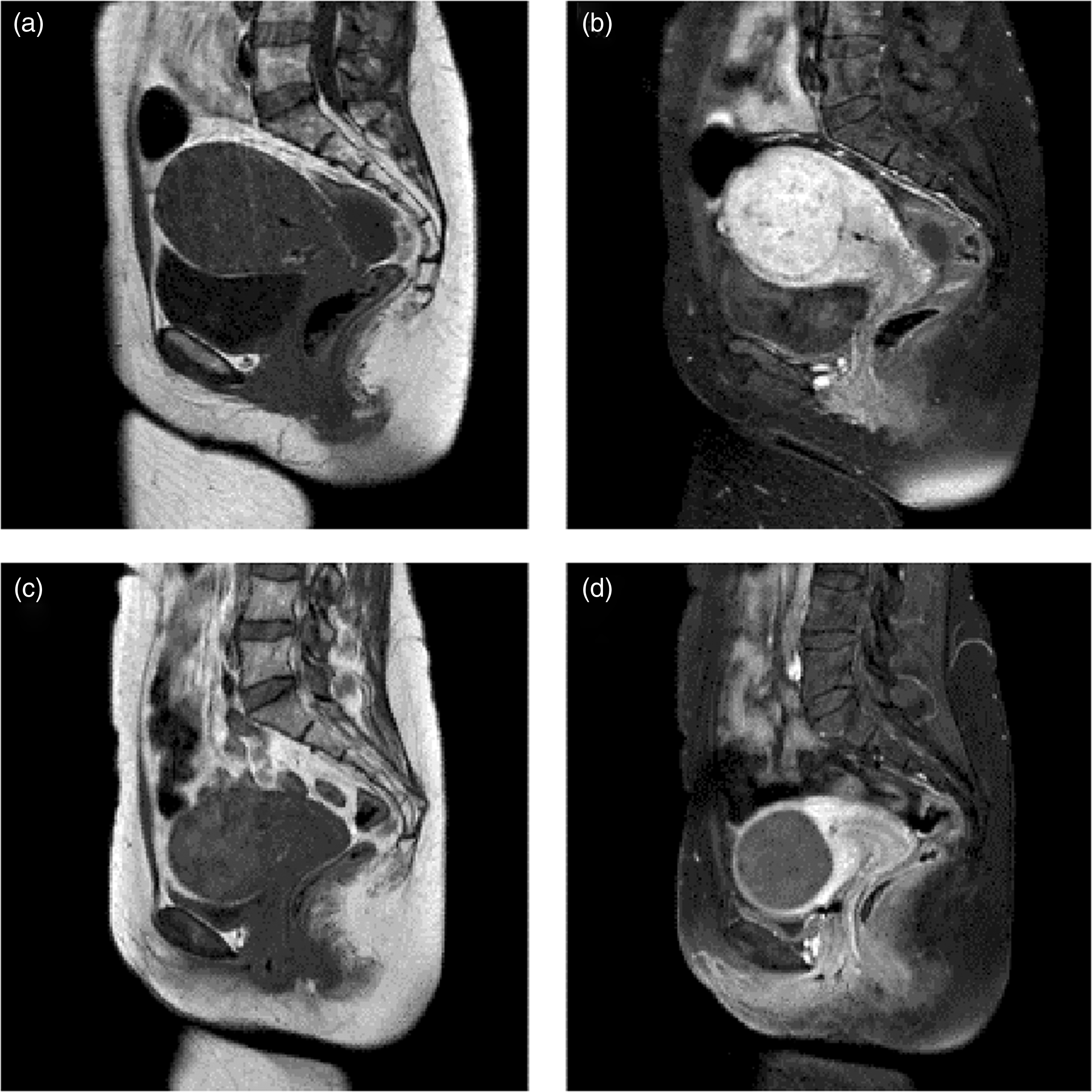
(a, b) Pre- and post-contrast sagittal T1W imaging before embolization demonstrating an enhancing dominant leiomyoma. (c, d) Pre- and post-contrast sagittal T1W imaging six months after embolization demonstrating non-perfusion of the dominant leiomyoma consistent with 100% infarction.
Patient demographics were recorded from the hospital’s electronic patient record. Clinical information was collected from an institute-specific standardized proforma completed by each patient at a UFE clinic before undergoing embolization. Details recorded include medical and gynecological history as well as baseline symptoms. Post-procedure clinical outcomes were collected from the records of post-procedure UFE clinic reviews performed at one and six months. A moderate to complete resolution of leiomyoma-related symptoms was considered a clinical success.
Adverse events (AE) were evaluated from procedural reports, electronic patient records, and routine post-procedure follow-up clinical reviews. These sources are a limitation for AE recording in this study, in particular for mild AE, as they rely on patient reporting and recall of AE up to six months after the procedure.
Length of stay was recorded from the electronic patient records.
Study outcomes
Primary outcomes included the rate of successful infarction of the dominant leiomyoma defined as ≥90% infarction of the dominant leiomyoma on CE-MRI performed six months after embolization as well as reduction in uterine volume and reduction in volume of the dominant leiomyoma at six months after embolization. Secondary outcomes included rates of AEs and clinical outcomes measured on a standardized departmental questionnaire. AE were graded using the Society of Interventional Radiology (SIR) classification (19).
Statistical methods
Statistical analyses were performed with GraphPad Prism 7.03 (GraphPad software, Inc.). The Student’s t-test was used for the comparison of continuous variables with the results presented as mean ± SD. Fisher’s exact test was used for the comparison of discrete variables with the results presented as counts and percentages. Pain scores at 24 h were compared using the Mann–Whitney test. A P value <0.05 was considered significant.
Results
A total of 158 patients underwent UFE with TAGM between July 2006 and December 2010. Of these, 52 were excluded (Fig. 3). Seven patients underwent UFE before elective myomectomy. A total of 155 patients underwent UFE with TAGM/GS between January 2011 and December 2016; 32 were excluded (Fig. 4). In total, 239 patients were included between the two patient groups.
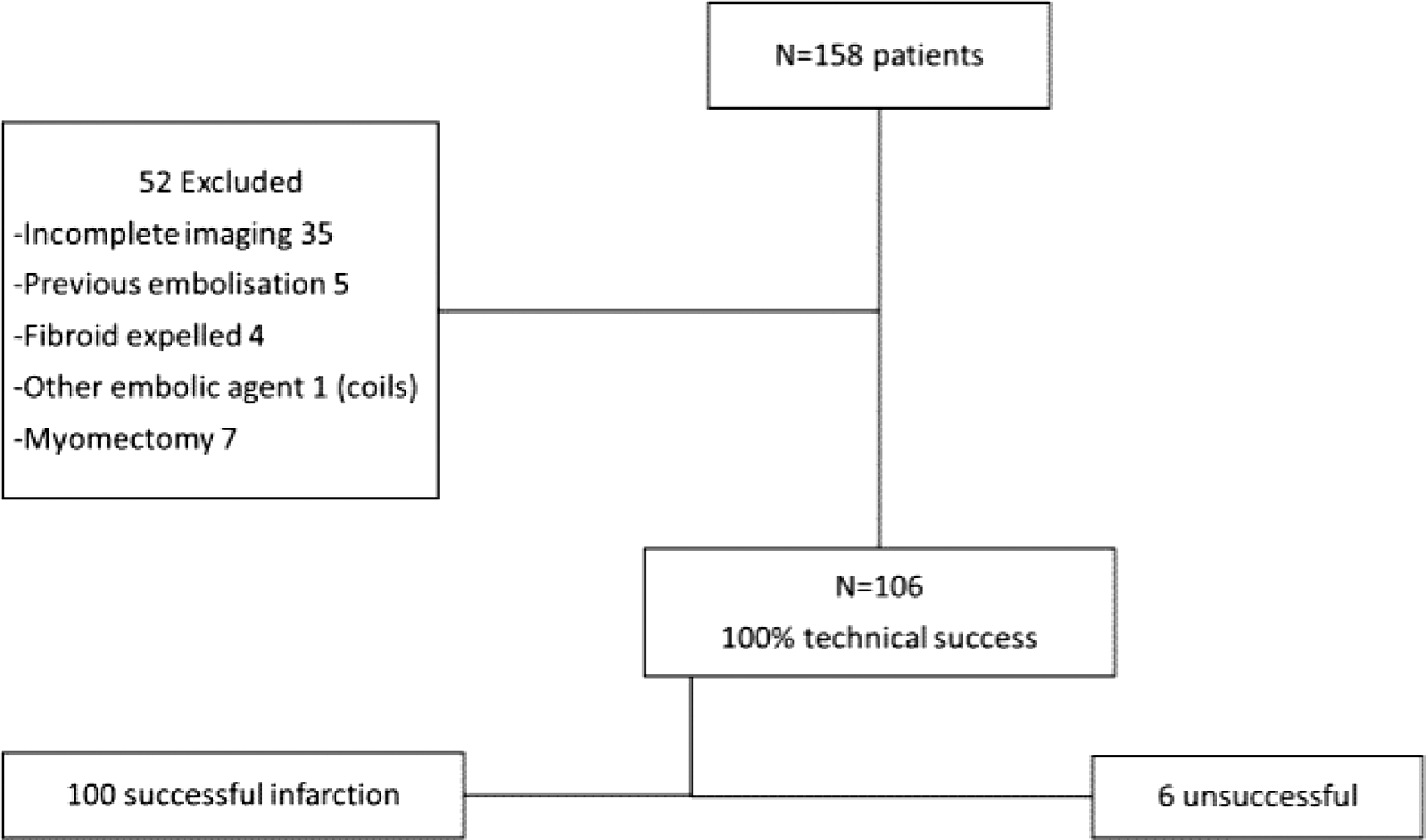
Consecutive patients undergoing UFE between July 2007 and December 2010 with TAGM as the embolic agent utilized.
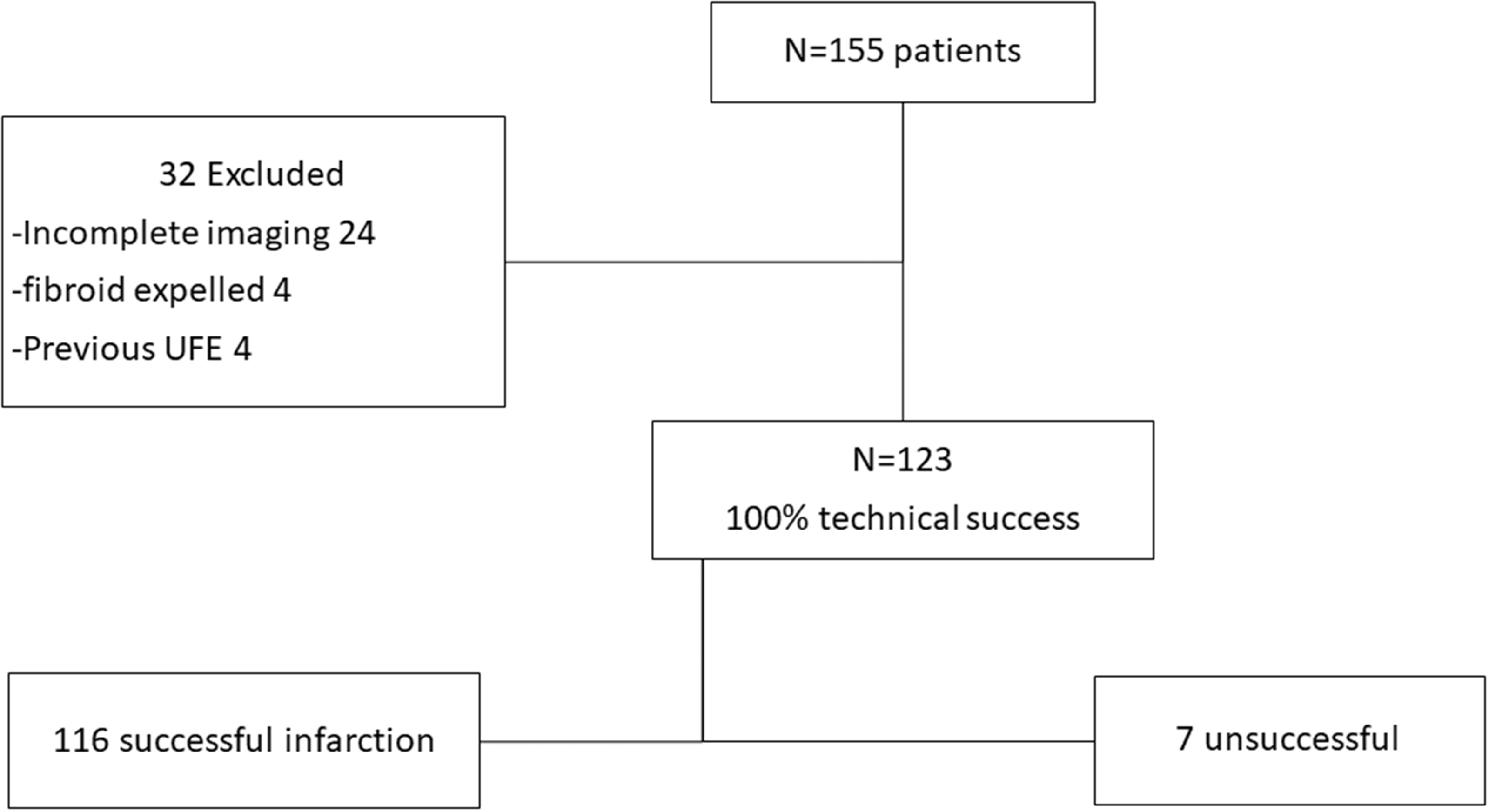
Consecutive patients undergoing UFE between January 2012 and December 2016 with combined TAGM and GS as the embolic agents utilized.
The baseline characteristics of the two groups were similar with no significant difference (Table 1). No difference was recorded in baseline uterine and dominant leiomyoma volume (Table 2). Mean reduction in uterine and dominant leiomyoma volume were similar between the two groups (Table 2). Both techniques achieved comparable radiological outcomes in terms of successful infarction (≥90%) of the dominant leiomyoma with no significant difference (Table 3).
Baseline characteristics.
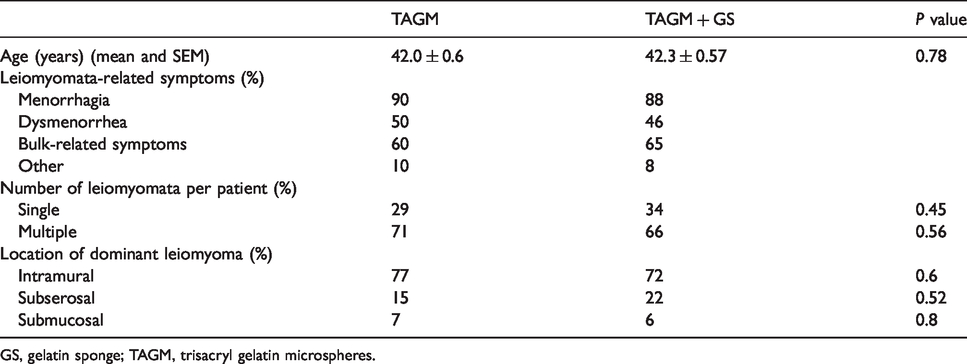
GS, gelatin sponge; TAGM, trisacryl gelatin microspheres.
Uterine and dominant leiomyoma volume and post-embolization changes.

Values are given as mean ± SEM.
GS, gelatin sponge; TAGM, trisacryl gelatin microspheres.
Radiological success and clinical success of UFE in the two patient groups.
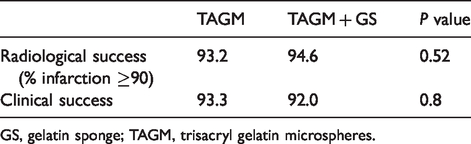
GS, gelatin sponge; TAGM, trisacryl gelatin microspheres.
Clinical success was defined as moderate to complete resolution of symptoms as documented in the patient’s electronic record and UFE clinic chart. No difference was identified with comparable results achieved with both techniques (Table 3).
A 100% technical success rate was achieved for UFE procedure in both groups with both uterine arteries accessed in all cases (except one patient with unilateral absence of a left uterine artery, supply was from the ipsilateral ovarian artery which was successfully embolized using the same TAGM/GS technique).
No major AEs occurred. Minor AEs were infrequent and similar between the two groups with two AEs (grade 1) recorded in the TAGM group (one groin hematoma and one vasovagal hypotensive episode) and two AEs (grade 1) in the TAGM/GS group (two groin hematomas) (1.9% vs. 1.6%, P = 0.82). No intervention was required for these AEs.
Mean pain scores at 24 h were 2.45 (95% confidence interval [CI] = 2.13–2.78) for the TAGM group and 2.66 (95% CI = 2.36–2.95) for the TAGM/GS group with no significant difference identified (P = 0.24).
Mean length of stay was 1.42 days for the TAGM group and 1.39 days for the TAGM/GS group with no significant difference recorded (P = 0.32).
The addition of GS following TAGM for embolization resulted in a significant mean reduction of 2.7 vials (P <0.0001) of TAGM utilized per case compared to embolization with TAGM alone (Table 4). A mean volume of 8.2 mL of GS was injected in slurry form with ≤ 1 Lyostypt® sheet utilized in all but seven cases. In our institute, the current price of one vial of Embosphere® is $268 and a sheet of Lyostypt® costs $14.70. The resultant mean cost of the embolic agents utilized for UFE performed with TAGM was $1688.40 versus $979.50 for UFE performed with TAGM/GS. An overall reduction in cost of embolic agents of $708.90 or 42% was achieved though the addition of GS to TAGM.
TAGM vials utilized in both patient groups.
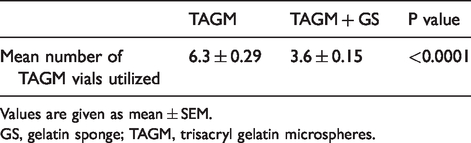
Values are given as mean ± SEM.
GS, gelatin sponge; TAGM, trisacryl gelatin microspheres.
Discussion
Symptomatic uterine leiomyomata can have a substantial impact on a person’s quality of life (20). UFE is an effective, minimally invasive treatment strategy for the management of symptomatic leiomyomata. Multiple embolic agents have been utilized with similar rates of radiological and clinical success (6) but with variable cost differentials.
As value-based healthcare systems are increasingly adopted internationally, radiology reimbursements will no longer be determined by predominantly volume-based metrics instead being dependent on the provision of value-added imaging and intervention services (21–23). It will be critical to demonstrate the cost-effectiveness of procedures in interventional radiology. Driving down the cost denominator without compromising patient outcomes and experience is a key target for improving the value equation (24,25).
The importance of maximizing value was accentuated in our institute due to a substantial reduction in healthcare funding triggered by the global economic recession. This stimulated a review of our technique for UFE with the aim to improve cost efficiencies while minimizing the impact on patient outcomes and access to the procedure.
Before this, UFE was performed in our institute with TAGM as a single embolic agent. Multiple studies have demonstrated the efficacy of TAGM as an embolic agent in UFE (8,9); however, a vial of TAGM costs our institute $268 with multiple vials typically required to achieve the target endpoint of embolization. GS has been previously reported as a suitable embolic agent in UFE; however, most of these studies have been published from a single center and, where radiological outcomes were measured, the studies involved small patient cohorts (11–16). A pilot study directly comparing TAGM and GS in UFE was recently published; however, this identified the need for an additional adequately powered study to evaluate for clinically and statistically significant differences in outcomes between these two agents (26). In our study, the addition of GS to TAGM resulted in a significant reduction in the mean volume of TAGM utilized to achieve the endpoint of embolization with an associated 42% reduction in total costs of embolic agents per procedure and without comprising clinical and radiological outcomes. To our knowledge, no previous study has demonstrated the utility and potential cost-effectiveness of combining embolic agents for UFE.
Measuring cost-effectiveness and value in radiology is challenging. When introducing a new procedure or technique, there are multiple factors beyond differences in material costs to consider that influence cost-effectiveness from a healthcare sector perspective (27), including costs related to staff training as well as changes in operator costs and potential impact on preprocedural and postprocedural costs. In this case, from a procedural perspective, the two techniques we describe differ only in the choice of embolic agents administered. All other steps of the procedure, from establishment of arterial access to catheterization of the uterine arteries and arterial closure, follow the same sequence and utilize the same or similar equipment. As a result, operator and equipment utilization are expected to be similar for the two procedures. Once an operator is familiar with the preparation and use of both embolic agents, which are a standard part of the armament of an interventional radiologist, no substantial additional training is required to perform UFE with a combination of TAGM/GS. While a complete cost analysis of all aspects of the care cycle for UFE were not available, other recorded metrics including length of inpatient stay, patient pain scores, rates of AEs, and outcome measures including radiological and clinical outcomes did not demonstrate a significant difference between the two groups. Furthermore, the pre and post-procedure protocol were unchanged regardless of the embolic agent used. This emphasizes the importance of optimizing the choice of embolic agents in UFE as a strategy for improving the value equation without compromising quality and outcomes.
The cost differentials between these two techniques and overall cost of delivering this service could be more accurately quantified using time-driven activity-based costing (TDABC) (28,29). This requires the creation of detailed process maps for each technique from admission to discharge and an assessment of per minute and itemized costings for each contact point on the process map. Combining this approach with outcome data helps to measure the value of care and can identify drivers of cost in a procedure that can be targeted for optimization (30). TDABC is also a promising tool for reimbursement in radiology. Many current reimbursement models, particularly relative value units (RVUs), focus on the predetermined complexity and time required for an imaging test or procedure and do not incentivize cost-effectiveness. TDABC can directly measure the costs of an imaging test or procedure, demonstrate the cost-effectiveness of any changes to a process, and provide a means of calculating the cost of traditionally non reimbursable components of radiology services, which is of particular importance in the current era of alternative payment models including bundled payments (30). The introduction of TDABC requires adequate resourcing as well as access to cost data and prospective recording of time data for all components of the process map.
The rate of AEs was similar between the two groups. All reported AEs were recorded at the time of the procedure or during the post-procedural hospital course. AEs are likely to be underreported in this study as the sources for documenting AE partially rely on patient reporting and recall of AEs up to six months after the procedure.
There was no difference in pain scores at 24 h between the two groups. Postprocedural pain is anticipated in most patients after UFE and well-planned proactive management of pain is important to ensure a positive recovery experience for patients (31). Our institute has a standardized UFE post-procedural management pathway which includes assessment by the pain management team and an analgesia protocol utilizing PCA where appropriate.
Post-procedural pain and analgesia requirements have been reported to vary depending on the embolic agent used for UFE. A study comparing UFE with gelfoam pledgets versus UFE with TAGM combined with gelfoam pledgets reported an increase in the volume of self-administered morphine delivered by a PCA pump in the TAGM/Gelfoam pledgets group (32). This difference was only observed in the immediate post-procedure period with no difference in analgesia volume requirements identified >3 h after the procedure (32). When compared to our study, gelfoam was used in pledget form as opposed to a slurry with a different technique used for preparation. Additionally, the choice of embolic agent in this study was not randomized and baseline uterine volume and dominant fibroid volume tended to be larger in the TAGM/Gelfoam pledget group which are potential confounding factors influencing the significance of these results. Further studies have demonstrated conflicting post-procedural pain scores for UFE performed with TAGM versus GS alone. Katsumori et al. (33) recorded an increase in pain scores in the GS group versus the TAGM group in the first 18 h after the procedure; however, pain scores >18 h were not evaluated. In contrast, Yadavali et al. (26) demonstrated an increased median pain score at 24 h after the procedure in the TAGM group versus the GS group (3 vs. 2, P = 0.07). These contrasting results suggest that other factors beyond the embolic agent administered influence post-procedural pain scores. Thus, to date, no consistent significant difference in post-procedural pain scores has been demonstrated between these two embolic agents and our study demonstrated no significant difference in pain scores at 24 h after the procedure when these embolic agents were combined compared to TAGM alone. Additionally, a significant difference in post-procedural pain may have been reflected in a prolonged length of stay for one group in our study; however, length of stay was similar for both groups.
The degree of leiomyoma infarction on post-embolization MRI was chosen as a primary outcome as it has been identified as a reliable indicator for the success of embolization and for long-term clinical outcomes (34–36) and has been utilized in most major studies comparing embolic agents. Our results in a large patient cohort demonstrate no significant difference in radiological outcome when UFE is performed with TAGM alone or using our technique with a combination of TAGM/GS with both techniques producing excellent successful infarction rates (≥90% infarction of the dominant leiomyoma) of 93.2% and 94.6%, respectively (P = 0.52). While in one study UFE with TAGM versus GS alone resulted in a significant difference in uterine volume reduction in the TAGM group alone (22), our study comparing TAGM to combined TAGM/GS demonstrated no significant difference in the mean reduction in volume of the uterus (P = 0.16) and dominant leiomyoma (P = 0.29). This suggests that our technique combining TAGM/GS for UFE has favorable outcomes compared to GS alone with results comparable to TAGM for UFE. Clinical success rates were similar between the two cohorts (P = 0.8) and are closely aligned with the rate of successful radiological outcome in our cohort.
This study has a number of limitations. The data were collected retrospectively; however, all data were acquired from records documented systematically at the time of the procedure and follow-up UFE clinics with similar baseline characteristics between the two groups. The pre-embolization proforma and post-procedural clinical follow-up utilized a standardized department-specific questionnaire which has not been validated in other studies; however, the primary outcomes of this study were based on MRI findings which have been shown to predict long-term clinical outcomes (34–36) and clinical outcomes in our study closely aligned with radiological outcomes. The six-month follow-up period may not be a sufficient duration to reflect the true long-term outcome differences between these techniques; however, as noted above, rates of leiomyoma infarction have been shown to predict long-term clinical outcomes (34–36) and no difference in infarction rates was identified between the two groups in the present study. The study extends over a time frame of 9.5 years which could impact the results between the two groups with variations in the procedure technique and acquired procedural experience over this period. The UFE program was established in our institute 10 years before the study period. Each operator had extensive experience in performing UFE before this timeframe, helping to reduce the impact this could have on the study results. In addition, the technique utilized was similar throughout the study period for all operators with primary variation occurring in catheter preference only. The cost of embolic agents TAGM and GS would also have varied over the time period with costing estimates based on present day prices; however, the cost of TAGM was always substantially greater than that of GS over the study period. Accurately determining cost in healthcare is challenging due to the complex and often fragmented nature of the cycle of care for a diagnosis and the need for longitudinal assessment of costs and outcomes (25). We recognize that this is just one aspect of the entire “episode of care” for the management of symptomatic uterine leiomyomata and that in order to maximise the value equation all aspects of care require optimization through streamlined multidisciplinary patient-centered care pathways with the appropriate expertise and facilities available to achieve best outcomes and optimization of costs at each contact point in the “episode of care” (37).
In conclusion, our results suggest that the introduction of GS combined with TAGM for UFE in the management of symptomatic uterine leiomyomata allows for a substantial reduction in the overall cost of embolic agents utilized per procedure, the main cost differential between the two described techniques, without compromising the excellent radiological and clinical outcomes achieved with this effective minimally invasive procedure. A longer-term prospective study simultaneously assessing overall costs of the procedure utilizing a strategy such as TDABC may help to further support the clinical efficacy and cost-effectiveness of embolization with combined TAGM/GS.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.