
Abstract
Background
Partial nephrectomy may be complicated by postoperative hemorrhage, which may be treated by transcatheter embolization.
Purpose
To assess the safety and efficacy of embolotherapy for hemorrhagic complications of partial nephrectomy and to analyze the potential correlation between multiple bleeding sites on angiography and surgical complexity
Material and Methods
A cohort of 25 patients presenting with severe, postoperative bleeding after partial nephrectomy and treated with catheter-directed superselective embolization was included. Patients’ demographics, radiological investigations before the embolization, and clinical outcome after embolization were analyzed. Mann–Whitney U test was used to analyze the potential difference in the RENAL score between patients with one or more bleeding sites in the resection area.
Results
Selective renal angiography revealed multiple bleeding sites at the resection bed in 8 (32%) patients with amorphous contrast extravasation in 10 (40%) patients. Embolization with use of a microcatheter and microcoils was effective to stop the bleeding in all but one patient, the latter requiring a second embolization two days later. Transient decrease in renal function was noted in 3/25 (12%) patients with full recovery in two of the three. Patients with multiple bleeding sites did not show significantly different RENAL scores compared to patients with a single bleeding site (P = 0.148).
Conclusion
Embolotherapy for postoperative partial nephrectomy-related bleeding is safe and effective with a low rate of recurrent bleeding. The number of bleeding sites at the resection area did not correlate to the RENAL score.
Introduction
Nephron-sparing partial nephrectomy has become the standard of care for small renal tumors irrespective of a clinical context of solitary kidney, bilateral involvement, or impaired renal function (1,2). Iatrogenic vascular lesions related to partial nephrectomy are rare complications with an incidence <5% (1). However, complications might become potentially life-threatening (3,4). Surgical reintervention with total nephrectomy is a radical option to definitively stop the bleeding. Minimally invasive, catheter-directed management is the preferred approach to hemorrhagic complications after partial nephrectomy.
Several case reports and small case series already described the technical feasibility and clinical follow-up data mentioned a very low rate of decreased renal function (3,5–9). Most of the reports analyzing embolization of postoperative hemorrhage after nephron-sparing surgery describe a single bleeding site on angiography (10,11), whereas Gupta et al. (12) drew the attention to multiple (≥2) bleeding sites on therapeutic angiography.
In the present study, we analyzed the number of bleeding sites, the potential relation with elaborative surgery and the outcome after embolotherapy, with regard to the effectiveness of the treatment of the active bleeding, and the residual renal function.
Material and Methods
Patient demographics
A search in the institutional patients’ database revealed 1375 patients who underwent open or laparoscopic partial nephrectomy between January 2000 and January 2016. Of the patients, 25 (1.8%) were identified with symptomatic vascular complications in the early postoperative period after partial nephrectomy and subsequently treated with catheter-directed selective embolotherapy. The medical records and all available imaging studies were retrospectively reviewed. Approval by the institutional ethical committee was obtained.
Pre-interventional diagnostic imaging
Diagnostic imaging before the embolization procedure included duplex-ultrasound imaging, triphasic contrast-enhanced computed tomography (CECT), and catheter-directed angiography. Triphasic CECT was performed on 4-, 16-, or 64-row scanners, depending on the time period of performance. Routinely, 80 mL of non-ionic iodized contrast medium was injected into an antecubital vein with an injection rate of 3 mL/s.
Embolization procedure
Depending on the general clinical condition of the patient, the embolization procedure was performed under local (n = 21, 84%) or general anesthesia (n = 4, 16%). After obtaining the patient’s informed consent, percutaneous access was made to the common femoral artery ipsilateral to the operated kidney with a 4-F vascular sheath. After flush aortography, a selective renal angiography with use of a 4-F Cobra or 4-F Simmons 1 catheter (Glidecath, Terumo Europe, Leuven, Belgium or Performa, Merit Medical, South Jourdan, UT, USA) was performed. Once the active bleeding site was identified, the injured vessel was assessed with use of a microcatheter (Progreat, Terumo Europe, Leuven, Belgium or Cantata, Cook Medical, Bjaeverskov, Denmark) and microcoils (Target microcoils, Boston Scientific, Natick, MA, USA or Microtornado, Cook Medical, Bjaeverskov, Denmark). After embolization, a completion selective renal angiography was performed to confirm disappearance of the vascular lesion.
Patients’ follow-up
All patients were followed up at the urology department, including clinical and biochemical evaluation, with special attention to the residual renal function. Significant increase in creatinine levels after embolization was defined as >10% increase after embolization compared to the pre-procedural levels. Long-term oncological follow-up was applied to all patients and included physical examination and triphasic CECT at three, six, and 12 months after initial surgery and yearly afterwards.
RENAL score and statistical analysis
RENAL score is a nephrometry score described by Kutikov et al. (13), including a classification system for renal masses undergoing excision and is based on: R = radius which is the tumor size as maximal diameter; E = exophytic/endophytic portion of the tumor; N = nearness of tumor deepest portion to the collecting system or sinus; A = anterior/posterior location of the tumor within the kidney; and L = location relative to the polar line. In the context of partial nephrectomy, this classification system provides a useful tool to assess the complexity and resectability of renal masses.
The Mann–Whitney U test was used to analyze the difference between the RENAL total score between patients with single or multiple bleeding sites at the surgical resection area. Analyses have been performed using the SAS software, version 9.4 of the SAS System for Windows (SAS, Cary, NY, USA). A P value <0.05 was considered significant.
Results
Patients’ symptoms prompting imaging studies after partial nephrectomy are lumbar pain (n = 3, 12%), hypotension (n = 1, 4%), hematuria (n = 12, 48%), blood in surgical drain (n = 1, 4%), hemodynamic shock (n = 1, 4%), and asymptomatic with drop in hemoglobin (n = 7, 28%).
Patients’ preoperative demographic data are summarized in Table 1. There was a clear predominance of male patients; the mean age was 66 years.
Patients’ demographic data.
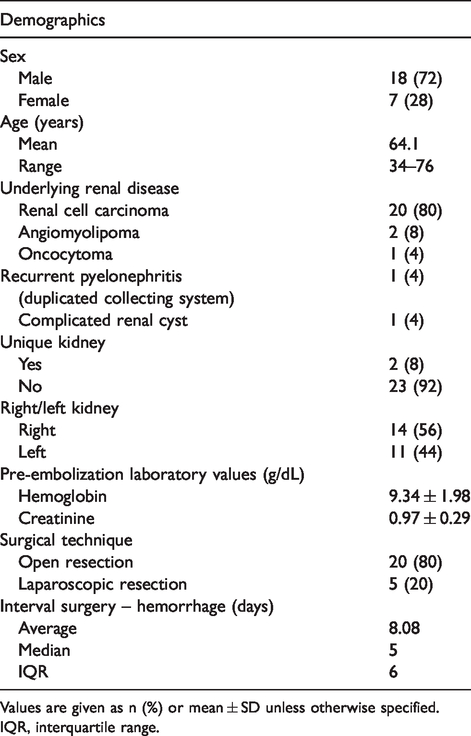
Values are given as n (%) or mean ± SD unless otherwise specified.
IQR, interquartile range.
Clinical suspicion of active postoperative hemorrhage was made by the attending urologist at 0–43 days (median = 5 days) after initial surgery.
Imaging findings, based on ultrasound (US) were available in 14 patients and included: perirenal hematoma (n = 10, 71%); intrarenal pseudoaneurysm (n = 1, 7%); and negative investigation (n = 3, 21%). Imaging findings, based on CECT, were available in 12 patients and included: perirenal hematoma and contrast extravasation (n = 8, 67%); and pseudoaneurysm (n = 4, 33%). No negative CECT was found. Finally, angiographic findings were available in all 25 patients and included: amorphous contrast extravasation (n = 10, 40%); pseudoaneurysm (n = 9, 36%); pseudoaneurysm associated with an arteriovenous fistula (n = 4, 16%) (Fig. 1); and pseudoaneurysm associated with contrast extravasation (n = 2, 8%). In 8 (32%) patients, two or more active bleeding sites were identified on selective renal angiography (Fig. 2): two lesions were detected in three patients and three or more lesions in five patients. RENAL scores, available for 20 patients, are summarized in Table 2, demonstrating no statistically significant difference between patients presenting with one or more bleeding sites (P = 0.148). Additionally, one patient had a concomitant contrast extravasation from a lower pole left renal artery and a left lumbar artery, which was detected on CECT and successfully embolized during therapeutic angiography with use of microparticles (Embosphere 300–500 µm, Merit Medical, South Jourdan, UT, USA) and microcoils (Fig. 3).
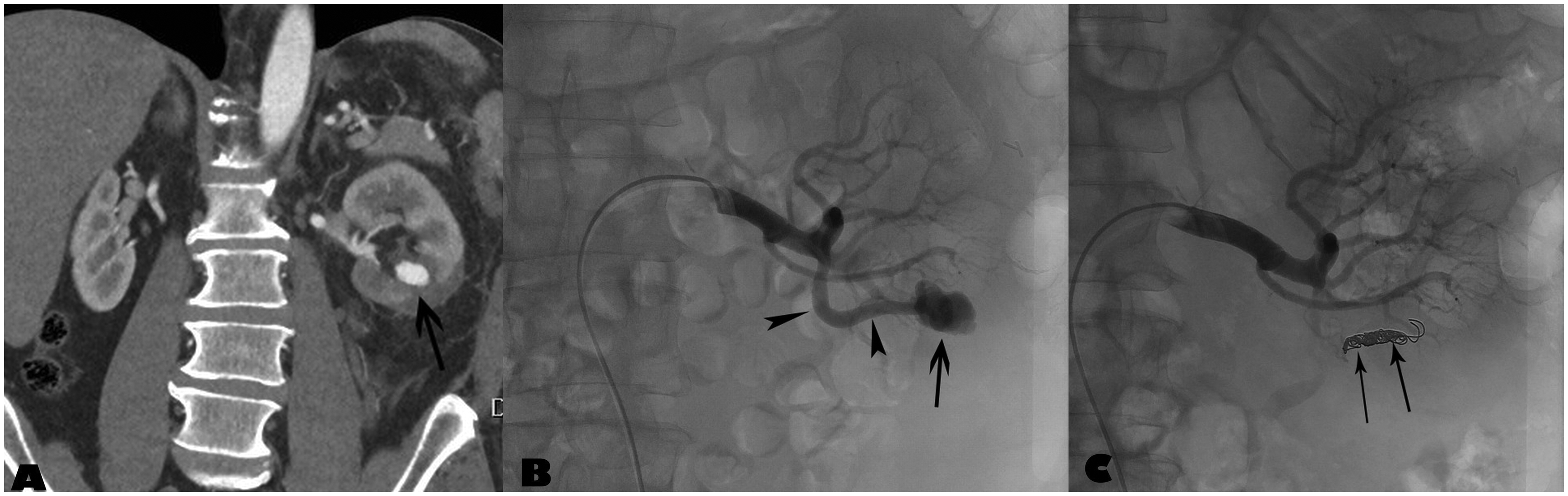
A 61-year-old man presented with macroscopic hematuria 23 days after partial nephrectomy of the left kidney. (a) Contrast-enhanced reconstructed coronal CT image revealed a pseudoaneurysm (arrow) at the section area. (b) Selective left renal angiography confirmed the pseudoaneurysm (arrow) and the afferent artery (arrowheads). (c) Embolization of the afferent artery was performed using microcoils (thin arrows).
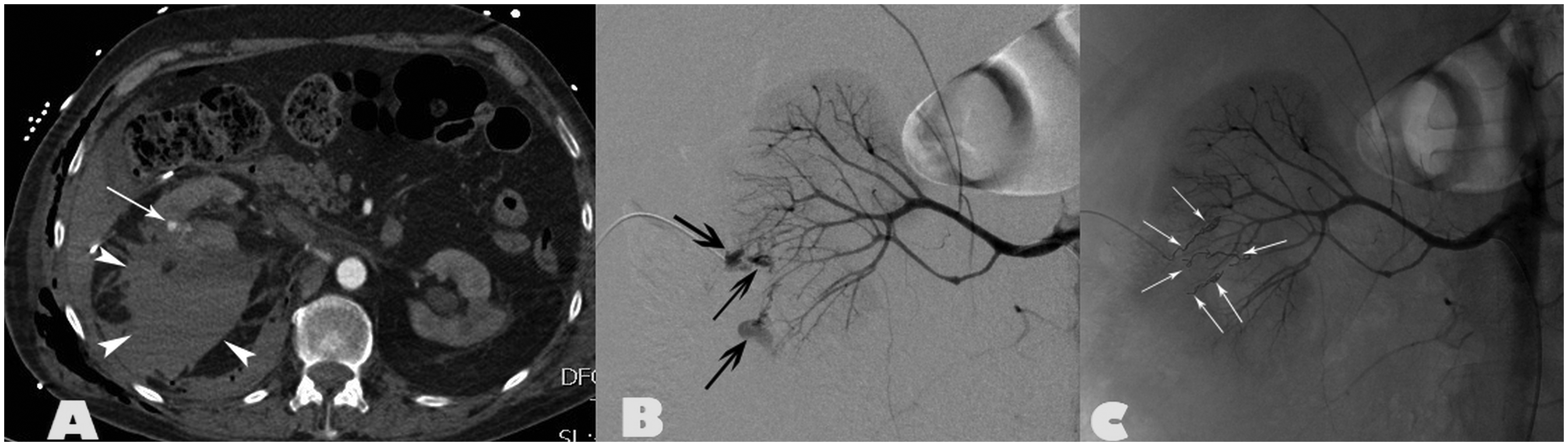
A 55-year-old man presented with lumbar pain and drop in hemoglobin (9.9 g/L) two days after partial nephrectomy for renal cell carcinoma. (a) Contrast-enhanced CT revealed a large retroperitoneal bleeding (arrowheads) and a contrast extravasation (thin arrow) in the right kidney. (b) Selective right renal angiography showed three (arrows) bleeding sites in the section area. (c) Embolization was performed with microcoils (thin arrows).
RENAL score for patients with one or more bleeding points on selective renal angiography.
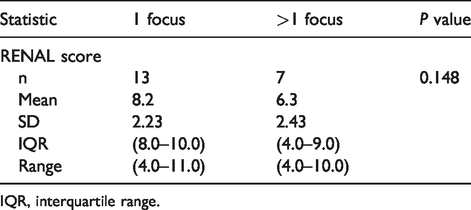
IQR, interquartile range.
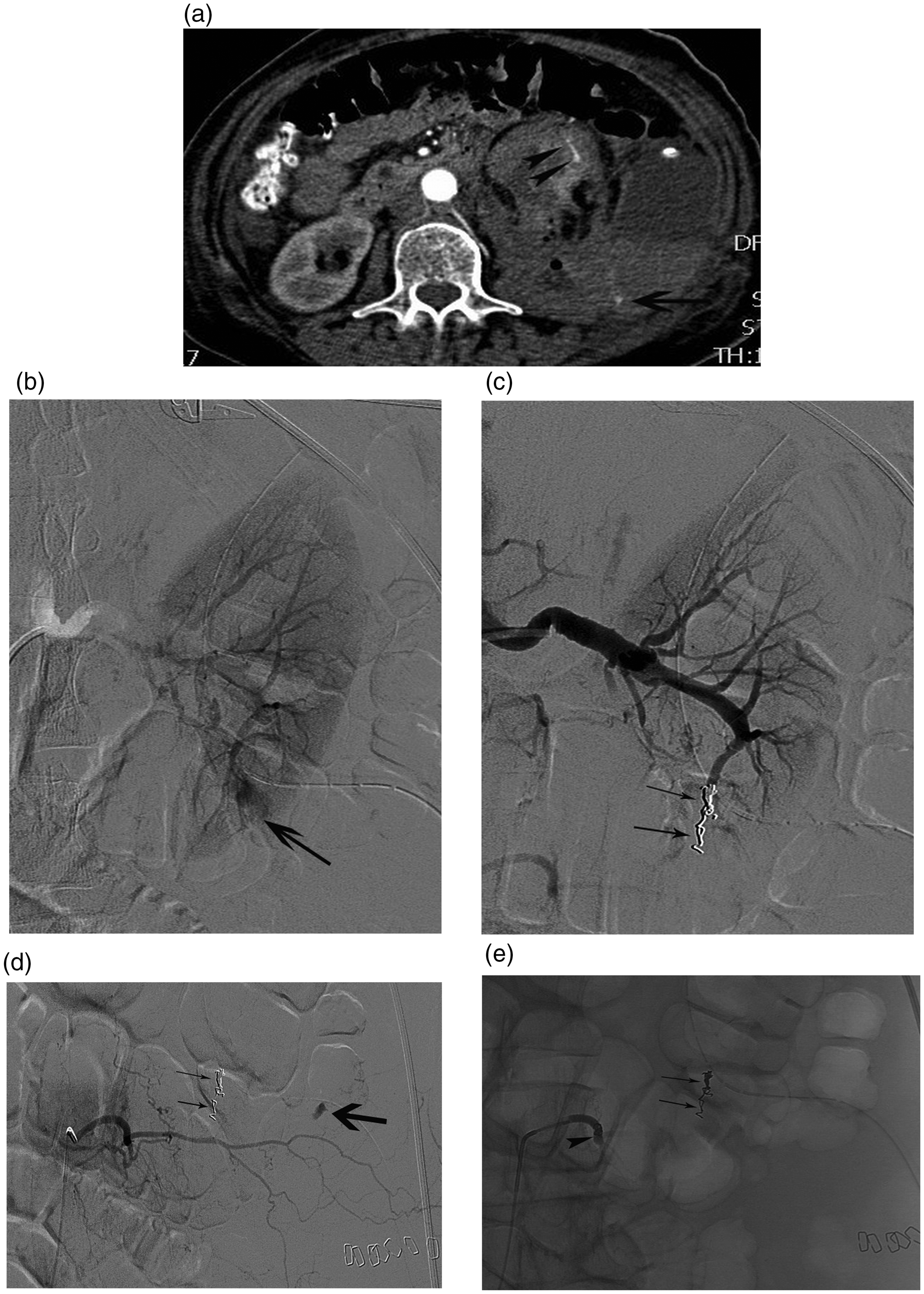
A 70-year-old woman underwent partial nephrectomy for renal cell carcinoma of the left lower pole. (a) Contrast-enhanced CT revealed contrast extravasation (arrowheads) in the left lower renal pole; additionally, a second site of contrast extravasation (arrow) was identified in the left retroperitoneum, distant to the left kidney: posterior abdominal wall bleeding. (b) Selective left renal angiography demonstrated a discrete contrast extravasation (arrow) at the lower pole section area. (c) This was managed with microcoil embolization (small arrows). (d) Selective injection of the third lumbar artery confirmed the extravasation (arrow). Note also the microcoils in the left renal lower pole. (e) Control lumbar angiography after additional embolization shows the microcoils in the proximal lumbar artery (arrowhead); microcoils in the left kidney (small arrows).
Angiographic success, defined by the absence of contrast extravasation on completion selective renal angiography was 100%; however, one patient presented with a drop in hemoglobin level (11.0 g/L to 9.3 g/L) two days after the initial embolization procedure despite successful selective embolization of three separate bleeding sites. Repeat selective renal angiography revealed an additional fourth bleeding site in the left lower pole that was embolized with microcoils (Fig. 4).
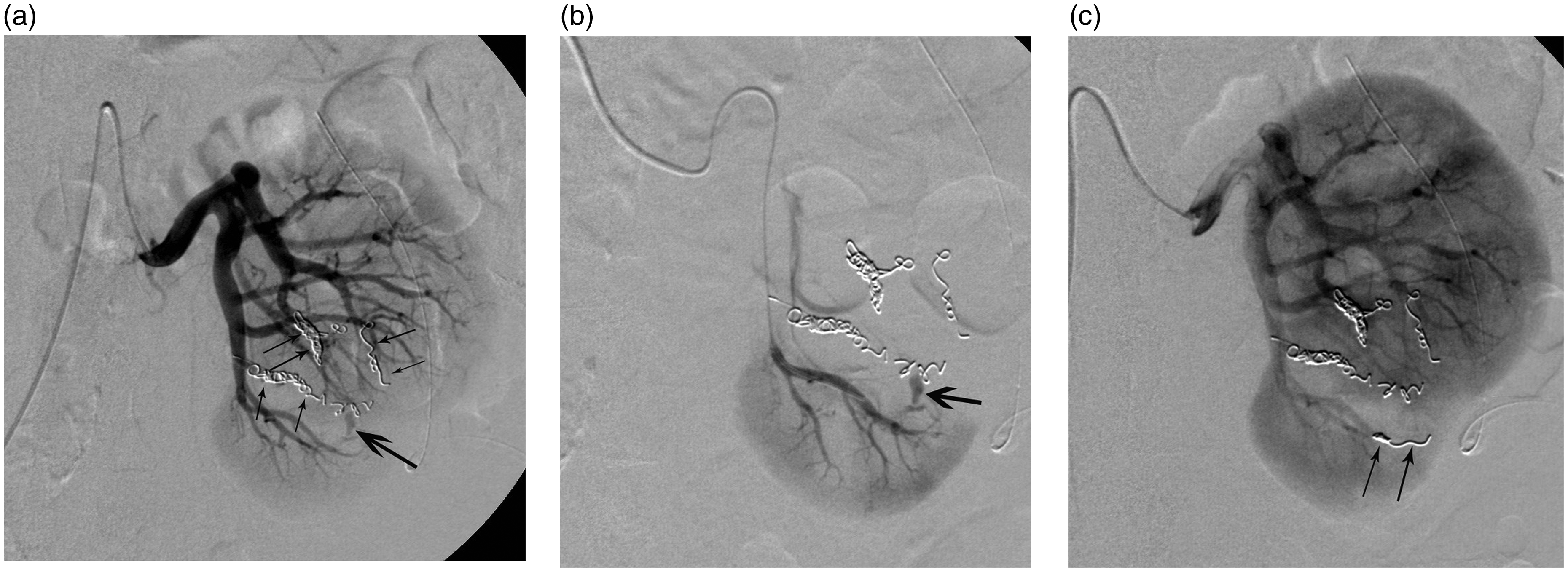
A 76-year-old woman underwent partial nephrectomy for renal cell carcinoma. Three days later, a drop in hemoglobin (7.6 g/L) was noted and embolization of three pseudoaneurysms in the interpolar section area of the left kidney was performed; however, a recurrent hemoglobin drop (11.0 g/L to 9.3 g/L) two days later was noted. (a) Repeat left renal angiography revealed a fourth small pseudoaneurysm (arrow), not detected during initial embolization procedure and close to the microcoils (small arrows). (b) Superselective catheterization confirmed the small pseudoaneurysm (arrow) (c) which was treated by additional microcoil embolization (small arrow).
No angiographic procedure-related complication was noted.
Of the 25 patients, 3 (12%) presented with a transient increase in serum creatinine level (>10% increase as compared to the pre-embolization values) three days after selective embolization (1.1 mL/dL to 3.8 mL/dL; 1.4 mL/dL to 3.7 mL/dL; and 1.3 mL/dL to 3.2 mL/dL). Of these three patients, two showed normalization of the serum creatinine levels, respectively, 7 and 13 days after embolization. The remaining patient presented with a persistent increase in serum creatinine level (2.2 mL/dL vs. 1.1 mL/dL before embolization). This was a cirrhotic patient with a previous history of radical nephrectomy and ipsilateral partial nephrectomy for bifocal renal cell carcinomas.
Long-term follow-up (median = 5.1 years, range = 0– 14 years) revealed recurrence of renal cell cancer in 1 (4%) patient out of 25, detected eight months after partial nephrectomy; this patient was treated by total nephrectomy.
Discussion
The present study demonstrates the high efficacy of catheter-directed embolization for hemorrhage related to nephron-sparing surgery. In this series, only 1/25 (4%) patients required a second embolization procedure to definite control the postoperative bleeding. This number is somewhat lower compared to published series, reporting repeat angiography for recurrent bleeding in 5%–15% of cases (10,11). The low incidence of postoperative hemorrhagic complications and the time interval between initial surgery and referral for embolotherapy are in line with other series, as summarized in Table 3.
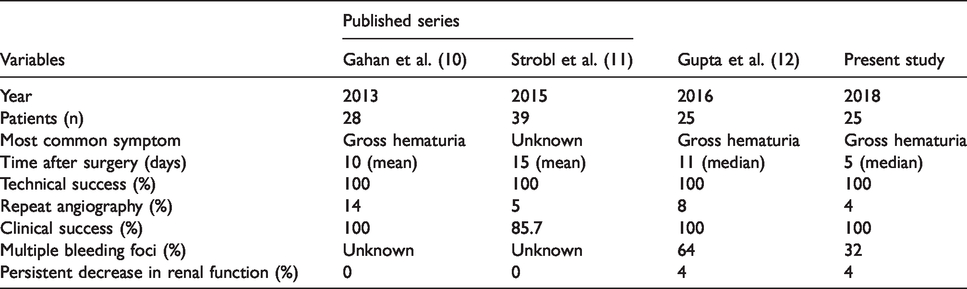
Overview of outcome data after embolization of hemorrhage related to partial nephrectomy, based on case series with >20 patients.
CECT seems to be more accurate than US to identify a postoperative bleeding: in 20% of cases the postoperative bleeding was missed by US whereas CECT showed the active bleeding in all patients. Disadvantages of CECT are the radiation load and the intravenous administration of contrast medium before the therapeutic angiography. Persistent decrease of renal function was observed in 1 (4%) patient after embolotherapy. This was a particular case of a patient with postoperative bleeding in a solitary kidney and after previous surgical resection of two renal cell carcinomas of this kidney. Another factor that may contribute to further renal impairment is necrosis related to the embolotherapy of functional renal parenchyma. Therefore, superselective embolization with microcatheters is recommended to avoid additional damage to the renal parenchyma.
Further, CECT offers the advantage to detect other unexpected complications. In one patient in the present series, an active retroperitoneal bleeding due to a traumatic lesion of a lumbar artery was diagnosed. Such bleeding sites can be missed at selective renal angiography without previous diagnostic CECT.
The present study demonstrates at least two bleeding sites in almost one-third of included patients, whereas Gupta et al. (12) found two or more bleeding points in nearly two-thirds of patients. Based on these two series, careful analysis of the selective renal angiography is recommended and potentially perform additional oblique views not to overlook additional bleeding sites from feeding vessels to the operative bed. The RENAL score for all included patients has been reassessed, in accordance to Kutikov et al. (13). This score in a way reflects of the potential difficulty of the partial nephrectomy. However, contrary to Gupta et al. (12), the authors could not confirm a correlation between a higher incidence for multiple postoperative bleeding sites in patients with a higher RENAL score. Therefore, careful angiographic analysis for multiple bleeding sites should be performed in all patients presenting with postoperative bleeding whatever the RENAL score or surgical complexity.
The present study has some limitations. This series is based on a retrospective analysis and not all patients received the same radiological investigations before embolization. Second, the patient sample size is small. Finally, the indication for partial nephrectomy was not the same for all included patients; the large majority (80%) was surgery for renal cell carcinoma.
In conclusion, this retrospective analysis demonstrates a high efficacy of catheter-directed microcoil embolization for postoperative hemorrhage complications of nephron-sparing surgery. Detection of multiple bleeding sites in the resection area is not uncommon and should be carefully evaluated in each patient independent of the RENAL and/or surgical complexity.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.