
Abstract
Background
Image noise, object repositioning, initial manual image alignment, and stitching of different volumes, i.e. anatomical regions may all affect the stitching error of fused cone-beam computed tomography (CBCT) images.
Purpose
To determine the geometric error of fused CBCT images of the hindfoot, lower leg, and forefoot after using stitching software, based on a marker-less validation method.
Material and Methods
CBCT images of the hindfoot, lower leg, and forefoot were acquired multiple times on a Planmed Verity scanner with and without repositioning the leg between acquisitions. Prototype stitching software was used to stitch hindfoot–forefoot volumes and hindfoot–lower leg volumes. Stitching error was determined via registration and by calculating the displacement of the tibia, first metatarsal, or proximal phalanges, with respect to the calcaneus, compared to their position on conventional CT.
Results
Overall total translation and rotation errors were 1.22 ± 0.62 mm (range 0.43–3.07 mm) and 1.27° ± 0.53° (range 0.29°–2.88°). Lower leg translation was smaller compared to forefoot translation (P < 0.001). No statistical difference was observed between lower leg and forefoot rotation errors (P = 0.186). Cadaver repositioning between acquisitions resulted in larger rotation errors (P < 0.05). Cadaver repositioning did not affect translation errors (P = 0.768).
Conclusion
Geometric error of fused CBCT images can be quantified using a marker-less validation method. Stitching of hindfoot volumes with forefoot and lower leg volumes induces translation and rotation errors of up to approximately 3 mm and 3°. Translation errors are larger in hindfoot–forefoot stitches compared to hindfoot–lower leg stitches.
Introduction
Cone-beam computed tomography (CBCT) enables the acquisition of high-resolution images of the extremities. It furthermore enables the acquisition of images under natural loading, so-called weight-bearing CBCT images. This type of functional imaging may reveal anomalies that would otherwise be non-discernable (1–6), such as the displacement of bone fragments in patients with deformities and a diminished joint space in patients with osteoarthritis (7,8). Unfortunately, the small scan volume of such systems (typically 16 × 13 cm) limits the clinical use of this type of CBCT scanner. To enable the acquisition of larger volumes of interest, some systems are equipped with stitching software, which enables the stitching or fusion of two volumes into one volume.
Although inaccurate stitching affects quantitative position analysis and joint space measurements, only a limited number of studies investigated the stitching error of CBCT images in dried skulls, plastic skull models, and cadaveric mandibles (9–13). To the best of our knowledge, no data are available on the stitching error of image volumes of the lower extremity. In addition, the development and use of a marker-less analysis method that utilizes bones as in vivo markers is preferred. This method of analysis can also be used for the validation of other stitching algorithms. We hypothesize that image noise, object repositioning between acquisitions, the initial manual image alignment, and stitching of different volumes, i.e. anatomical regions, affect the stitching error. The aim of the present study was to acquire multiple volumes of the hindfoot, lower leg, and forefoot with and without repositioning the cadaver between acquisitions and to determine the positioning error of bones in stitched images.
Material and Methods
Image acquisition
A fresh frozen human cadaveric lower leg specimen was scanned on a conventional Somaton definition AS+ CT scanner (Siemens Healthcare, Erlangen, Germany) using a clinical CT protocol (120 kVp single-energy, 95 mAs, 0.6 mm, and sharp reconstruction filter I70). This CT scan served as reference and provided the gold standard regarding the relative position of bones. The specimen was used to preclude relative position changes of bones. Subsequently, the specimen was scanned multiple times (96 kV, 6.3 mA) on a Verity CBCT scanner (Planmed Oy, Helsinki, Finland). High definition scan and reconstruction parameters were used, with a voxel size of 0.2 × 0.2 ×0.2 mm, 500 projections, 20 ms pulse length, and default kernel. The hindfoot, distal lower leg, and forefoot were each acquired within a cylindrical scan volume of 16 × 13 cm (Fig. 1).
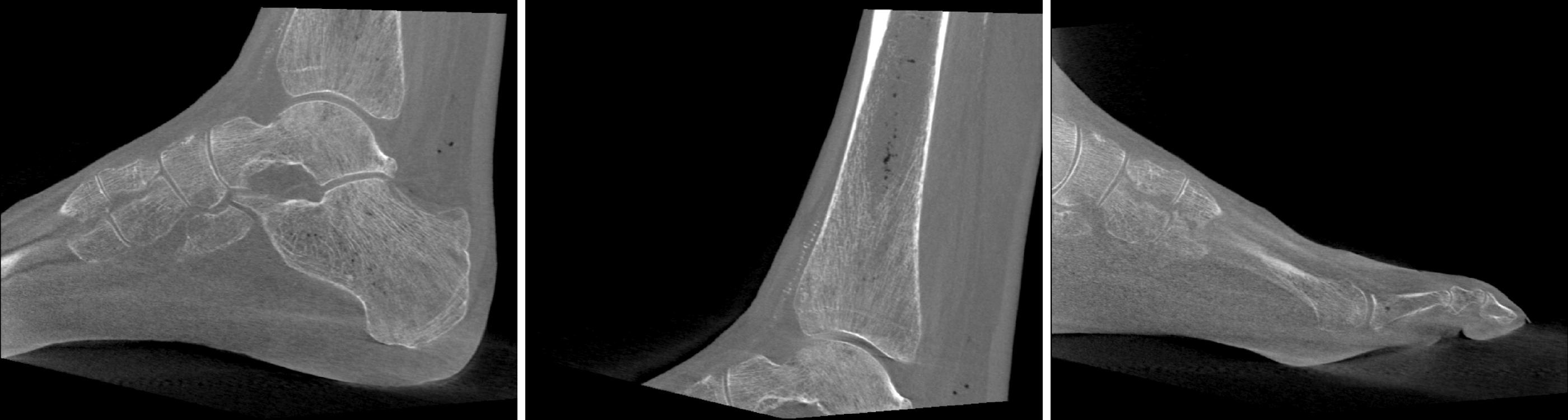
Images of the hindfoot (left), distal lower leg (middle), and forefoot (right) are shown using a window level of –100 and window width of 2000. The forefoot is acquired by rotating the foot 180° due to size limitations of the gantry.
Stitching of volumes
Scan volumes were imported in Romexis (version 5.2.1.R, Planmeca Oy, Helsinki, Finland), down-sampled to 0.4 mm volumes and exported to a workstation. Novel prototype stitching software of Planmed Oy (Helsinki, Finland) enabled semi-automatic stitching of any preferred anatomical regions, for example the hindfoot with the forefoot or distal lower leg. The prototype software enabled the alignment of both volumes by translating and rotating both images in three planes. After the manual alignment of both volumes, the stitching software optimized the stitching. The 3D volume stitching algorithm is based on applying an iterative closest point (ICP) rigid registration algorithm (14) on 3D point sets sampled from bone isosurfaces of the stitched volumes. The bone isosurfaces were extracted by applying the marching cubes algorithm (15) and volume-specific bone Hounsfield units (HU) threshold values. Four different bone HU thresholds values (1250, 1420, 1590, and 1760 HU) were used to extract the bone isosurfaces from each of the unstitched image volumes. The ICP registration was performed for each of the 4 × 4 isosurface pairs, resulting in 16 registration transformation candidates. The goodness of the transformations was determined by applying them to the image volumes and computing the mean square difference of the overlapping image voxel HU values, with the smallest mean squared error (MSE) value taken as an indication of the best fit. The final stitched volume was reconstructed using the registration transformation corresponding to the smallest MSE value, with trilinear interpolation and blending performed in the overlapping volume region.
Quantification of the positioning error
The geometric error in stitched images was quantified by investigating the relative position of bones in the stitched images and by comparing these with their position in a conventional CT scan of the whole foot, which served as reference. The error was determined by quantifying the relative position of the tibia and bones in the forefoot with respect to the calcaneus. In case of the forefoot, the first metatarsal bone (MTT1) or proximal phalanges 1 and 5 were used. Phalanges 1 and 5 were grouped together to improve the registration accuracy of these relatively small bones. To quantify the relative position, the tibia, MTT1, and proximal phalanges 1 and 5 were first segmented in the conventional CT scan. Their relative position served as reference in this study. Next the relative position of these bone segments in stitched images were found by registration (16).
For each stitched image, the registration process provided a matrix Mm to align the segmented moving bone (tibia or forefoot bone(s)) with the target image, and a matrix Mc to align the segmented calcaneus with the target image. The relative positioning error was then determined from the matrix describing the residual relative displacement: Me = Mc−1Mm. The residual translation error (dx, dy, dz) and rotation error (φx, φy, φz, rotation sequence: yxz) were extracted from this matrix. In addition, we used the norm of the translation and rotation error parameters to represent the overall translation and rotation error. In this paper, the geometric error is expressed in terms of accuracy and precision. The average error of repeated measurements was used to represent the accuracy of stitching, the variability served to represent the precision of stitching. The translation (in mm) and rotation (in degrees) of the tibia and bones in the forefoot were expressed in a coordinate system based on inertial axes of the calcaneus (Fig. 2).
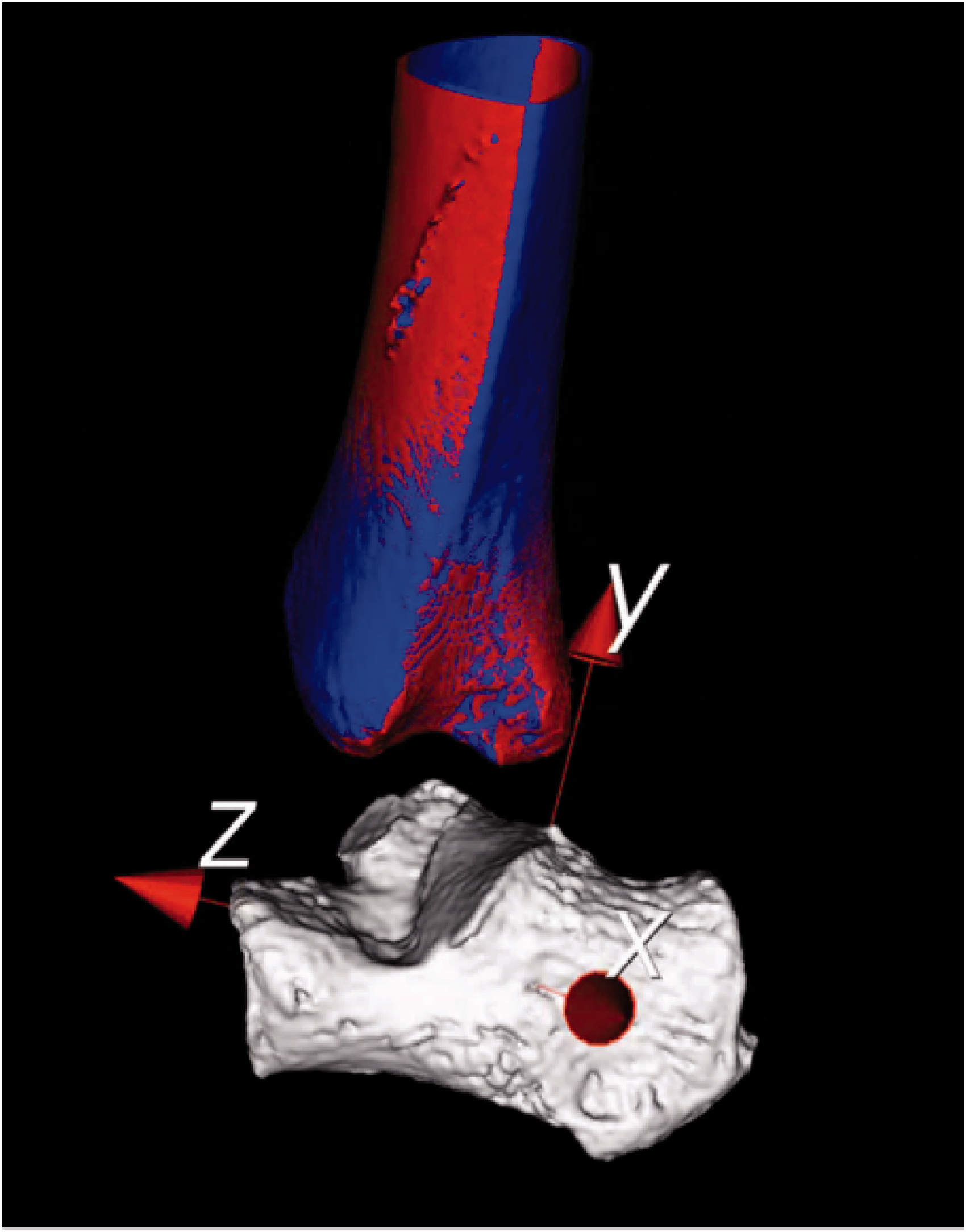
A translation and rotation of the tibia is shown between a stitched scan (blue) and the conventional computed tomography scan (orange). The location of the calcaneus served as a reference.
Experiments
First, we evaluated the methodological error of our procedure by determining the apparent bone repositioning in repeated scans within a single volume. The study protocol consists of four experiments including hindfoot–lower leg stitches and hindfoot–forefoot stitches. We quantified the geometric stitching error with and without moving the cadaver specimen between subsequent acquisitions (Fig. 3).
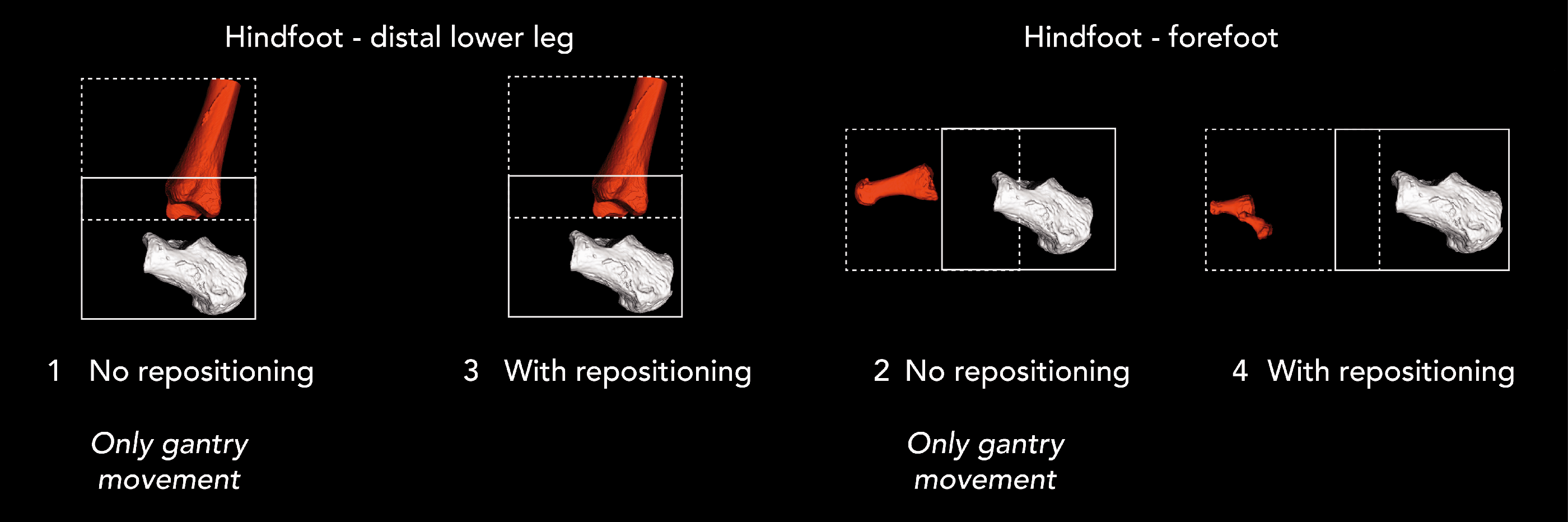
The calcaneus, first metatarsal, and phalanges 1 and 5 were used to calculate the stitching accuracy in experiments 1–4.
Quantifying methodological evaluation error
The methodological error of our procedure was obtained by quantifying the geometric error of two bones within a single volume. We segmented the calcaneus and navicular bone in the conventional CT scan and calculated the translation and rotation of the navicular with respect to the calcaneus in five hindfoot CBCT scans.
Quantifying geometric stitching error, effect of noise
In experiment 1, the hindfoot and distal lower leg were both scanned five times without moving the cadaver, which resulted in 5 × 5 = 25 stitches. Only up and down gantry movement was applied for scanning and subsequent stitching of the hindfoot and distal lower leg scan.
In experiment 2, the hindfoot and forefoot were both scanned five times without moving the cadaver between the scans, resulting in 25 stitches. In this case the gantry was rotated 90°, simulating a supine, non-weight-bearing position. The tilted gantry moved up and down in order to scan the hindfoot and forefoot. However, the entire foot could not be acquired in this way due to the size limitations of the gantry. Therefore, MTT1 was evaluated instead of the proximal phalanges 1 and 5.
Quantifying geometric stitching error, effect of leg repositioning
In experiment 3, the hindfoot and distal lower leg were scanned four times while applying small changes to the position and orientation of the cadaver after each scan. This resulted in 16 stitches. The gantry moved up and down in order to acquire the hindfoot and distal lower leg.
In experiment 4, the hindfoot and forefoot were scanned four times while applying small changes to the position and orientation of the cadaver after each scan. As in experiment 3, this resulted in 16 stitches. To be able to acquire the entire forefoot, the cadaver was rotated 180° using the same gantry height (Fig. 4). Contrary to experiment 2, the proximal phalanges 1 and 5 were evaluated.

In experiments 1, 3, and 4, the cadaver lower leg was orientated in the upright or standing position, using the weight-bearing computed tomography stool (left image). In experiment 2, the lower leg was orientated in a supine or standard position and only up and down tilted gantry movement was applied (right image).
Statistical analysis
Shapiro–Wilk test and visual inspections were performed to determine whether data were normally distributed. Since the data were normally distributed and consisted of independent variables, the small sample sizes of 25 and results of four groups were compared; one-way ANOVA with post-hoc Tukey analysis was used. Mann–Whitney U tests were used to compare results with and without repositioning and to compare the results of both stitching approaches. A significance level of 5% was used for all tests; all tests were two-tailed. SPSS software, version 25 was used.
Results
In Fig. 5, examples of a stitched hindfoot and lower leg and hindfoot and forefoot are shown without any visible stitching artifacts. However, due to translation and rotation stitching errors, stitching artifacts may be introduced, which are mainly visible in soft tissue regions in hindfoot–forefoot stitches and in the tibiotalar joint in the case of hindfoot–lower leg stitches (Fig. 6).

Stitched images of hindfoot and lower leg (left) and of hindfoot and forefoot (right) are shown without any visible stitching artifacts.
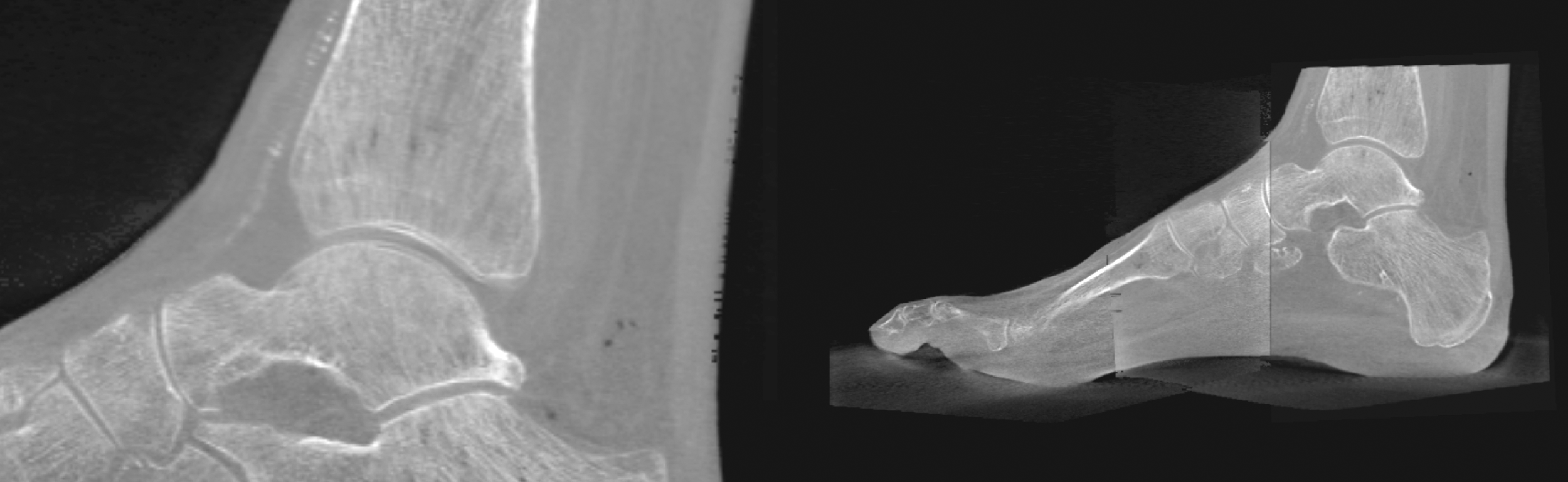
A stitching artifact in the tibiotalar region is shown since the cortexes of the tibia and talus are represented twice (left). Soft tissue artifacts can be observed in the overlapping area of a hindfoot–forefoot stitch (right).
Quantifying methodological evaluation error
The precision of the method used was determined by measuring the translation and rotation of the navicular bone with respect to the calcaneus. Both bones were segmented in the conventional CT scan and were registered in five CBCT scans of the hindfoot. The maximum translation of the navicular bone with respect to the calcaneus in x, y, and z-direction and total translation were 0.09, 0.05, 0.2, and 0.23 mm (Fig. 7). The maximum rotation of the navicular bone with respect to the calcaneus around the x, y, and z-axes and total rotation were 0.06°, 0.13°, 0.48°, and 0.50°.
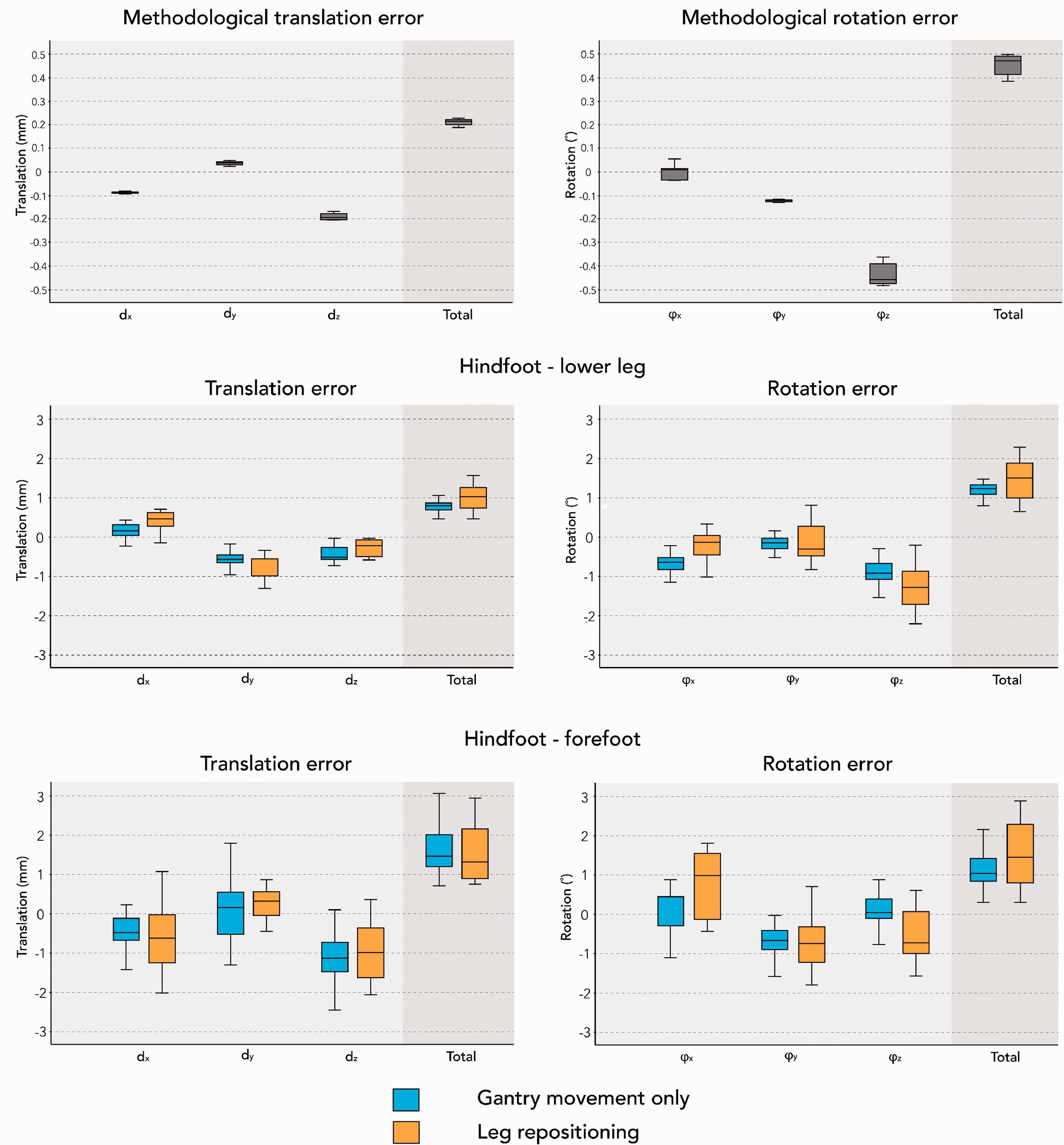
The methodological error of the procedure expressed in dx, dy, dz, total translation error, rotation error ϕx, ϕy, ϕz, and total rotation error. Translation in x, y, and z-direction, total translation, rotation around the x (a), y (b), and z (c)-axes and total rotation of the tibia, MTT1, and proximal phalanges 1 and 5 with respect to the calcaneus for experiments 1–4. Total translation and total rotation of the tibia (experiments 1 and 3), MTT1 (experiment 2), and proximal phalanges 1 and 5 (experiment 4) with respect to the calcaneus are shown. MTT1, first metatarsal.
Translation and rotation errors
Fig. 7 illustrates the translation error dx, dy, dz, total translation error, rotation error φx, φy, φz and total rotation error of the tibia, MTT1, and proximal phalanges 1 and 5 with respect to the calcaneus for experiments 1–4. Translations in the x, y, and z-direction were both positive and negative and were in the range of –2.44 and 2.23 mm. In addition, rotations around the x, y and z-axes were both positive and negative and were in the range of –2.21° and 1.80°.
The norm of the translation and rotation error parameters was used to represent the overall translation and rotation error and was expressed as a positive value. The average total translation error of experiments 1 and 4 was found to be 1.22 ± 0.62 mm and was in the range of 0.43–3.07 mm, where the mean total rotation error was 1.27° ± 0.53° and was in the range of 0.29°–2.88°.
Quantifying geometric stitching error, effect of noise
In hindfoot–lower leg stitches, the total translation of the tibia was smaller than the translation of bones in the forefoot in hindfoot–forefoot stitches (P < 0.001). No statistical difference in rotation errors was observed between hindfoot–lower leg stitches and hindfoot–forefoot stitches (P = 0.186).
Quantifying geometric stitching error, effect of leg repositioning
Repositioning the cadaver between acquisitions resulted in larger rotation errors compared to experiments without repositioning the cadaver (P < 0.05). Reposition did not result in statistical differences with respect to translation errors (P = 0.768).
Discussion
Several CBCT scanners enable the acquisition of two-dimensional and three-dimensional (3D) images under natural loading, referred to as “weight-bearing cone-beam CT,” albeit with a limited field of view (FOV). In CBCT imaging, resolution and FOV differ compared to conventional CT (9,11). Stitching software enables the semi-automatic fusion or stitching of multiple CBCT volumes into one 3D volume. Hereby the depiction of larger volumes, such as an entire foot, is possible. However, the accuracy and precision of stitching may be affected by image noise, by object repositioning, by errors due to manual image alignment, and by stitching different anatomical regions. In the present study, we acquired multiple volumes of a cadaveric hindfoot, lower leg, and forefoot with and without repositioning the specimen between acquisitions and determined the translation and rotation accuracy and precision of stitched volumes. The actual stitching error was determined by quantifying the relative position of the tibia and bones in the forefoot with respect to the calcaneus.
Our marker-less method for evaluating the relative position of bone segments showed a measurement error of approximately 0.23 mm and 0.50° caused by segmentation and registration in conventional CT and CBCT images. The magnitude of the methodological errors demonstrates that the method used is appropriate for evaluating the stitching accuracy. The overall total translation and rotation errors were 1.22 ± 0.62 mm (range = 0.43–3.07 mm) and 1.27° ± 0.53° (range = 0.29°– 2.88°). The lower leg translation error was smaller compared to the forefoot translation error (P < 0.001). No statistical difference was observed between lower leg and forefoot rotation errors (P = 0.186). Repositioning the cadaver between acquisitions resulted in larger rotation errors (P < 0.05). Cadaver repositioning did not affect translation errors (P = 0.768).
Based on the results of the present study, we found that the average total translation error was 1.22 ± 0.62 mm (range = 0.43–3.07 mm) where the average total rotation error was 1.27° ± 0.53° (range = 0.29°–2.88°). Repositioning the cadaver between acquisitions resulted in larger rotation errors compared to experiments without repositioning the cadaver (P < 0.05). However, repositioning did not result in statistical differences with respect to translation errors (P = 0.768). On the other hand, translation errors were smaller in hindfoot–lower leg stitches compared to hindfoot–forefoot stitches (P < 0.001), with no statistical difference in rotation errors between both stitching approaches (P = 0.186). Stitched hindfoot–forefoot images can be acquired in supine and upright position, with no statistical difference in translation and rotation errors. However, the depiction of the entire foot is preferred in the upright position since images can be acquired under weight-bearing conditions and larger foot sizes are less of an issue.
A cadaver specimen was used to preclude relative positional changes of bones in the foot and lower leg. In patients, relative position changes of bones due to repositioning or small movements between acquisitions may affect the accuracy and precision of stitching. Patient movement should be minimized between acquisitions. Therefore, the system should be adapted to preclude the currently required 180° of foot rotation to scan the forefoot.
Several studies investigated the stitching accuracy in the facial region using dried skulls, plastic skull models, and cadaveric mandibles by use of fiducial markers (9–13). Brullmann et al. (13) aligned and merged CBCT skull images of patients using image-based registration. LEGO bricks were used as fiducial markers due to the specific and well-defined size and shape. The software matched both volumes by applying translation and rotation changes with a high registration accuracy < 0.5 mm.
Kopp and Ottl et al. (11) measured distances between several reproducible points fixated on a human cadaveric mandible and used direct sliding caliper as a reference. Standard deviations for vertical distances were in the range of 0.21–0.42 mm and standard deviations for horizontal and diagonal distances were in the range of 0.20–1.03 mm. Angulation mismatch was harder to detect automatically, which emphasizes the importance of minimizing repositioning and small movements between subsequent acquisitions. Kim et al. (10) also determined the accuracy and validity of CBCT images compared to conventional multidetector CT using 10 skull models. They found no significant differences between conventional CT images and manually stitched CBCT images (P = 0.017). However, software-aligned stitches were statistically different compared to conventional CT images (P = 0.005). Despite the fact that manual or semi-automatic stitching can be time-consuming, visual alignment and recognition of stitching artifacts may be of value in acquiring accurate and reliable stitches.
Egbert et al. (9) measured the linear distance accuracy and reliability of small FOV CBCT images and tested the suitability for the fabrication of surgical guides. Again, digital calipers were used to measure inaccuracies. Reference points were fixed on cadaveric mandibles serving as a reference and a mean error of 0.34 mm was found. Ozemre et al. (12) investigated the accuracy of stitched CBCT and compared stitched results with an I-CAT device. Linear distances between anatomical landmarks were measured on skulls by multiple observers, where real distances were measured using high-precision digital calipers. A similar FOV size of 17 × 12 cm was used in case of the CBCT images, where 17 × 23 cm was used in case of the I-CAT. They found coronal and sagittal stitching errors of only > 1.54–1.67 or < 0.01 mm compared to reference measurements.
In most studies, stitching accuracy was expressed by a translation error with respect to reference objects or fiducial markers. The use of fiducial markers in CBCT extremity imaging is not clinically feasible due to possible relative position changes of markers. We also expressed the stitching error in translation errors with respect to the calcaneus, which served as a reference object. Average translation errors were found to be in the same range compared to other similar studies (9–13). Unlike other studies, we furthermore provided rotation errors expressed by a total rotation error, consisting of rotations around the x, y, and z-axes.
The average stitching error in terms of translation (1.2 mm) and rotation (1.3°) is small compared to the magnitude of relevant geometrical foot and ankle parameters such as the calcaneal pitch (13°–23°), navicular height (3–5 cm), and Meary’s angle (2°–10°) (17). Therefore, the relative error is small and the clinical impact due to stitching errors can be expected to be minor.
The present study has several limitations. First, we only used a single cadaver and evaluating more cadavers will provide stitching accuracy in different patients with different foot sizes. Furthermore, despite the fact that the use of a frozen specimen enhanced the robustness of the method used to assess the stitching accuracy and precision, the evaluation in patients would be an interesting next step. Also, other different anatomical regions can be stitched semi-automatically using this software. Currently, fully automatic stitching is only possible using commercial software for hindfoot–lower leg volumes. Also, the stitching accuracy and precision was determined based on different structures, i.e. the tibia, MTT1, and proximal phalanges 1 and 5. Finally, when stitching of multiple volumes into one composed volume is necessary to depict a volume of interest, radiation exposure increases and conventional CT or radiography may be preferred imaging modalities. However, conventional CT and radiography lack the functional high-resolution 3D imaging under natural loading.
In conclusion, geometric error of fused CBCT images of the hindfoot, lower leg, and forefoot can be quantified using a marker-less validation method. Stitching of hindfoot volumes with forefoot and lower leg volumes induces translation and rotation errors of up to approximately 3 mm and 3°. Translation errors are larger in hindfoot–forefoot stitches compared to hindfoot–lower leg stitches. Stitching of images acquired with gantry movement only is advised since repositioning volumes between acquisitions increases rotation errors.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JE is employee of Planmed Oy.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Amsterdam Movement Sciences (AMS) institute.