
Abstract
Background
Mammographic features of calcifications on mammograms showing invasive breast cancer are associated with survival. Less is known about mammographic features and progression to invasive breast cancer among women treated for ductal carcinoma in situ (DCIS).
Purpose
To investigate mammographic features of calcifications in screen-detected DCIS in women who later did and did not get diagnosed with invasive breast cancer.
Material and Methods
This registry-based nested case-control study analyzed data from women with screen-detected DCIS in BreastScreen Norway, 1995–2016. Within this cohort of women with DCIS, those who were later diagnosed with invasive breast cancer (cases) were matched (1:2) to women who were not diagnosed with invasive breast cancer (controls) after their DCIS and by the end of 2016. Information on mammographic features were collected by a national radiological review, where screening mammograms were reviewed locally at each of the 16 breast centers in Norway. We used conditional logistic regression analysis to estimate associations between mammographic features of calcifications in the DCIS mammogram and the risk of subsequent invasive breast cancer.
Results
We found a higher risk of invasive breast cancer associated with fine linear branching (casting) morphology (odds ratio 20.0; 95% confidence interval [CI] 2.5–158.9) compared to fine linear or fine pleomorphic morphology. Regional or diffuse distribution showed an odds ratio of 2.8 (95% CI 1.0–8.2) compared to segmental or linear distribution.
Conclusion
Mammographic features of calcifications in screen-detected DCIS were of influence on the risk of invasive breast cancer. Unfavorable characteristics of DCIS were fine linear branching morphology, and regional or diffuse distribution.
Keywords
Introduction
Ductal carcinoma in situ (DCIS) represents neoplastic proliferation of epithelial cells confined within the basement membrane of the ductal-lobular system of the breast and is considered a non-invasive precursor of breast cancer (1,2). Current standard treatment for DCIS includes surgical excision with or without radiotherapy (1–3). Women are typically diagnosed with DCIS with screening mammography rather than a palpable or symptomatic lesion (2–4). The incidence of DCIS has increased substantially in the western world in recent decades (4,5). The incidence of DCIS in Norway increased from 4 to 11 per 100,000 women-years from 1993 to 2007 in parallel with the implementation of the population-based screening program, BreastScreen Norway (6).
A previous study estimated a 3.8-fold increased long-term risk of a subsequent ipsi- or contralateral invasive breast cancer among women with a prior in situ lesion diagnosed and treated in BreastScreen Norway 1995–2016, compared to women screened negative (7). Other studies, both from Norway and internationally, have indicated a two- to ninefold increased risk of invasive breast cancer for women diagnosed and treated for DCIS compared to women in the general population (8–12). The overall survival among women treated for DCIS is excellent, and this statistic has introduced a concern that an unknown proportion of women diagnosed with DCIS could have been overdiagnosed and, more importantly, overtreated (4,5). A prerequisite to address the issue of overtreatment is to identify distinct criteria or markers to differentiate lesions less likely or likely to progress (1,2).
Morphology and distribution of calcifications on screening mammograms are predictors of malignancy existence (13–15). Further, risk of diagnostic upstaging to invasive breast cancer among women who had a core needle biopsy with DCIS was associated with preoperative mammographic features (16–20). Suspicious calcifications are present in 60%–95% of DCIS diagnosed (21–24). Mammographic features of calcific DCIS were associated with histologic grade, lesion diameter, subtype, estrogen, and HER2 receptor status (3,21,25–27).
Several studies have reported associations between survival and mammographic features of calcifications on mammograms showing invasive breast cancer (13,28–31). Less is known about associations between mammographic features of calcifications and long-term risk of progression to invasive breast cancer among women diagnosed and treated for DCIS. Among women aged 44 years and older who did not undergo surgical resection for ≥1 year after diagnosis of DCIS, progression to invasive disease was more frequent in high-grade DCIS, in lesions with calcifications, and among the younger women (23). Mammographic features have been suggested as a potential biomarker of DCIS recurrence (22,32).
High-quality registry data from BreastScreen Norway and the Cancer Registry of Norway (CRN) allowed us to design a case control study to investigate the potential of descriptors of calcifications on screening mammograms showing DCIS to serve as a marker for increased long-term risk of invasive breast cancer. In this study, we let the term “breast cancer” refer to invasive breast cancer, and the phrase “risk of breast cancer” refer to long-term risk of progression to invasive breast cancer.
The aim of the present study was to investigate mammographic features of calcific screen-detected DCIS among women who later did and did not get diagnosed with breast cancer.
Material and Methods
We designed a matched case-control study using individual level data on women who attended BreastScreen Norway, 1995–2016. BreastScreen Norway is a population-based screening program for breast cancer, administered by the CRN. The program offers approximately 650,000 women aged 50–69 years biennial two-view digital mammographic screening. The participation rate for each screening round is approximately 75%, whereas 84% of invited women attended at least once during 1995–2016 (33).
We identified all participants diagnosed with screen-detected DCIS during the study period, 1995–2016 (n = 3019). Within this cohort, we conducted a nested case-control study as follows. Women diagnosed with breast cancer >6 months after the diagnosis of DCIS and by the end of 2016 were defined as cases (n = 200 women). Bilateral DCIS was considered a single case. Each case was matched to two women (controls) who had not been diagnosed with breast cancer after DCIS by the end of 2016 (Fig. 1). The controls were matched on calendar year (±1 year) and residential municipality at time of DCIS diagnosis, and they were sampled with replacement. Radiological review was performed by breast radiologists locally at the 16 breast centers in Norway, blinded to the outcome (breast cancer). The radiologists were specifically instructed to complete the review of the screening mammograms showing DCIS before accessing any follow-up information including results from the one-year follow-up screen.
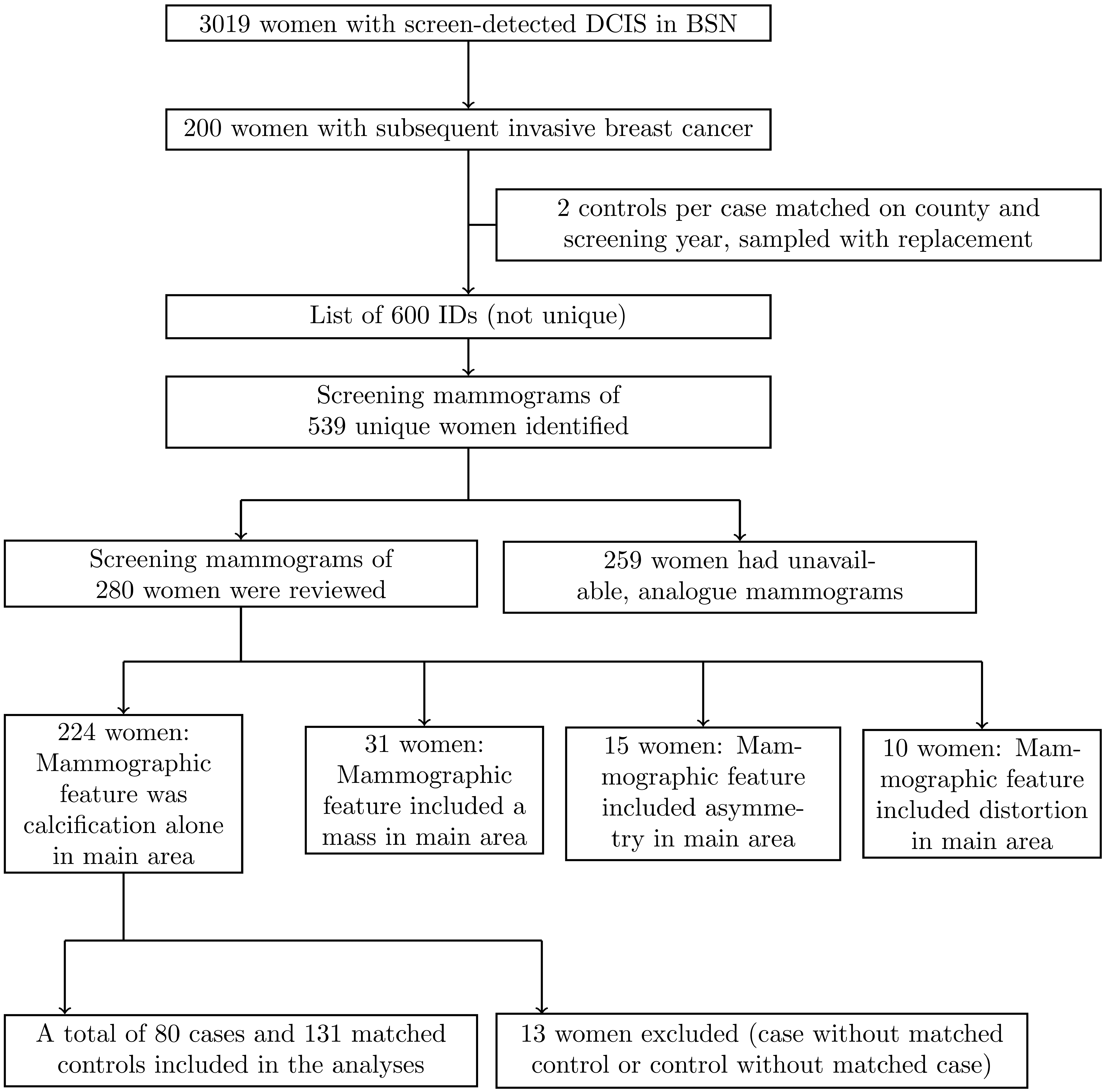
Flow chart describing the selection of the study population.
The transition from screen film mammography (SFM) to full field digital mammography (FFDM) was gradually implemented in BreastScreen Norway from 2000 to 2011. We aimed to include all cases regardless of screening equipment, to allow for review of SFM when available. As controls were matched to cases on county and calendar year, this ensured that most triplets (each case with its two matched controls) had screening mammograms from similar technical equipment.
The regional ethical committee approved the study (No. 2012/576b).
Radiological review
The American College of Radiology Breast Imaging Reporting and Data System (BI-RADS®) lexicon 5th edition was used to classify all mammographic findings with respect to: Mammographic density (BI-RADS® type a, b, c, or d), focality (whether there was one or more lesions in the breast), mammographic diameter, location (laterality, quadrant, and depth), and mammographic features (calcifications, masses, asymmetries, and architectural distortions). Calcifications were further described by morphology and distribution according to the BI-RADS® 5th edition standardized breast image reporting (34).
The radiological review was performed locally at each of the 16 breast centers in Norway. Review forms with a multiple-choice design were individually marked with the ID of the woman and invitation number for the examination where DCIS initially was diagnosed. Paper forms were mailed in bulk to a dedicated and responsible radiologist at each of the breast centers. After reviewing each set of screening mammograms, completed forms were returned to the CRN where results were manually coded, stored, and merged with data from the CRN before they were made available for analyses.
Study population
The initial collection of cases and matched controls comprised 539 unique women (200 cases and 340 controls) (Fig. 1). Controls were sampled with replacement and some women were selected as a control for more than one case. We received completed review forms for all 207 women (100%) with DCIS detected on FFDM screening mammograms, and for 73 of 332 women (22%) with DCIS detected on SFM. In total, we received completed review forms for 51.5% of all cases and 52.0% of all controls. Of 16 breast centers in Norway, 15 reviewed 3–73 mammograms each showing DCIS. One center had cases screened with SFM only and was not included in the study as they did not return any completed review forms (SFM mammograms were not available). We excluded information from 16 of the cases (16%) and 44 of the controls (21%) whose mammographic features of the main (largest if multifocal or multicentric) DCIS lesion included a mass, distortion, or asymmetry. From the collection of women with available information, the final study sample consisted of all cases with at least one matched control, and their 1–2 matched controls with available information per case. This resulted in a study population of 80 cases and 131 matched controls whose mammographic findings of the main DCIS lesion were based purely on calcifications alone (Fig. 1). The mean follow-up time was 5.2 years after the diagnosis of DCIS (time from diagnosis of DCIS to the diagnosis of invasive breast cancer among the cases).
Statistical analysis
Descriptive analyses were used to identify differences in distribution of mammographic features in DCIS with and without a subsequent breast cancer. Descriptive statistics were presented as frequencies, proportions, and median with interquartile range (IQR).
Conditional logistic regression models were used to obtain odds ratios (ORs) as measures of relative risk of breast cancer associated morphology and distribution of calcifications on the screening mammograms. The conditional model ensures that the matching factors are adjusted for (county, screening year). We adjusted for the following potential confounders: age, focality, mammographic density, treatment for DCIS, and technical equipment for mammography (SFM vs. FFDM).
We performed several sensitivity analyses. Conditional logistic regression analyses were repeated restricted to women screened with FFDM, women with a unilateral diagnosis of DCIS and women with DCIS treated with breast conserving treatment, respectively.
Data preparation and analyses were performed using Stata version (StataCorp, College Station, TX, USA). We used a two-sided statistical significance level of 0.05.
Results
The study sample consisted of 80 cases and 131 matched controls whose mammographic features of the DCIS were purely calcifications in the main area (Fig. 1). The median time from screen-detected DCIS to breast cancer was 55 months (IQR = 28–85 months). Among the cases with unilateral DCIS and whose subsequent breast cancer had available information regarding laterality, 48% of the 52 women treated with breast conserving surgery and 24% of the 21 women treated with mastectomy were diagnosed with breast cancer in the ipsilateral breast.
The cases and controls were similar with respect to age and mammographic density, and their DCIS showed a similar distribution with respect to mammographic size, location in the breast, histologic grade, and screening equipment used for detection (Table 1). When comparing cases and controls on morphology of calcifications on the initial DCIS diagnostic image, images from cases were more likely to display coarse heterogeneous and, in particular, fine linear branching morphology. Case images were less likely than control images to display fine linear or fine pleomorphic morphology (Table 2). With regards to the distribution of calcifications, case images showed more regional or diffuse distribution of the calcifications than control images, and less linear or segmental distribution. The cases and controls were similar with respect to distribution of primary surgery, however with a higher proportion of reoperations among cases compared to controls (Supplemental Table 1).
Age at diagnosis, mammographic density, prevalence, size, location, and grade of screen-detected DCIS among 80 cases and 131 controls.
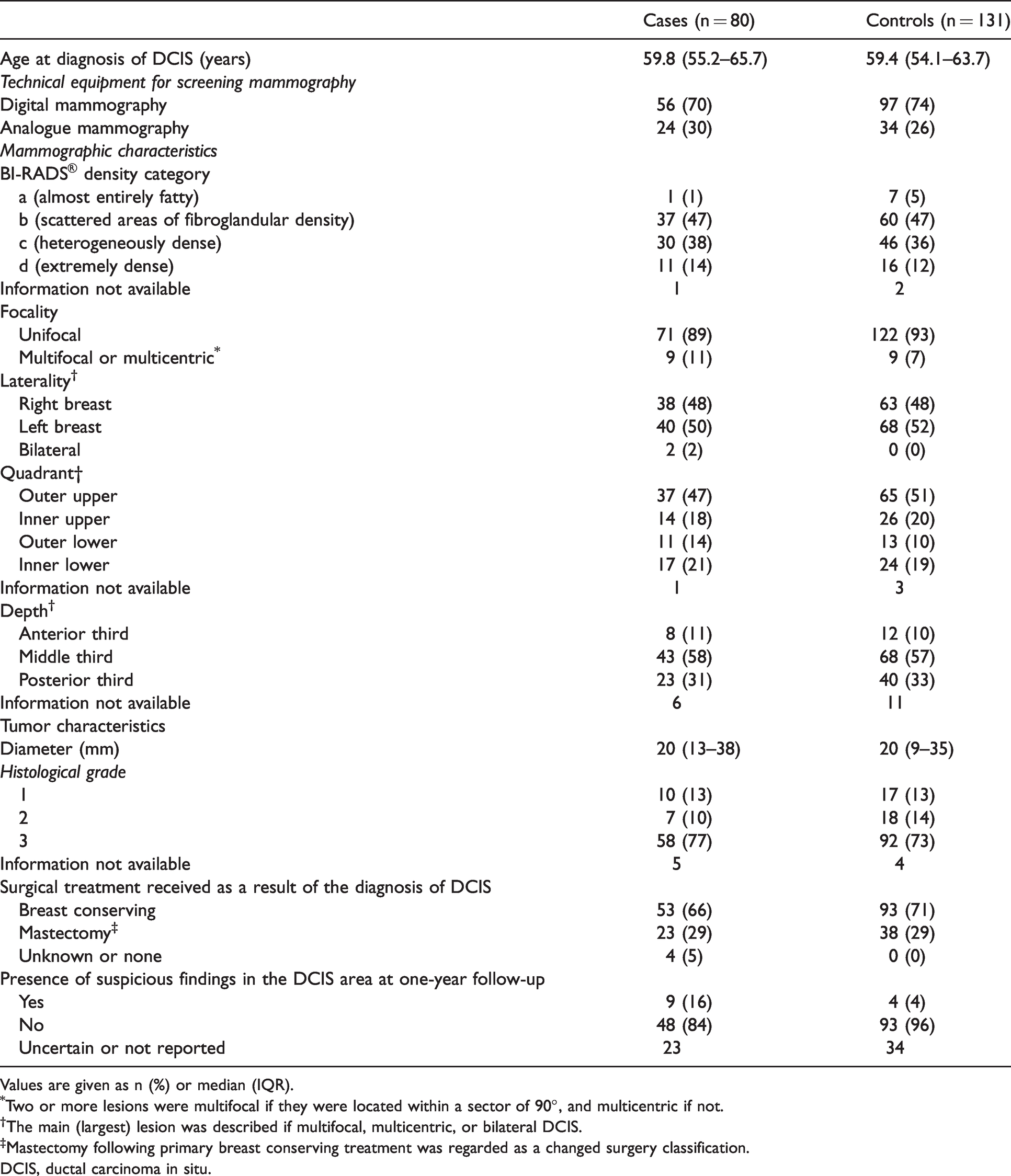
Values are given as n (%) or median (IQR).
*Two or more lesions were multifocal if they were located within a sector of 90°, and multicentric if not.
†The main (largest) lesion was described if multifocal, multicentric, or bilateral DCIS.
‡Mastectomy following primary breast conserving treatment was regarded as a changed surgery classification.
DCIS, ductal carcinoma in situ.
Mammographic features of the main (largest, if multifocal or multicentric) lesion of screen-detected DCIS, according to BI-RADS®.
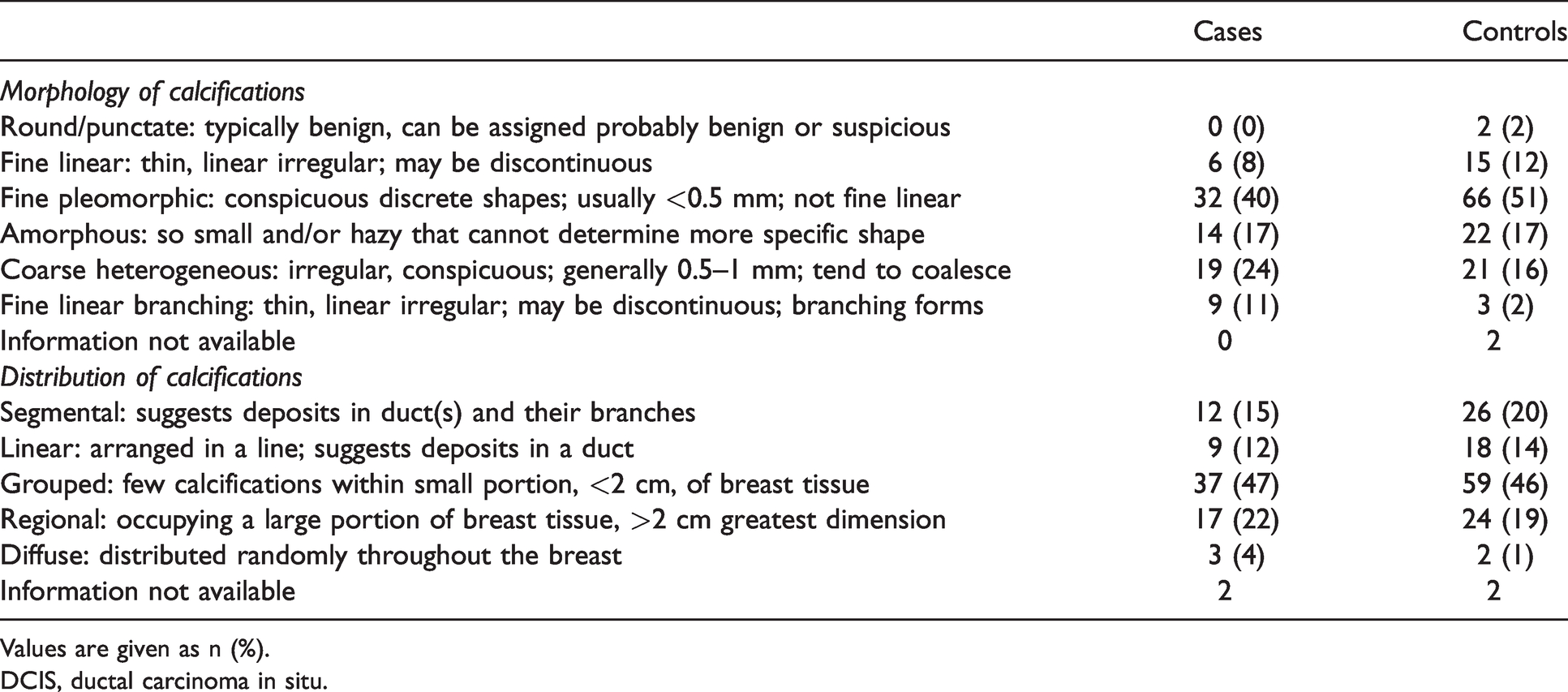
Values are given as n (%).
DCIS, ductal carcinoma in situ.
One year after diagnosis of DCIS, there were no diagnoses of DCIS or breast cancer. However, while 96% of controls with available information had no suspicious findings in the prior DCIS area at the one-year follow-up screen, the same was true for 84% of the cases.
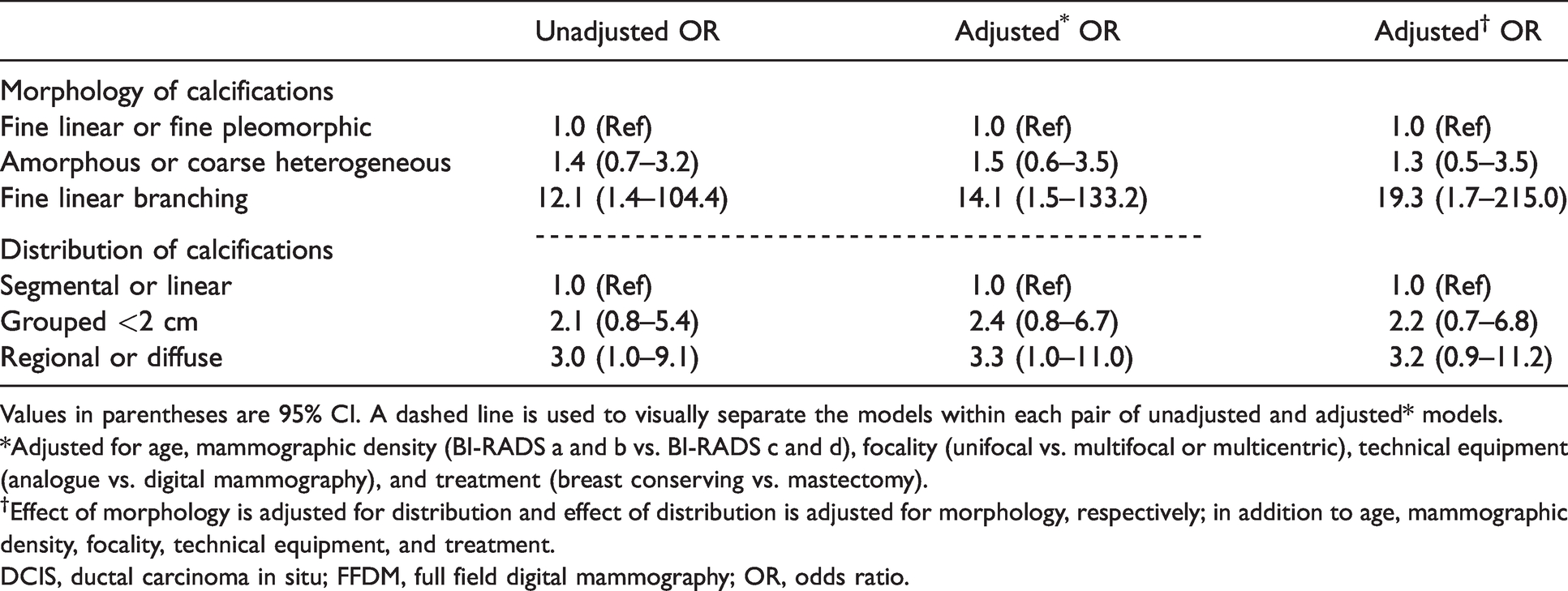
Fine linear branching calcification morphology was associated with a 20-fold increased risk of breast cancer (OR = 20.0, 95% CI = 2.5–158.9) compared to fine linear or fine pleomorphic calcification morphology (Table 3). Compared to a segmental or linear distribution of calcifications, a grouped distribution was associated with a suggestive twofold increased risk of breast cancer (OR = 1.9, 95% CI = 0.7–5.0) and a regional or diffuse distribution was associated with a threefold increased risk of breast cancer (OR = 2.8, 95% CI = 1.0–8.2). Separate ORs for each BI-RADS category concerning suspicious morphology of calcifications are listed in Supplemental Table 2. Several sensitivity analyses confirmed our conclusions (Table 4, Supplemental Tables 4 and 5). Mammographic features of screen-detected DCIS were of influence on the risk of diagnosis of invasive breast cancer.
OR of a subsequent invasive breast cancer associated with mammographic features of calcification of screen-detected DCIS, among 80 cases and 131 controls.
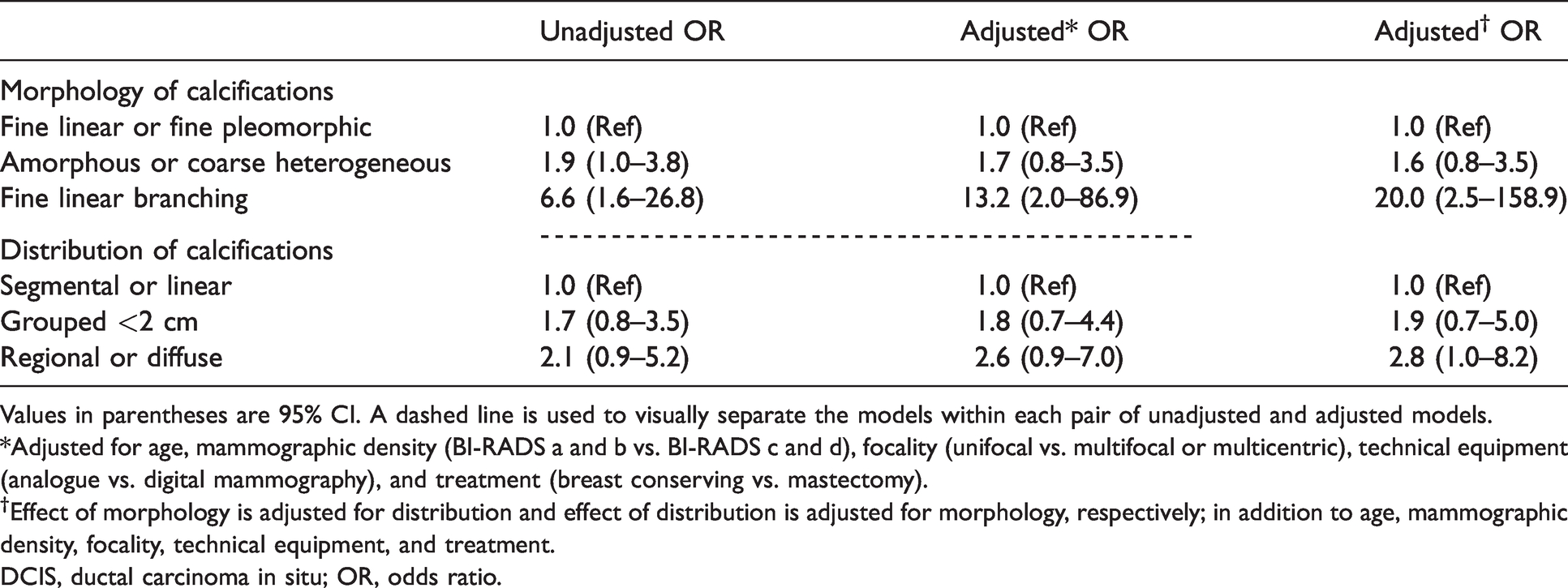
Values in parentheses are 95% CI. A dashed line is used to visually separate the models within each pair of unadjusted and adjusted models.
*Adjusted for age, mammographic density (BI-RADS a and b vs. BI-RADS c and d), focality (unifocal vs. multifocal or multicentric), technical equipment (analogue vs. digital mammography), and treatment (breast conserving vs. mastectomy).
†Effect of morphology is adjusted for distribution and effect of distribution is adjusted for morphology, respectively; in addition to age, mammographic density, focality, technical equipment, and treatment.
DCIS, ductal carcinoma in situ; OR, odds ratio.
OR of a subsequent invasive breast cancer associated with mammographic features of calcification of screen-detected DCIS, in a sensitivity analysis restricted to women screened with FFDM.
Values in parentheses are 95% CI. A dashed line is used to visually separate the models within each pair of unadjusted and adjusted* models.
*Adjusted for age, mammographic density (BI-RADS a and b vs. BI-RADS c and d), focality (unifocal vs. multifocal or multicentric), technical equipment (analogue vs. digital mammography), and treatment (breast conserving vs. mastectomy).
†Effect of morphology is adjusted for distribution and effect of distribution is adjusted for morphology, respectively; in addition to age, mammographic density, focality, technical equipment, and treatment.
DCIS, ductal carcinoma in situ; FFDM, full field digital mammography; OR, odds ratio.
Discussion
We estimated an increased risk of breast cancer among women whose diagnostic DCIS image displayed fine linear branching calcifications, with up to 20-fold increased risk in adjusted estimates. However, the number of cases and controls is small and the confidence interval is wide. Compared to fine linear morphology, the estimated risk was 1.5–2-fold for amorphous or coarse heterogeneous calcifications (not statistically significant). We also observed a 2–3-fold increased risk associated with regional or diffuse distribution of calcifications on the screening mammogram. The risk did not vary with location of the prior DCIS, and we did not observe a statistically significant increased risk associated with mammographic density. The higher proportion of reoperations among cases could indicate an increased complexity associated with complete excision of DCIS among the cases, which could have explained an increased risk of subsequent invasive disease.
To the best of our knowledge, no previous study has assessed risk of progression to breast cancer by several BI-RADS® descriptors of calcifications on screen-detected DCIS. Mammographic features (morphology of calcifications) did not predict recurrence of either in situ or invasive lesions in a cohort of women with DCIS, followed for an average of 15 years (35). In a cohort of 1657 women treated for DCIS, the overall local recurrence rate was low, and dense breast tissue and fine linear (branching) calcifications were associated with increased risk of local recurrence (22). Our results can be related to several studies showing decreased survival associated with fine linear branching morphology of calcification among women diagnosed with either DCIS or breast cancer (24,28–31). In fact, Tabár et al. (29) have called for additional research on optimal treatment strategies for breast cancer presenting with “casting” (e.g. fine linear branching) calcifications. Similar to our study, a previous study did not detect any associations between the location of the DCIS and the risk of a subsequent breast cancer (36).
We performed our analyses of relative risk of breast cancer after a screen-detected DCIS on an individual level. We chose to assess long-term relative risk of breast cancer from six months after a diagnosis of DCIS regardless of laterality of the diagnoses and whether the diagnoses were unilateral or bilateral. Thus, our study is not designed to differentiate between disease as a result of progression of a local residue of the treated DCIS lesion and increased risk of a new lesion due to biologic predisposition. From the woman’s perspective, the laterality of the subsequent breast cancer diagnosis is likely of less importance in the face of a diagnosis of invasive cancer and the treatment of a second breast cancer.
The multistep model of human breast cancer progression indicates progression through sequential stages, from premalignant hyperplastic breast lesions with or without atypia to carcinoma in situ (DCIS or lobular carcinoma in situ [LCIS]) to invasive carcinoma (1,2). Two main sub-models explain the place of DCIS in the development of breast cancer. In the linear progression model, low-grade DCIS progress to high-grade DCIS and “dedifferentiates” to become invasive breast cancer. In the parallel disease model, low-grade DCIS tends to progress to low-grade invasive ductal carcinoma, and high-grade DCIS tends to progress to high-grade invasive ductal carcinoma (1). There is consensus that neither sub-model represents the full truth; however, in combination they illustrate the diverse reality of breast tumor progression and the challenge in interpreting the results of this study.
Variability in risk of progression to breast cancer after treatment for DCIS could be related to several factors. Intuitively, there could be variability in the inherent potential of biologic drivers of progression between lesions; there might be a subclass of DCIS lesions which impede complete excision, or additional modalities of treatment (e.g. radiotherapy) could be more or less effective on certain subclasses of DCIS lesions. A subclass of DCIS defined by the presence of a mammographic feature could be more (or less) heterogeneous than the subclass we compare it to, and each subclass could contain sub-subclasses of both increased and decreased risk. Heterogeneity could be biological, radiological, or a combination. Specifically related to the results of our study, the “fine linear” calcification morphology is less specific in its definition compared to “fine linear branching,” resulting in a higher potential for within-group variation.
Our results on effect of primary DCIS treatment are in line with another study: An increased risk of a breast cancer after DCIS was observed both in women treated with breast conserving surgery and in those treated with mastectomy (12). Whether the breast cancer is diagnosed in the ipsi- or contralateral breast compared to the DCIS, might indicate different mechanisms behind its progression. Most women with a DCIS are not diagnosed with breast cancer, and women treated for DCIS have a long-term disease-free survival of 96%–98% (8). Concerns related to overdiagnosis and overtreatment have initiated groundbreaking trials of active surveillance among women with non-high-grade DCIS: the LORIS trial (UK) (37); the LORD trial (Belgium and Netherlands) (38); the COMET trial (US) (39); and the Loretta trial (Japan) (40). There is, however, an ongoing debate regarding the active surveillance trials, concerning whether the inclusion criteria will succeed in identifying a population of sufficiently low risk of progression (3,41–44).
One of the women in our study refused treatment of her bilateral DCIS. A sensitivity analysis excluding the two women with bilateral DCIS did not change our conclusions. In a sensitivity analysis excluding women with DCIS detected with SFM, the association between the distribution of calcifications and the risk of progression to breast cancer remained similar. Remember that we received completed review forms for all women (100%) with DCIS detected on FFDM screening mammograms, so there is no risk of selection bias related to mammograms not available for review in this subsample. The associations between morphology and the risk of breast cancer appeared stronger among the women whose DCIS was detected by FFDM (Table 4, Supplemental Table 3).
The strengths of this study included the long follow-up within the cohort (1995–2016). Furthermore, all cancer cases are reported by law to the CRN (45), which ensures complete data inclusion. A limitation of the study was the small sample size, which precluded more detailed comparisons across variables, and resulted in considerable uncertainty of the estimates. Further, as the review of mammograms were performed locally with relatively few cases per breast center, our study might suffer from some inter-variability between radiologists regarding evaluation of BI-RADS descriptors. Our results should be interpreted carefully given the low number of cases and controls. The radiologic review allowed us to assess several variables not accessible in a study limited to routinely registered data from the CRN. In addition, all cases and controls were reviewed based on established BI-RADS® 5th edition criteria (34), enabling more uniform evaluations based on updated and current knowledge.
In conclusion, the mammographic features of screen-detected DCIS were associated with risk of invasive breast cancer in this study. Unfavorable characteristics of DCIS were fine linear branching morphology of calcifications, and regional or diffuse distribution of calcifications on the screening mammograms. Further research, including larger sample sizes, is definitely needed to verify our findings and to obtain more precise estimates. Combining information about mammographic features of calcifications with histological subtypes of DCIS, or to established risk factors for breast cancer, would bring additional and valuable insight in future research. Uncertainty remains in understanding whether mammographic features can help guide optimal treatment, ranging from the option of active surveillance to various intensified treatments of screen-detected DCIS.
Supplemental Material
sj-pdf-1-acr-10.1177_02841851211006319 - Supplemental material for Patterns of aggressiveness: risk of progression to invasive breast cancer by mammographic features of calcifications in screen-detected ductal carcinoma in situ
Supplemental material, sj-pdf-1-acr-10.1177_02841851211006319 for Patterns of aggressiveness: risk of progression to invasive breast cancer by mammographic features of calcifications in screen-detected ductal carcinoma in situ by Marie Lilleborge, Ragnhild S Falk, Tone Hovda, Marit M Holmen, Giske Ursin and Solveig Hofvind in Acta Radiologica
Footnotes
Acknowledgments
The authors are immensely grateful for the efforts of the radiologists at each of the 16 local breast centers of BreastScreen Norway in locally reviewing a total of 249 screening mammograms showing DCIS: Østfold Hospital Trust (Marit Almenning Martiniussen, Merete Kristiansen), Akershus University Hospital (Maryam Lahooti, Mahboobeh Piadeh, Khalida, Nasreen Chaudhrey, Manouchehr Seyedzadeh, Joana Reis), Oslo University Hospital (Marit Muri Holmen, Tatjana Samardzic), Innlandet Hospital Trust division Lillehammer (Lars Hagen Henriksen), Vestre Viken Hospital (Hilde Bjørndal and Linda Romundstad), Tønsberg Hospital, Vestfold (Judy Lynn Albertsen, Marte Myrebøe Schulze), Telemark Hospital (Marit Solveig Bekken, Anne-Lina Fjellhøy, Beatrice Ruger), Sørlandet hospital, Kristiansand (Helene Sandvik Solli, Gunn Aagedal Hervold), Stavanger University Hospital (Siri Fagerheim), Haukeland University Hospital (Silje Kathrin Gjelseng Viga-Berge, Signe Johnsen Landa, Åsmund Lyngøy), Førde Hospital (Zsolt Richard Francziszty, Bernadett Hrabovszky), Møre og Romsdal Hospital Trust (Solveig Roth Hoff, Fride Tennebø), St. Olavs Hospital, Trondheim University Hospital (Håkon Lund-Hanssen), Nordland Hospital Trust Bodø (Heinrich Backmann, Enno Rodegerdts), University Hospital of North Norway (Rica Mortensen). The authors are also grateful to Morten Olsen at the Cancer Registry of Norway who shared the workload with the first author (ML) in digitally coding the results of the review from paper forms. The authors would like to thank the BreastScreen Norway’s specialist group on radiology and our multidisciplinary project group “Premalignant lesions in the breast” for valuable input.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received the following financial support for the research, authorship, and/or publication of this article: The work was funded by The Norwegian Cancer Society (grant no. 5746604). The funding source did not contribute to the design or conduct of the study, nor to the writing or submission of this manuscript. The ideas and opinions expressed herein are those of the authors, and endorsement by the Cancer Registry of Norway and the Norwegian Cancer Society is not intended nor should be inferred.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.