
Abstract
Background
Lipoma arborescens is characterized by the villous proliferation of the synovium and diffuse hyperplasia of fatty tissue in the subsynovial layer, almost always with a periarticular lesion. According to past articles, fewer cases have depicted the imaging features of lipoma arborescens.
Purpose
To evaluate the computed tomography (CT) and magnetic resonance imaging (MRI) features of lipoma arborescens.
Material and Methods
The imaging features of 15 patients with pathologically proven lipoma arborescens were retrospectively analyzed including lesion number, shape, location, size, margins, attenuation on CT, and signal intensity and enhancement patterns on MR images.
Results
All cases (n=15) showed joint or bursa effusion. The primary lesion attached to the bursa wall adjacent to the bone in 13 cases and to the lateral wall in two cases. CT shows a mass with fatty tissue attenuation values in the suprapatellar pouch (n=3) or subdeltoid bursa with an erosion of the humeral head (n=2), among them two cases showed branched slightly high density in the center of the fat density tissue. Fifteen cases on routine MRI display mass-like subsynovial mass with fatty tissue signal on all of the sequences and suppression of the signal on fat-suppression sequences. Among them, five lesions showed branched slightly low T1-weighted imaging, high proton density-weighted imaging, and T2-weighted imaging signals in the center. It showed the enhancement of the linear surface and the bursa wall in contrast-enhanced MRI (n=3).
Conclusion
Lipoma arborescens have specific CT and MRI features that enable them to make a conclusive diagnosis of this rare condition, which helps the diagnosis before treatment.
Introduction
Lipoma arborescens is an infrequent non-neoplastic lesion that tends to occur in the synovium lining of joints or bursae, occurring in < 1% of all lipomatous conditions, also called lipomatosis arboresces (1). It is characterized by the villous proliferation of the synovium and diffuse hyperplasia of fatty tissue in the subsynovial layer, almost always with a periarticular lesion. According to past articles, fewer cases have depicted the imaging features of lipoma arborescens, and some are case reports (1–10). The aim of the present study was to assess the magnetic resonance imaging (MRI) and computed tomography (CT) characteristics of lipoma arborescens combined with the pathology and other associated findings.
Material and Methods
Patients
Fifteen patients (seven men, eight women; age range = 16–62 years; mean age = 35.7 years) who were pathologically diagnosed with lipoma arborescens from June 2010 to May 2020 were retrospectively reviewed. The ethics committee of the study hospital provided approval. Nine cases were confirmed by surgery and six were confirmed by puncture biopsy. The images of 15 patients were retrospectively reviewed, including MRI (n = 15), CT (n = 5), and digital radiography (n = 4). There were six cases located in the right knee joint, five in the left knee joint, two in the right shoulder, and two in the left shoulder. There were 11 cases in the suprapatellar bursa of the knee joint and four cases in the bursae subdeltoidea of the shoulder joint. All knee patients showed knee joint swelling and pain; duration was in the range of two weeks to four years. Four cases had a traumatic history. One case had a three-month history of left shoulder joint pain and two patients with right shoulder lipoma arborescens had a mass in the joint for 1–2 years, another asymptomatic lesion of the left shoulder was incidentally discovered on examination.
Imaging techniques
All 15 patients had MRI examinations; T1-weighted (T1W) and T2-weighted (T2W) fast spin echo (FSE) images, and fat-saturated FSE, T2W images, or fat-saturated proton density (FS PD) images were obtained. Three patients underwent gadolinium contrast enhancement using the FS T1W imaging sequence and gadolinium gadodiamide 0.1 mmol/kg intravenous injection. T1W imaging (TR = 300–500 ms, TE = 10–20 ms, field of view [FOV] = 200–400 mm, and matrix = 256–512 × 208–512), FSE T2W imaging (TR = 2500 ms, TE = 100 ms, FOV = 20–40 cm, and matrix = 256–512 × 208–512), and FSE PD imaging (TR = 2200 ms, TE = 30 ms, FOV = 20–40 cm, and matrix = 256–512 × 208–512) were carried out. In all cases, there were images of at least three planes, with the section thickness at in the range of 3–4 mm and the intersection gap in the range of 0.5–1 mm.
Three patients accepted routine CT examinations (matrix = 512 × 512, FOV = 250–400 mm) using the soft-tissue algorithm (section thickness = 5 mm, increment = 5 mm).
Imaging analysis
Two musculoskeletal radiologists blindly observed the lesions for lesion number, shape (villous, frond-like lesions with a narrow base or mound-like lesions with a wide base), location (the main lesion attached to the bursa wall adjacent to the bone or adjacent to the lateral wall), and size. Whether the margins were well-defined or not, the density and homogeneity were analyzed together on CT, and signal intensity and enhancement patterns on MRI were evaluated. For the size assessment, the greatest three-dimensional size was measured for each lesion. Moreover, other associated findings including meniscus degradation, degenerative changes, meniscal tear, joint effusion, discoid meniscus, synovial loose body, synovial cyst, marrow edema tibial plateau, supraspinatus tendon tear, and bony erosion were also recorded.
Results
All patients (n = 15) demonstrated joint or bursa effusion (Figs. 1–15). Nine patients with 12 lesions revealed villous or frond-like lesions with a narrow base (Figs. 1–15), while six patients with seven lesions showed a mound-like lesion with a wide base (Figs. 1–4). The main lesion was attached to the bursa wall adjacent to the bone in 12 cases (Figs. 1–12) and adjacent to the lateral wall in three cases (Figs. 13–15). The three-dimensional size of the villous or frond-like lesions with narrow base lesion were in the range of 4.1 × 11.4 × 10.7 mm–35.2 × 32.4 × 43.9 mm (Figs. 1–15). The lesion’s most extensive base in the mound-like lesion with a wide base was in the range of 4.3–21.9 mm, while the height of the lesion was in the range of 3.9–7.3 mm (Figs. 1–4). All lesions showed well-defined margins (Figs. 1–15).
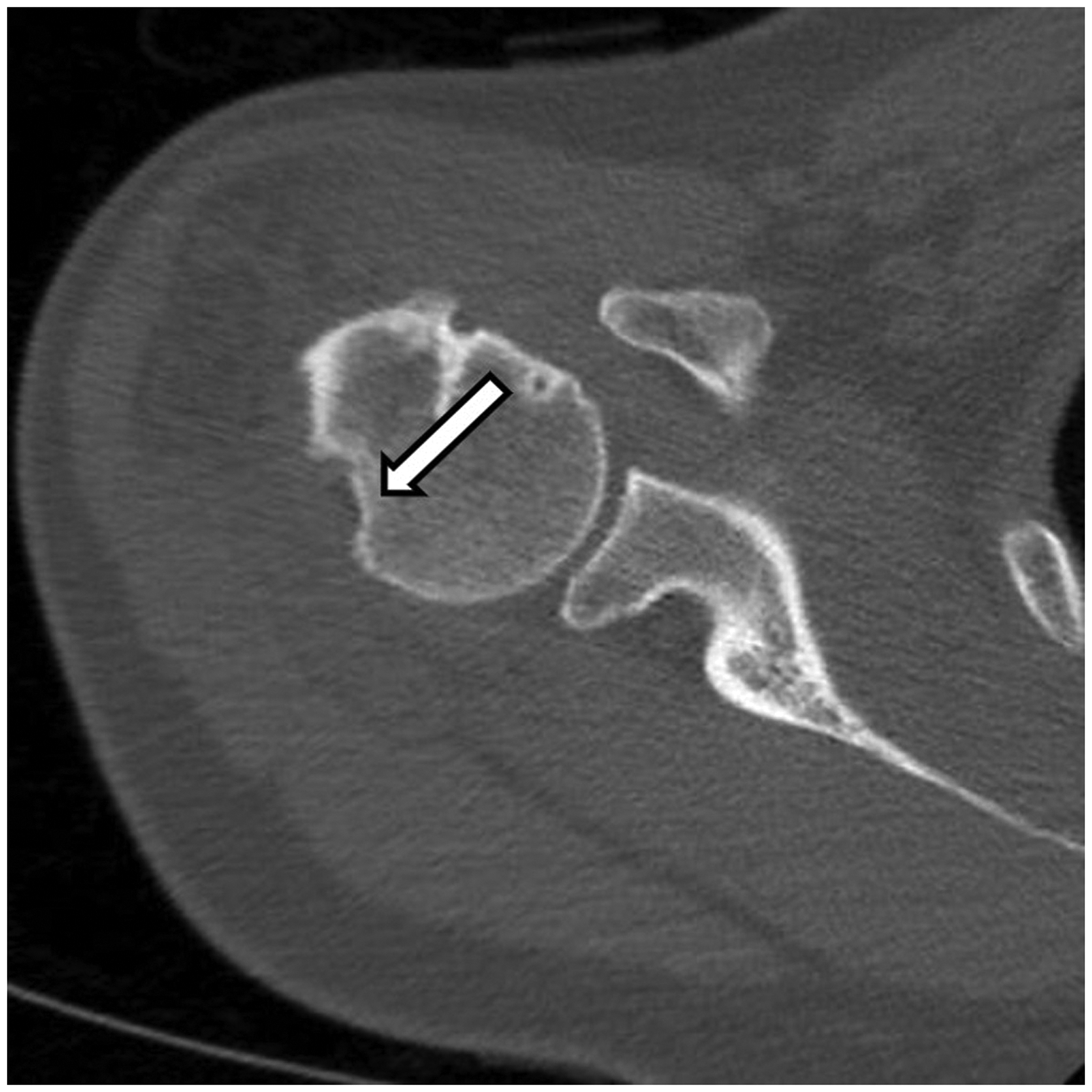
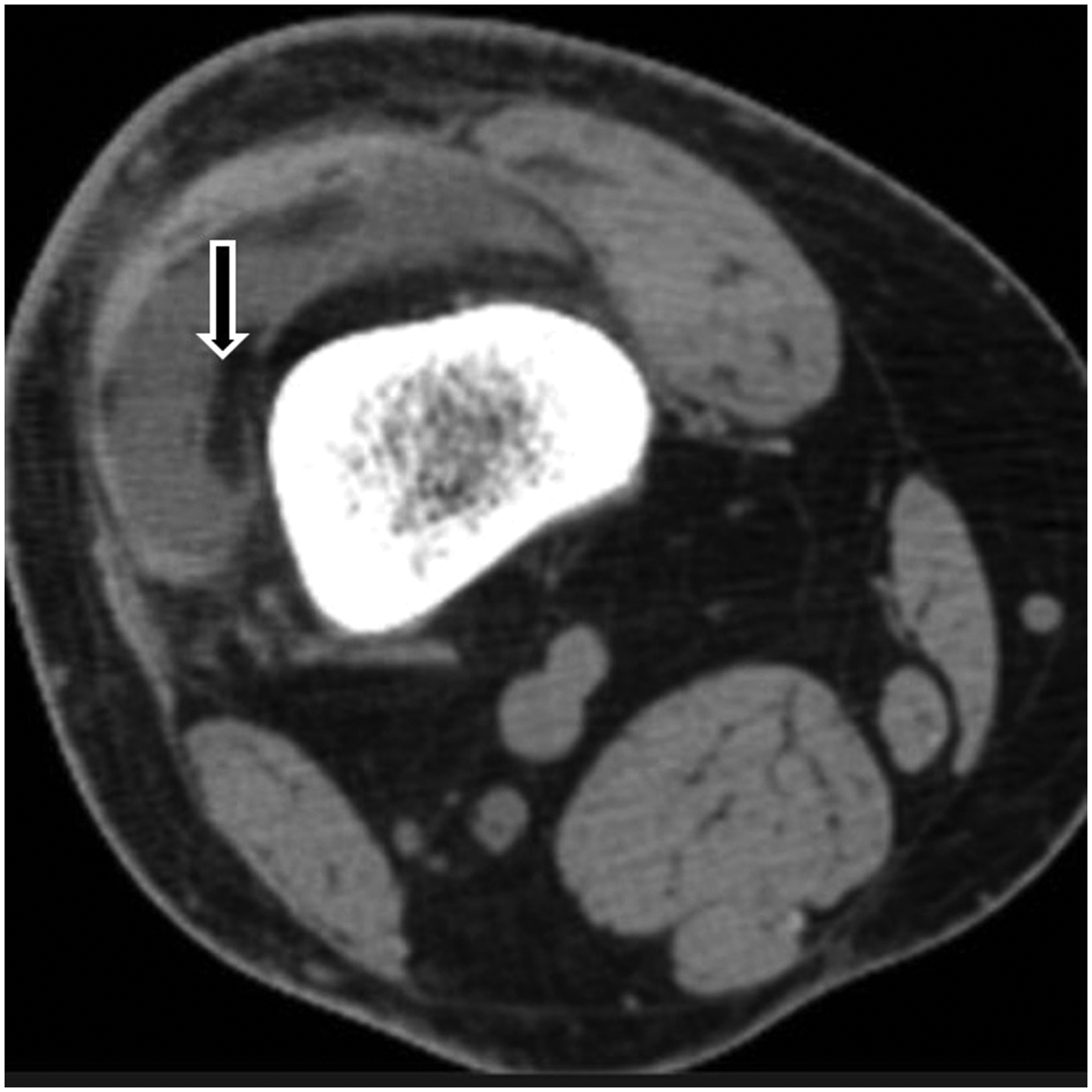
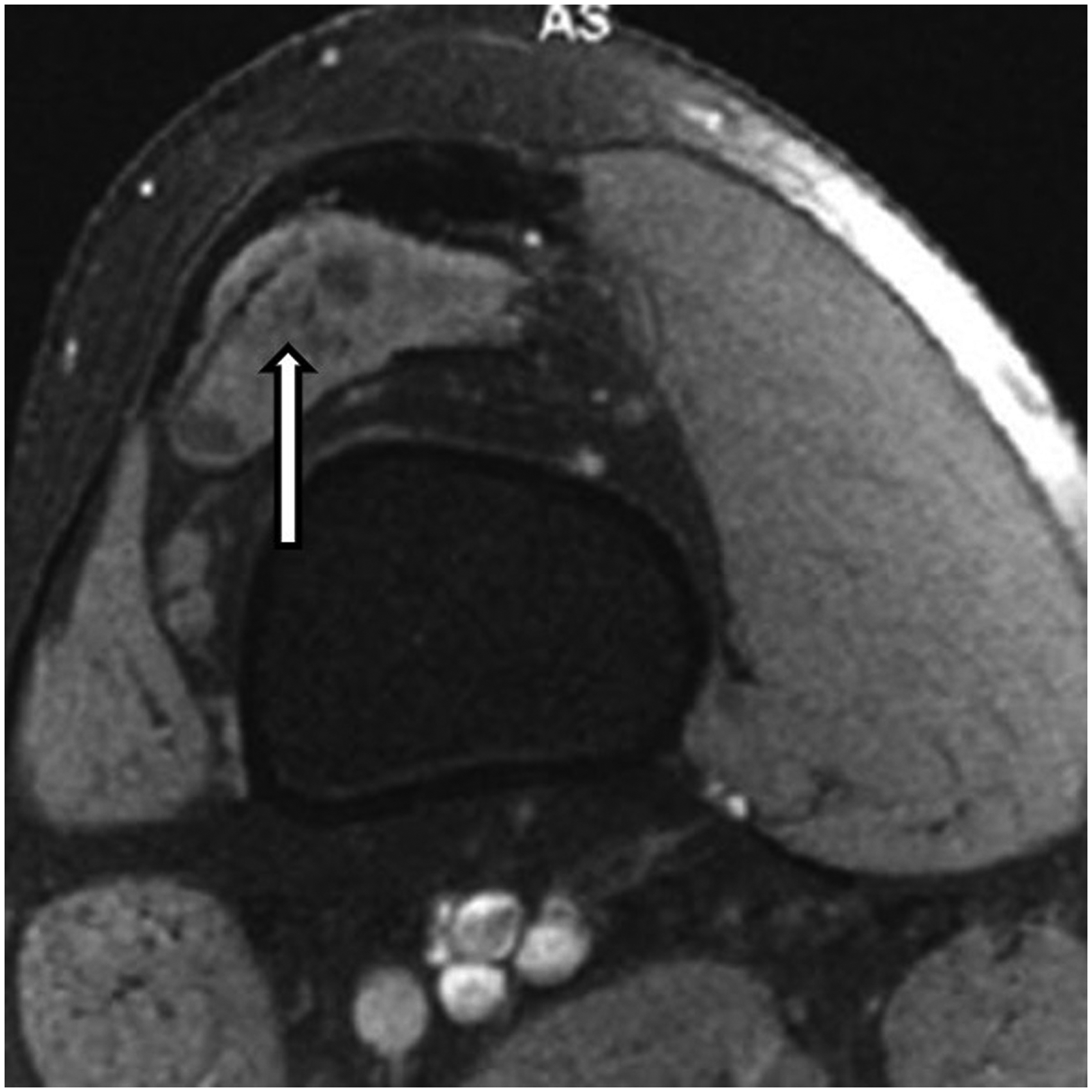
A 34-year-old female patient with lipoma arborescens in the subdeltoid bursa. Non-enhanced computed tomography images of the shoulder. Axial view: bone-window image show large discrete bony erosion of the right humeral head (arrow).
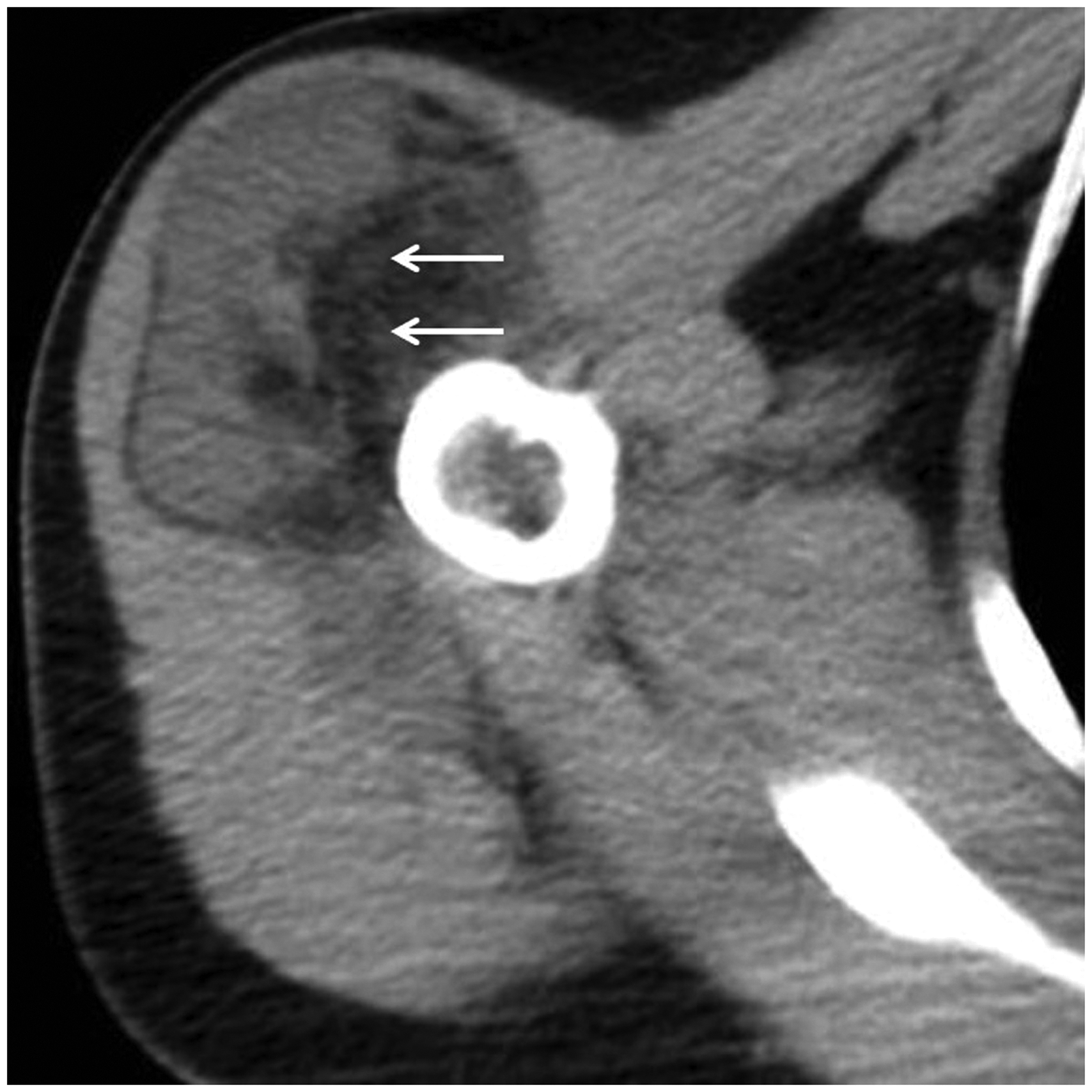
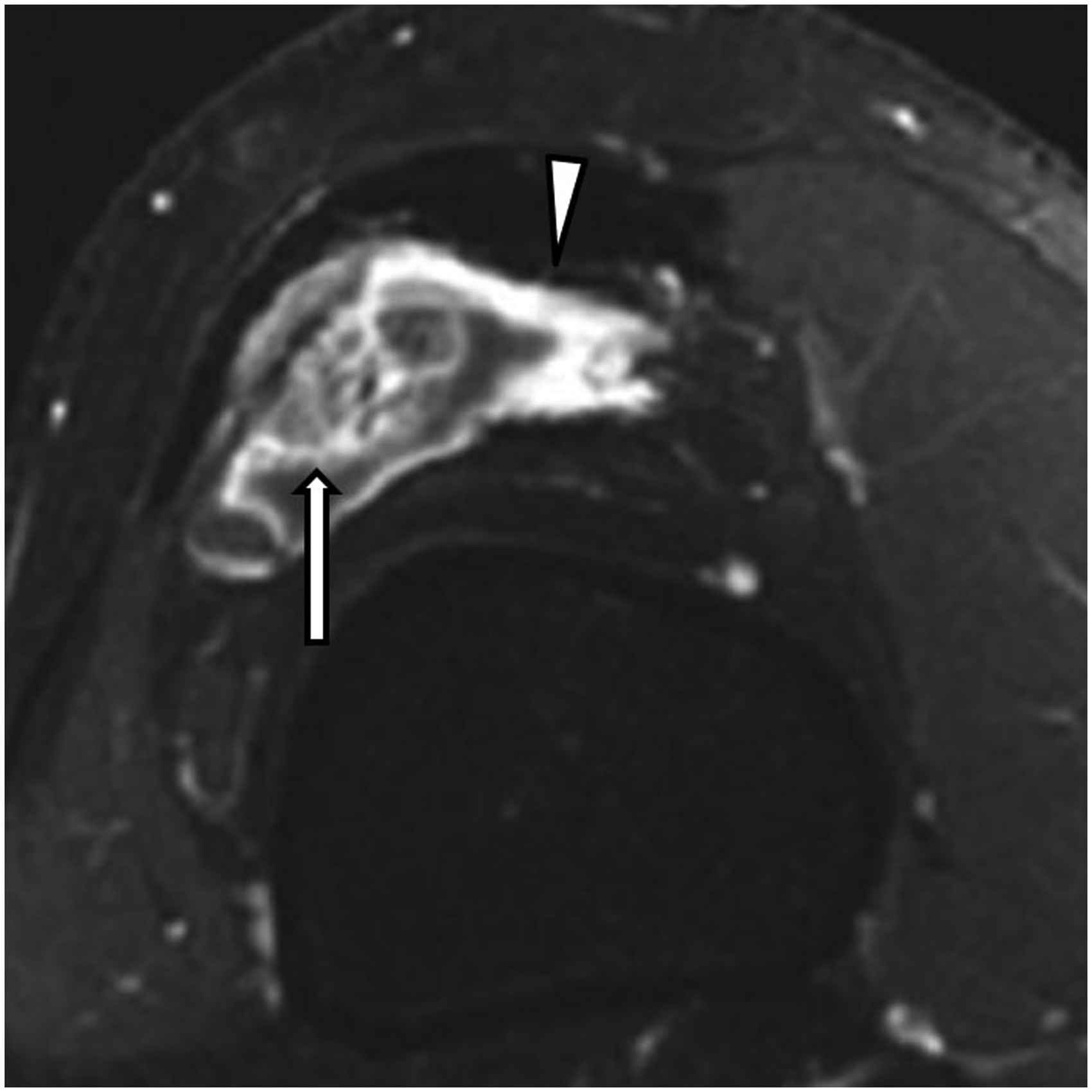
A 34-year-old female patient with lipoma arborescens in the subdeltoid bursa. Non-enhanced computed tomography images of the shoulder. Axial view: soft tissue-window image displays villous frond-like structures with fat density; branches with slightly high density were noted in the center of the fat density tissue (small arrow).

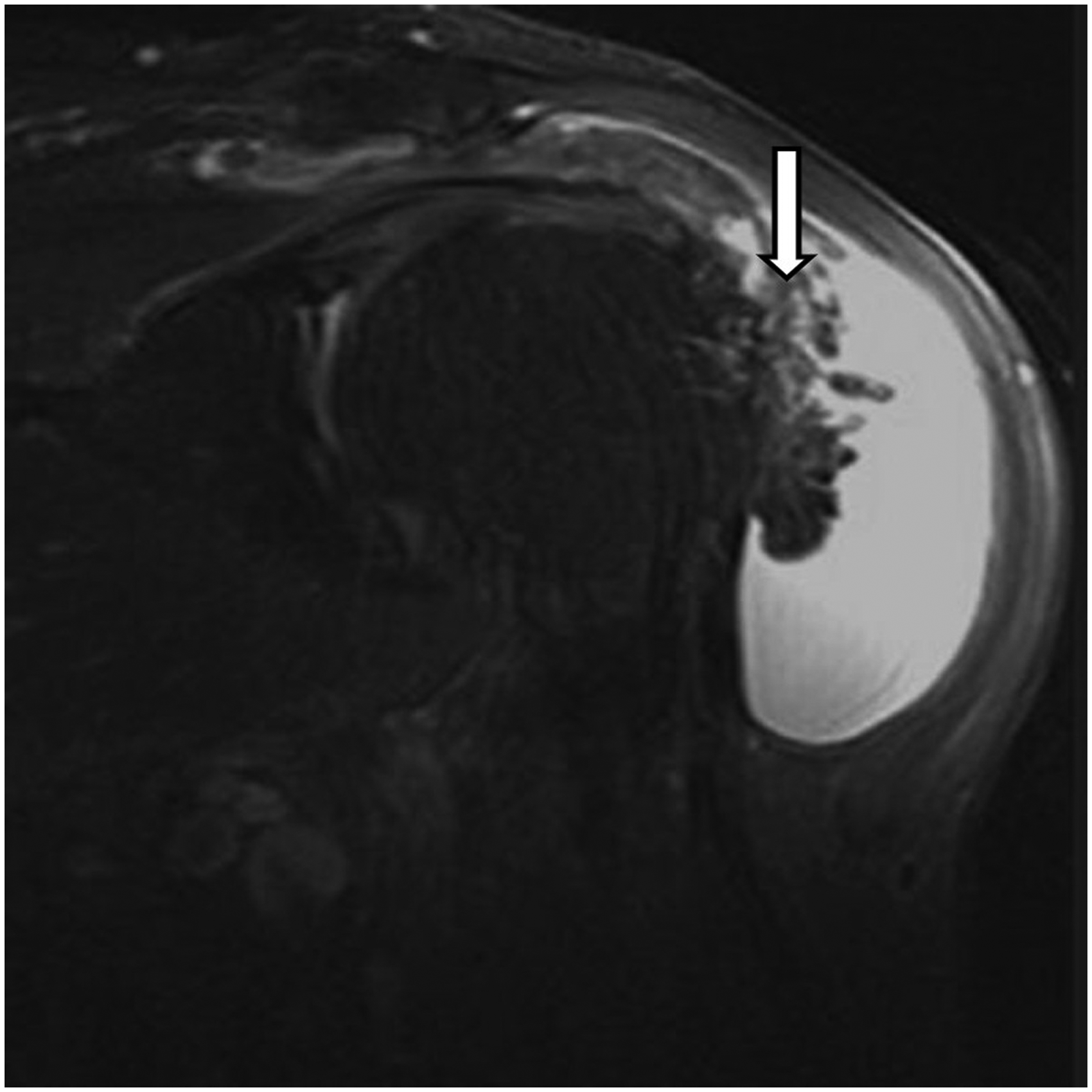
A 34-year-old female patient with lipoma arborescens in the subdeltoid bursa. Coronal T1-weighted image reveal multi-colliculus like lesions with a wide base (large arrow), frond-like lesions with a narrow base (asterisk), a mound-like lesion with a wide base (arrowhead), adipose tissue signal intensity with branches like long T1 slight signal in the central region (small arrow). The main lesion was attached to the bursa wall adjacent to the bone.
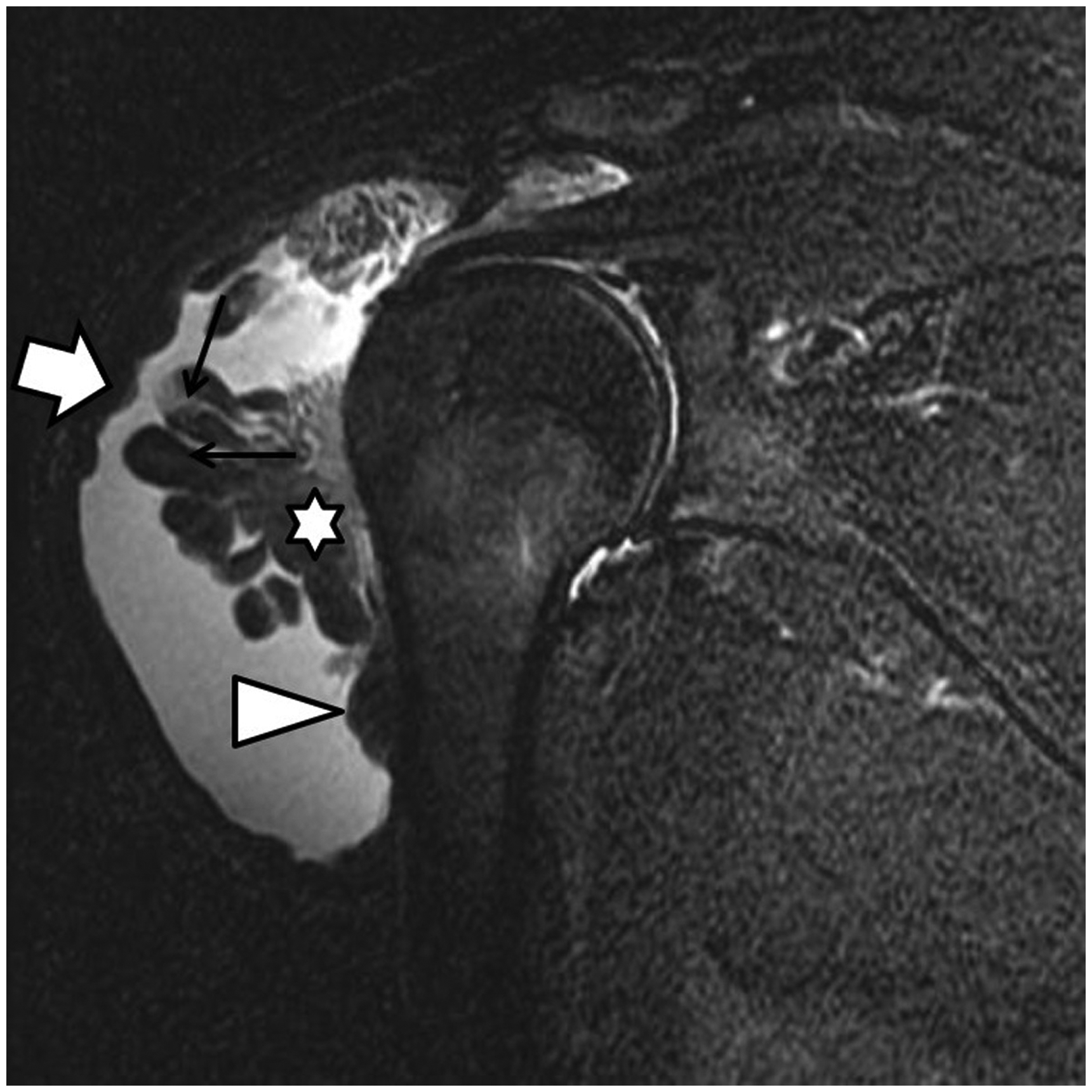
A 34-year-old female patient with lipoma arborescens in the subdeltoid bursa. Fat-saturated proton density image reveal multi-colliculus like lesions with a wide base (large arrow), frond-like lesions with narrow base (asterisk), a mound-like lesion with a wide base (arrowhead), adipose tissue signal intensity with branches like high fat-saturated proton density imaging signals in the central region (small arrow). The main lesion was attached to the bursa wall adjacent to the bone.
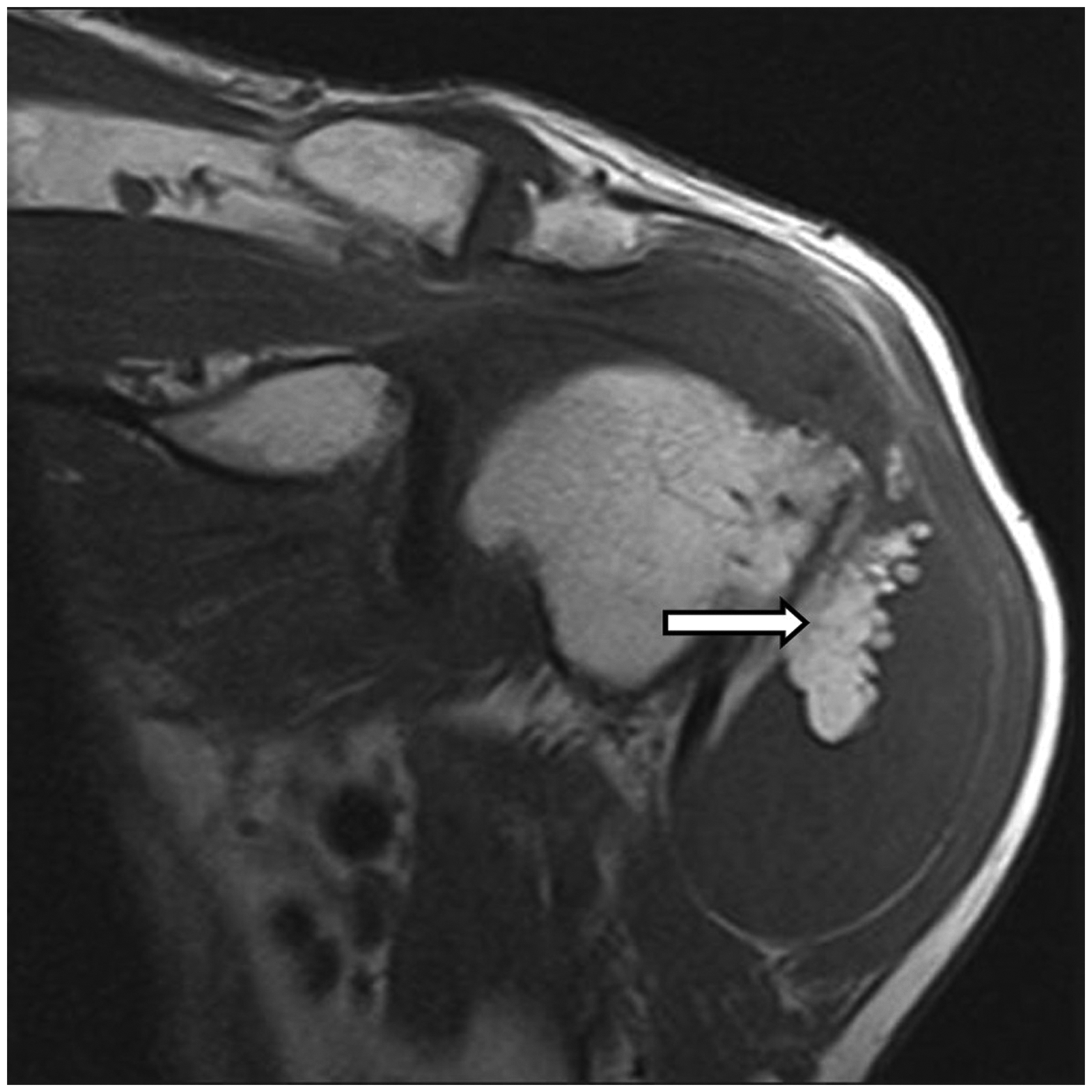
A 44-year-old male patient with lipoma arborescens in the subdeltoid bursa. Coronal T1-weighted image reveal frond-like lesions (arrow) with adipose tissue signal intensity. The main lesion was attached to the bursa wall adjacent to the bone.
A 44-year-old male patient with lipoma arborescens in the subdeltoid bursa. Fat-saturated proton density images reveal frond-like lesions (arrow) with adipose tissue signal intensity. The main lesion was attached to the bursa wall adjacent to the bone.
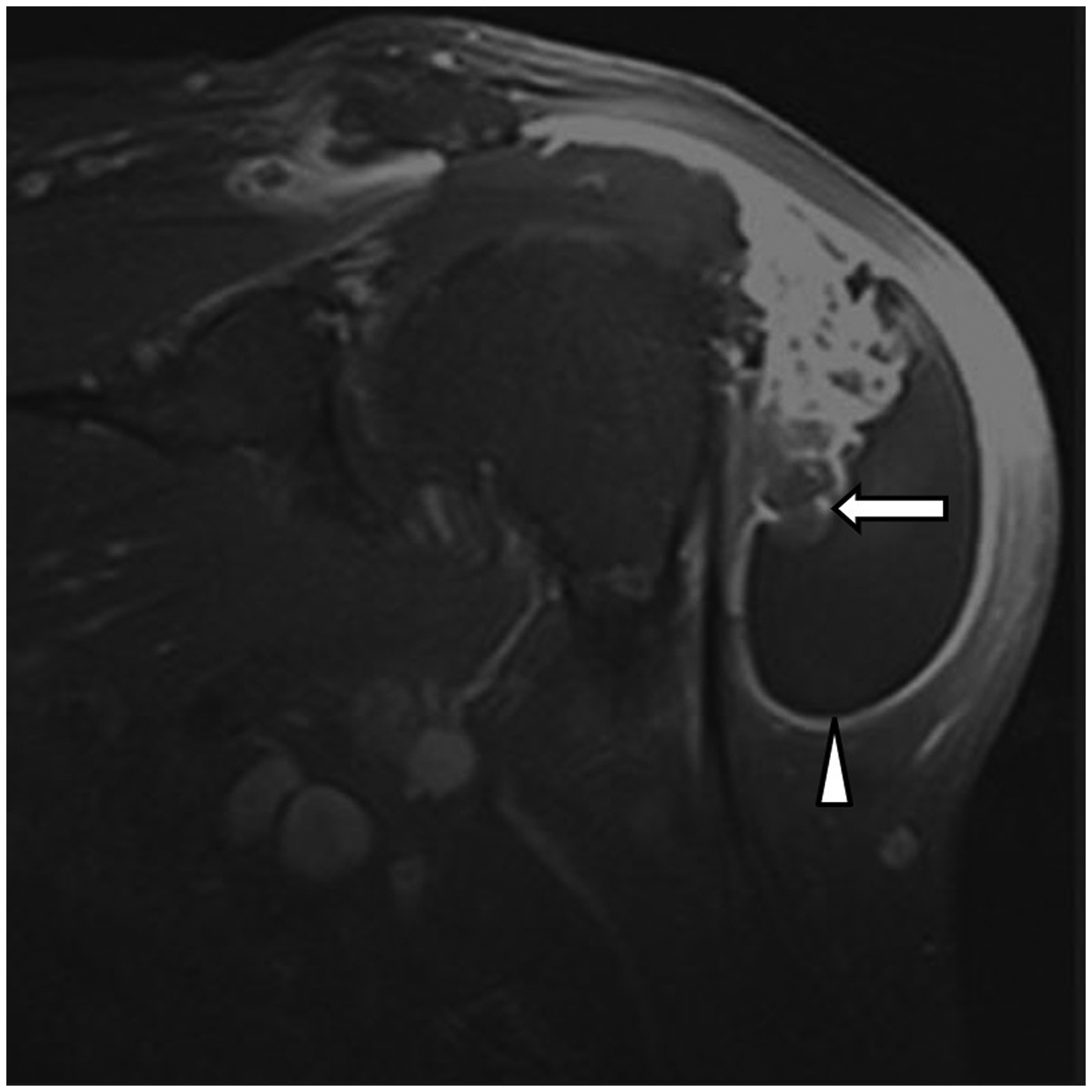
A 44-year-old male patient with lipoma arborescens in the subdeltoid bursa. T1-weighted contrast-enhanced images show linear surface enhancement (arrow) and enhancement of the bursa wall (arrowhead).
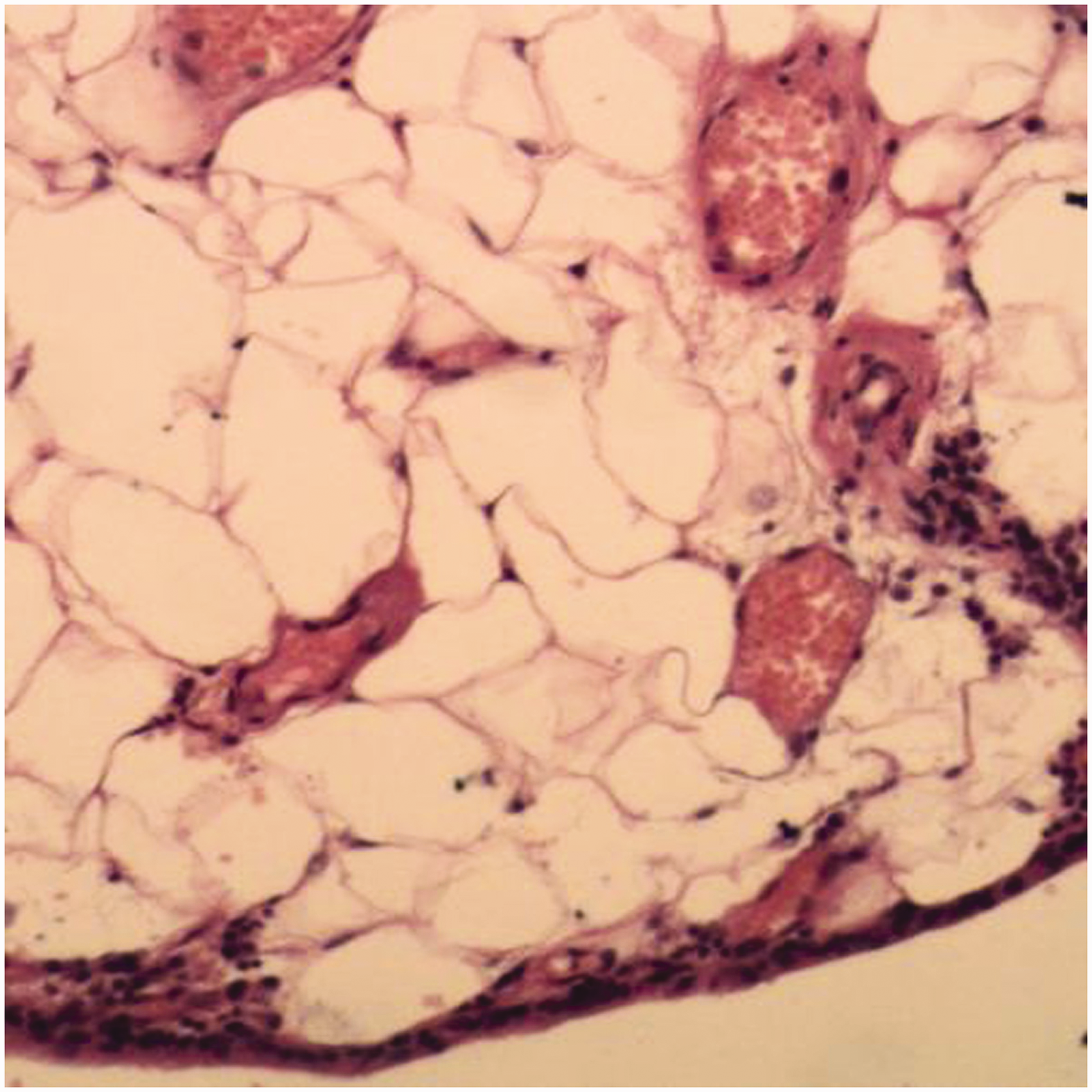
A 44-year-old male patient with lipoma arborescens in the subdeltoid bursa. Histologic examination (×100, hematoxylin and eosin stain) shows hypertrophic nodular villous proliferation with mature adipose cells in subsynovial connective tissue. Deep in the hyperplastic layer of synovial cells, there are prominent vessels and scattered clusters of chronic inflammatory cells.
An 18-year-old male patient with lipoma arborescens in the suprapatellar pouch. Non-enhanced computed tomography images of the shoulder. Axial view: soft-tissue window images display lesions of villous structures with the fat density tissue.
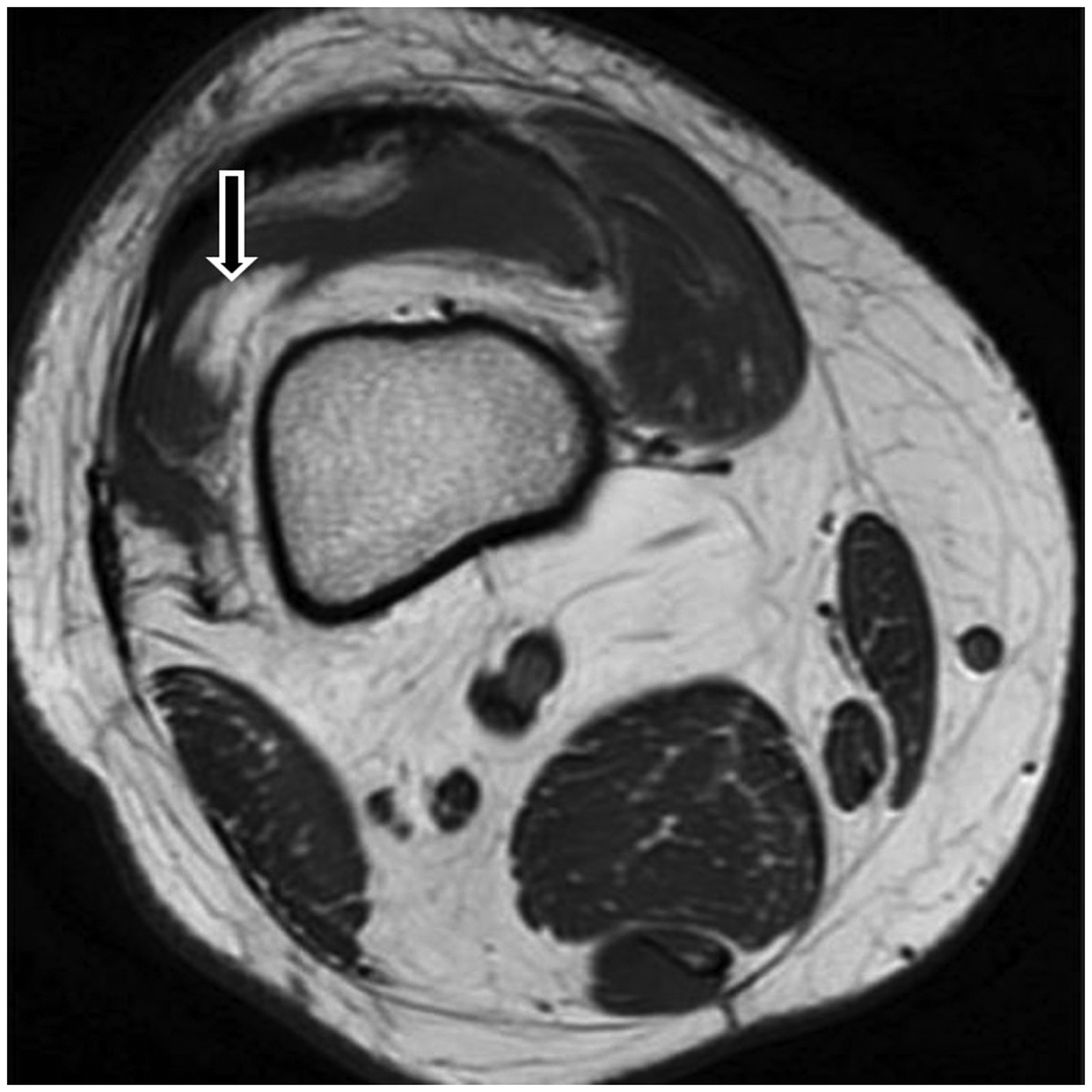
An 18-year-old male patient with lipoma arborescens in the suprapatellar pouch. Axial T1-weighted image showed villous lesions with short T1. The main lesion is attached to the bursa wall adjacent to the bone.
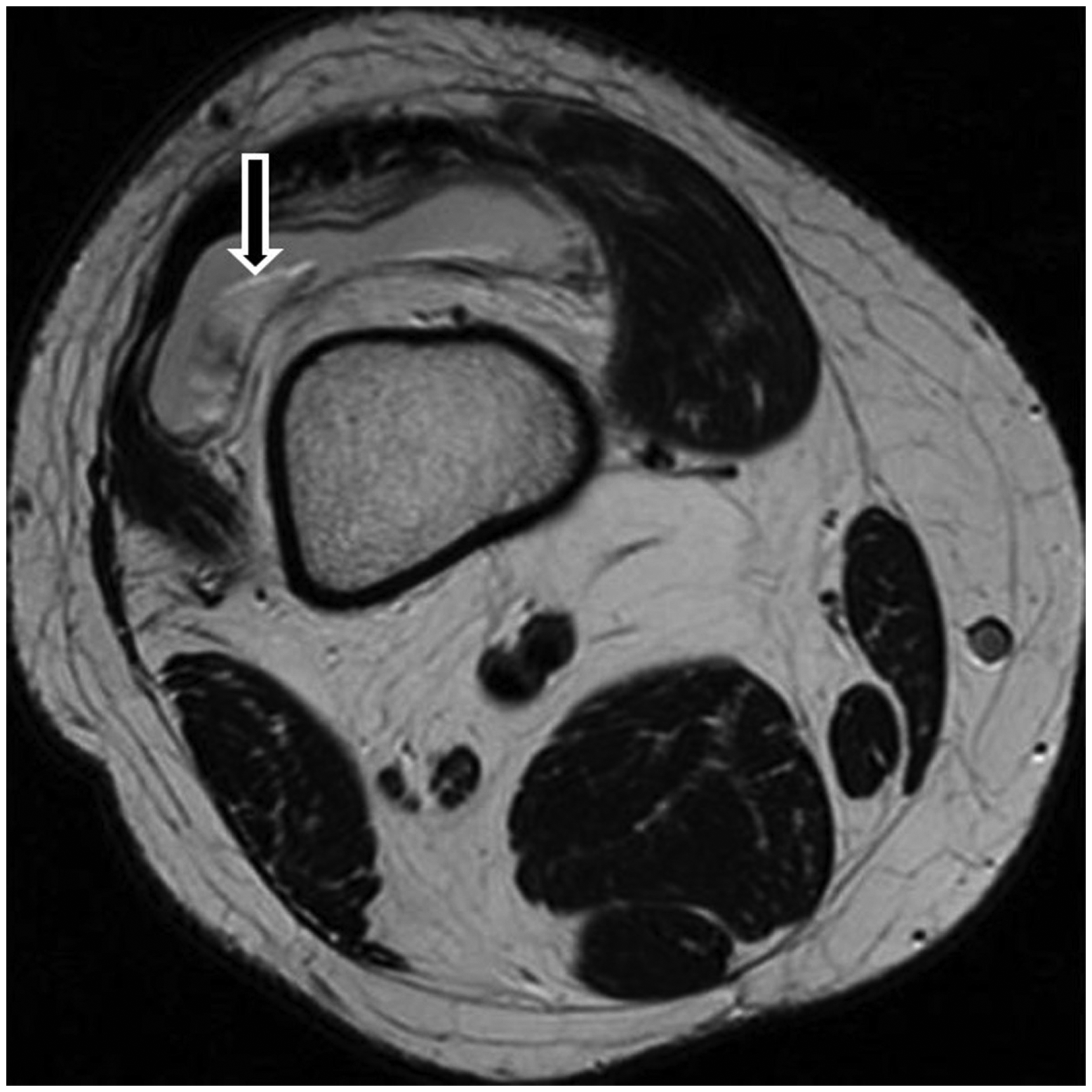
An 18-year-old male patient with lipoma arborescens in the suprapatellar pouch. Axial T2W image showed villous lesions with long T2 signal intensity on T2W imaging. The main lesion is attached to the bursa wall adjacent to the bone. T2W, T2-weighted.
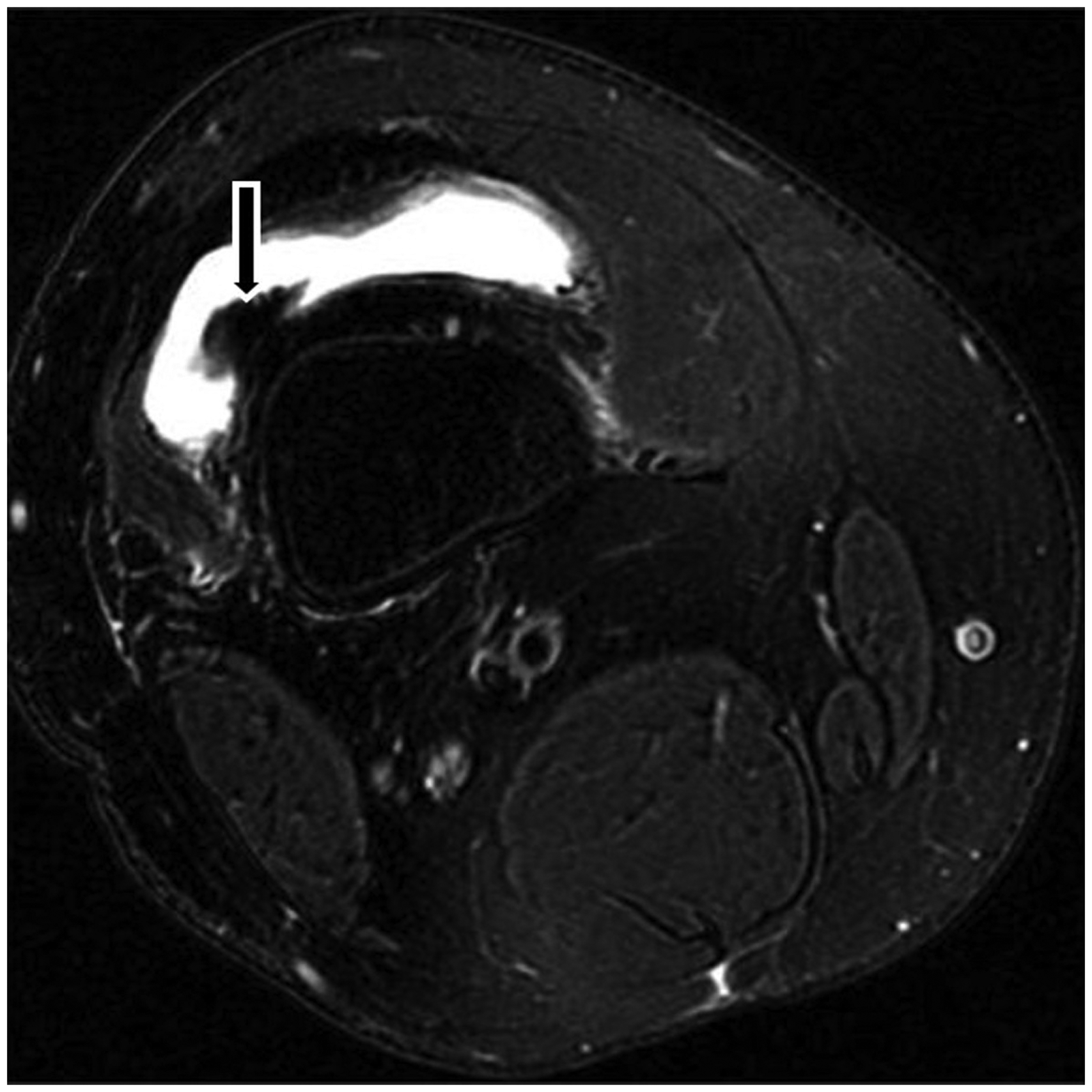
An 18-year-old male patient with lipoma arborescens in the suprapatellar pouch. Axial FS PD imaging showed villous lesions with suppression of the signal on FS PD imaging. The main lesion attached to the bursa wall adjacent to the bone. FS PD, fat-saturated proton density.
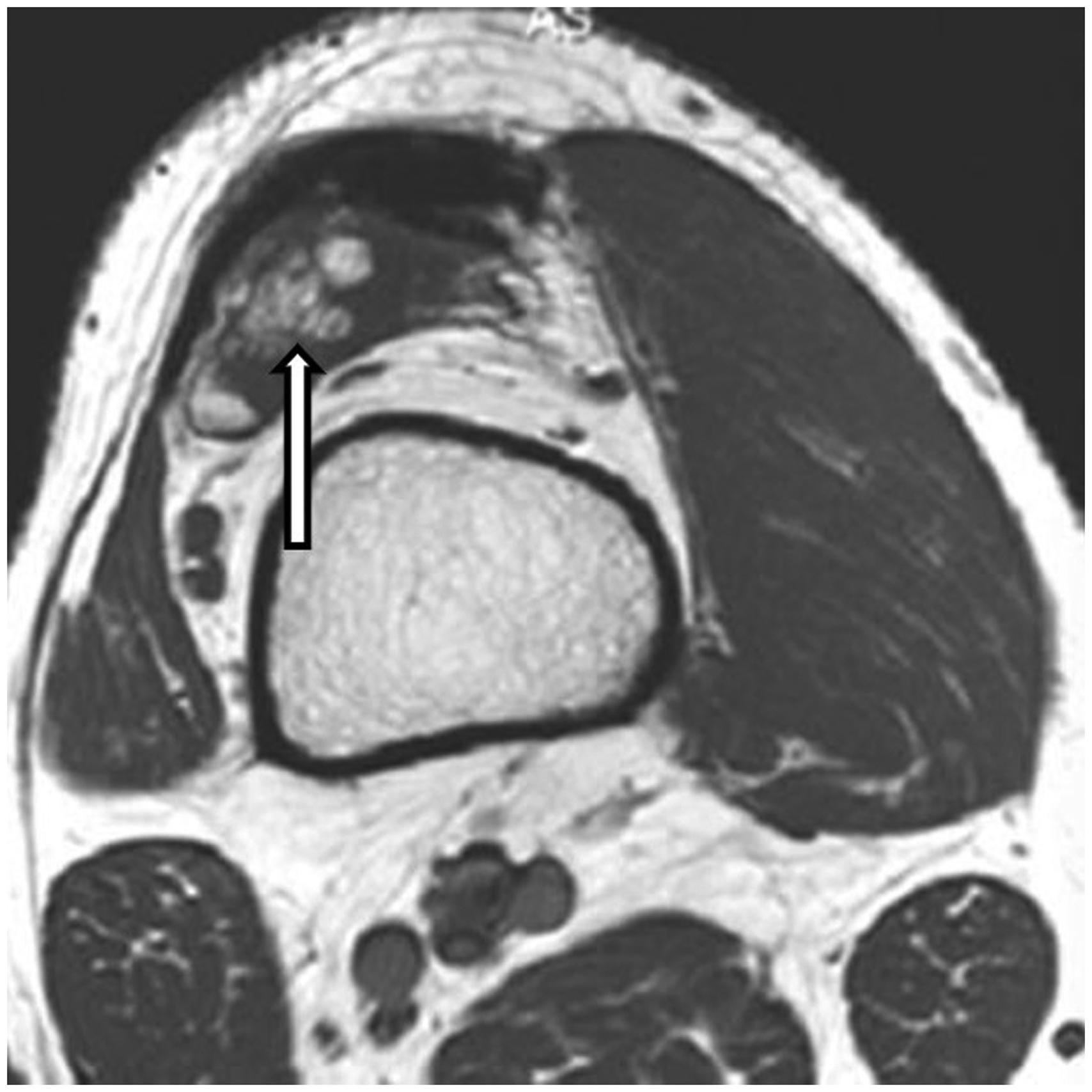
A 41-year-old female patient with lipoma arborescens in the suprapatellar pouch. Axial T1-weighted image showed villous lesions with adipose tissue signal intensity. The main lesion is attached to the bursa wall adjacent to the lateral wall of the bone.
A 41-year-old female patient with lipoma arborescens in the suprapatellar pouch. Axial fat-saturated proton density imaging showed villous lesions with adipose tissue signal intensity. The main lesion is attached to the bursa wall adjacent to the lateral wall of the bone.
A 41-year-old female patient with lipoma arborescens in the suprapatellar pouch. Axial T1-weighted contrast-enhanced image revealed linear surface enhancement (arrow); the bursa wall was also enhanced (arrowhead).
In all 15 patients, routine MRI displayed a synovial mass with fatty tissue signal on all the sequences and suppressed signal on fat suppression sequences (Figs. 3–6 and 11–15). Among them, five lesions showed branched shape with slightly low T1W imaging, high PD imaging, and T2W imaging signal intensity in the center (Figs. 3 and 4). Contrast-enhanced MRI images (n = 3) displayed linear surface enhancement, the bursa wall also enhancement (Figs. 7 and 15).
On CT, the patient with knee involvement showed synovial mass–associated fat tissue floating in the effusion of the suprapatellar bursa (n = 3) or subdeltoid bursa (n = 2). Two cases showed a branched shape with slightly high density in the center of the fat density tissue (Fig. 2). All patients (n = 2) with shoulder involvement manifested visible bony erosion of the humeral head with compressive bone resorption and sclerotic borders (Fig. 1).
On digital radiography, three patients with knee involvement showed slightly increased density in the suprapatellar pouch, one patient with a synovial loose body. One patient with shoulder involvement showed prominent bony erosion of the humeral head. The associated lesions in these 15 cases are listed in Table 1. Only two patients were associated with joint effusion with no other associated lesions.
Associated lesions from MRI, CT, and DR of lipoma arborescens in 15 patients.
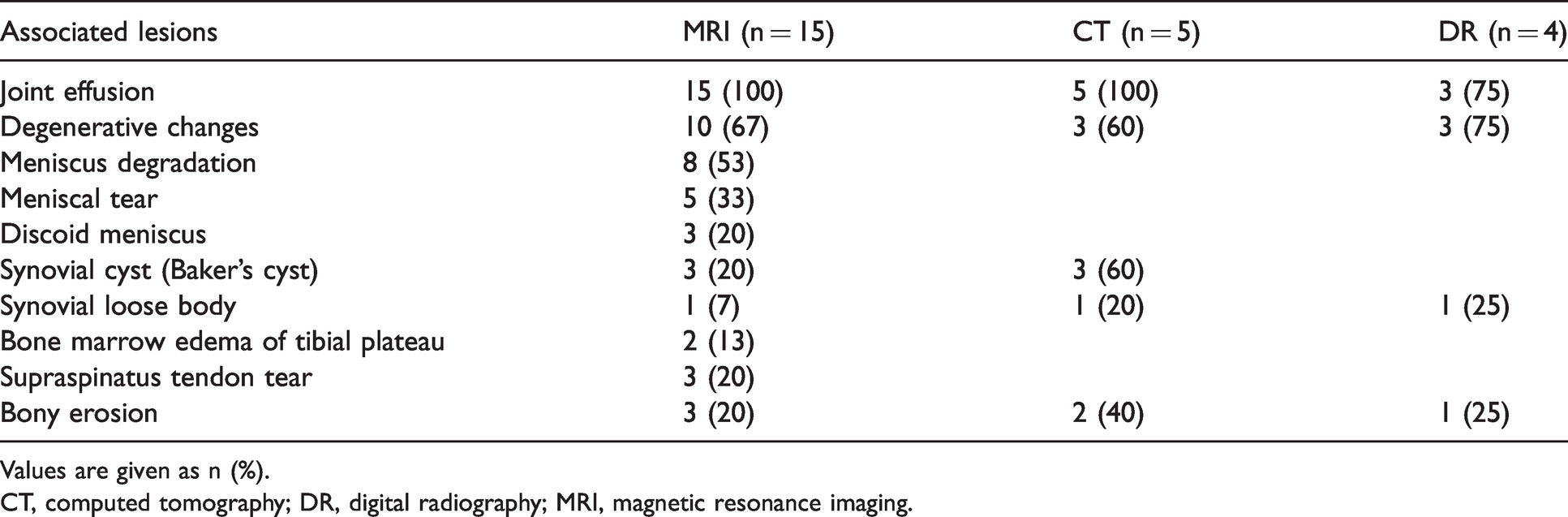
Values are given as n (%).
CT, computed tomography; DR, digital radiography; MRI, magnetic resonance imaging.
Histopathology showed that the surface of the lesions displayed normal (single-cell layer) or mildly hyperplastic synovium (2–3 cell layers). The center of the lesion showed abundant mature adipose, and some dilated capillaries or chronic inflammatory cells, which may be indicative of chronic synovitis in some cases. The subsynovial tissue may be consistent with fibrosis, chronic inflammatory cells, and vessels.
Discussion
Lipoma arborescens, often occurring in the suprapatellar pouch of the knee, which was first depicted in 1904 by Hoffa, attributing its macroscopic tree-like morphology to a fatty synovial mass Although the etiology of lipoma arborescens is unknown, it has been speculated that it could be due to synovial tissue reaction, which might be associated with joint trauma, meniscal lesions, chronic arthritis, or synovitis, rather than a true neoplasm (11). In this study, most of the lesions (12/15) have associated findings. Lipoma arborescens may occur at any age, and it could affect patients aged 8–70 years. Most lesions occur in their fifth to seventh decade, with an almost equal predominance between male and female individuals (4) or a slight predilection for boys/men (3,11). The findings of this study were similar to past reports. The patients’ age was in the range of 16–62 years, and the ratio of women to men was 8:7. Most lipoma arborescens are asymptomatic. Sometimes it is accompanied by typical clinical manifestations, including gradual swelling lasting for years with pain and weakness. It may sometimes occur with associated intermittent episodes of joint effusion (12). Lipoma arborescens is most common in the knee joint and can also occur in other joints, including shoulders, elbow, wrist, and hip (11). In the present study, 11 cases occurred in the knee joint and four cases were located in the shoulders, in agreement with the previous studies.
Lipoma arborescens has characteristic features. According to the literature and the present study, the typical imaging appearance of Lipoma arborescens is listed below.
Conventional radiographs generally demonstrate non-specific findings in the form of soft-tissue swelling (12,13). The typical CT appearance includes the following: (i) synovial cysts and an arborescent, frond-like synovial mass associated with fat tissue density; (ii) no enhancement on postcontrast CT; and (iii) osseous erosion of the joint (5,14,15).
The typical MRI features of lipoma arborescens include the following: (i) joint effusion; (ii) a synovial mass accompanied with a frond-like or arborescent shape that generally shows a signal intensity similar to that of fat on all imaging and suppression of the signal on fat suppression sequences (6,16); (iii) without hemosiderin; and (iv) a synovial mass with no enhancement after postcontrast administration (7) or synovium showed enhancement indicative of chronic synovitis (17).
Based on these characteristic manifestations on CT and MRI, especially MRI, a definite diagnosis of lipoma arborescens can be made (18). MRI with fat saturation sequences has a high specificity and can draw relatively accurate conclusions, thus avoiding unnecessary biopsy (1,16,18). The previous studies (19,20) found that the lesions were arborescent, frond-like synovial masses. This study also found a mound-like lesion with a wide base synovial mass, suggesting the diversity shape of lipoma arborescens. On MRI, five cases of the frond-like fatty synovial mass showed branches like low T1, slight high T2, or FS PD imaging signal intensity on MRI and a slightly high density on CT images in the central region. Although it is impossible to achieve complete agreement between pathology and imaging, the central region signal intensity and density seen on MRI and CT images may reflect the vascular density obvious infiltration of inflammatory cells, and a small amount of fibrous tissue hyperplasia that was proven by our histologic examination.
In the present study, contrast-enhanced MRI images displayed linear surface enhancement (n = 3), as was demonstrated in chronic synovitis by histologic examination, as reported by the past study (17). Prominent bone erosion surround with hardened edges in the shoulder is an uncommon sign in the knee (16), which may reflect the fact that the space of the shoulder joint is smaller than the knee joint, as mentioned in the literature (17). In the present study, most of the shoulder lesions (3/4) caused obvious bony erosion.
Based on the previous experience, the differential diagnosis should contain but is not limited to synovial hemangioma, synovial osteochondromatosis, synovial lipoma, rheumatoid arthritis, and pigmented villonodular synovitis (PVNS) (18). Synovial hemangiomas usually appeared in intermediate signal intensity on T1W and T2W imaging, accompanying some punctate or linear areas of low signal intensity associated with fluid voids or phleboliths. MRA showed the honeycomb-shaped vascular channels. Synovial osteochondromatosis typically showed the typical calcifications of the chondroid (low signal intensity on MRI, calcification density on CT). The synovial lipoma is characterized by a signal intensity or density similar to fat tissue, but the lesion shape is oval or rounded. Rheumatoid arthritis displayed iso-low signal intensity on T1W and T2W imaging due to some fibrous pannus existed. PVNS typically showed a diffuse hypo-signal intensity on both T1W and T2W imaging, because it was possible to see the presence of hemosiderin in the tissue. CT displayed soft-tissue density.
There are some traits that should be considered characteristic of lipoma arborescens. These include synovial cysts and an arborescent, frond-like synovial mass associated with fat tissue density on CT. They generally show a signal intensity similar to that of fat on all imaging, and suppression of the signal on fat-suppression sequence. Lesions show branched slightly low T1W imaging, high PD imaging, and T2W imaging signal intensity in the center. There is no enhancement on postcontrast CT or MRI. Fewer cases that occurred near the bone tend to accompany osseous erosions, showing prominent bony erosion with compressive bone resorption and sclerotic border. Joint effusion without hemosiderin.
The present study has some limitations. The number of cases included in the study was relatively small. In addition, not all of these cases have a contrast-enhanced examination, so postcontrast imaging characteristics were insufficient.
In conclusion, the characteristic appearances of lipoma arborescens on CT and MRI make it possible to make a reliable diagnosis of this rare condition, which may prevent additional work-up and delayed treatment.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.