
Abstract
The encouraging results of modern breast cancer care builds on tremendous improvements in diagnostics and therapy during the 20th century. Scandinavian countries have made important footprints in the development of breast diagnostics regarding technical development of imaging, cell and tissue sampling methods and, not least, population screening with mammography. The multimodality approach in combination with multidisciplinary clinical work in breast cancer serve as a role model for the management of many cancer types worldwide. The development of breast radiology is well represented in the research published in this journal and this historical review will describe the most important steps.
Keywords
When it all started
The starting point of diagnostic radiology of the breast is usually recognized as the year 1913, when Dr Albert Salomon, a resident at the Royal Surgical University Clinic in Berlin, published his work “Beiträge zur Patologie und Klinik der Mammacarcinome” (1). He describes in detail a carcinoma imaged by roentgenogram of an amputated breast, which includes many of the descriptive parameters we still use today, such as the tumor shadow, calcifications, spiculations, and cysts. Furthermore, he mentions normal and metastatic lymph nodes. Today, more than 100 years later, many of his observations are still valid. This historical article will follow the developmental path of diagnostic radiology of the breast and highlight the footprints made in Acta Radiologica over the years.
Early focus on breast cancer treatment
Many of the early studies in Acta Radiologica concern radiotherapy in the treatment of breast cancer rather than diagnostics (2–5). There has been tremendous development in early detection in combination with improved treatment during the 20th century. A report by Sigvard Kaae in 1947 shows that the five-year total survival rate in a small Danish cohort for both stages I and II together was 55%, for stage I 69%, and for stage II 41% (2). He reported on his findings regarding preoperative radiation treatment. In another paper in 1948, Kaae gives his view on typical symptoms in patients with breast cancer and the time until they seek help (patient's delay). We especially appreciate his notions on information bias, which he tries to minimize by interviewing 500 consecutive women himself rather than trusting the medical records: “The present study is based on a material from the Radium Center in Copenhagen from the period June 1944–December 1946. I have personally questioned all the patients in order to get the anamnestic data as full and correct as possible, because I have found that the information obtained from the usual record entries made by shifting assistant physicians without special interest in the subject are very often incomplete, or even directly misleading.”
It goes without saying that Kaae himself might have caused some misleading confirmation bias by searching for information supporting his ideas and hypotheses. Nevertheless, he correctly concludes that a breast lump or induration in the breast of a woman aged over 20 years are the most important symptoms (also acknowledging other less common symptoms) (3). Further, he found that actual pain is seldom an early symptom of breast cancer. The latter is still a challenge to communicate to women, who many times seek advice for breast pain due to fear of breast cancer. Kaae makes assumptions about what impact earlier diagnosis would have on survival and discusses regular health examinations as one solution. In many ways, his clinical observations were valid and showed the need for an earlier diagnosis of breast cancer.
When breast imaging comes into play
The first articles more related to diagnostics were published in the mid-1950s and described the use of a tracer dose of radioactive colloidal gold injected into the breast tumor area some days before radical excision to detect lymph nodes with a scintillation counter (6,7). Interestingly, it took until the 21st century to refine the diagnosis of axillary involvement with the introduction of the sentinel node technique, saving many women from morbidity after axillary dissections (8).
Although several attempts to develop a radiographic technique to image the breast were made in the preceding decades, a major step towards modern mammography was taken by Raoul Leborgne in Montevideo, Uruguay in the 1940s and published in 1951 (9). He used 20−30 kV, 5 mAs per 1-cm thickness of the compressed breast, a target-film distance of 60 cm, and plain films with the patient standing. The craniocaudal (CC) view was acquired followed by a spot view obtained by using a long metallic cone attached to the X-ray tube. Leborgne was the first to use local compression that later became standard in mammography. The degree of breast compression is still today a matter of interest (10–12), to achieve good image quality and because there are no firm guidelines on how much compression is needed. The associated pain is one factor that may make some women refrain from participating in mammography screening.
Charles Gros is regarded by many as the father of “modern” mammography, who in collaboration with the industry designed the first dedicated mammography unit, “Senographe,” by CGR in France in 1967. He also published a textbook that was the educational source for many radiologists worldwide (13). Nils Bjurstam in Gothenburg brought this technique to Sweden, and he had much impact on the spread and development of both clinical and screening mammography in Scandinavia.
Scandinavian pioneers in breast cancer screening
The first screening-related publication in Acta Radiologica is a report from Malmö in 1970 (14). In 1966 and 1967, Langeland invited 10% of the female population aged 16–67 years in Malmö to undergo breast cancer screening by clinical examination, hence not mammography. The results of the study were inconclusive, and we now know that mammography can detect tumors at a much earlier, non-symptomatic stage than clinical examination. The Health Insurance Plan (HIP) study in New York, USA took place during 1963–1969 and is regarded as the first mammography screening trial, even if clinical examination was also part of the protocol (15). The list of Scandinavian pioneers and contributors to the establishment of population-based breast cancer screening is long and impressive, and they have all made footprints in Acta Radiologica. Bengt Lundgren started one of the first pilot projects on breast cancer screening in Sandviken in 1974, first using thermography, thereafter single view mammography (16,17). Ingvar Andersson started randomized trials in Malmö in 1976 (18–20) and shortly thereafter the Kopparberg-Östergötland (WE) study was initiated on an initiative of the Swedish National Board of Health and Welfare and headed by László Tabár (21). The Stockholm (22) and Gothenburg (23) trials followed in the early 1980s headed by Lars Hellström and Nils Bjurstam, respectively. The most solid data of the effects of mammography screening on breast cancer mortality relate to the Swedish trials and indicate that a 20% reduction in breast cancer mortality can be achieved among women invited to screening, although this has been the subject of much debate over the years (24).
Mammography, dose, and transition to digital mammography
In the surge of finding non-irradiating breast imaging methods, reports on less successful initiatives such as light-scanning and diaphanography can be found in the Acta Radiologica records (25–29), although neither of the techniques proved accurate enough. Several publications in Acta Radiologica relate to refinements of dose and image quality in mammography (30,31). In the mid-1970s, it was possible to reduce substantially the radiation dose through the introduction of rare-earth intensifying screens (32). A major contribution to image quality and reduction of the dose was made by Mats Danielsson, who introduced a solid-state detector using a direct photon counting technique in a scanning geometry (33).
The transition from analog to digital images in the early 2000s was a huge step forward: no film processing, digital storage, and the possibilities to postprocess the digital images further improved radiation dose, image quality, reading possibilities, and reading conditions. This is nicely highlighted in the editorial accompanying the follow-up publication of the large Oslo I study conducted by Per Skaane et al. comparing screen-film mammography (SFM) and full-field digital mammography (FFDM) with soft-copy reading (34,35). This large, paired screening study showed that FFDM was as good as SFM for the detection of cancer. There was great hope that FFDM would perform better in women with dense breasts than SFM. However, it has not been proven that the rate of screening-detected cancers is increased, nor that the interval cancer rates are decreased with the use of FFDM (36). Nevertheless, the digitalization of radiology, including breast imaging, has from a technological and workload point of view been a significant improvement to the medical society.
Digital breast tomosynthesis and the future of screening
The major limiting factor in SFM as well as in FFDM is the so-called anatomical noise, i.e. the breast tissue itself, that may hide or simulate a tumor in two-dimensional imaging, especially in denser breasts. With the development of more powerful computers and detectors with faster read-out, it was possible to reintroduce the idea of tomosynthesis, a pseudo-three-dimensional technique described already in 1932 by BG Ziedses des Plantes, who developed methods of reconstructing an arbitrary number of planes from a set of projections (“planigraphy”) in which the X-ray tube and the film moved together around the plane of interest (37). While computed tomography (CT) started to dominate in other imaging areas, tomosynthesis emerged as a low-dose alternative to CT with applications in bone, chest, and breast radiography (38). In Sweden, tomosynthesis was first investigated in the breast by Ingvar Andersson in Malmö (39). In Acta Radiologica, the first article on breast tomosynthesis was published in 2011 by Svane et al., investigating the unique photon-counting breast tomosynthesis system resulting in lower dose compared to FFDM in an initial clinical series and using a halved compression force at digital breast tomosynthesis (DBT) for increased comfort (40). The ability of DBT to reduce the anatomical noise resulting in increased lesion visibility and conspicuity (Fig. 1) was described by several groups in smaller clinical series compared to other imaging techniques (41–43), and in an experimental study using breast specimens (44). To date, DBT has been investigated in large, prospective population-based screening trials clearly showing around a 30% increase in cancer detection, although results on interval cancer rates have been inconsistent (45,46). Also in this setting, the Scandinavian countries have contributed with most of the pioneer DBT screening trials, just like in the early era of mammography screening. DBT is now widely adopted worldwide in the clinical setting; however, it has not yet been fully implemented in population screening. Ongoing discussions and trials are investigating risk-adapted screening or individualized screening approaches where mammography, breast tomosynthesis, ultrasound, and magnetic resonance imaging (MRI) may have major roles in different groups.
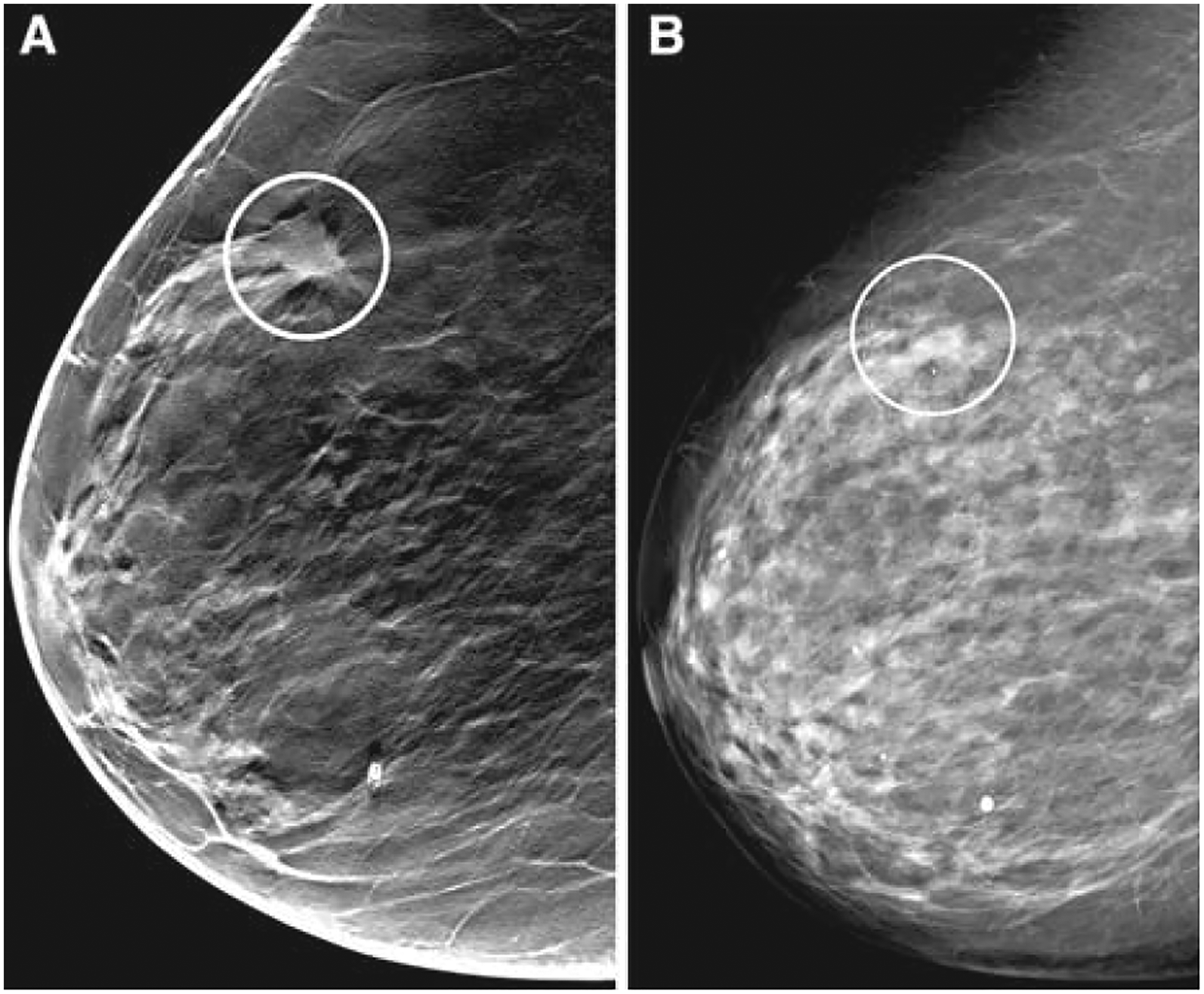
An illustration of the increased lesion conspicuity and more accurate tumor size measurements with DBT compared to DMG. A 67-year-old asymptomatic woman with a measurable tumor on DBT but not measurable on DMG. (A) DBT in the oblique view shows a well-defined spiculated tumor (circle) whose largest diameter was measured to be 12 mm. (B) On the corresponding two-dimensional view, an ill-defined area of increased density is seen (circle). On histopathology, a 15-mm grade 3 invasive ductal carcinoma was found. (Fig.2.) from Förnvik et al. (41)). DBT, digital breast tomosynthesis; DMG, digital mammography.
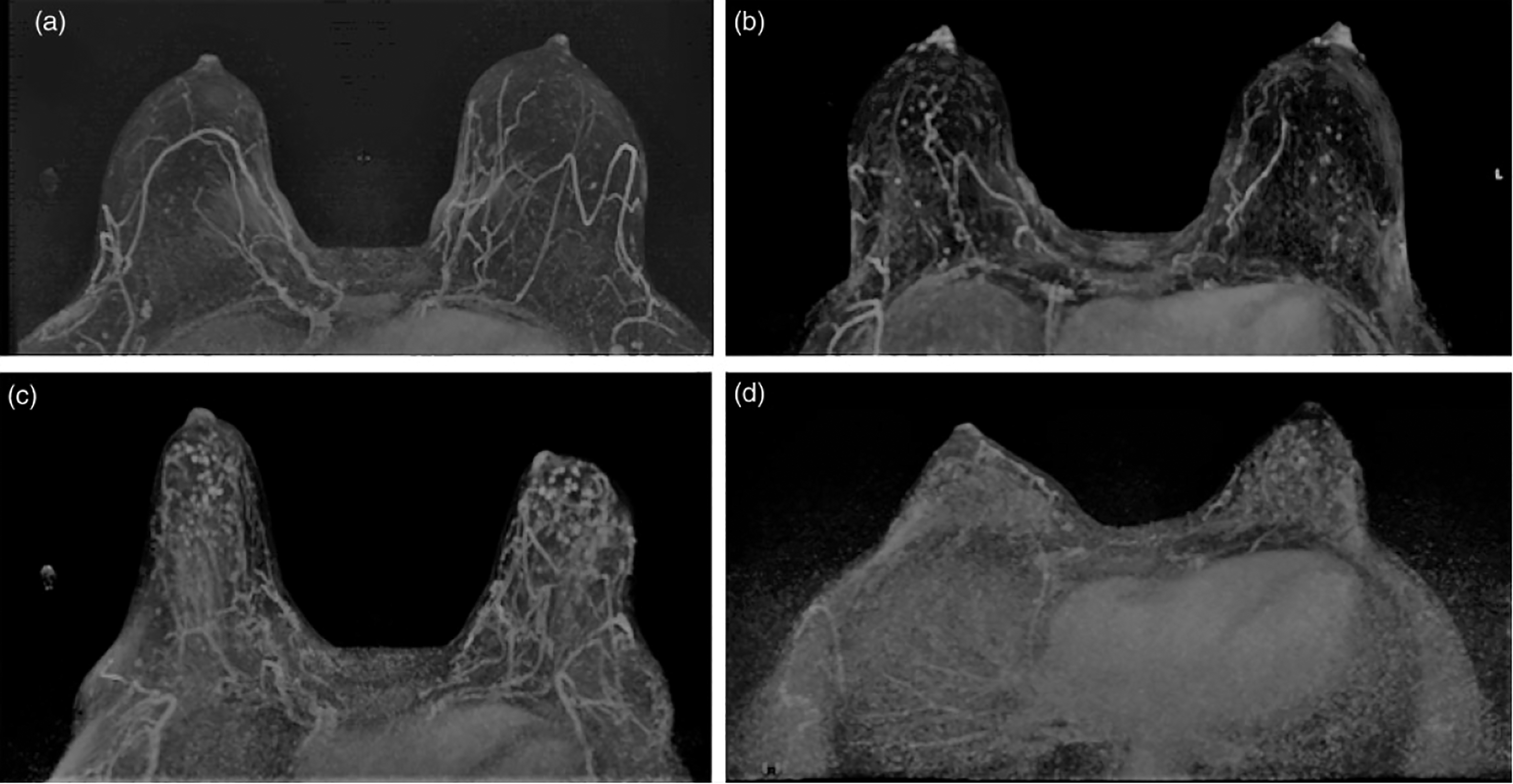
Imaging does not only provide diagnostics, it may also carry prognostic and treatment predictive information. In later years, these so-called imaging biomarkers have also gained increased interest in breast imaging. Breast parenchymal enhancement, BPE is a new potential imaging biomarker for breast cancer risk. BPE in DCE-MRI is the proportion of enhancing normal fibroglandular tissue of the breast here investigated by Hellgren et al. in relation to established risk factors for breast cancer (77). The four images show (a) minimal, (b) mild, (c) moderate, and (d) marked BPE in four different women, according to the American College of Radiology Breast Imaging- Reporting and Data System (BI-RADS) Atlas 5th Edition (101). BPE, background parenchymal enhancement; DCE-MRI, dynamic contrast-enhanced magnetic resonance imaging.
Ultrasound: a focused method and guide to interventions
Ultrasound entered breast imaging in the 1980s and the first ultrasound report in Acta Radiologica concerned ultrasound-guided percutaneous drainage of breast abscesses (47). Ultrasound is more or less compulsory as an adjunct to mammography in the imaging of symptomatic patients as well as in the workup of non-palpable cancer-suspicious lesions, including as guidance for needle biopsies and other preoperative interventions (48–51). It is the first diagnostic imaging method of choice for younger women (age <30 years). It has been investigated as a supplementary screening method for women with dense breasts but has not yet proven to be cost-effective (52,53). Three-dimensional automated breast ultrasound is a promising development of the method that may be useful in screening women with dense breasts (54). Ultrasound elastography, visualizing and measuring relative tissue stiffness, has gained much interest during the last decade, to better characterize lesions (55–59). Contrast-enhanced ultrasound (CEUS) may also play a role in the preoperative staging of breast cancer, including the demonstration of multifocality as well as monitor treatment response of neoadjuvant therapy (60). However, neither elastography nor CEUS has in most places been fully implemented, since biopsy is still regarded as the gold standard and dynamic contrast-enhanced breast MRI has emerged as the most accurate breast imaging method.
Breast interventions: challenges and solutions for non-palpable lesions
With the introduction of mammography screening and earlier diagnosis, more non-palpable lesions only visible on mammograms (often microcalcifications) became detected, which uncovered a need for imaging guidance and localization methods for fine-needle aspirations and placement of preoperative indicators. The Swedish radiologist Björn Nordenström was one of the pioneers who developed a stereotactic technique by which the sampling site could be located at a precision within ± 1 mm (61). This was further developed into the so-called Fisher table where the patient lies prone. Gunilla Svane in Stockholm performed several early studies on stereotactic needle applications in 1983 (62–64). Cytology was the dominating method for diagnosis of breast cancer earlier but is now to a large extent replaced by core-needle biopsy (65–69) or vacuum-assisted biopsy by stereotactic technique or guided by ultrasound (49,70).
Magnetic resonance imaging of the breast
In 1979, MRI of a carcinoma in a breast specimen was one of the first performed studies for human applications by Sir Peter Mansfield himself (71). It was early on concluded during the clinical introduction of the MRI technique in the mid-1980s that native (unenhanced) MR did not have a place in the distinction of benign and malignant changes of the breast and that intravenous contrast enhancement was needed (72) (Figure 2). Kaiser et al. further refined the protocols with the addition of several postcontrast acquisitions allowing better temporal resolution of the contrast enhancement and together with high spatial resolution sequences. This combination is now considered state-of-the-art in breast imaging with MRI: dynamic contrast-enhanced MRI (DCE-MRI) (73). However, non-enhanced, high contrast images are useful for indications such as breast implant complications, but as shown by Boné et al. in Acta Radiologica in 1995 contrast-enhanced MRI is needed when imaging patients with breast implants after cancer surgery (74).
The usefulness of diffusion-weighted imaging in breast MRI has been an area of intensive investigations lately (75,76) as well as the role of background parenchymal enhancement as an imaging biomarker for breast cancer risk (77) (Figure 2). DCE-MRI has, in many settings, an important role in preoperative staging (78). The increased use of neoadjuvant treatment regimens in breast cancer during the last decade has called for more refined imaging evaluation than the conventional breast imaging methods sometimes can offer, and DCE-MRI has the best accuracy in predicting complete pathological response (79). It is, however, not clear how the information from DCE-MRI can be used, for example in the treatment planning following complete response and whether it can be used for prognostication (80–84). In screening, DCE-MRI has shown impressive results in women within the densest breast category in the detection of breast cancer as well as in reducing interval cancers (85).
What is yet to come?
In breast imaging, DCE-MRI and CEUS are, so far, the most studied methods providing functional information. However, scintimammography with 99mTc-sestamibi has been investigated and has been used in some places to increase diagnostic accuracy (86–90). DCE-MRI has largely overtaken this role but is now partly challenged by contrast-enhanced spectral mammography (91,92), which also may be a good alternative for patients with MRI contraindications (93). 18F-fluorodeoxyglucose positron emission tomography (FDG-PET) is investigated for staging purposes in breast cancer as exemplified by Park in 2011 (94) but has not yet been proven to add more information than CT and sentinel node biopsies. Breast-cancer–specific PET tracers are being investigated, which may change the imaging landscape in a near future.
Breast screening practices constantly suffer from a lack of skilled breast radiologists and a high workload. Computer-aided detection (CAD) was seen by many as a possible solution with encouraging numbers for sensitivity but failed in practice much due to low specificity, i.e. a high number of false-positive markings (95–97). Machine-learning-based methods for the detection of breast cancer are now promoted as the “new radiologists” with applications extended from mammography to DBT as well as to three-dimensional whole breast ultrasound (98,99).
A future perspective must include phase-contrast X-ray imaging: In 2010, Keyriläinen et al. published in Acta Radiologica a report about phase-contrast X-ray imaging of the breast (100). When X-rays traverse an object, the amplitude and phase change, which results in attenuation, interference, and refraction, and in phase-contrast X-ray imaging, these are converted to intensity changes. This is perhaps the start of a new era with synchrotron radiation facilities becoming available in the clinical environment with the ongoing development of compact radiation sources.
Tremendous improvements have been made in the diagnosis and treatment of breast cancer during the last century, although much of it has happened in the last 40 years. Breast cancer mortality has decreased continuously due to early detection and improved treatment. Still, breast cancer is among the most common causes of cancer death in women in many western countries. Therefore, our work must continue. Every successful diagnostic and therapeutic effort lays new ground and may have an impact on many women worldwide.