
Abstract
Background
Chest radiography (CR) patterns for the diagnosis of COVID-19 have been established. However, they were not ideated comparing CR features with those of other pulmonary diseases.
Purpose
To create the most accurate COVID-19 pneumonia pattern comparing CR findings of COVID-19 and non-COVID-19 pulmonary diseases and to test the model against the British Society of Thoracic Imaging (BSTI) criteria.
Material and Methods
CR of COVID-19 and non-COVID-19 pulmonary diseases, admitted to the emergency department, were evaluated. Assessed features were interstitial opacities, ground glass opacities, and/or consolidations and the predominant lung alteration. We also assessed uni-/bilaterality, location (upper/middle/lower), and distribution (peripheral/perihilar), as well as pleural effusion and perihilar vessels blurring. A binary logistic regression was adopted to obtain the most accurate CR COVID-19 pattern, and sensitivity and specificity were computed. The newly defined pattern was compared to BSTI criteria.
Results
CR of 274 patients were evaluated (146 COVID-19, 128 non-COVID-19). The most accurate COVID-19 pneumonia pattern consisted of four features: bilateral alterations (Expß=2.8, P=0.002), peripheral distribution of the predominant (Expß=2.3, P=0.013), no pleural effusion (Expß=0.4, P=0.009), and perihilar vessels’ contour not blurred (Expß=0.3, P=0.002). The pattern showed 49% sensitivity, 81% specificity, and 64% accuracy, while BSTI criteria showed 51%, 77%, and 63%, respectively.
Conclusion
Bilaterality, peripheral distribution of the predominant lung alteration, no pleural effusion, and perihilar vessels contour not blurred determine the most accurate COVID-19 pneumonia pattern. Lower field involvement, proposed by BSTI criteria, was not a distinctive finding. The BSTI criteria has lower specificity.
Introduction
The COVID-19 pandemic was declared a world emergency in January 2020 (1). COVID-19 infection may lead to rapidly evolving pneumonia with unfavorable prognosis (2). Nowadays, chest imaging is still used for triage of patients with COVID-19 and assists clinician in both the diagnosis and management of COVID-19 pneumonia (3). Although chest computed tomography (CT) has higher sensitivity compared to chest radiography (CR) in detecting COVID-19 pneumonia (4), the Fleischner statement leaves the choice of imaging modality to the clinical teams, depending on local resources and expertise (3). Because of the lower cost and larger accessibility of CR, this technique remains a valuable resource in an emergency department (ED) setting, also reducing the risk of cross-infection with portable CR systems (5,6). Common features on CR of COVID-19 pneumonia have been described, and CR patterns have been proposed (5,7,8). Among them, the British Society of Thoracic Imaging (BSTI) defined a classic pattern (lower lobe and peripheral predominant multiple opacities that are bilateral >> unilateral), an indeterminate pattern (that does not fit classic or non-COVID-19 descriptors), a non-COVID-19 pattern (pneumothorax/lobar pneumonia/pleural effusion/pulmonary edema), and negative CR, to help ED doctors in diagnosing typical CR alterations of COVID-19 pneumonia (8). However, to define the patterns, the CR features of COVID-19 pneumonia have been not compared to other pulmonary diseases, which could present CR features shared with COVID-19 pneumonia.
Therefore, the aim of the present study was to compare CR features of COVID-19 pneumonia to those of other pulmonary diseases to determine the most specific CR COVID-19 pattern, and then to compare these features to those proposed by the BSTI criteria.
Material and Methods
Study design and patient selection
We retrospectively evaluated patients consecutively admitted to the ED of the Ca' Foncello General Hospital (Treviso, Italy) between March and April 2020 with COVID-19 infection confirmed by real-time reverse transcription polymerase chain reaction (RT-PCR). We then evaluated patients admitted to the ED between March and April 2019, for respiratory symptoms compatible with COVID-19 infection (9), such as cough, dyspnea, sputum production, chest pain, sore throat, or rhinorrhea.
Inclusion criteria were as follows:
available anteroposterior (AP) or posteroanterior (PA) CR, performed at admission; diagnosis of COVID-19 pneumonia among patients with COVID-19 and of pulmonary disease among non-COVID-19 patients; good CR image quality.
For both groups, the final diagnosis was reached following local protocols at that time and reported from the ED discharge letters. In particular, following COVID-19 protocol, the diagnosis of COVID-19 pneumonia was verified by CR and lung ultrasound (LUS) and confirmed only when both techniques were concordant. COVID-19 protocol also included a chest CT in case of discrepancy between CR and LUS. LUS was performed by the clinicians at the ED, whereas CR and CT were analyzed by the radiologists.
According to the criteria of the American College of Radiology 2017 statement (10) (Supplementary Material), the quality of CR was assessed by consensus between a thoracic radiologist (NL) with 7 years of experience and a general radiologist (GM) with 25 years of experience.
The following clinical data were recorded in an anonymous database: age, gender, time interval between disease onset and CR, presence of fever, respiratory symptoms, and discharge diagnosis.
The study was approved by the local ethical committee (protocol 837/CE, CESC Treviso and Belluno).
Image acquisition
All CR were performed using a portable CR system (Multix; Siemens, Enlargen, Germany). PA and sitting AP CR had a tube voltage in the range of 110–140 kVp with Automatic Exposure Control. AP bedside CR was performed with 85 kVp and 4.0 mAs.
Image analysis
The most frequent CR findings of COVID-19 pneumonia (11–14) were identified by literature search and named “main alterations”: interstitial opacities (i.e. interlobular septal thickenings, resembling or not a reticular pattern); ground glass opacities (GGO); or consolidation. In our analysis, the superimposition of interstitial opacities and GGO were considered GGO.
All CRs were fully anonymized and assessed in random order. One chest radiologist with 7 years of experience in chest imaging (NL, reader 1) evaluated all CR. To assess intra-reader concordance, reader 1 repeated the analysis, after one month, on 100 randomly selected images. For the inter-reader concordance, two general radiologists, with 20 years (AD, reader 2) and 10 years (LB, reader 3) of experience, evaluated 50 randomly selected images. Radiologists were blinded to the clinical information of the patients.
All readers were asked to evaluate the following CR features: main alterations presence or absence, their uni-/bilaterality, prevalent location (upper, middle, lower, no prevalence), and distribution (peripheral, perihilar, no prevalence). Moreover, they had to define the predominant finding, as well as its location and distribution. Location was defined by three zones (upper, medium, lower), adapting the division in lung fields as previously described (15) (Fig. 1). Peripheral and perihilar distribution were defined as reported by Wong et al. (16) (Fig. 1). The presence of nodules, bands, cavitation, pneumothorax, pleural effusion, increased heart size (cardiothoracic ratio >0.5), or blurred contour of hilar pulmonary vessels (17,18) were also assessed.
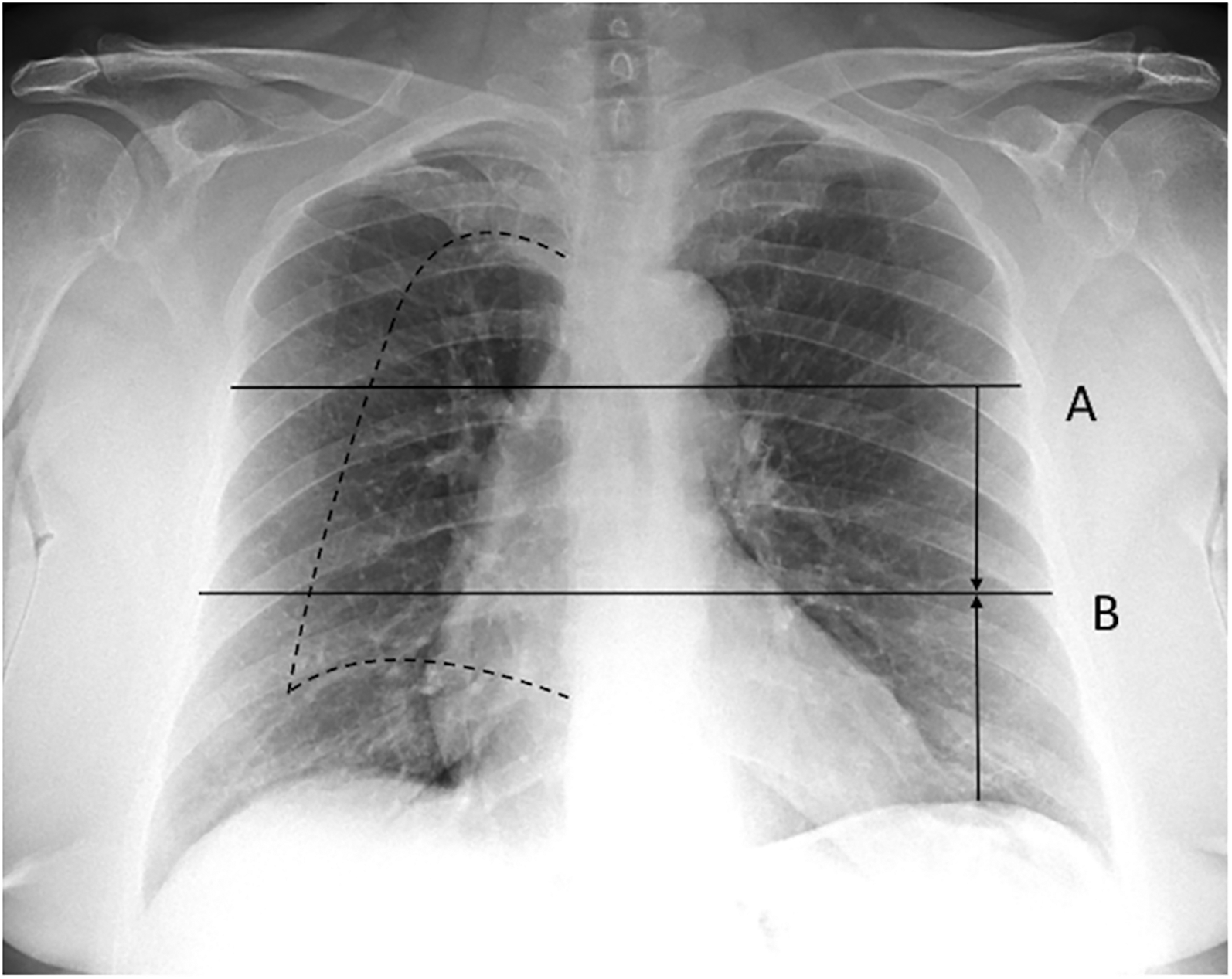
Chest radiography anatomical division. Location: Upper-middle-lower zones are identified by two anatomical landmarks: (a) the inferior wall of the aortic arch and (b) halfway between A and the dome of the lower hemi-diaphragm. Distribution: peripheral and perihilar zone are delimited by the halfway between the lateral edge of the lung and hilum (dotted line).
Each radiologist performed a preliminary training on 10 CR of COVID-19 pneumonia and 10 CR of non-COVID-19 pulmonary disease. CR exploited for the training were not included in the final dataset. All lung alterations were defined according to the Fleischner glossary of terms for thoracic imaging (19) (Supplementary Material).
Statistical analysis
Intra- and inter-reader agreements were investigated using intraclass correlation coefficient (ICC). We used a two-way mixed model for the intra-reader agreement and a two-way random model for the inter-reader agreement. ICC were considered as follows: <0.40 = poor; 0.40–0.59 = fair; 0.60–0.74 = good; and 0.75–1.00 = excellent (20). To define a COVID-19 pattern on CR, we considered the findings scored by the reader 1 with a good or very good intra-reader agreement. Moreover, the features should have been described in at least 10 individuals per group. All radiographic features were assessed as dichotomous variables according to presence or absence. We used these variables to calculate odds ratios (OR) (21) between COVID-19 and non-COVID-19 individuals, together with 95% confidence intervals (CI) and Fisher’s exact test (22). P < 0.05 was considered significant. We adopted Bonferroni correction for multiple testing (23).
Finally, considering only the variables with a significant P value, we defined a CR pattern to predict the presence of COVID-19 pneumonia compared to non-COVID-19 patients, using a binary logistic regression model (24): each radiographic feature that had a non-significant P value on the regression analysis was removed. Then, sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy of the selected CR features were calculated. Lastly, the same analysis was repeated to test the efficacy of the BSTI CR criteria for COVID-19, selecting the following variables: bilateral main alterations; prevalent peripheral distribution; prevalent lower localization; bilateral involvement; absence of pleural effusion; absence of blurred contour of hilar pulmonary vessels; and absence of pneumothorax. The data were analyzed using SPSS version 25.0 (IBM Corp., Armonk, NY, USA).
Results
Patients
A total of 300 patients had an available PA or AP CR. All patients with COVID-19 had confirmed COVID-19 pneumonia, while 21 non-COVID-19 patients were excluded because a diagnosis of pulmonary disease was ruled out at dismission. Five patients (four with COVID-19, one without COVID-19) were discarded because of low image quality.
Thus, 274 patients were finally included in the study (127 PA and 147 AP CR examinations): 146 (53%) patients with COVID-19 and 128 (47%) non COVID-19 patients (Fig. 2).
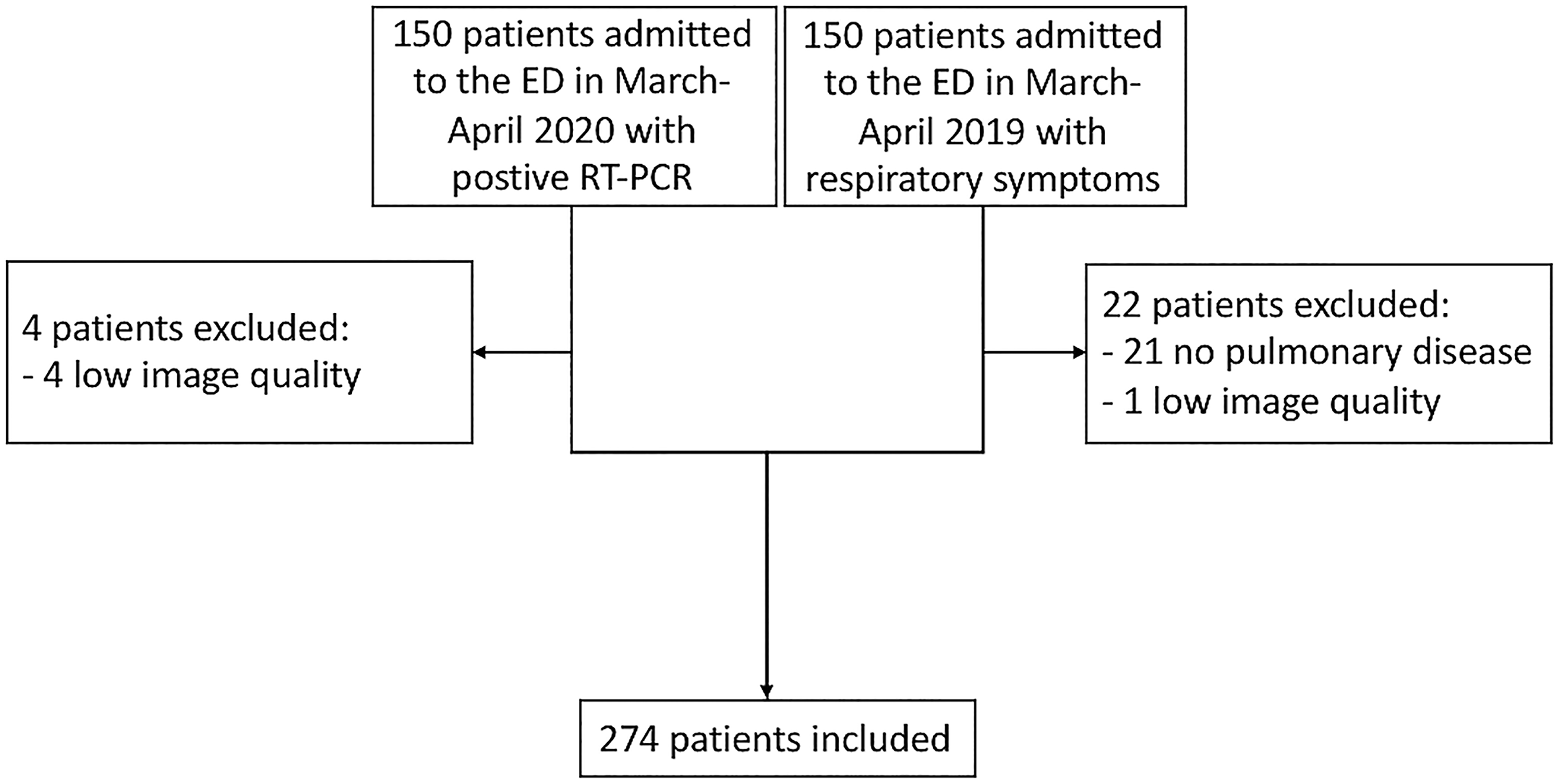
Flow chart of patients’ inclusion. ED, emergency department; RT-PCR, real-time reverse transcription polymerase chain reaction.
Among patients with COVID-19, 21 (14.4%) needed a CT scan at the time of diagnosis to confirm COVID-19 pneumonia. The final diagnoses of non-COVID-19 patients included the following: 64 (50%) cases of pneumonia other than COVID-19; 40 (31%) cases of cardiopulmonary disease (i.e. pulmonary edema or pulmonary embolism); 24 (19%) cases of other diseases, including bronchitis, suspected tumors, and chronic obstructive pulmonary diseases. The mean time interval between disease onset and CR ± standard deviation was 6.9 ± 3.9 days and 6.9 ± 9.1 days in COVID-19 and non-COVID-19 individuals, respectively. Patients’ characteristics are shown in Table 1.
Patient characteristics.
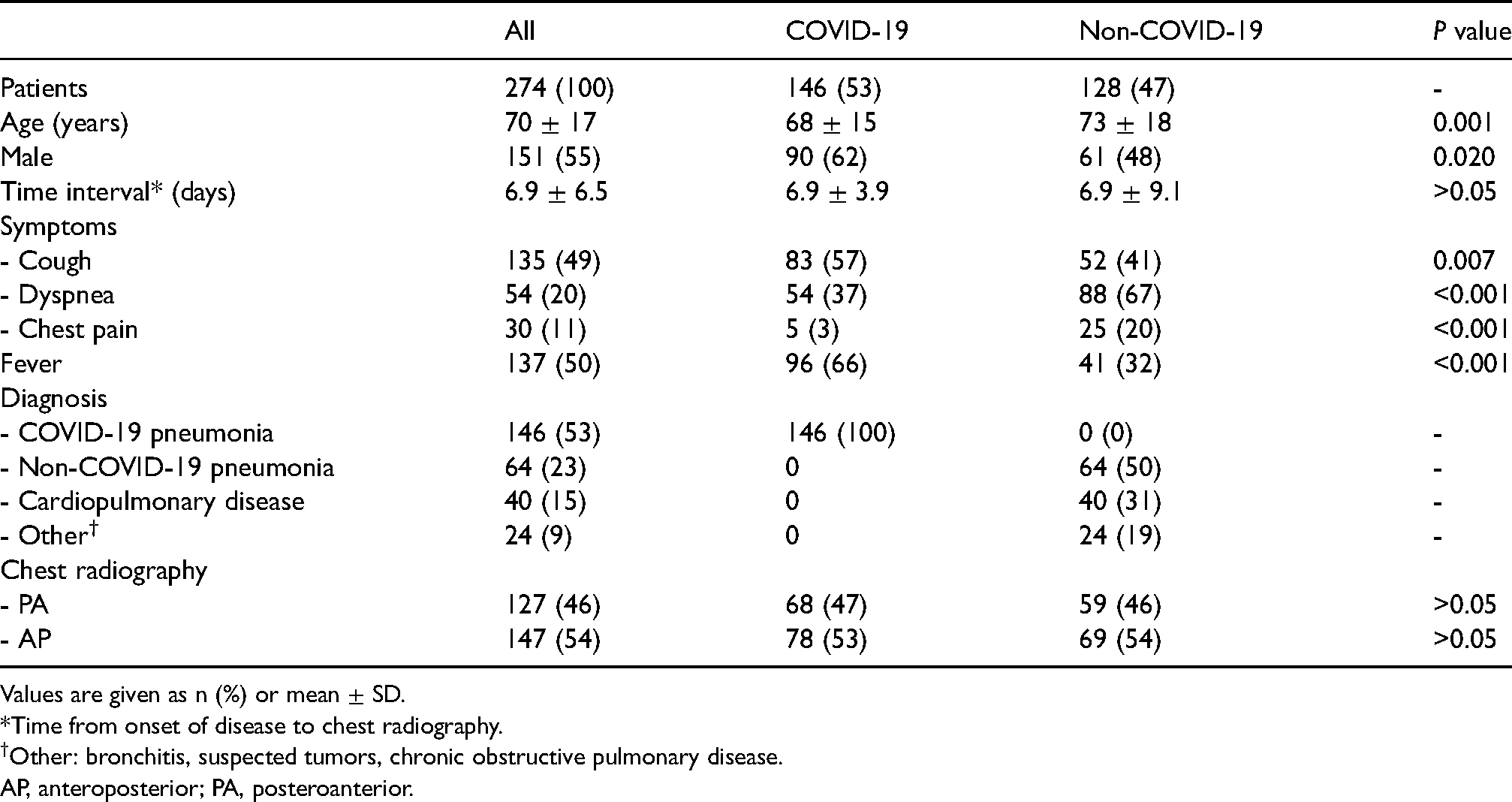
Values are given as n (%) or mean ± SD.
*Time from onset of disease to chest radiography.
Other: bronchitis, suspected tumors, chronic obstructive pulmonary disease.
AP, anteroposterior; PA, posteroanterior.
Intra-reader and inter-reader concordance
Intra-reader concordance was good or excellent for all variables, except for bands and increased heart size (fair). inter-reader concordance was moderate for most variables, except for prevalent localization (good), main alteration location (good, for reader 3), and blurred contour of hilar pulmonary vessels (fair, for reader 2). Intra and inter-reader agreements are shown in Table 2.
ICCs for intra- and inter-reader agreement.
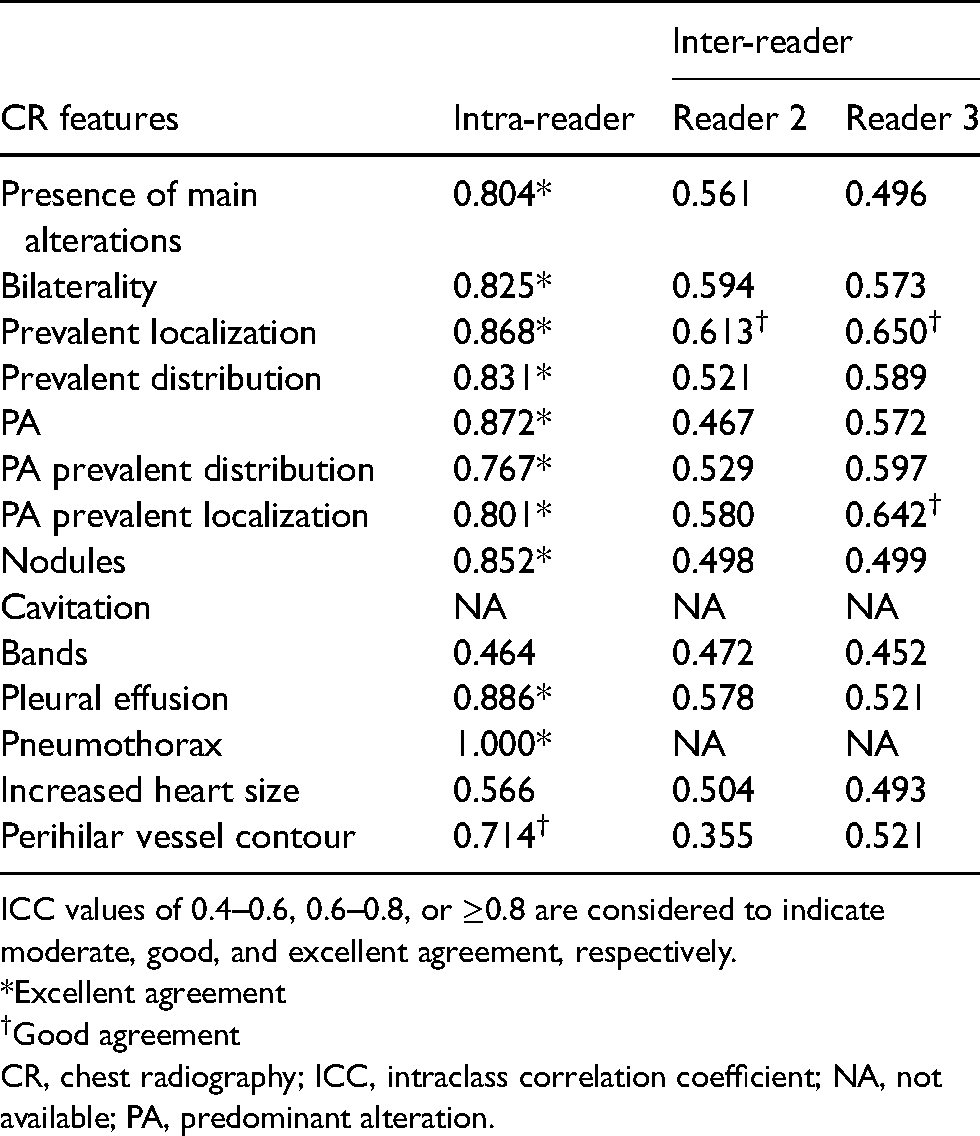
ICC values of 0.4–0.6, 0.6–0.8, or ≥0.8 are considered to indicate moderate, good, and excellent agreement, respectively.
Excellent agreement
Good agreement
CR, chest radiography; ICC, intraclass correlation coefficient; NA, not available; PA, predominant alteration.
CR findings and odds ratios
CRs were positive for main alterations in 104 (71%) COVID-19 and 69 (54%) non-COVID-19 patients. Main alterations were bilateral in 91 (62%) COVID-19 and 54 (42%) non COVID-19 patients. The most frequent location was the lower zone: 74 (51%) COVID-19 and 54 (43%) in non-COVID-19 patients. The prevalent distribution was usually peripheral in COVID-19 patients (n = 54, 38%), while there was no prevalence in 39 (30%) non-COVID-19 patients. The predominant CR feature was more often represented by interstitial opacities in both groups: 62 (42%) COVID-19 and 45 (35%) non-COVID-19 patients. The predominant CR feature was more often involving lower zones in both groups (79 COVID-19 patients [54%] and 52 non-COVID-19 patients [52%]), the periphery in COVID-19 patients (n = 61, 42%) and had no prevalent distribution in non-COVID-19 patients (n = 42, 33%). The contour of hilar pulmonary vessels was blurred in 26 (18%) COVID-19 and 42 (33%) non-COVID-19 patients. All CR features are reported in Table 3.
Chest radiography features of COVID-19 and non-COVID-19 patients.
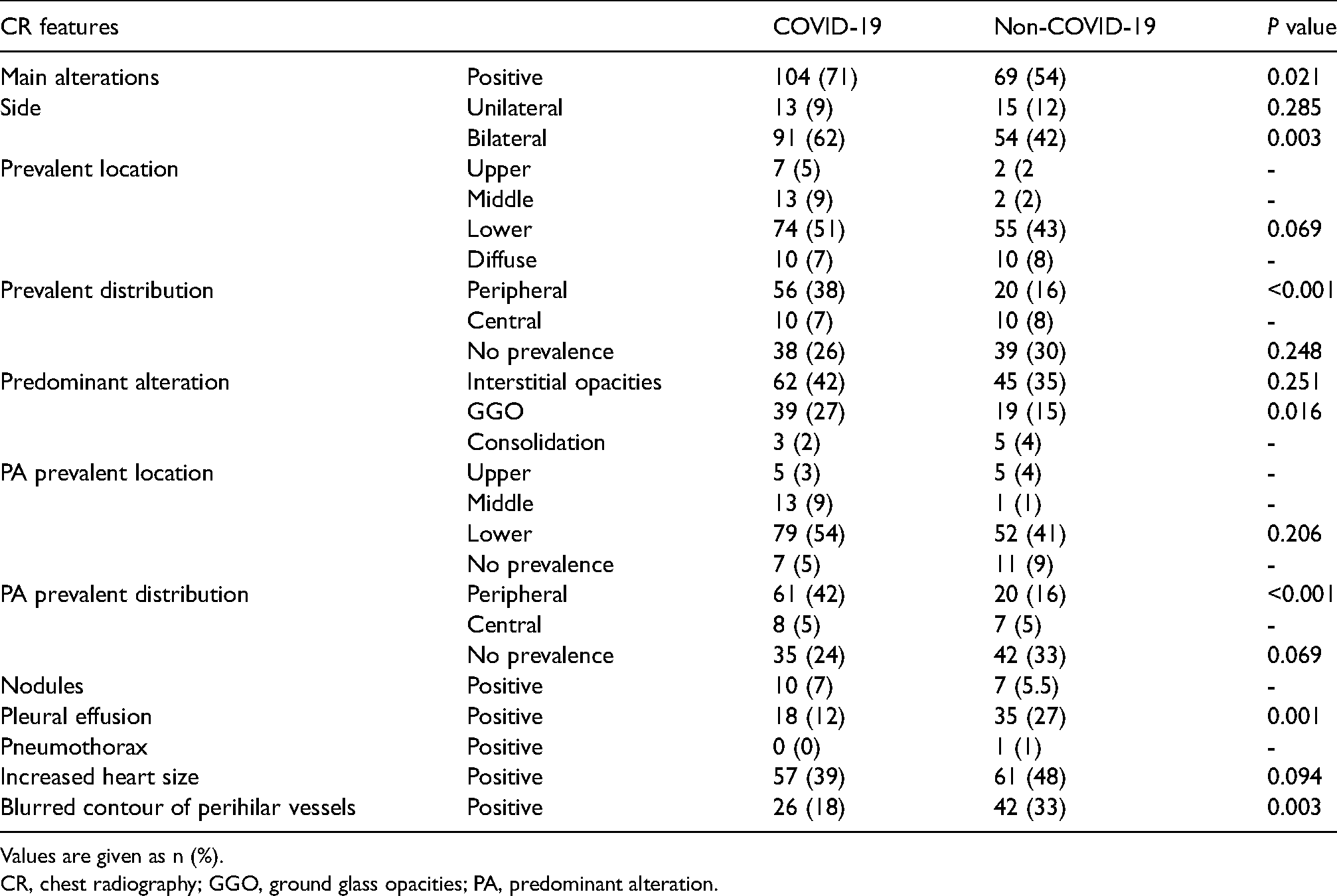
Values are given as n (%).
CR, chest radiography; GGO, ground glass opacities; PA, predominant alteration.
In total, 14 CR features were present with >10 patients per group, with good or very good intra-reader concordance, and were, therefore, further analyzed. After Bonferroni correction, the P value threshold was set to 0.003. Significant OR for patients with COVID-19 were as follows: bilaterality of main alterations (OR = 2.0, 95% CI = 1.2–3.3; P = 0.003); peripheral distribution (OR = 3.3, 95% CI = 1.8–5.8; P < 0.001); prevalent peripheral distribution of the predominant alteration (OR = 3.7, 95% CI = 2.0–6.5; P < 0.001); conversely, for non-COVID-19 patients, ORs were as follows: pleural effusion (OR = 0.4, 95% CI = 0.2–0.7; P = 0.001) and blurred contours of hilar pulmonary vessels (OR = 0.4, 95% CI = 0.3–0.8; P = 0.003).
Best CR COVID-19 pattern and BSTI model performance
By selecting the CR features with a significant P value, we tested them with a logistic regression to define the most specific CR COVID-19 features. The final pattern included four features (Table 4): bilateral main alterations (Expβ = 2.852, P = 0.002); prevalent peripheral distribution of the predominant alteration (Expβ = 2.287, P = 0.013); absence of pleural effusion (Expβ = 0.391, P = 0.009); and no blurred contours of hilar pulmonary vessels (Expβ = 0.341, P= 0.002). This pattern showed a sensibility of 48.6% (95% CI = 40.28–57.03), specificity of 81.3% (95% CI = 73.40–87.60), PPV of 74.7% (95% CI = 66.54–81.49), NPV of 58.1% (95% CI = 53.71–62.37), and accuracy of 63.9% (95% CI = 57.87–68.56). BSTI criteria showed a sensitivity of 50.7% (95% CI = 42.29–59.05), specificity of 76.6% (95% CI = 68.26–83.59), PPV of 71.2% (95% CI = 63.44–77.81), NPV of 57.7% (95% CI = 52.95–62.21), and accuracy of 62.8% (95% CI = 56.75–68.51).
Results of linear regression for CR features in COVID-19 pneumonia.
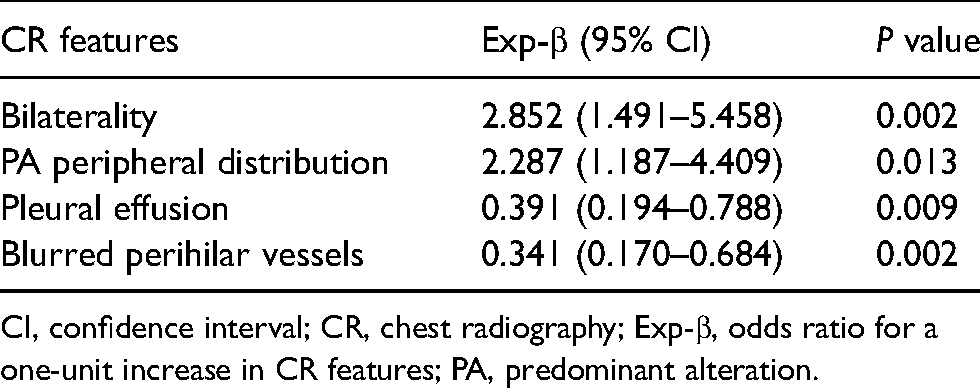
CI, confidence interval; CR, chest radiography; Exp-β, odds ratio for a one-unit increase in CR features; PA, predominant alteration.
Discussion
In the present study, we compared CR features of COVID-19 pneumonia to those of other pulmonary diseases, to determine the most accurate CR COVID-19 pattern for a confident diagnosis at the time of admission to the ED. We then compared these features to the BSTI criteria.
Our analysis showed that the most accurate CR pattern for COVID-19 pneumonia diagnosis consists of four features (Fig. 3): (i) bilateral main alterations (namely interstitial opacities, GGO, or consolidation); (ii) peripheral distribution of the predominant alteration; (iii) absence of pleural effusion; and (iv) contours of perihilar pulmonary vessels not blurred.
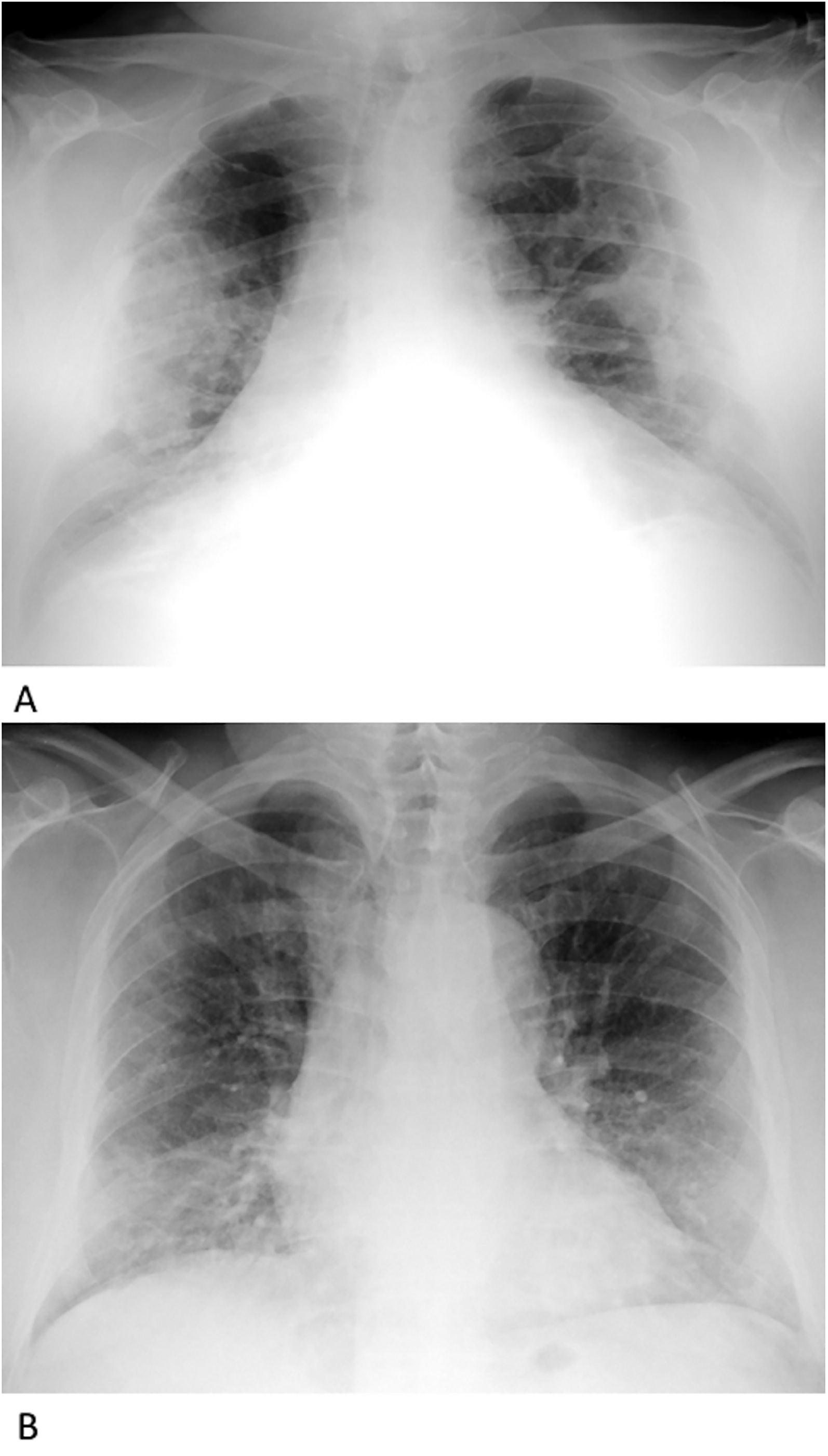
Application of COVID-19 pneumonia CR models. Sitting in AP CR, COVID-19 pneumonia fits our pattern: bilateral alterations, mostly sustained by GGO with a peripheral predominant distribution (consolidations are also present), absence of pleural effusion, and contour of perihilar vessels not blurred. The alterations mostly involve middle fields: this aspect does not fit the BSTI classic pattern. A nodule is also present in the upper zone of the right lung. Sitting in AP CR, COVID-19 pneumonia fits both our and BSTI classic patterns: bilateral alterations with predominant peripheral and lower involvement distribution (mostly by GGO in this example), absence of pleural effusion, pneumothorax or pulmonary edema, with contour of perihilar vessels not blurred. AP, anteroposterior; BSTI: British Society of Thoracic Imaging; CR, chest radiography; GGO, ground glass opacities.
Our pattern showed a slightly better performance than the BSTI criteria, with higher specificity. Looking at single CR features, the most interesting result is that a lower field distribution of alterations was confirmed as a common feature in patients with COVID-19 but did not result as a distinctive sign, being frequent also in non-COVID-19 patients. Conversely, bilaterality and peripheral distribution were confirmed as useful CR features to diagnose COVID-19 pneumonia. This is in agreement with the findings reported on CT by Shi et al. (25): they observed that in COVID-19 pneumonia all lung segments can be involved, with a prevalent peripheral distribution. Moreover, the peripheral distribution of the predominant alteration is more determinant from a differential diagnostic perspective. On the other hand, other features such as nodules, bands, cavitation, and pneumothorax were rarely encountered in both groups.
In the present study, we also exploited the observed findings to test the efficacy of the BSTI criteria, matching the results of some of the previous works, that directly applied to that model. In particular, the BSTI criteria obtained the same specificity of Tsakok et al. (76%) (26), though they observed higher sensitivity (60%), while Borakaty et al. (27) obtained a slightly higher sensitivity but lower specificity (56% and 69%, respectively). However, the latter considered only GGO among CR opacities, while we considered all most common CR features of COVID-19 pneumonia. Kemp et al. (28) found higher sensitivity and specificity (84 and 83%): nevertheless, statistical analysis was performed on readings by non-radiologists. Authors suggested that clinicians could have been prone to an overdiagnosis, as radiologists more often described CR as negative (data on radiologists’ analysis were not provided). Lastly, Hare et al. (8) described a 44% sensitivity and 100% specificity of the BSTI classic pattern. However, readers were informed on COVID-19 status: we believe that this approach may lead to a significant analysis bias.
Moreover, there are some differences in the aforementioned studies that need to be specified and that, in our opinion, may increase the strength of our work. First, in the other works, with the only exception of Hare et al. (8), patients were chosen in the same time period, splitting COVID-19 and non-COVID-19 by RT-PCR (25–27). However, RT-PCR can fail in the diagnosis of COVID-19 (4), especially in the early phase of COVID-19 disease, and patients with negative RT-PCR could have been wrongly included among non-COVID-19 patients. For this reason, we decided to enroll non-COVID-19 patients admitted to the ED the year before, when COVID-19 was not yet present. Additionally, we searched our archives during the same range of months (March–April), in order to have similar epidemiological/seasonal conditions. We then selected non-COVID-19 patients among those with respiratory symptoms, while Hare et al. (8) enrolled non-COVID-19 patients with cough and fever. Fever is one of the most common signs in patients with COVID-19 (9) but it was present in less than two-thirds of the total amount of our patients with COVID-19. Thus, we preferred evaluating non-COVID-19 patients with respiratory symptoms, regardless of fever, in order to address patients’ enrollment on chest disease only, but ensuring a large spectrum of possible differential diagnosis. Lastly, all studies (8,26–28) enrolled COVID-19 patients with positive RT-PCR, while we included COVID-19 patients with both RT-PCR positivity and reported diagnosis of COVID-19 pneumonia. In fact, patients with COVID-19 may be infected without evidence of pneumonia, as demonstrated by CT, the most sensitive imaging tool for COVID-19 pneumonia diagnosis (4). Similarly, we enrolled non-COVID-19 patients with a diagnosis of pulmonary disease.
Regarding inter-reader concordance, the moderate agreement for most of the features was not a surprise: a moderate inter-reader agreement was also observed in BSTI criteria application (8). This highlights the importance of cardiothoracic expertise in imaging evaluation of CR. Bands and heart size analysis had a poor to moderate intra-reader agreement; however, bands were uncommon in both groups and may not influence the resulting pattern. Regarding heart size, moderate intra-reader agreement was expected, since supine AP CR determines a magnification of the heart shadow that would need a correction (17). Following a similar rationale, we preferred to analyze the sharpness of hilar vessels contour (17,18) instead of hilar dimensions (29), as a possible sign of pulmonary edema: in fact, vascular pedicle dimension is also influenced by the same geometric issue (30).
The present study has some limitations. First, the patients were evaluated over a short period and the epidemiological background may not be representative of the whole year. Moreover, to create the CR pattern, we adopted the score of the most experienced reader. This choice aimed to select the radiologist dedicated to chest imaging, and, presumably, with the highest intra-reader concordance for all CR features. Second, protocols for disease diagnosis at the ED were different between COVID-19 and non-COVID-19 patients, as the combination of CR and LUS was specifically defined to manage the COVID-19 wave. Moreover, the ongoing therapy of admitted patients, such as antibiotics and corticosteroids, could have potentially modified imaging manifestation of COVID diseases at time of CR examination. Finally, although the heterogeneity of the non-COVID-19 group ensure a good representation of the general population with pulmonary diseases encountered at the ED, the small sample size per subgroup did not allow for the assessment of the influence of specific disease (i.e. pulmonary edema) in determining the final CT pattern. Further studies on a larger number of patients with a specific non-COVID-19 disease, such as other infective pneumonitis, are warranted.
In conclusion, we proposed a new CR pattern for the identification of COVID-19 pneumonia that should be helpful in differential diagnosis, consisting of four features: (i) bilateral involvement of interstitial opacities, GGO, or consolidations; (ii) prevalent peripheral distribution of the predominant alteration; (iii) absence of pleural effusion; and (iv) perihilar pulmonary vessels not blurred. Bilaterality and a predominant peripheral involvement are confirmed as features able to discriminate between COVID-19 pneumonia and non-COVID-19 pulmonary diseases, but lower field location is not specific for COVID-19 pneumonia. This pattern slightly outperformed the BTSI criteria in terms of specificity and accuracy.
Supplemental Material
sj-doc-1-acr-10.1177_02841851211055163 - Supplemental material for Chest radiography findings of COVID-19 pneumonia: a specific pattern for a confident differential diagnosis
Supplemental material, sj-doc-1-acr-10.1177_02841851211055163 for Chest radiography findings of COVID-19 pneumonia: a specific pattern for a confident differential diagnosis by Nicholas Landini, Giulia Colzani, Pierluigi Ciet, Giovanni Tessarin, Alberto Dorigo, Luca Bertana, Carla Felice, Luca Scaldaferri, Martina Orlandi, Cosimo Nardi, Micaela Romagnoli, Luca Saba, Roberto Rigoli and Giovanni Morana in Acta Radiologica
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.