
Abstract
Background
Although magnetic resonance imaging (MRI) is often the “gold standard” for diagnosing knee problems, it has many limitations. Therefore, ultrasonography has been suggested as an effective rapid alternative in many knee abnormalities, especially after injuries of the meniscus and collateral ligaments.
Purpose
To determine the diagnostic accuracy of point-of-care ultrasound (POCUS) in detecting injuries of the meniscus and collateral ligament compared to MRI.
Material and Methods
An observational cross-sectional blinded study was conducted of 60 patients with clinically suspicious meniscus and collateral ligament injuries who were planned for an arthroscopy and or operative procedure. These patients underwent both blinded POCUS and MRI of the knees before the intervention procedure and results of both imaging modalities were compared according to the operative and arthroscopic findings.
Results
The preoperative reliability of POCUS compared to MRI for the assessment of meniscus injuries was sensitivity (92.9% vs. 90.5%), specificity (88.9% vs. 83.3%), positive predictive value (PPV; 95.1% vs. 92.7%), negative predictive value (NPV; 84.2% vs. 79%), and overall accuracy (91.7% vs. 88.3%). However, for diagnosing collateral ligament injures, POCUS versus MRI assessed sensitivity (92.3% vs. 88.5%), specificity (100% vs. 97.1%), PPV (100% vs. 95.8%), NPV (94.4% vs. 91.7%), and overall accuracy (96.7% vs. 93.3%).
Conclusion
Ultrasonography is a useful screening tool for the initial diagnosis of meniscal and collateral ligament pathology compared to or even with potential advantages over MRI, especially when MRI is unavailable or contraindicated. As newly advanced portable ultrasonography becomes available, it could be considered as a point-of-injury diagnostic modality.
Keywords
Introduction
Acute knee pain affects many people in the world, accounting for approximately 25% of adults, with an increasing prevalence of almost 65% over the past 20 years (1). It is usually caused by a wide variety of causes, either injury or disease. In its initial evaluation, especially in primary care centers, the exclusion of urgent causes of injuries of the meniscus (medial and lateral) and ligaments (collaterals; medial, lateral and cruciate; anterior and posterior) is mandatory for considering the need for referral (2).
Injuries of the meniscus may be the most common knee injury, with a prevalence rate of 61 cases per 100,000 people, more common in men with a peak age incidence of 31–40 years (3). In addition, affection of knee ligaments after an injury can easily occur, especially the medial collateral ligament, which is the most common knee ligament affected after injury, with an incidence rate of 7.3 per 1000 (4,5).
As the menisci play an important role in the stabilization of the knee joint, their damage leads to exposing the cartilage to shear forces resulting in early degenerative changes and osteoarthritic changes, especially in young people (6). The timing and accuracy in the diagnosis of this injury are important factors for the prognosis and decline of its morbidity rate (7).
At the beginning of the 1980s, magnetic resonance imaging (MRI) was introduced as a non-invasive tool for the assessment of knee pathology, especially menisci and ligaments with high sensitivity and specificity of 79%–93% and 88%–96%, respectively, in the detection of meniscal tear (8), and sensitivity and specificity of 85% and 90%, respectively, for the diagnosis of collateral ligament (CL) injuries (9). Therefore, it was considered a “golden standard” imaging modality for these problems. However, it is associated with misdiagnosis in some cases, in addition to its high cost, occasional unavailability, and limitations of its use in cases of cardiac pacemakers and metal implants (10).
Recently, ultrasound (US), being cheaper, available, non-ionic, dynamic study, and with no contraindication, was suggested to play a role in the diagnosis of knee meniscus and CL pathology with high sensitivity and specificity, therefore, raising potentiality as a rapid diagnostic screening test or when MRI is a contraindication (11–13).
The aim of the present study was to determine the accuracy of point-of-care ultrasound (POCUS) in diagnosing meniscus and CL injuries when compared to MRI, especially in emergency and clinical site situations.
Material and Methods
Study design
A prospective observational cross-sectional blinded study was conducted of patients with knee pain and suspected injuries of the meniscus and CLs who were planned for operative and/or arthroscopy procedures and attending our Radiology Department for preoperative imaging, during the period from June to December 2020. Written informed consent, including publishing radiological images of all individuals, was obtained after a thorough study protocol explanation. This study was approved by the Research Ethics Committee of the Faculty of Medicine, Ain Shams University in Egypt (FWA000017585) on 25 June 2020 (Reference number of approval: FMASU R27/2020).
Patients
A total of 60 patients aged 18 years and older, who presented for knee imaging for various reasons (such as trauma, pain, swelling, and instability), with clinical suspicion of meniscal and/or CL injuries, and planned for operative and or arthroscopy procedures after MRI were included in the study. Exclusion criteria included patients with fractures/dislocation, rheumatoid arthritis, previous knee operations, or those with limitations of MRI (cardiac pacemakers, metal implant, or claustrophobia), in addition to those refusing to participate in the study or who did not complete it till the end of arthroscopy.
These patients underwent full history taking, thorough clinical examination, and MRI of the knees; then, blinded POCUS was appointed and done by another radiologist with a maximum interval of three days between both imaging modalities to avoid changes in the appearance of the findings. Both MRI and POCUS studies were interpreted with different radiologists with at least five years of experience in MRI or US imaging of the joints and musculoskeletal system and they were blinded about the other imaging results. Follow-up of the arthroscopy procedures (served as the reference standard for the study of the meniscus) and the operative interventions (served as the reference standard for the study of collateral ligaments) was then carried out and the results of both imaging modalities were later compared according to interventional findings.
The technique of non-contrast MRI
All metallic objects were removed from the patient’s body and the patient was placed in a supine position. A 1.5-T Philips scanner (Achieva Medical Systems, Andover, MA, USA) was used, using a special knee coil. A standard MRI morphological sequence protocol for the knee in all orientations including axial T2-weighted (T2W) imaging, axial proton density (PD), sagittal PD, sagittal T2W imaging, and coronal STAIR without contrast was used. To maximize spatial resolution, we used small fields of view (14–16 cm), thin slices (3 mm), and a high matrix size. Axial views parallel to the knee joint line included the whole patella and fibular head, while sagittal oblique views parallel to the medial aspect of the lateral condyle included both CL and coronal views parallel to the posterior aspect of the femoral condyles included the entire patella to 2 cm posterior to femoral condyles. All MRI data were transferred to the workstation, where image analysis and interpretations were performed.
The technique of knee US examination
Many machines were used, including the Siemens ACUSON Juniper. The patient was placed in a supine position, using a high-resolution linear multi-frequency transducer 9–15 MHz (ideally 12 MHz) superficial probe. The knee was divided into anterior, medial, lateral, and posterior compartments for structured evaluation of the tendons, ligaments, joint space, and osseous structures, as well as peripheral nerves and vasculature. The medial and lateral menisci were evaluated in the medial and lateral (body and anterior horns) and posterior (posterior horns) compartments, while the medial collateral ligament (MCL) and lateral collateral ligament (LCL) were evaluated in the medial and lateral compartments, respectively (14).
To examine the menisci, the transducer was placed longitudinally spanning the joint line and always oriented perpendicular to the meniscus. The anterior horns and mid-zones could be imaged with the patient supine or in the lateral decubitus position with the knee extended; the posterior horns were imaged with the patient prone. Dynamic flexion and rotation could help open the joint line to improve visualization, especially with applying mild valgus or varus stress to image the medial and lateral meniscus, respectively.
The MCL was visualized in the coronal plane, and axial images also were obtained while the patient remained in the supine position but rotated the hip externally. The MCL extended from the medial femoral condyle to the medial tibial metaphysis, appearing as thin hyperechoic bands comprising superficial and deep components separated by hypoechoic fibro adipose tissue.
The LCL complex was imaged with the patient supine and the leg in internal rotation or the lateral decubitus position. The iliotibial band (ITB) was positioned somewhat anteriorly, and the fibular collateral ligament and biceps femoris tendon were just posterior. The fibular collateral ligament was a thin band extending from the lateral femoral epicondyle to the fibular head and appeared slightly hypoechoic (15).
Imaging analysis
MRI and US findings were analyzed for injuries of both the meniscus and CLs. Meniscus injuries were noted as either degeneration (diffuse, ill-defined pattern of hypoechoic changes), tear (well-defined anechoic or hypoechoic disruption and/or cleft), extrusion (abnormal displacement of meniscus tissue and associated edema), or peri-meniscal cysts (anechoic or hypoechoic cystic structures found within the substance of the meniscus).
On the other hand, CL injuries or tears were classified as follows: Grade 1 = mild, ligament stretching without discontinuity of the fibers and associated edematous changes; Grade 2 = moderate, partial tear or disruption of the ligament; or Grade 3 = severe, complete tear appears as discontinuity of ligament fibers and/or retraction, often associated with hematoma (16).
Statistical analysis
All data were subjected to statistical analysis, tabulation, and comparison, using SPSS version 23 (IBM, Armonk, NY, USA). Quantitative data were described in terms of range, mean and standad deviaton (SD), while qualitative data were presented as numbers and percentages (%). In addition, sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy were calculated for the data when appropriate.
Results
A total of 60 patients (45 men, 15 women; age range = 18–60 years; mean age = 32.9 ± 13.3 years) were included in the present study (Table 1).
Distribution of patients according to age and sex among our patients.
Values are given as n (%).
According to arthroscopic evaluation, identifiable meniscal pathology was detected in 42 patients (70%), of which 32 were medial menisci and 10 were lateral menisci. The statistical parameters (sensitivity, specificity, PPV, NPV, and accuracy) for both POCUS and MRI assessments of meniscal pathology are presented (Tables 2 and 3). Meniscal tears included different radial, horizontal, and longitudinal tears, mostly affecting posterior horns of the medial meniscus or both horns of the lateral one. US was not able to detect two medial meniscal (MM) tears and one lateral meniscal (LM) tear diagnosed on arthroscopic examination, while MRI was not able to detect three MM tears and one LM tear (Tables 2 and 3). The four meniscus tears missed on MRI were all radial tears. On the other hand, two false-positive cases of meniscus injury (one MM and one LM) were diagnosed by US, while MRI detected three false-positive cases (two MM and one LM) (Tables 2 and 3).
The results of POCUS and MRI in the diagnosis of meniscus pathology compared to the arthroscopy results as the reference.
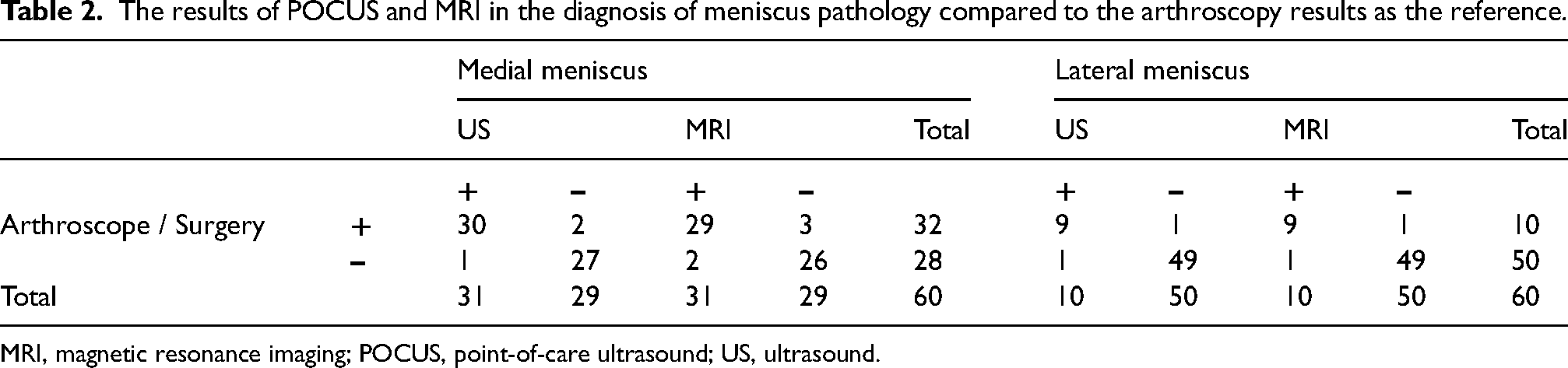
MRI, magnetic resonance imaging; POCUS, point-of-care ultrasound; US, ultrasound.
Statistical parameters and diagnostic accuracy of POCUS & MRI in the diagnosis of meniscus pathology compared to the arthroscopy results as the reference.
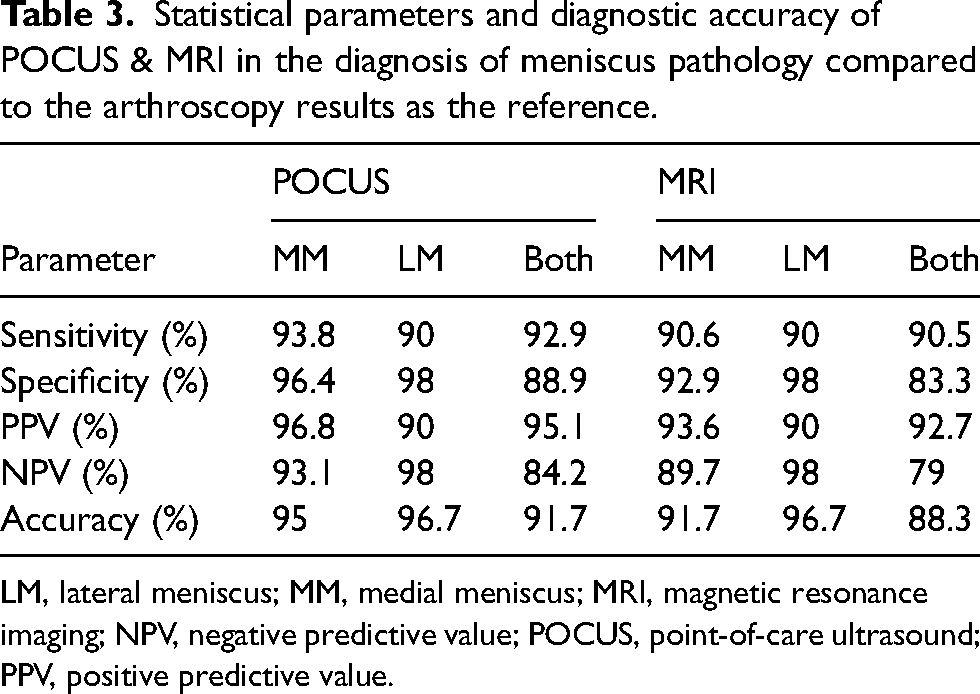
LM, lateral meniscus; MM, medial meniscus; MRI, magnetic resonance imaging; NPV, negative predictive value; POCUS, point-of-care ultrasound; PPV, positive predictive value.
With regard to CL, the operative evaluation identified 26 patients (43.4%) with ligament pathology (18 medial and 8 lateral) of different grades. The statistical parameters for both POCUS and MRI assessments of CL pathology are presented in Tables 4 and 5. US was not able to detect one medial tear and one lateral CL tear detected intraoperatively, while MRI was not able to identify two medial CL tears and one lateral CL tear. In addition, no false-positive cases were diagnosed by US, while MRI showed one false-positive case of medial CL tear (Tables 4 and 5). A comparison of the overall accuracy of US and MRI in the detection of both meniscus and CL is demonstrated (Fig. 1).
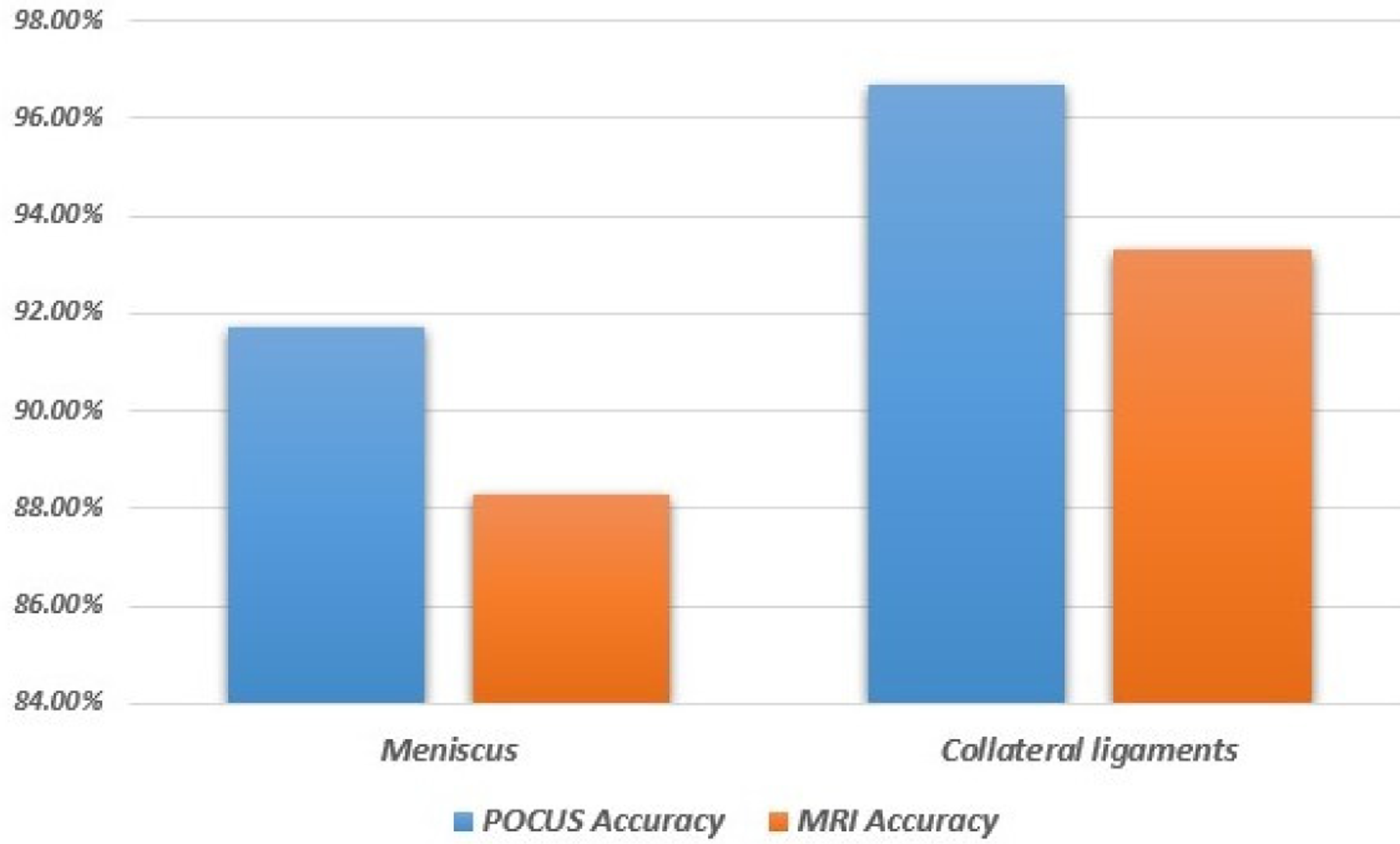
Comparison of POCUS and MRI diagnostic accuracy in detection of both meniscus and collateral ligaments pathology compared to arthroscopy findings. MRI, magnetic resonance imaging; POCUS, point-of-care ultrasound.
The results of POCUS and MRI in the diagnosis of collateral ligament pathology compared to the postoperative results as the reference.
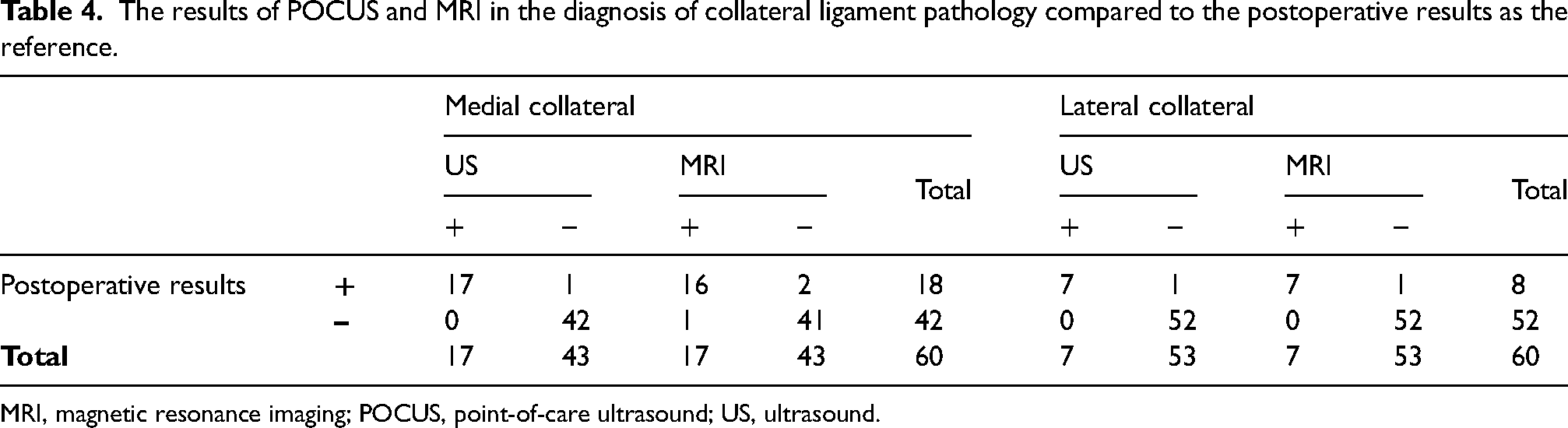
MRI, magnetic resonance imaging; POCUS, point-of-care ultrasound; US, ultrasound.
Statistical parameters and diagnostic accuracy of POCUS and MRI in the diagnosis of collateral ligament pathology compared to the postoperative results as the reference.
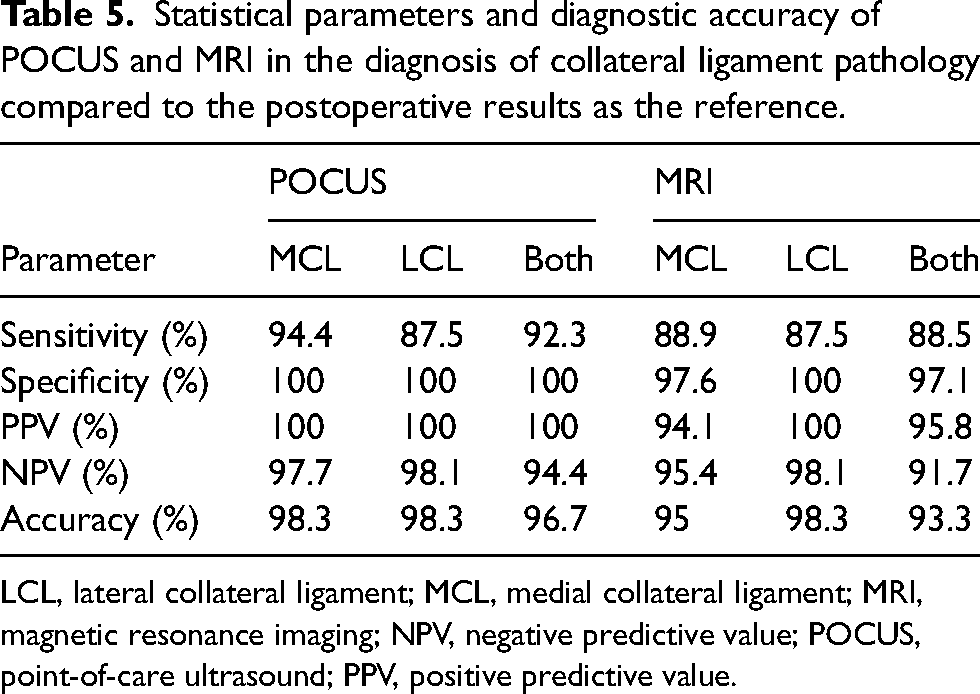
LCL, lateral collateral ligament; MCL, medial collateral ligament; MRI, magnetic resonance imaging; NPV, negative predictive value; POCUS, point-of-care ultrasound; PPV, positive predictive value.
Some of our cases with meniscus and CL pathology are presented in Figs. 2–6.
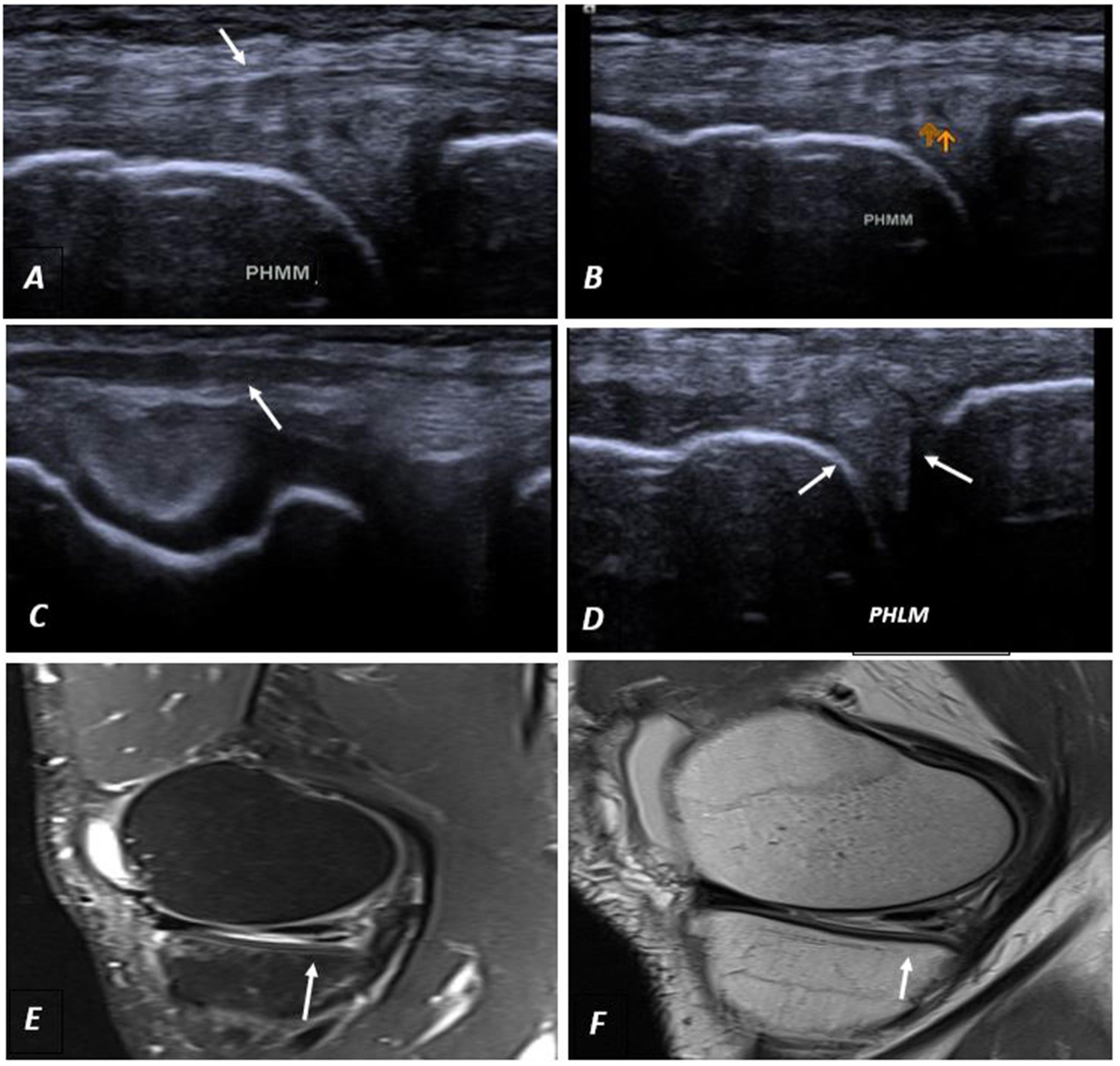
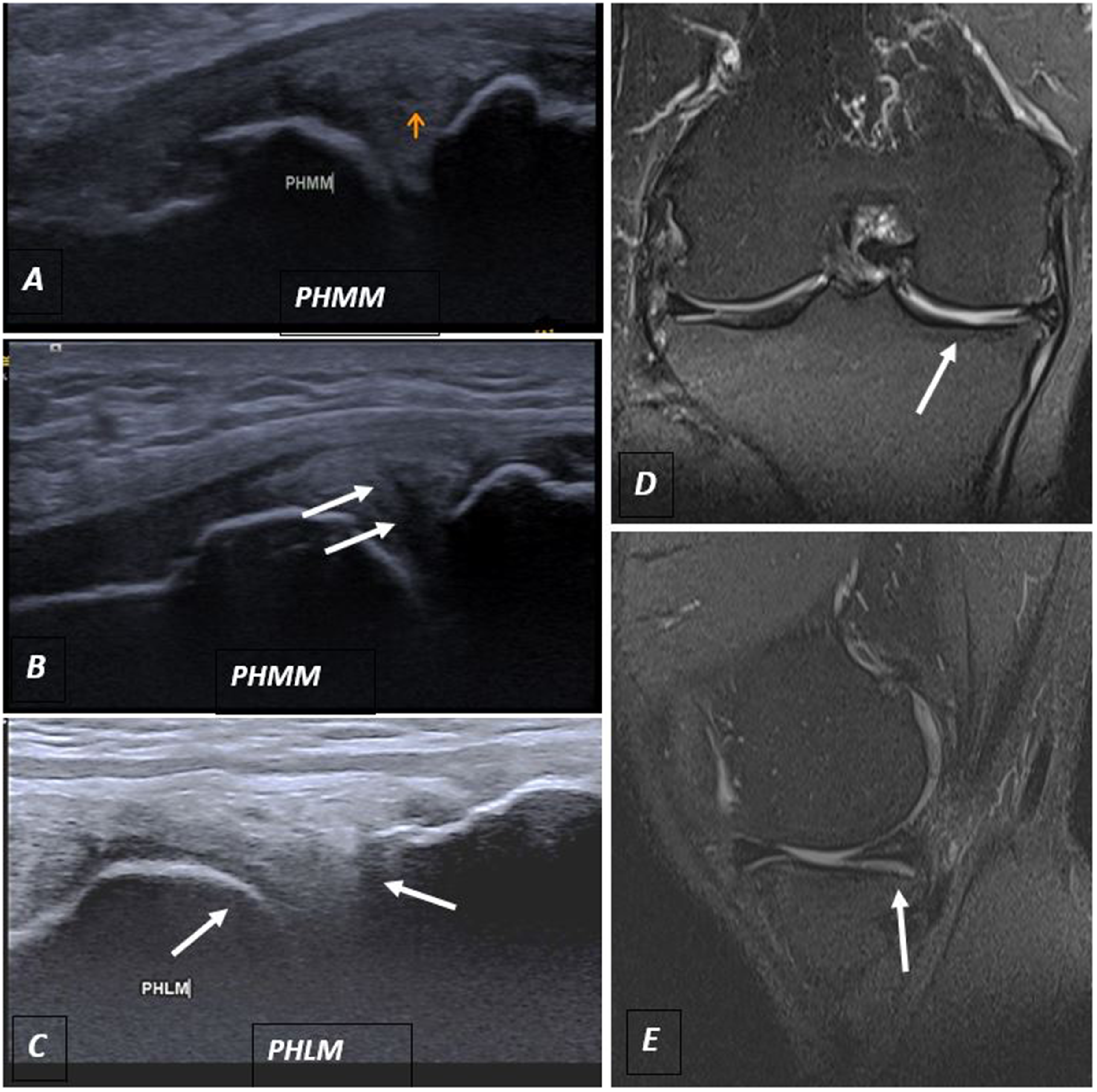
A case with PHMM horizontal tear touching the articular surface as detected on the US and MRI. (a, b) Grayscale US finding of the normal appearance of the medial collateral ligament (white arrow in a) and linear hypoechoic tear of the PHMM touching the articular surface (two orange arrows in b). (c) The US shows normal lateral collateral ligament (white arrow). (d) The US shows a normal lateral meniscus (white arrow). (e, f) On MRI of the same patient, sagittal STAIR sequence and sagittal gradient sequence show grade 3 injury of the PHMM with linear signal intensity reaching to the inferior articular surface (white arrow) indicating a horizontal tear. MRI, magnetic resonance imaging; PHMM, posterior horn of medial meniscus; US, ultrasound.
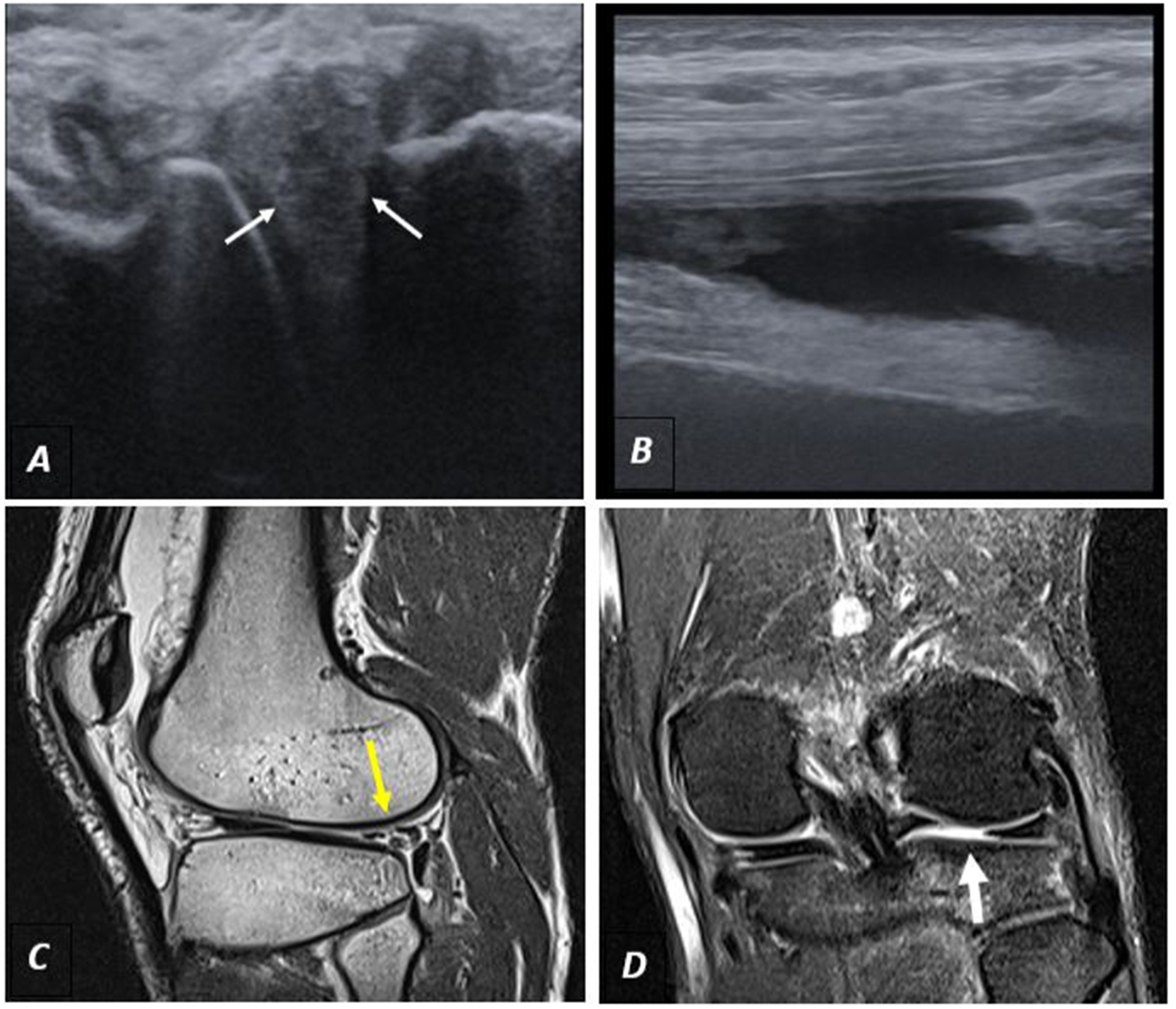
A case with a lateral meniscus tear touching the articular surface detected on the US and MRI. (a) Grayscale US finding of hypoechoic tear touching the articular surface (white arrow). (b) The US detected an associated knee effusion that appeared as an anechoic fluid inside the joint. (c, d) On MRI of the same patient, sagittal PD in (c) and coronal STAIR in (d) show tear traversing the lateral meniscus body (yellow arrow in c and thick white arrow in d). MRI, magnetic resonance imaging; PD, proton density; US, ultrasound.
A case with a medial meniscus tear and meniscal extrusion as well degeneration of the posterior horn lateral meniscus as detected on US and MRI. (a, b) US images show a hypoechoic root tear of the PHMM with subsequent meniscal extrusion (white arrow). (c) The US shows heterogeneous posterior horn lateral meniscus with hypo- and hyperechoic areas denoting its degeneration (white arrow). (d) On MRI of the same patient, coronal STAIR shows root tear of the medial meniscus with meniscal extrusion (white arrow). (e) On MRI, sagittal STAIR high signal in the body of the lateral meniscus does not reach the articular surface denoting its degeneration (white arrow). MRI, magnetic resonance imaging; PHMM, posterior horn of medial meniscus; US, ultrasound.
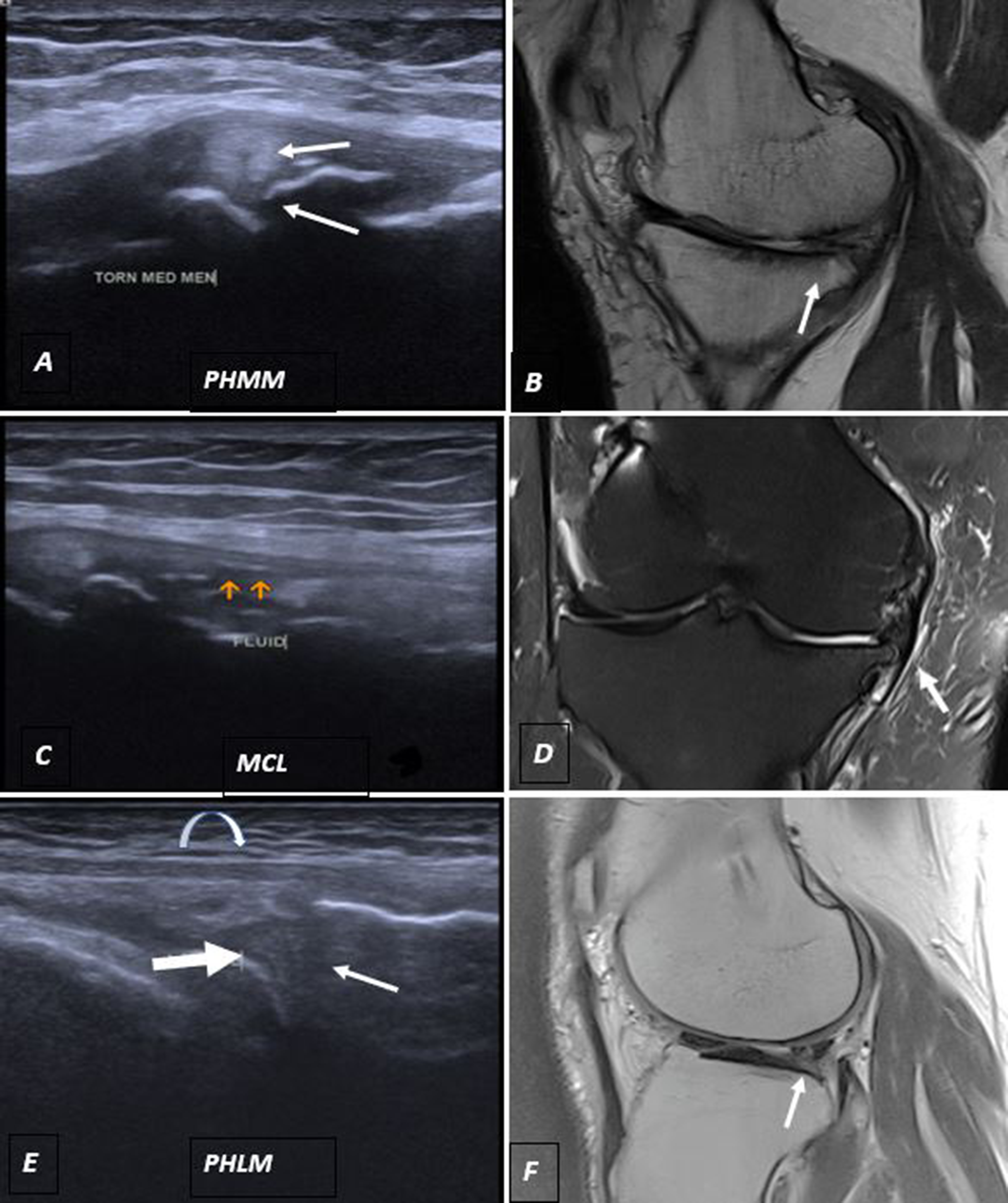
A case with posterior horn medial meniscus tear, medial collateral ligament grade I sprain, and lateral meniscal degeneration on US and MRI. (a) The US shows PHMM hypoechoic tear touching the articular surface with meniscal extrusion (white arrow). (b) MRI sagittal PD shows torn PHMM with ghost meniscal sign denoting its tear (white arrow). (c) US shows fluid collection around the medial collateral ligament (orange arrow) associated with marginal osteophyte. (d) MRI coronal STAIR sequence shows a fluid signal surrounding the medial collateral ligament (white arrow) denoting MCL grade I sprain. (e) US shows internal heterogeneity affecting the PHLM (white arrow) denoting its degeneration with a normal appearance of the lateral collateral ligament (curved arrow). (f) MRI sagittal PD shows a high signal inside the PHLM (white arrow) reaching the inferior articular surface denoting its tear (which was misdiagnosed in the US as a degeneration). MCL, medial collateral ligament; MRI, magnetic resonance imaging; PD, proton density; PHLM, posterior horn of lateral meniscus; PHMM, posterior horn of medial meniscus; US, ultrasound.
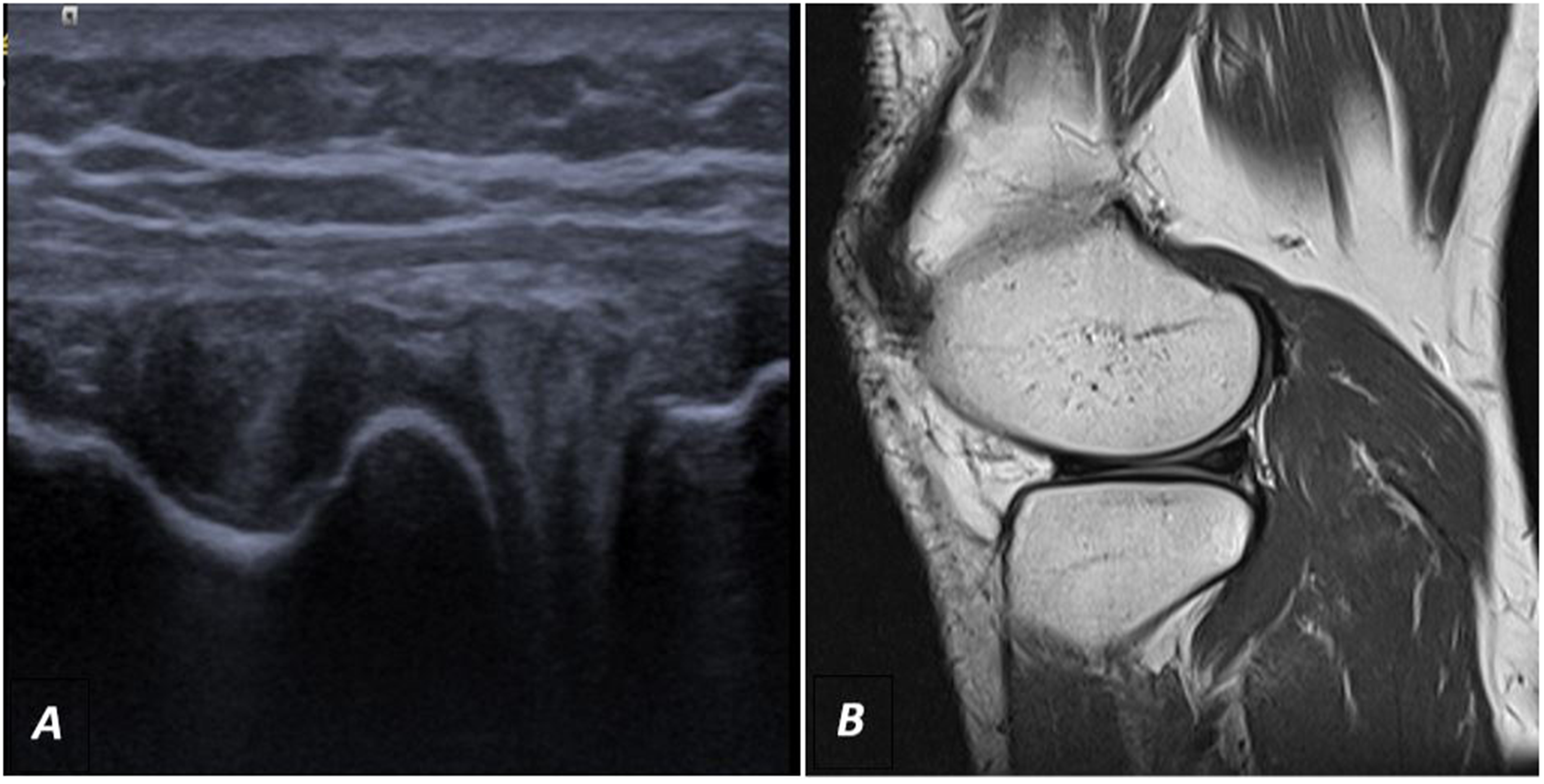
A case with an anterior and posterior horn lateral meniscus degeneration on both US and MRI. (a) US gray-scale shows hypoechoic areas inside the anterior and posterior horn of the lateral meniscus not reaching the articular surface, denoting their degeneration. (b) MRI sagittal images of the same patient show high signal intensity inside the AHLM and PHLM denoting their degeneration. AHLM, anterior horn of lateral meniscus; MRI, magnetic resonance imaging; PHLM, posterior horn of lateral meniscus; US, ultrasound.
Discussion
The most painful source during knee injuries results from soft-tissue injuries of the meniscus and CLs, which have become popularly diagnosed by US replacing MRI (17,18). These injuries were found to be more prevalent in young people and men in the present study, as they are more exposed to sports injuries, which is in accordance with the results of previous reports (18–20).
Injury to menisci usually occurs secondary to twisting injury of the knee, while the foot is anchored to the ground as may occur with twisting sports (21).
In the present study, meniscal injuries were detected via arthroscopy in 42 of 60 patients (70%) with a higher incidence of MM injury detected in 32 patients compared to only 10 patients with LM injuries. In fact, the medial and lateral menisci vary in size, attachments, and load transmission, and the MM is more vulnerable to injury, about five times than the lateral ones (21), due to its firm attachment to the MCL (usually injured together) and joint capsule (16), which matches our results. On the other hand, the LM, on the outside of the knee, is more circular in shape and moveable, making it less prone to tear, except when the anterior cruciate ligament is injured (22).
When comparing preoperative blinded US and MRI of meniscus pathology in our patients to their arthroscopic findings, US showed higher diagnostic parameters regarding the detection of MM injury while both were similar in the detection of LM injury. US was not able to detect two MM tears and one LM tear diagnosed on arthroscopic examination, which was explained by them being small tears that cannot be seen by US which is still an operator-dependent technique, while MRI was unable to detect three MM tears and one LM tear as they were all radial tears.
The overall sensitivity and specificity for US detection of meniscus injuries is in the range of 83%–97.2% and 83%–100%, respectively, as was found by previous studies (16,23). Cook et al. (12) reported sensitivity (91.2% vs. 91.7%), specificity (84.2% vs. 66.7%), PPV (94.5% vs. 84.6%), NPV (76.2% vs. 80%), and overall accuracy (89.5% vs. 81.1%) for both US and MRI of meniscus pathology, supporting our results. This could be attributed to the finding that radial meniscal tears are difficult to visualize on MRI, which accounts for a large number of tears missed by MRI (24). Therefore, US, being more dynamic, was found to be twice as likely than MRI to correctly determine the presence or absence of meniscal pathology seen arthroscopically and is therefore considered a useful tool for the diagnosis of meniscal pathology with potential advantages over MRI (12). On the other hand, the presence of some false-positive cases of tears diagnosed by MRI or US may be attributed to subjective bias of radiologists (25), in addition to the possibility of difficult visualization of the tears of inferior surfaces of menisci at surgery as mentioned by Crawford et al. (24).
In another study comparing US imaging to arthroscopic results, Najafi et al. (13) found that the accuracy rate of US in diagnosing tears of the medial meniscus (98%) was a little higher than that of the lateral ones (97%), which matches our findings. In addition, Behairy et al. (25) found the same result using MRI. In fact, as the posterior horn of the MM is larger than the anterior one, contrary to the LM which has equal-sized horns, this may make the MM easier to be imaged and detect its pathology compared to the LM.
By comparing US to MRI, Unlu et al. (26) found that US imaging was not as efficient as MRI in the detection of meniscal degeneration but more effective in the diagnosis of tears; therefore, they stated that it is not a suitable substitute for MRI in the routine diagnostic evaluation of meniscus lesions. However, they recommend it as a quick exam to stratify patients for further evaluation in selected cases such as young patients, traumatic cases, and cases with a contraindication for MRI (26).
In addition, Ghosh et al. (16) on comparing POCUS imaging to MRI, as a standard assessment for meniscus injury as mentioned before, determined US sensitivity (100%), specificity (50%), PPV (87.5%), and NPV (100%). This was also emphasized by other authors, who studied both horns (anterior and posterior) of the MM and LM and found almost 100% comparable results to MRI (13,27), which led Hussein et al. to conclude that there was no statistically significant difference between US and MRI in the detection of meniscal injury (20).
With regard to CL injuries, 26 patients (43.4%) in the present study were diagnosed with CL pathology (18 medial and 8 lateral) by operative findings. Ultrasound showed higher diagnostic accuracy compared to MRI in the detection of MCL injury while both were similar in the diagnosis of LCL injuries. US was not able to detect one medial tear and one lateral CL tear that were detected intraoperatively, while MRI was not able to identify two medial tears and one lateral tear.
Theoretically, visualizing the CLs, especially the medial ones, under US is relatively easy due to their superficial location, which makes them often injured together with the meniscus. However, data on the sensitivity and specificity of US use in diagnosing CL tears are not as abundant as in meniscal injuries (16).
By comparing US imaging of 30 patients with meniscal-ligamentous injuries of the knee to MRI, Hussein et al. (20) found a highly significant association between the results of MRI and US with a sensitivity of 80% and specificity of 100% for US in the detection of CL injury. In addition, Ghosh et al. (16) found that US demonstrated a sensitivity of 67% and specificity of 83% in the detection of medial CL tears yielding a PPV of 67% and NPV of 83% with a correlation between POCUS and MRI findings in the majority of cases.
The advantages of US over MRI in the diagnosis of the meniscus and CL tears after knee injuries are related to its effectiveness, especially with new high-quality US machines available on laptops and hand-held versions, which allows for point-of-injury diagnostic imaging, in addition to financial and comfort (portability) benefits with reducing costs and efforts. Of course, the availability of easy bilateral comparison and repetition is a great advantage for accurate US studies. In addition, dynamic imaging in the US allows for perfect assessment of meniscus and CL with knee movement, contrary to MRI, reducing unnecessary further imaging or surgeries with its related morbidities (12,28).
However, it should be mentioned that there are some limitations for the use of POCUS, including the availability of well-experienced musculoskeletal radiologists with inter- and intra-observer variability, and the need for continuously updated protocols for this assessment. In addition, further studies with a larger number of patients are recommended to evaluate the real accuracy of US imaging in comparison to the higher strength (3-T) MRI machines. Moreover, we should emphasize that this study was targeted to the evaluation of meniscus and CLs; however, other internal elements of the knee such as cruciate ligaments, cartilage, and others were not evaluated, and so MRI assessment will be requested, if the injury of these elements was suspected, or if we need a comprehensive full evaluation of the knee pathology (12).
In conclusion, this study stressed the role of US as a useful screening tool for the initial diagnosis of meniscus and CL pathology mostly after injury compared to or even with potential advantages over MRI, especially when it is unavailable or contraindicated. As newly advanced portable ultrasonography equipment becomes available, it could be considered for use as a point-of-injury diagnostic modality for these problems.
Footnotes
Acknowledgements
The authors thank all the study participants for their patience and support.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.