
Abstract
Background
There are not many studies on the differences of ultrasound (US) findings between epidermal cysts (ECs) located in the trunk and those in the extremities.
Purpose
To compare the sonographic findings of ECs according to location in the body (trunk vs. extremity) and evaluated the feasibility of strain elastography (SE).
Material and Methods
This is a retrospective study of 76 patients with surgically confirmed non-ruptured EC who underwent US including SE. The US analyses included size, shape, ratio of depth to length (DLR), involvement of more than half the dermis, “submarine sign,” and SE characters of each lesion. SE findings were assigned into four grades based on elasticity.
Results
The submarine sign was more significantly observed in ECs located in the trunk versus extremities (P value = 0.004 and 0.035, respectively). Truncal lesions were significantly more likely to possess an ovoid shape (P < 0.05) and exhibited higher DLR (P < 0.05). There were more cases with low elasticity according to SE (grade 3 or 4) compared to high elasticity (grade 1 or 2). However, we did not observe significant differences between the two locations (P > 0.05). More-than-half signs also did not exhibit a significant difference (P > 0.05).
Conclusion
The submarine sign, ovoid shape, and tall lesions (higher DLR) are common in the trunk. However, the degree of elasticity and number of more-than-half signs did not differ between the two groups.
Introduction
Epidermal cysts are common superficial epithelial lesions lined with simple squamous epithelium (1–4). These lesions usually arise in hair-bearing regions of the body such as the scalp, face, neck, trunk, and back. Formation of epidermal cysts occurs when hair follicles are obstructed (3,5–7). These cysts rarely arise in the extremities, palms, and soles, which are non-follicular areas of the body; however. they can occur in these areas due to traumatic implantation of the epidermis into the dermis or subcutaneous layer (3,4,8). Ultrasonography (US) has been clinically used as the first modality for superficial lesions. This technique is widely available, cost-effective, and provides real-time dynamic examinations. Despite its feasibility, differentiation of epidermal cysts from other superficial lesions remains challenging. To address this difficulty, Lee et al. reported that a “submarine sign” can be applied for the diagnosis of epidermal cyst (1). Additionally, strain elastography (SE) is a non-invasive method for evaluating tissue elasticity and can be helpful for accurate diagnoses. Tissue elasticity is typically expressed as tissue strain, where the harder the lesion, the more resistant the tissue to extrinsic compression, with softer lesions exhibiting larger strain (1,4,9). There have been several studies on accurate diagnosis of superficial lesions using SE (4,9–11). Most of them focused on differentiation between malignant and benign lesions. However, most superficial lesions are benign (2). Since the imaging characteristics of epidermal cysts differ according to organs such as breast, testis, and superficial soft tissue, the imaging characteristics of the trunk and extremities may also differ (12,13). We hypothesized difference in ultrasound findings between epidermal cysts of the trunk and those of extremities. In addition, to accurately diagnose superficial soft tissue epidermal cyst, it is important to understand the specific findings in the trunk or extremities. Since few studies have been performed on the differences of US findings between epidermal cysts located in the trunk and those in the extremities, we divided and assessed epidermal cysts based on location. We then attempted to use SE to acquire additional information about the epidermal cysts including size, depth-to-length ratio (DLR), and morphology, such as the “submarine sign.” The aim of the present study was to compare the sonographic findings of epidermal cysts according to location in the body and evaluated the feasibility of SE.
Material and Methods
Case selection
We selected patients who underwent surgical excision for confirmed non-ruptured epidermal cyst in the electronic medical records (EMR). The selected patients exhibited superficial soft tissue masses with palpability and underwent sonographic examination with SE before excision between January 2019 and January 2020 at our hospital (Kangbuk Samsung Hospital). A total of 76 cases in 76 patients was included (44 male patients and 32 female patients), with a mean age of 41.3 years (age range = 5–78 years). No cases were excluded because we initially targeted patients with confirmed non-ruptured epidermal cyst. The institutional review board of our center approved this study. Due to the retrospective nature of the study, the requirement for informed consent was waived.
Gray-scale and SE examinations
A radiologist experienced in musculoskeletal aspects for 20 years performed US examinations with SE using a LOGIQ E9 (GE Medical System, Milwaukee, WI, USA) imaging device equipped with linear 6–15 MHz probes. Gray-scale imaging and SE were performed simultaneously. The gray-scale images were performed in the longitudinal and transverse planes. SE was performed at least twice for each lesion to verify reproducibility. A transducer was placed perpendicular to the lesion to apply repetitive minimal pressure. The force transmitted to the lesion was adjusted according to the pressure graph presented on the monitor, exhibiting optimal strain at the region of interest (ROI) (4). The rectangular ROI in the strain image was enlarged to cover the entire lesion. The SE image was superimposed on the gray-scale image using a color-coded representation of elasticity. The relative stiffness of the mass was represented as color, ranging from blue to red in a continuous spectrum (blue = low elasticity, red = high elasticity).
Image analysis
Two radiologists experienced in musculoskeletal aspects (with 19 and 10 years of experience, respectively) and who were from a single center independently reviewed the gray-scale images and SE. First, they classified the cases according to location of the lesion: extremities vs. trunk, including the head and neck. We then compared the characteristics of the US images according to location of the lesion. The US imaging characteristics were size, shape, DLR, involvement of more than half of the dermis, “submarine sign,” and SE characteristics of each lesion. The maximal size of the lesions was measured in length and depth, and the DLR was calculated. In addition, we evaluated the depth of the lesions and determined whether they involved more than half of the depth of the dermis (more-than-half sign). The shape of the lesions was classified into ovoid, round, and irregular shapes. The presence of a “submarine sign” indicated that the lesion has a focal projection of a hypoechoic portion from the hypodermis to the dermis (1). The SE scores were reviewed, and SE characteristics were classified into four grades in a continuous color spectrum (Figs. 1–3): score 1 (very soft, high elasticity), predominantly green to red (>70% of the ROI); score 2 (moderately high elasticity), more green than blue (50%–70% of the ROI); score 3 (moderately low elasticity), more blue than green of the ROI; and score 4 (low elasticity), predominantly blue with a few small areas of green in the ROI (4).
More-than-half sign. An epidermal cyst located on the back of a 43-year-old woman. Gray-scale ultrasound showed a 13-mm, ovoid-shaped hypoechoic mass. The depth-to-length ratio was 0.7, with involvement of more than half of the depth of the dermis (more-than-half sign). Strain elastography showed predominantly blue colors in the mass. The grade was 4 (very hard, low elasticity).
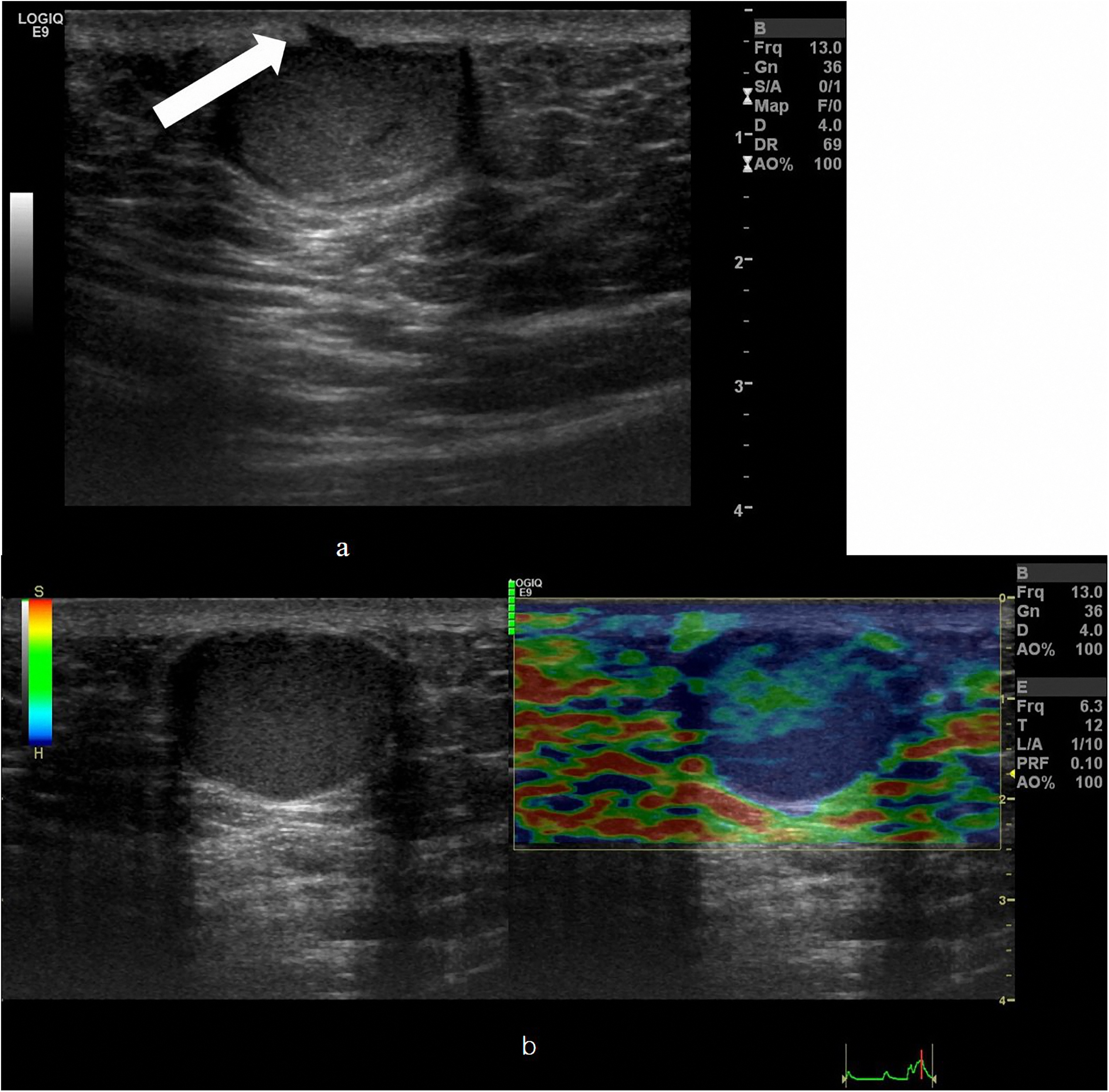
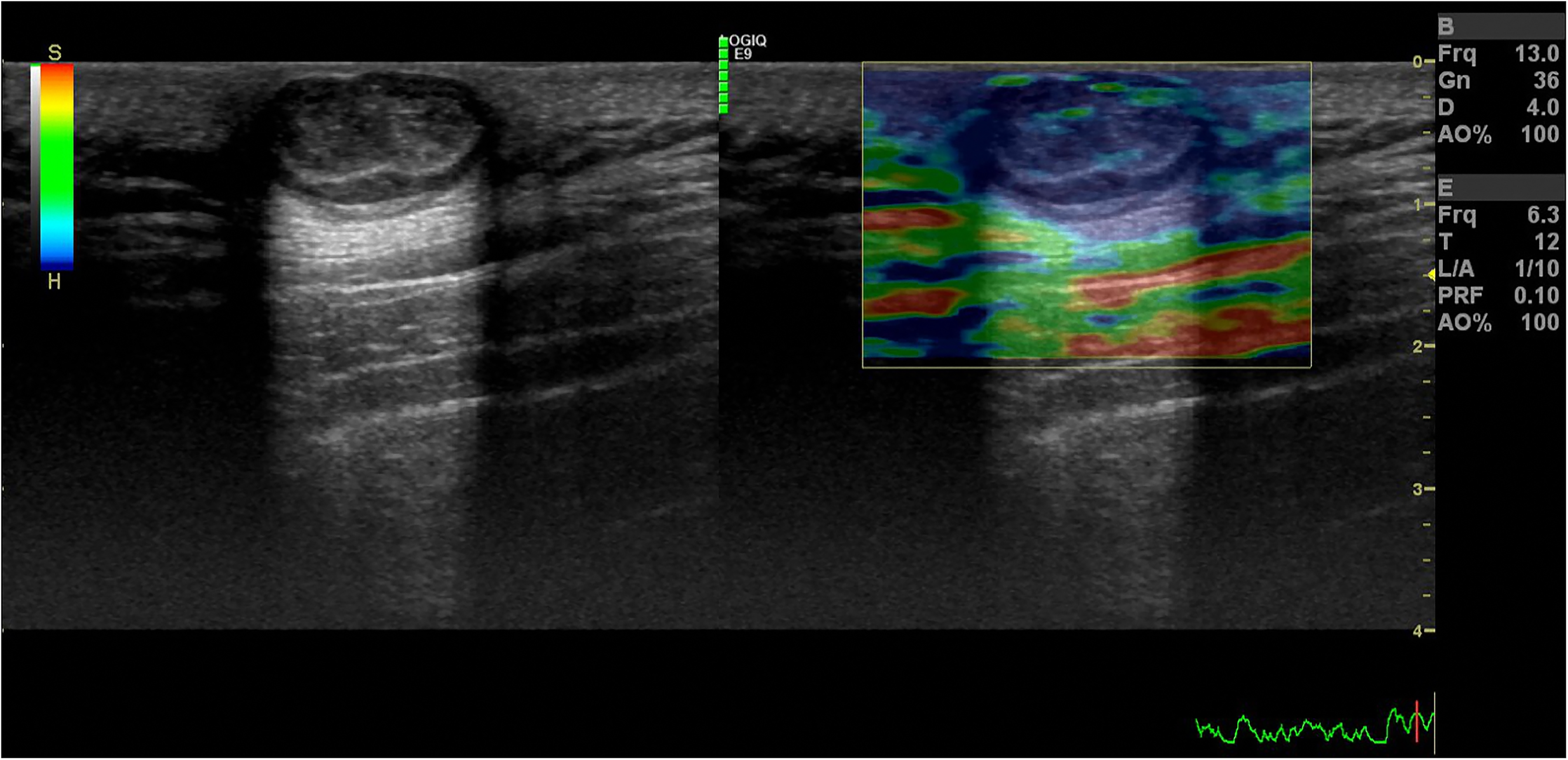
Submarine sign. An epidermal cyst located on the buttock of a 48-year-old woman. (a) Gray-scale ultrasound showed a 42-mm, ovoid-shaped hypoechoic mass. The lesion exhibited a focal projection of the hypoechoic portion from the mass to the epidermis (submarine sign, arrow). (b) Simultaneous strain elastography showed predominantly blue colors in the mass. The grade was 4 (low elasticity).
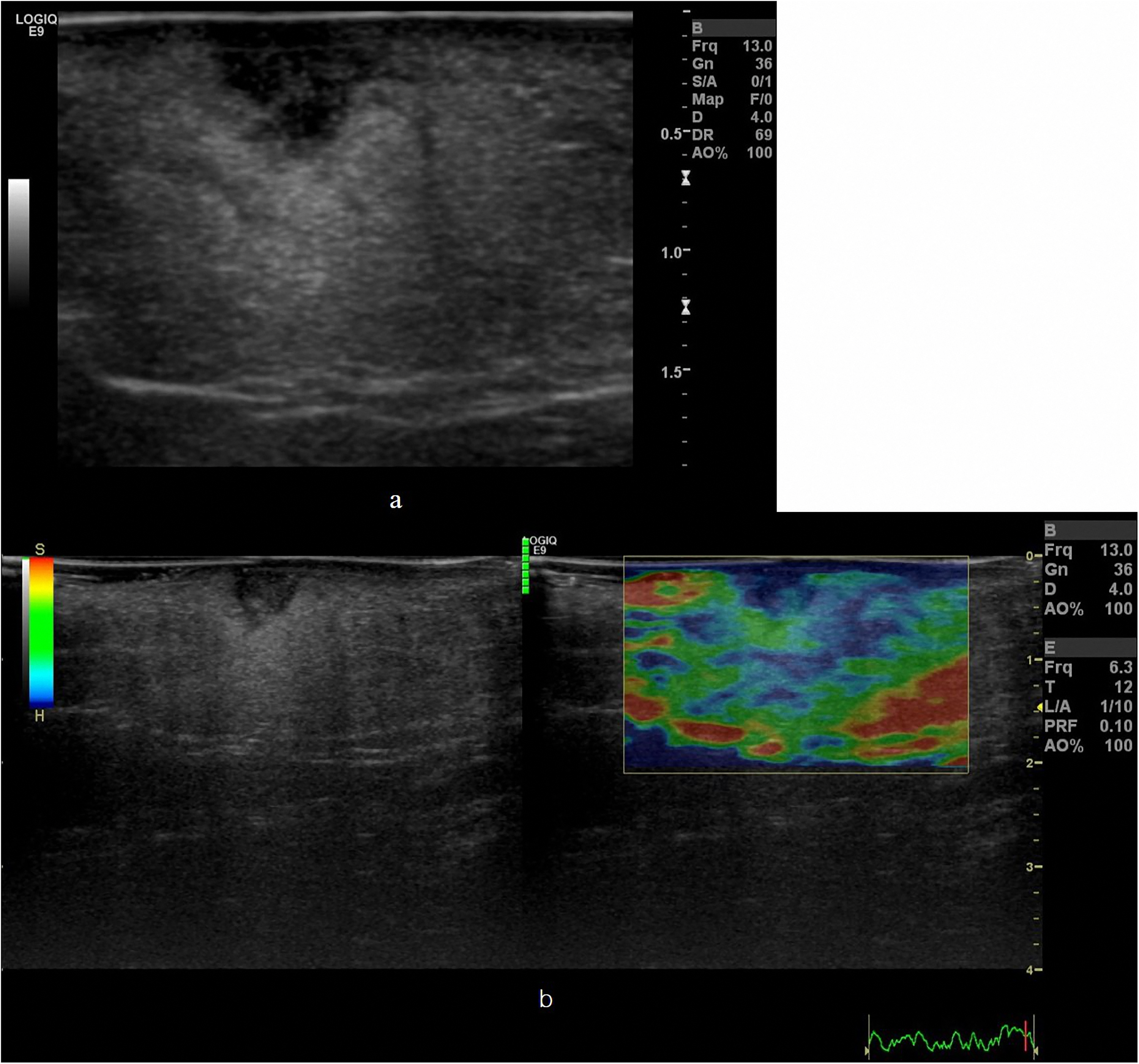
Irregularly shaped mass. An epidermal cyst located on the leg of a 78-year-old woman. (a) Gray-scale ultrasound showed an 8-mm, irregular shaped hypoechoic mass. The depth-to-length ratio was 0.61, and the more-than half sign was positive. Note the increased echoes around the lesion. (b) Simultaneous strain elastography showed predominantly blue colors in the mass. The grade was 4 (low elasticity).
Statistical analysis
Inter-observer agreement of each US imaging characteristic was analyzed using kappa statistics. Cohen's weighted kappa value was used to determine the agreement between the two readers since the elasticity grade indicated by the SE was classified into four grades. The kappa (κ) value was interpreted as follows: 0 = no agreement; 0.01–0.2 = slight agreement; 0.21–0.4 = fair agreement; 0.41–0.6 = moderate agreement; 0.61–0.8 = substantial agreement; and 0.81–1 = almost perfect agreement (14). The DLR was analyzed using an intraclass correlation coefficient (ICC) with a 95% confidence interval (CI).
The interpretation of ICC was as follows: <0.5 = poor; 0.50–0.75 = fair; 0.75–0.90 = good; and >0.90 = excellent (15).
A chi-square test and Fisher’s exact test were used to compare the differences according to the location of the epidermal cyst. The DLR was analyzed using Student's t-test. A P value <0.05 was considered statistically significant. All statistical analyses were conducted using SPSS version 24.0 (IBM Corp., Armonk, NY, USA) and Medcalc version 17.2 (Medcalc Software, Ostend, Belgium).
Results
In total, 76 cases were evaluated: 28 cases were located in the extremities, while 48 cases were located in the trunk. Of the 28 cases located in the extremities, 20 were located on the lower limb and eight were located on the upper limb (Table 1). There was no relationship between the demographic data and the size or hardness of the lesion. The inter-reader agreement of each sonographic finding is presented in Table 2. Almost perfect agreement was observed for DLR, shape of the epidermal cysts located in the extremities, and submarine signs of epidermal cysts located in the trunk, while substantial agreement was noted for the other cysts. Table 3 describes the differences in findings according to location of the lesion. Submarine signs were observed more significantly in epidermal cysts located in the trunk versus extremities (P = 0.004, 0.035, respectively). Only 1 (3.6%) case of an extremity lesion reviewed by reader 1 and 2 (7.1%) cases reviewed by reader 2 exhibited a submarine sign. Although the extremity lesions exhibited a similar incidence of irregular and ovoid shapes, truncal lesions exhibited a greater number of ovoid shapes (P < 0.05). The depth of truncal lesions was larger compared to extremity lesions (P = 0.007, 0.024, respectively), whereas the length did not significantly differ (P > 0.05). The DLR was significantly different between the two locations, with more frequent truncal lesions (P = 0.001, 0.018, respectively). Based on SE, there were more cases with low elasticity (grades 3 or 4) than with high elasticity (grades 1 or 2). However, there was no significant difference between the two locations (P > 0.05). A more-than-half sign did not exhibit a significant difference between locations (P > 0.05).
Demographic data.
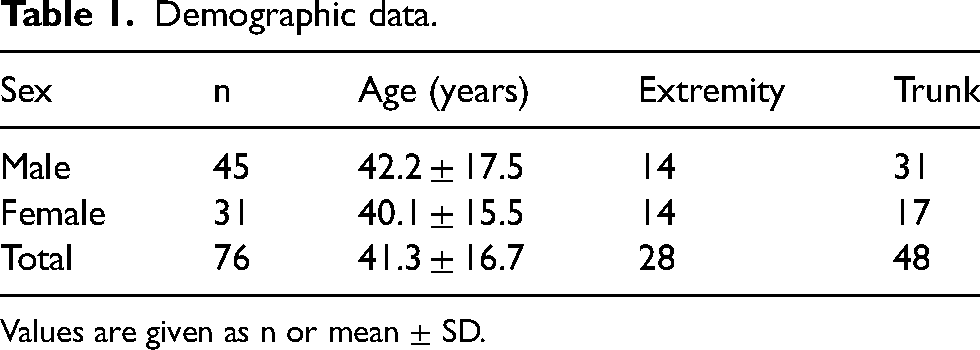
Values are given as n or mean ± SD.
Inter-reader agreement of the sonographic findings.
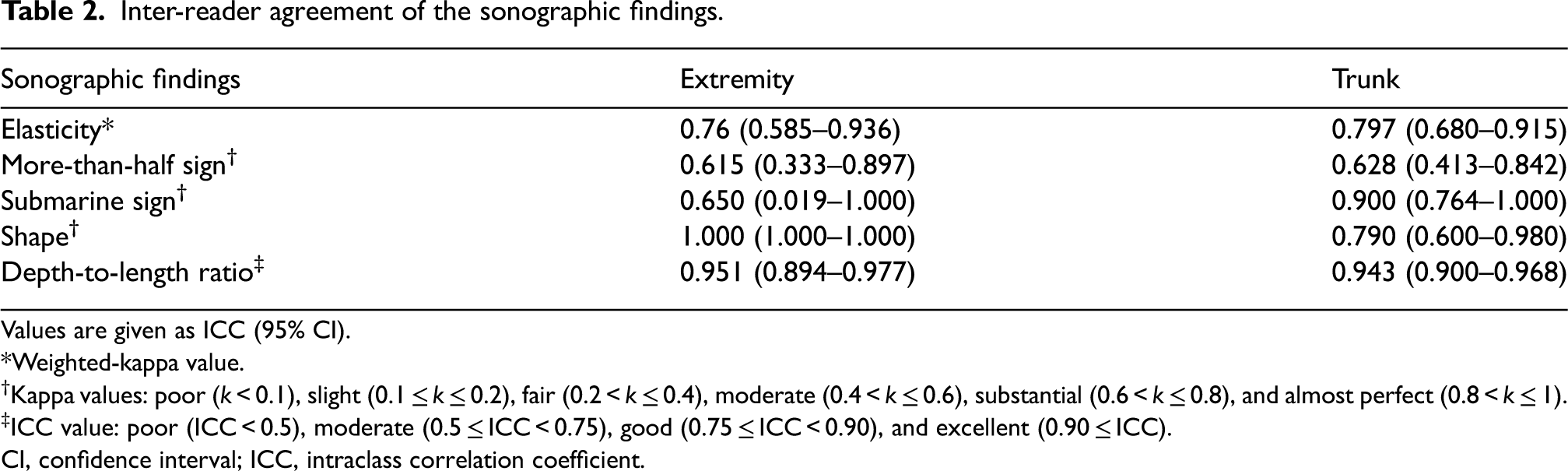
Values are given as ICC (95% CI).
*Weighted-kappa value.
Kappa values: poor (k < 0.1), slight (0.1 ≤ k ≤ 0.2), fair (0.2 < k ≤ 0.4), moderate (0.4 < k ≤ 0.6), substantial (0.6 < k ≤ 0.8), and almost perfect (0.8 < k ≤ 1).
ICC value: poor (ICC < 0.5), moderate (0.5 ≤ ICC < 0.75), good (0.75 ≤ ICC < 0.90), and excellent (0.90 ≤ ICC).
CI, confidence interval; ICC, intraclass correlation coefficient.
Chi-square test or Fisher's exact test for sonographic findings according to location of the epidermal cyst.
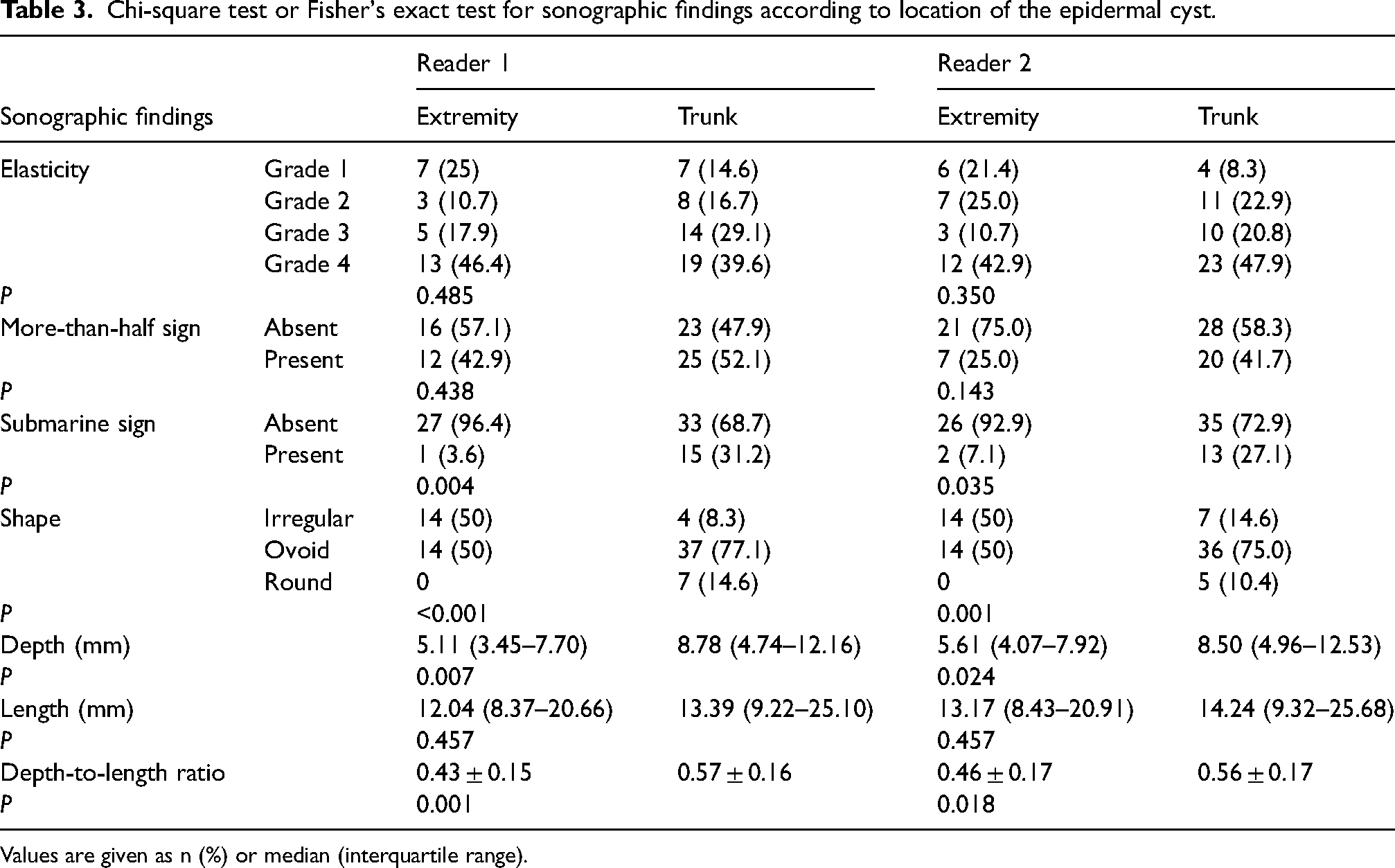
Values are given as n (%) or median (interquartile range).
Discussion
The present study analyzed the difference of sonographic findings of non-ruptured epidermal cysts based on their location on the body. For both readers, there were significant differences of submarine signs, lesion shape, and DLR according to location.
Submarine signs were more prevalent in the trunk. Epidermal cysts typically occur spontaneously. However, misplacement of remnant epithelial tissue during embryogenesis, occlusion of the follicle, traumatic or surgical implantation of epithelium, and presence of HPV infection are etiologic factors (7,16). Among these factors, the submarine sign is thought to be related to the punctum connecting the lesions to the skin surface, and the punctum becomes more prominent when the follicular orifice is obstructed (1,16).
In this study, epidermal cysts located in the extremities including the palmoplantar areas without hair are expected to have a higher probability of trauma or HPV infection compared to those resulting from follicle obstruction, which is a more common pathophysiology of epidermal cysts located in the trunk (16,17). In fact, the submarine sign was less frequently observed in the extremities.
An irregular shape was observed more often in the extremities, while a round shape was observed only in the trunk (Table 3). The ovoid shape was also observed more in the trunk. Epidermal cysts located in the trunk exhibited higher DLR (tall lesions). There are several possible reasons for these results. Since the hypodermal fat of the trunk is relatively thicker compared to the extremities, there is more space for lesion growth. This can explain the higher DLRs and dominant round and ovoid shapes in the trunk. Irregular shapes of epidermal cysts located in the extremities are thought to be more common because of the relatively narrow potential spaces and indentations due to adjacent structures such as bones or ligaments. A previous study reported that epidermal cysts located near a small joint exhibited lobulated margins because of indentations of the lesions by a joint (7). Epidermal cysts near the metatarsophalangeal joint exhibited lobulated margins due to high pressure in an erect position and adjacent hard structures (17,18).
In terms of elasticity of the lesion, we did not observe a significant difference of elasticity based on the location of the lesion. Although hard lesions (grades 3 and 4, 64% vs. 69% for reader 1 and 53% vs. 68% for reader 2, respectively) were slightly greater in number than soft lesions (grades 1 and 2, 36% vs. 31% for reader 1 and 47% vs. 32% for reader 2, respectively), there were no significant differences between the SE of the extremity and trunk. The elasticity of a soft tissue lesion depends on its histology and pathologic changes, which can modify the mechanical properties of the tissue structure (9). Since epidermal cysts in this study were targeted to non-ruptured epidermal cysts with the same histopathology, it is reasonable to believe that there is no difference in elasticity based on location. In addition, the result of elasticity in this study is concordant with the results from other previous studies that reported no characteristic elasticity among benign soft tissue lesions (4,9,10).
Tissue elasticity imaging techniques include SE and shear wave elastography (SWE). The SE is operator-dependent because it uses low frequency compression of the tissue by applying manual compression and release forces. To overcome this problem, SE may use the relative strain ratio of the lesion and reference tissues (19–22). In SWE, the US probe generates a push pulse that travels through the tissue and the shear wave propagates perpendicular to the axial displacement (19). This technique provides both qualitative color-coded maps and quantitative maps either of shear wave velocity (cm/s) or elasticity (kPa) (19–25). In the present study, we used the SE technique only.
The present study has some limitations. First, it is a retrospective study, which has selection bias. Second, several inter-reader agreements of sonographic features were low, possibly due to the inherent limitations of sonographic assessments such as subjectivity and operator dependency. In addition, the confidence interval for the submarine sign in the extremities was very wide. This may be due to the asymmetric dataset of the distribution of the submarine sign, a limitation of Cohen’s kappa analysis.
In conclusion, there were significant differences in the US findings between epidermal cysts in the truck and those in the extremities. The submarine sign, ovoid shape, and tall lesion (higher DLR) are common in the trunk. However, the characteristics of elasticity and the more-than-half sign did not differ between the two groups.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article