
Abstract
Background
There are many ways to treat prostatic hyperplasia; these are currently more inclined to minimally invasive treatment. We mainly compared the differences between two treatment methods, ultrasound-guided transperineal laser ablation (US-TPLA) and prostatic artery embolization (PAE).
Purpose
To evaluate the efficacy and safety of US-TPLA and PAE in the treatment of benign prostatic hyperplasia (BPH).
Material and Methods
The clinical information for 40 patients with BPH admitted to our hospital between June 2018 and January 2021 were retrospectively analyzed. The changes in International Prostate Symptom Score (IPSS), quality of life (QoL), maximum urinary flow rate (Qmax), postvoid residual (PVR), prostate volume (PV), and the incidence of complications were compared between groups.
Results
The IPSS (P < 0.001; P < 0.001), QoL (P < 0.001; P < 0.001), Qmax (P < 0.001; P < 0.001), PVR (P < 0.001; P < 0.001), and PV (P < 0.001; P < 0.001) at three and six months after US-TPLA and PAE improved with respect to those before surgery. There was no significant difference in IPSS (P = 0.235; P = 0.151), QoL (P = 0.527; P = 0.294), Qmax (P = 0.776; P = 0.420), PVR (P = 0.745; P = 0.607), and PV (P = 0.527; P = 0.573) between the groups at three and six months after surgery. No serious complications occurred in either group.
Conclusion
US-TPLA and PAE seem to have a similar short-term efficacy. The efficacy of the two procedures is comparable, and neither is associated with serious complications. US-TPLA and PAE are both effective complementary measures for the treatment of BPH.
Introduction
Benign prostatic hyperplasia (BPH) occurs mainly in older men. The incidence at the age of 60–69 years is 70%, and the incidence at the age >80 years is as high as 80% (1). With age, lower urinary tract symptoms (LUTS) become increasingly serious, and the patient’s quality of life (QoL) significantly decreases. α-blockers (e.g. benzylamine and tetrazolium) and 5-reductase inhibitors are the first-choice treatments for BPH (2). However, these treatments often fail to achieve the desired results, and some patients require further surgery. Transurethral resection of the prostate (TURP) is currently considered the gold standard treatment for BPH (3), but nonetheless is associated with potential complications, such as intraoperative bleeding, infection, retrograde ejaculation, and other prostate resection syndromes. However, the advent of laser technology suggests an effective alternative to TURP. The risk of complications is low and similar efficacy can be achieved, compared with TURP. It is more of a low-cost treatment compared to TURP. Most conveniently, it can be performed in the outpatient operating room (4–6). Ultrasound-guided transperineal laser ablation (US-TPLA) and prostatic artery embolization (PAE) are new minimally invasive interventional techniques developed in recent years, both of which are suitable for BPH in older people (7,8). We confirmed the safety and efficacy of US-TPLA in a retrospective study of 20 patients (9). Although both techniques have been reported separately, comparisons between the two have not been performed currently. The aim of the present study was to analyze the efficacy and safety between both technologies.
Material and Methods
Patients
Drug treatment was ineffective in all patients between June 2018 and January 2021, and the patients were unwilling to receive surgery. They voluntarily chose either US-TPLA or PAE. The inclusion criteria were as follows: (i) men aged >50 years diagnosed with BPH with LUTS, with no fertility requirements; (ii) International Prostate Symptom Score (IPSS) ≥13; (iii) prostate volume (PV) ≥30 mL; (iv) maximum urinary flow rate (Qmax) ≤15 mL/s; and (v) postvoid residual (PVR) ≤400 mL. The exclusion criteria were as follows: (i) severe urethral stricture; (ii) history of prostate, bladder neck, or urethra surgery; (iii) severe coagulation disorder or urinary infection; (iv) known nervous system diseases (such as multiple sclerosis, Parkinson's disease, or history of spinal cord injury); (v) bladder-derived LUTS; and (vi) prostate-specific antigen (PSA) > 10μg/L, or imaging examination of suspected prostate cancer. According to the American Society of Anesthesiologists (ASA) scoring system, 16 cases were ASA score 2 and four cases were ASA score 3 in US-TPLA; 15 cases were ASA score 2 and five cases were ASA score 3 in PAE. All patients provided signed informed consent before operation and the study was approved by the institutional review board. The need for approval was waived by the local ethical committees as data were collected retrospectively and reported anonymously.
Instruments and Methods
In the US-TPLA group, an Italian Esaote MyLabClass-C color Doppler ultrasound instrument equipped with a TRT33 biplanar linear array probe (frequency = 4–13 MHz) and EchoLaser X4 laser ablation system was used for interventional therapy. Under the guidance of a transrectal TRT33 biplanar probe, 2% lidocaine was used for anesthesia from the skin to the left lobe prostate capsule, and the right lobe was anesthetized in the same manner. The needle was inserted into the hyperplastic area surrounding the urethra of one side of the prostate, by ensuring that the distance from tip of the needle to the bladder was >15 mm (Fig. 1a) and the distance from the needle to the urethra was 8–10 mm from the side view (Fig. 1b). A second needle was inserted with the first needle used as a reference. After the needle sheath was withdrawn approximately 1 cm, ablation was initiated. The power of the ablation instrument was set to 3 W, and the energy value of the single fiber was set to 1800 J. If necessary, the proximal end of the prostate was ablated with a “pull-back technique” to ensure complete vaporization of the targeted tissue. The contralateral prostate was ablated in the same manner. Finally, the ablation range was confirmed in contrast-enhanced ultrasound (Fig. 1c, d). If the hyperplastic area surrounding the urethra was not completely ablated, the needle could be used again for ablation. Technical success was defined as complete ablation of the hyperplastic area surrounding the urethra (10).
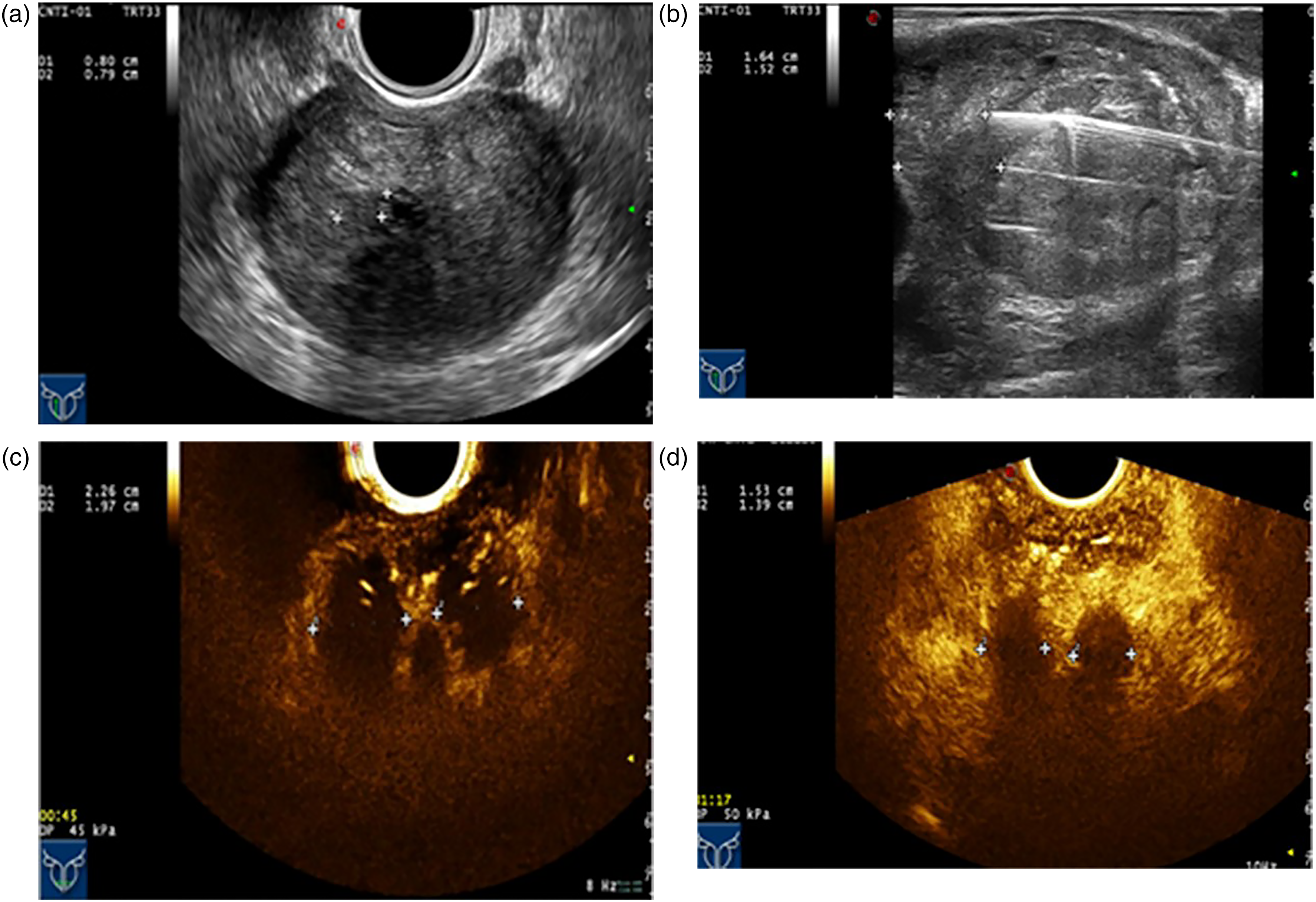
US-TPLA for benign prostatic hyperplasia. (a) The distance between the needle body and the urethra should be controlled to approximately 0.8 cm on the axial image. (b) The distance between the needle tip and the bladder should be controlled to approximately 1.5 cm on the sagittal image. (c) After ablation, contrast-enhanced US revealed no perfusion in the hyperplasia zone of the prostate. (d) Follow-up at 3 months after surgery. The volume of the ablation area was slowly absorbed and decreased. US-TPLA, ultrasound-guided transperineal laser ablation.
In the PAE group, a GE Innova 3131-IQ and GE IGS530 DSA were used to guide the treatment of PAE. After local subcutaneous anesthesia, the right femoral artery was punctured with the Seldinger technique, and a 5-Fr catheter sheath was inserted. Then, the 5-Fr catheter was placed in the bilateral internal iliac arteries. The contrast agent (flow rate = 4 mL/s, total volume = 12 mL, injection pressure = 2000 kPa) was injected at the 37° ipsilateral and 15° cephalic positions. After the position of the prostatic artery opening was confirmed (Fig. 2a, b), a 2.7-Fr microcatheter was hyper-selected and inserted into the prostatic artery for staining under image guidance. Then, 40–120 μm or 100–300 μm of Embosphere was slowly injected for embolization until the blood flow of the main prostatic artery stopped. After complete embolization was confirmed by angiography, the contralateral prostatic artery was embolized in the same manner. Magnetic resonance imaging (MRI) was performed to observe changes in PV (Fig. 2c, d). Technical success was defined as successful embolization of both prostatic arteries (11).
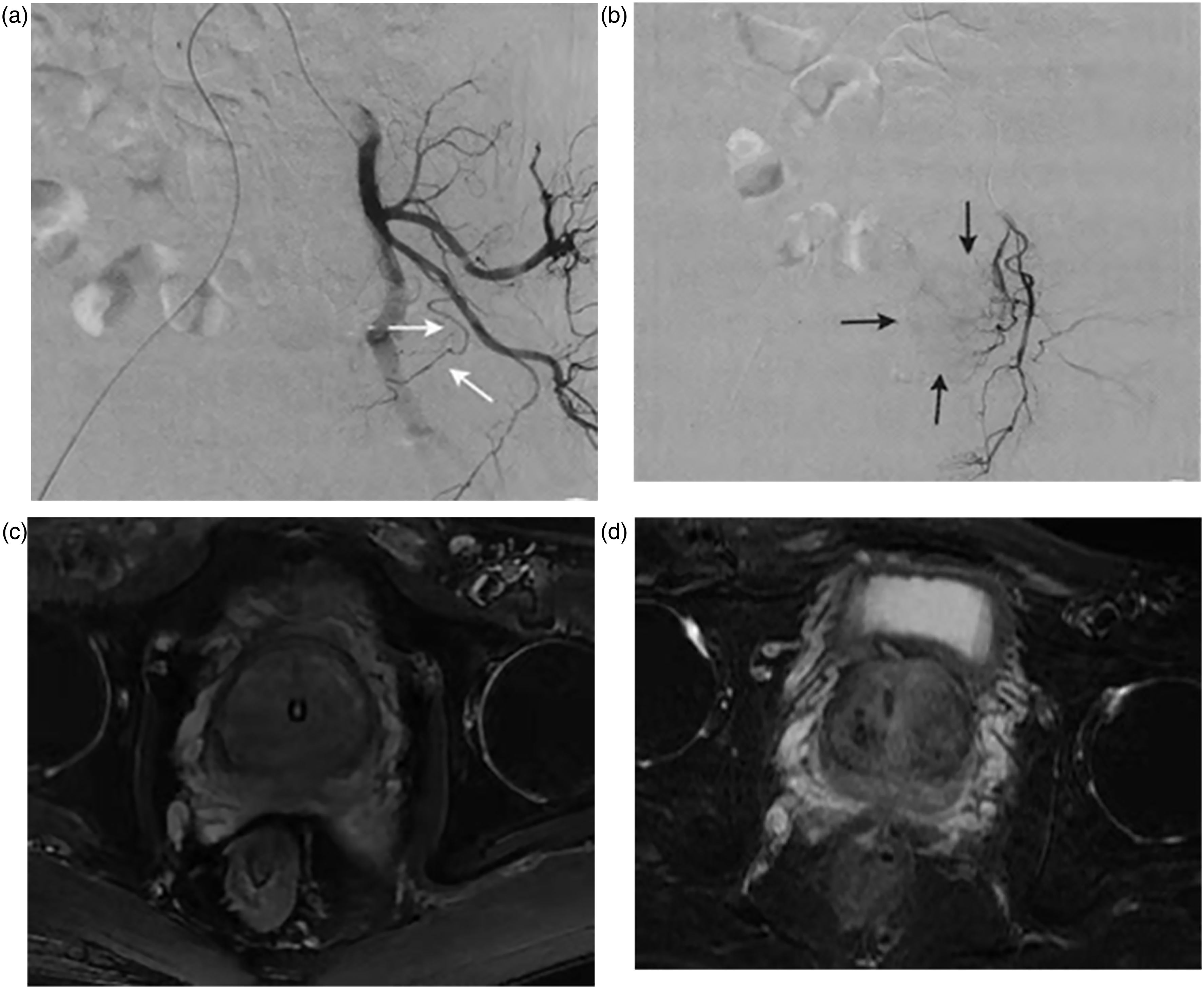
Interventional treatment of PAE. (a) The prostatic artery is seen at 45° lateral to the patient's position (white arrow). (b) The prostatic artery was selected with a microcatheter and injected with contrast agent (black arrow). (c) Preoperative MRI of PV (indwelling catheter). (d) Follow-up at 3 months by postoperative MRI showed that the PV decreased (catheter removed). MRI, magnetic resonance imaging; PAE, prostatic artery embolism; PV, prostate volume.
The changes in IPSS, QoL, Qmax, PVR, and PV were recorded at three and six months after the surgery. A urometer was used to record the urine flow rate per second during urination and construct a curve indicating whether the lower urinary tract was obstructed. The Qmax was calculated from the urine flow rate curve. PVR was measured by ultrasound immediately after urination (PVR = maximum transverse diameter × maximum longitudinal diameter × maximum anteroposterior diameter × 0.52). PV is the prostate volume measured by transrectal ultrasound or MRI (maximum transverse diameter × maximum longitudinal diameter × maximum anteroposterior diameter × 0.52). Complications mainly included fever, pain, hematuria, urethral stricture, bladder injury, and urinary retention. All methods were performed in accordance with the relevant guidelines and regulations.
Statistical analysis
Using SPSS version 24.0 statistical software (IBM Corp., Armonk, NY, USA), the measurement data, including age, IPSS, QoL, Qmax, PVR, and PV, were expressed as X ± S, and the complications were expressed as percentages. Univariate analysis of variance or T-test was used to compare the intra-group and inter-group efficacy of the two treatments. The incidence of complications between groups was expressed with the Fisher exact probability method. Differences were considered statistically significant at P < 0.05.
Results
A total of 40 patients (mean age = 72.3 ± 9.0 years) with BPH in our hospital were enrolled in the study. There were 20 cases of US-TPLA (mean age = 73.9 ± 9.2 years). All 20 patients had repeated use of anti-BPH drugs, but no history of long-term adherence. A total of 16 patients were defined as ASA score 2 due to chronic obstructive pulmonary disease (COPD) complicated with NYHA Classes I, and four patients were defined as ASA score 3 due to COPD complicated with NYHA Classes II. The IPSS was 22.7 ± 5.2 (range = 15–35); the QoL was 5.0 ± 1.7 (range = 2–8); the Qmax was 8.3 ± 3.0 mL/s (range = 4–15 mL/s); the PVR was 82.8 ± 57.4 mL (range = 0–200 mL); and the PV was 70.7 ± 23.8 mL (range = 38–140 mL). The PAE group comprised 20 patients (mean age = 70.6 ± 8.8 years). All 20 patients had repeated use of anti-BPH drugs, but no history of long-term adherence. A total of 15 patients were defined as ASA score 2 due to COPD complicated with NYHA Classes I, and five patients were defined as ASA score 3 due to COPD complicated with NYHA Classes II. The IPSS was 24.4 ± 4.7 (range = 13–34); the QoL was 5.1 ± 1.4 (range = 2–7); the Qmax was 8.2 ± 2.9 mL/s (range = 5–15 ml/s); the PVR was 83.9 ± 56.6 mL (range = 0–235 mL); and the PV was 72.5 ± 28.7 mL (range = 40–160 mL). There was no significant difference in preoperative IPSS (P = 0.276), QoL (P = 0.838), Qmax (P = 0.752), PVR (P = 0.779), and PV (P = 0.835) between groups (P > 0.05). The IPSS (P < 0.001; P < 0.001), QoL (P < 0.001; P < 0.001), Qmax (P < 0.001; P < 0.001), PVR (P < 0.001; P < 0.001), and PV (P < 0.001; P < 0.001) at three and six months after US-TPLA and PAE improved with respect to those before surgery (Table 1). No significant difference was observed in IPSS (P = 0.235; P = 0.151), QoL (P = 0.527; P = 0.294), Qmax (P = 0.776; P = 0.420), PVR (P = 0.745; P = 0.607) and PV (P = 0.527; P = 0.573) between the groups at three and six months after surgery (Table 2). The patients who developed complications in this study have been classified as Clavien–Dindo. There were three patients in the US-TPLA group with Grade I complications, among which two patients showed postoperative hematuria and all returned to normal after staying in bed; one patient experienced urethral burns. The incidence of complications in the US-TPLA group was 3/20. There were two patients in the PAE group with Grade I complications, which mainly manifested as unbearable pelvic pain, with an incidence of approximately 2/20. Both patients were improved after analgesic drugs. There was no significant difference in complications between the groups.
Efficacy of US-TPLA and PAE at three and six months after surgery.
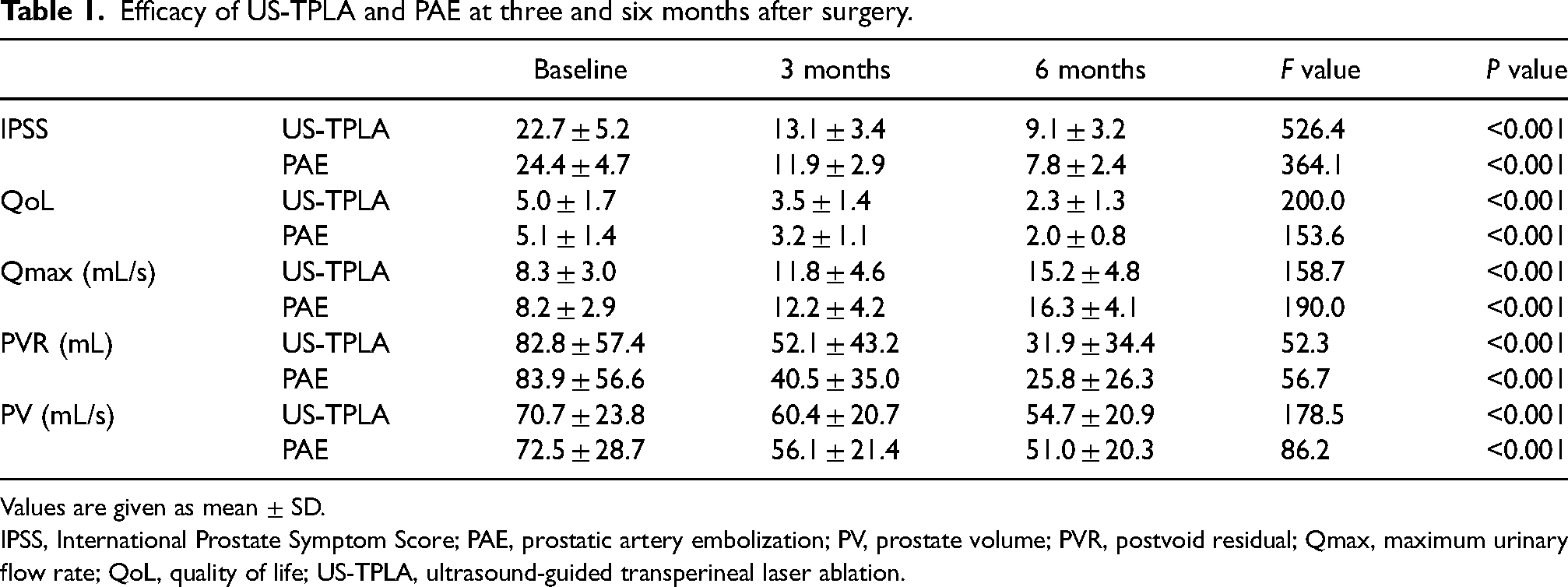
Values are given as mean ± SD.
IPSS, International Prostate Symptom Score; PAE, prostatic artery embolization; PV, prostate volume; PVR, postvoid residual; Qmax, maximum urinary flow rate; QoL, quality of life; US-TPLA, ultrasound-guided transperineal laser ablation.
Comparison of US-TPLA and PAE at three and six months after surgery.
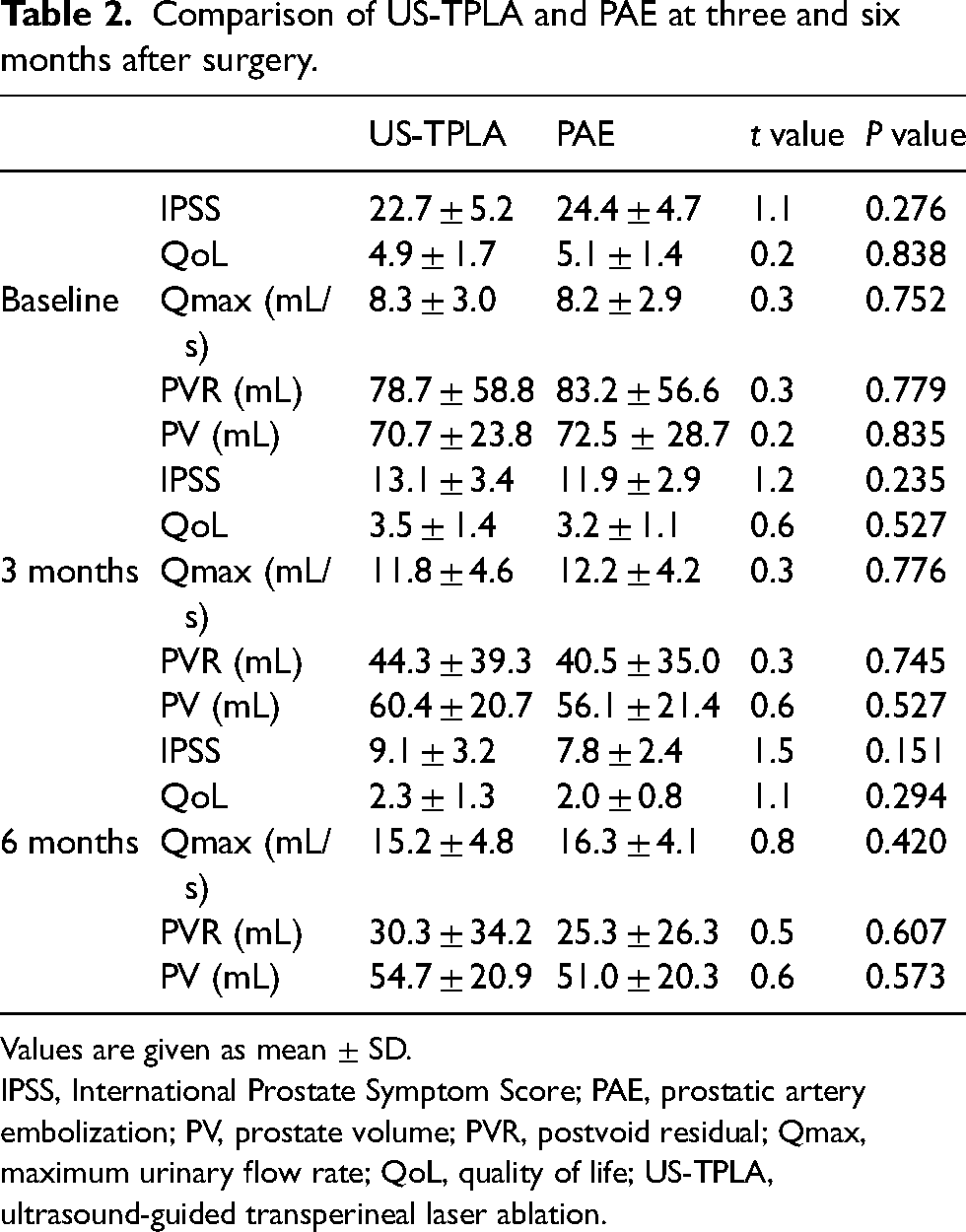
Values are given as mean ± SD.
IPSS, International Prostate Symptom Score; PAE, prostatic artery embolization; PV, prostate volume; PVR, postvoid residual; Qmax, maximum urinary flow rate; QoL, quality of life; US-TPLA, ultrasound-guided transperineal laser ablation.
Discussion
In recent years, with the introduction of laser technology, holmium laser enucleation of the coagulation (HoLEP) has become the main minimally invasive treatment for BPH. Much literature has also shown that HoLEP can not only solve lower urinary tract obstruction, but also reduce the incidence of intraoperative bleeding and other complications (12). However, many patients with BPH are accompanied by diabetes, coronary heart disease, and other underlying diseases. Therefore, the risk of general or epidural anesthesia is correspondingly increased. In addition, transurethral removal of hyperplastic prostate tissue will also have retrograde ejaculation in nearly 75% of patients (13). Therefore, in recent years, scholars have also been studying the perineal pathway or the prostatic artery pathway to treat prostate hyperplasia.
In 1988, Littrup et al. (14) first proposed ablative treatment for the prostate by injection of anhydrous ethanol. The treatment is effective, but the anhydrous ethanol flows back up the needle path. With continual improvements in instruments and equipment, solid ablative therapy of anhydrous ethanol was gradually replaced by radio frequency, microwave, and laser methods. In 2017, Patelli et al. (10) first proposed US-TPLA for BPH in a prospective study. After three months of follow-up, the IPSS, QoL, PVR, Qmax, and PV all improved in 18 enrolled patients. To further confirm the feasibility of this technology, Pacell et al. (15) included 160 patients in a subsequent multicenter study. After a one-year follow-up, the mean IPSS improved from 22.2 ± 4.5 to 7.0 ± 2.9; the QoL improved from 4.2 ± 0.6 to 1.6 ± 0.9; the Qmax improved from 8.6 ± 5.2 mL/s to 15.0 ± 4.0 mL/s; the PVR improved from 71.7 ± 93.9 mL to 17.8 ± 51.0 mL; and the mean PV improved from 87.9 ± 31.6 mL to 58.5 ± 22.9 mL. Of the patients, 3.7% had transient dysuria, 1.2% lost ejaculation function, and only one patient had a prostate abscess. PAE is also an emerging minimally invasive interventional technique, particularly for patients at high risk under general anesthesia; it has been found to be an effective complementary method (16–18). Leng et al. (19) have shown that PAE can effectively decrease the volume of the prostate, thus diminishing the symptoms of prostate obstruction. After the PAE treatment, 90.3% of patients no longer need a catheter to resolve LUTS. Through a prospective randomized controlled study, Ray et al. found that PAE and TURP have a similar efficacy at 12 weeks after surgery, but the complications of PAE are far fewer than those of TURP. Ectopic embolism is a rare and serious complication, but the risk of untargeted embolism can be decreased by cone-beam computed tomography (20,21). The difference between US-TPLA and PAE has not been reported to date. The results of this study showed no statistically significant difference in preoperative indexes between groups, and the mean IPSS, QoL, Qmax, PVR, and PV at three and six months after surgery improved with respect to the preoperative indexes. These findings suggest the efficacy of US-TPLA and PAE in the treatment of BPH. However, at both three months and six months after surgery, the IPSS, QoL, Qmax, PVR, and PV between the groups showed no statistically significant difference, because the techniques both work by blocking blood vessels and decreasing PV to relieve symptoms. US-TPLA is used to cauterize the internal glandular region by emitting laser energy to block the internal glandular blood flow. When the androgen supply is insufficient, the vicious cycle of neuro-humoral regulation is interrupted, thus decreasing smooth muscle tone and absorption of burned necrotic areas. Therefore, the gradual reduction of PV alleviates LUTS. PAE achieves this goal through embolization of the main prostatic artery (22). However, HoLEP surgery is performed on prostate tissue with enucleation hyperplasia through direct urethral laser, with better and more accurate effect. A review of the previous literature and follow-up of three months after surgery showed that IPSS, QoL, and Qmax improved significantly, but HoLEP also had risks of urethral stricture and venous air embolism (23,24). Although the improvement effect of IPSS, QoL, and Qmax indexes of US-TPLA and PAE is not particularly prominent three months after surgery, IPSS, QoL, and Qmax will be further improved with the reduction of prostate volume, and its long-term effect is worthy of expectation. This study included two patients with prostatic arterial stenosis accompanied by arteriosclerosis, in whom US-TPLA was performed instead of PAE. One patient needed three needles to achieve the desired result in US-TPLA, because the PV was approximately 160 mL. Because of cost, PAE was the last choice. At six months after surgery, the LUTS was significantly relieved, and the PV was reduced to 115 mL. There were no serious complications in either group. Complications occurred in three patients in the US-TPLA group. Two patients developed hematuria after surgery, and all recovered to normal after symptomatic treatment. One patient experienced urethral burn, and no clear urethral stricture or LUTS was found after the catheter indwelling time was extended to 15 days. PAE resulted in unbearable pelvic pain in two patients, both of whom improved after drug treatment. This symptom may be due to cytotoxic edema after embolization and ischemic prostatitis (25–27).
The benefits of TURP are clear. However, US-TPLA and PAE are effective complementary treatments for LUTS in patients with underlying cardiopulmonary disease who are not candidates for general anesthesia. Rare complications did not affect subsequent QoL. US-TPLA does not require an X-ray for the operation, and it can accurately display the position of the needle tip, then accurately ablate the target area and achieve the desired range through “pull-back” ablation. However, for large prostates, US-TPLA may need to be further validated because laser ablation is limited in scope. In contrast, PAE is not easily limited by the volume of the prostate. In general, as long as the prostate arteries on both sides can be successfully identified and embolized, efficacy can be achieved. However, the presence of prostate arterial variation or arteriosclerosis in patients also poses challenges for operators (28). Notably, although the PV of one patient in the PAE group decreased, the LUTS remission was unclear. The reason for this finding might have been that the bladder detrusor muscle was damaged at an early stage (29). Therefore, intervention before irreversible damage of bladder function is an important condition to improve efficacy. Some researchers have even found that timely intervention with US-TPLA improves sexual function in patients (30).
Both US-TPLA and PAE are effective complementary treatments for patients. The short-term efficacy of the two techniques is considerable, and both have characteristics of minimal injury, quick recovery, and few complications. For patients with BPH, individualized treatment may provide the most benefit. US-TPLA may be more appropriate for patients with severe systemic arteriosclerosis or prostate arterial variation. However, patients with a large PV may be better candidates for PAE because of the limited laser ablation range of US-TPLA.
The present study has some limitations. Because the sample size of this study was small, calculation of the difference in efficacy of the two technologies was not possible. The IPSS and QoL results are highly subjective. Finally, a long-term follow-up with larger multicenter samples is needed to further verify the efficacy of the two technologies.
In conclusion, US-TPLA and PAE seem to have a similar short-term efficacy, both of which can effectively relieve LUTS, providing a new choice for some special patients with BPH. However, the long-term efficacy needs to be verified by multicenter randomized controlled studies.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.