
Abstract
Background
The radiological and surgical anatomy of the frontal sinus should be well-known in all age groups to successfully manage frontal sinus diseases and reduce the risk of complications in sinus surgery.
Purpose
To define frontal sinus and frontal cells according to the International Frontal Sinus Anatomy Classification (IFAC) criteria in pediatrics and adults.
Material and Methods
A total of 320 frontal recess regions of 160 individuals (80 pediatric, 80 adults) who underwent a computed tomography (CT) scan of the paranasal sinus (PNS) were included in the study. Agger nasi cells, supra agger cells, supra agger frontal cells, suprabullar cells, suprabullar frontal cells, supraorbital ethmoid cells, and frontal septal cells were evaluated in the CT analysis.
Results
The incidence rates of the investigated cells were determined to be 93.1%, 41.9%, 60.0%, 76.3%, 58.5%, 18.8%, and 0% in the pediatric group, respectively, and 86.3%, 35.0%, 44.4%, 54.4%, 46.9%, 19.4%, and 3.4% in the adult group, respectively. Considering the unilateral and bilateral incidence of the cells, agger nasi cells were highly observed bilaterally in both the pediatric group (89.87%) and the adult group (86.48%).
Conclusion
Our study results show that IFAC can be used as a guide to increase the chance of surgical treatment in the pediatric and adult groups and that the prevalence of frontal cells can be determined radiologically and contributes to the generation of estimations of the prevalence of frontal cells.
Keywords
Introduction
Endoscopic evaluation of frontal sinus diseases is complicated due to factors such as the structure of the frontal recess, the formation of frontal, ethmoidal, and agger cells, the presence of concha bullosa, and frontal sinus hypoplasia and hyperplasia (1). Surgeons must have a high-quality computed tomography (CT) study to evaluate the anatomy of the frontal sinus and its drainage pathway before proceeding with surgery. CT scans also show the surgeon the extent of the pathology, the aggressiveness of the disease, and the involvement of adjacent vital structures, reducing the risk of possible complications during surgery (2,3). Therefore, before functional endoscopic sinus surgery (FESS), the surgeon should know the development of the frontal sinus with age, its morphological features and variations, and the anatomy of its neighboring structures within the skull base. In addition, it is important to be able to analyze radiological examinations before the surgical procedure and perform the surgical procedures using this anatomy knowledge as a surgical guide.
The most commonly used classification of frontoethmoidal cells to date has been described by Bent et al. (4). However, the advent of FESS has led to increased interest in the detailed anatomy of the nose and paranasal sinuses (PNS). However, most of the structures of surgical importance were not found in the official Terminologia Anatomica used by basic anatomists, and there was also no common classification among surgeons (5–9). For all these reasons, the International Frontal Sinus Anatomy Classification (IFAC) was developed in 2016 to use a common terminology among surgeons, to increase the success in revealing pathologies related to the frontal sinus, to increase the sensitivity of dissections in surgical planning, and to prevent possible complications at the same time (6). IFAC emphasized the location and number of cells and the effect of cells on the frontal sinus drainage pathway. This system will help surgeons better understand the frontal sinus by giving surgeons an accurate naming of cells based on their location. When any new anatomical classification is proposed, in addition to determining the prevalence of anatomical variants identified by the classification system, the consistency/difference of the proposed classification system across age groups is extremely important. Therefore, the aim of the present study was to define frontal sinus and frontal cells according to the IFAC criteria in pediatrics and adults.
Material and Methods
This retrospective cross-sectional study was conducted after approval was obtained from the non-interventional ethics committee of Ankara Bayındır Hospital (BTEDK-14/22). The research was conducted with images of individuals who underwent CT of the paranasal sinuses between 1 January 2019 and 16 August 2022. Informed consent was obtained from all participants included in the study. All procedures in this study were performed in accordance with the ethical standards of the institutional and/or national research committee, in addition to the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
In order to determine the sample size, a power analysis was performed using the G*Power (version 3.1.9.7) program. The power of the study is expressed as 1-β (β = probability of type II error). In the calculation, the effect size (d) was found to be 0.730 to obtain 90% power at the α = 0.05 level. Accordingly, it was determined that the research should be conducted with at least 80 patients in each group and 160 patients in total. The study examined 320 frontal sinus (right and left) regions of 160 patients. The patients were divided into two groups: 80 adults (48 men, 32 women; mean age = 45.66 ± 13.28 years; age range = 18–54 years) and 80 children (26 boys, 54 girls; mean age = 11.41 ± 3.13 years; age range = 6–17 years).
Inclusion and exclusion criteria
Patients who had a paranasal sinus CT scan performed due to various nasal complaints but did not have any paranasal pathology, including sinusitis, were included in the study. All cases were questioned regarding previous sinonasal surgery, nasal polyposis and maxillofacial trauma, and significant craniofacial or maxillofacial anomalies. Patients with these diagnoses or surgical histories were not included in the study. Previous skull base or paranasal sinus surgery history, congenital facial anomaly, current or previous diseases causing erosion of the ethmoid roof, and presence of chromosomal anomaly were accepted as exclusion criteria.
CT analysis
All patients underwent axial CT study (tube voltage = 120 kV, 200–300 mA, field of view = 25 cm, high resolution = 0.6 mm contiguous axial slice) obtained using a Somatom Definition AS + 128-detector spiral MSCT device (Siemens, Malvern, USA. The evaluation was performed using Advantage Workstation Release 4.3 Software DICOM Viewer 19933–2006 version (General Electric Company, Suite 3700, Boston, USA) on axial, coronal, and sagittal reconstructed images. The bone window was used to interpret the scans. An image-processing software dedicated to digital imaging and communications in medicine (DICOM) images was used to visualize the digital three-dimensional volumetric image on axial, coronal, and sagittal planes.
The study data were collected sequentially. The data were obtained from the medical registry and manually from the CT study registry located in the registry and filing office of the diagnostic imaging department or online from PACS. Two radiologists, with 15 and 18 years of professional experience, evaluated all images separately. The online PACS-IW system was accessed to track the type of CT study each patient had. CT studies of the paranasal sinuses were taken and recorded on a DVD-R. These images were then imported into the OSIRIX 64-bit DICOM Viewer software on a laptop. All the obtained data were entered into the study proforma and then transferred to SPSS version 22.0 software (IBM Corp., Armonk, NY, USA).
Measurements
IFAC divided the frontal recess cells into anterior, posterior, and medial groups. Cells located anterior to the drainage pathway include agger nasi cells, supra anger cells, and supra agger frontal cells; those based posteriorly include suprabullar cells, suprabullar frontal cells, and supraorbital ethmoid cells; those based medially include frontal septal cells (Fig. 1). The presence of these cells was investigated in our study. In addition, frontal sinus asymmetry was noted by detecting frontal sinus hypoplasia, hyperplasia, aplasia, and septal deviation status.
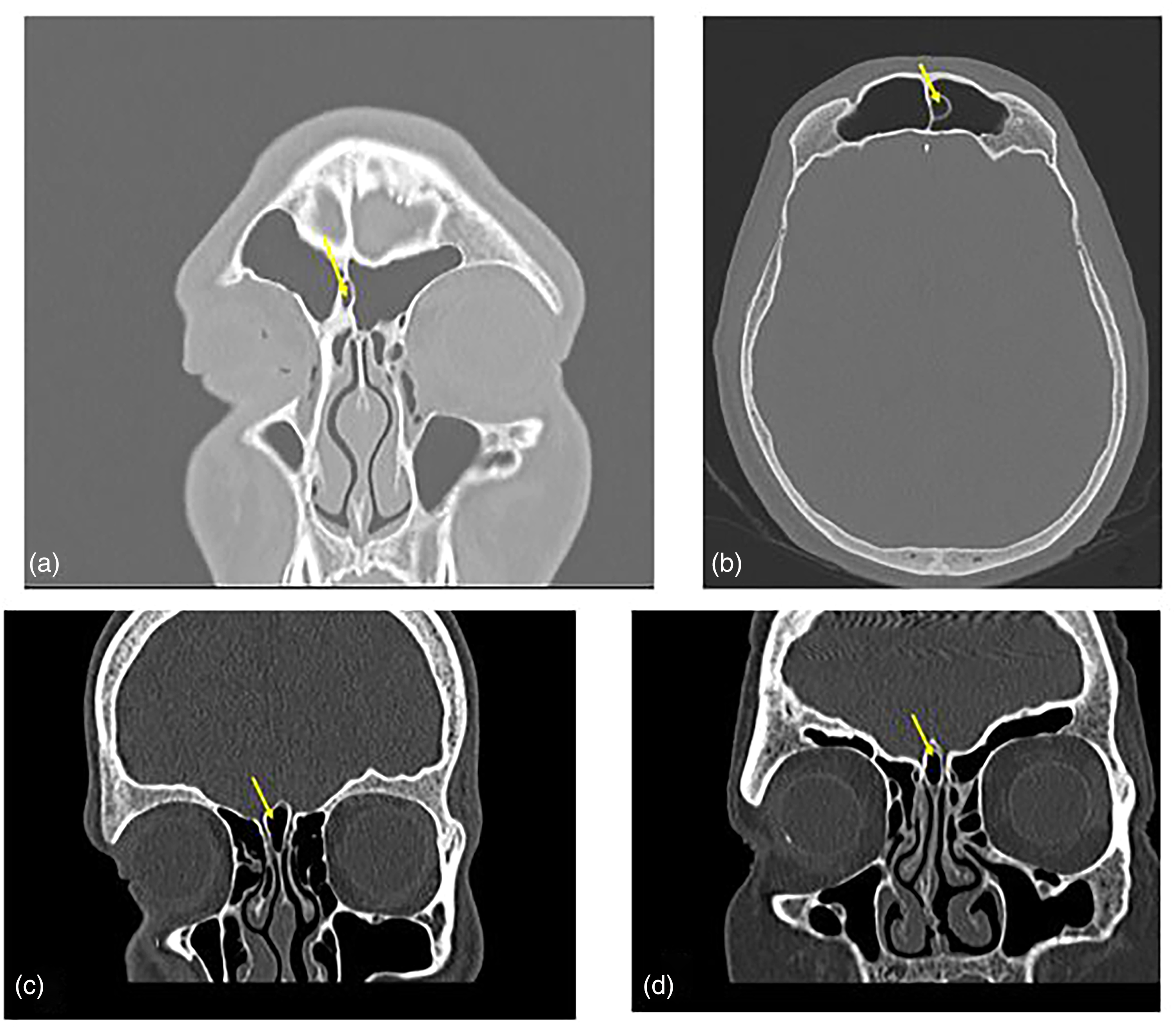
(a) A 15-year-old male patient with a frontal septal cell. (b) A 46-year-old patient with a frontal septal cell. (c) The coronal section of a 15-year-old patient, crista galli pneumatization. (d) The coronal section of a 45-year-old patient, crista galli pneumatization.
Statistical analysis
Analyses were performed using SPSS version 22.0 (IBM Corp., Armonk, NY, USA). The study examined intra- and inter-observer agreement by calculating Cohen's kappa coefficient and intra-class correlation coefficient. Inter-observer agreement was analyzed as 92%. The descriptive data were presented as numbers and percentages for categorical data, and median and range or mean ± standard deviation for continuous data. Categorical data were compared using chi-squared and Fisher’s exact tests, when appropriate. Normally distributed data were compared using the independent t-test. P < 0.05 was considered statistically significant for all analyses (2–6).
Results
Frontal sinus general anatomical structures
In the evaluation according to age, the rate of septal deviation differed between age groups. Of those aged <18 years, 70.3% did not have a septal deviation; of those aged >18 years, 63.5% had a septal deviation (P < 0.005). Frontal sinus hypoplasia was detected in 71.4% of participants aged <18 and in 28.6% of adults (P < 0.005). Frontal sinus hyperplasia had the lowest rate, but there was no significant difference between the ages (Table 1).
Frontal sinus anatomical structures and variations.
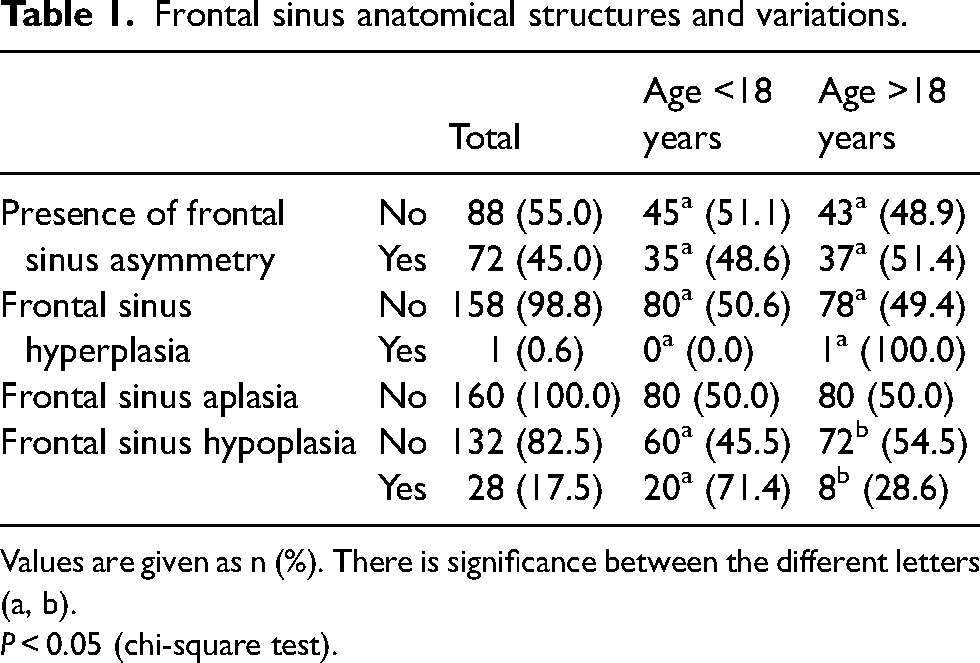
Values are given as n (%). There is significance between the different letters (a, b).
P < 0.05 (chi-square test).
IFAC frontal sinus classification by age
Without the distinction of parties, in the frontal sinus classification according to IFAC, in those aged <18 years: for anterior-based cells, there were agger nasi cells at a rate of 93.1% (n = 149), supra agger cells at 41.9% (n = 67), and supra agger frontal cells at 60.0% (n = 96).
In patients aged <18 years, the prevalence of anterior-based cells were as follows: agger nasi cells were detected at a rate of 93.1% (n = 149) and supra anger cells at 41.9% (n = 67). For posterior-based cells, suprabullar cells were detected at a rate of 76.3% (n = 122), suprabullar frontal cells at 58.8% (n = 94), and supraorbital ethmoid cells at 18.8% (n = 30). For medially based cells, there were no frontal septal cells. In adult patients aged >18 years, the prevalence of anterior-based cells were as follows: agger nasi cells were detected at a rate of 86.3% (n = 138), supra agger cells at 35.0% (n = 56), and supra agger frontal cells at 44.4% (n = 71) (Table 2).
IFAC frontal sinus classification by age regardless of side.
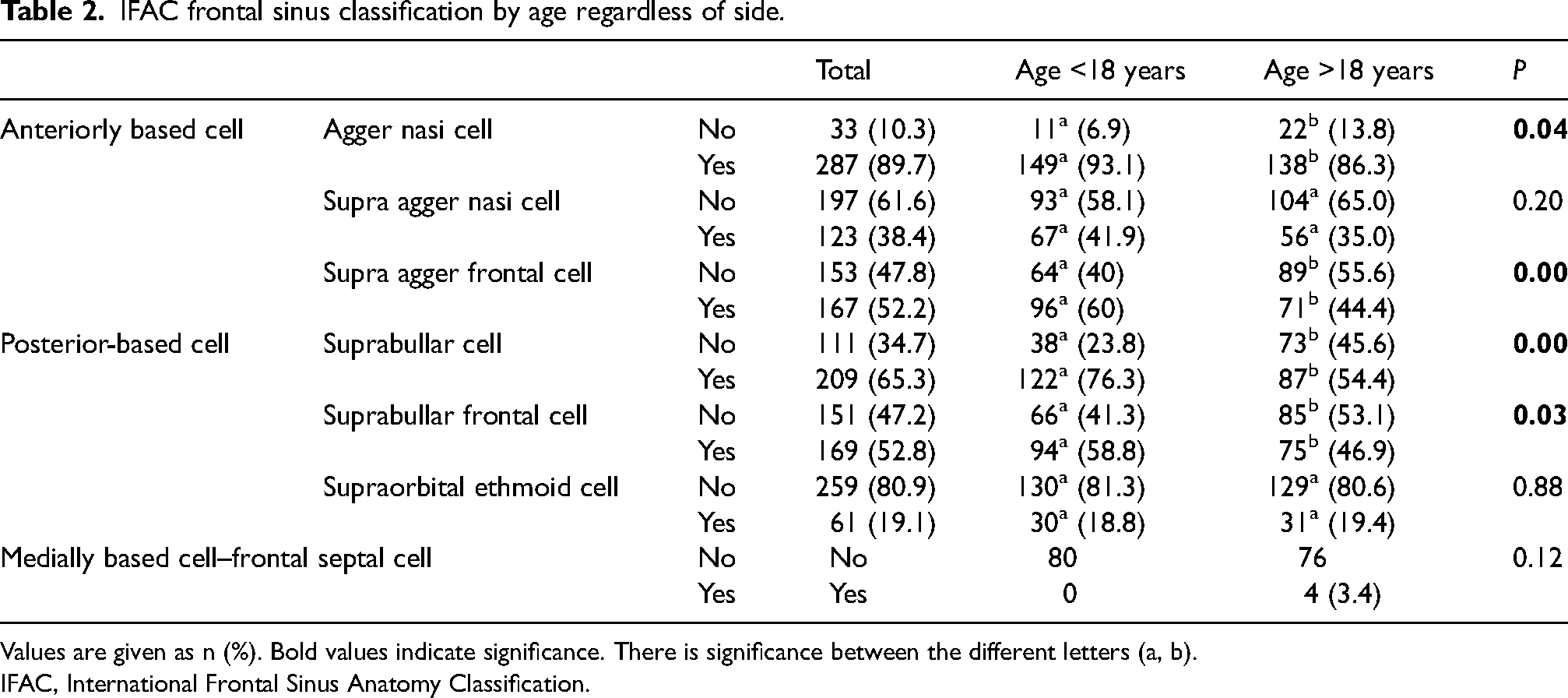
Values are given as n (%). Bold values indicate significance. There is significance between the different letters (a, b).
IFAC, International Frontal Sinus Anatomy Classification.
Unilateral and bilateral distribution
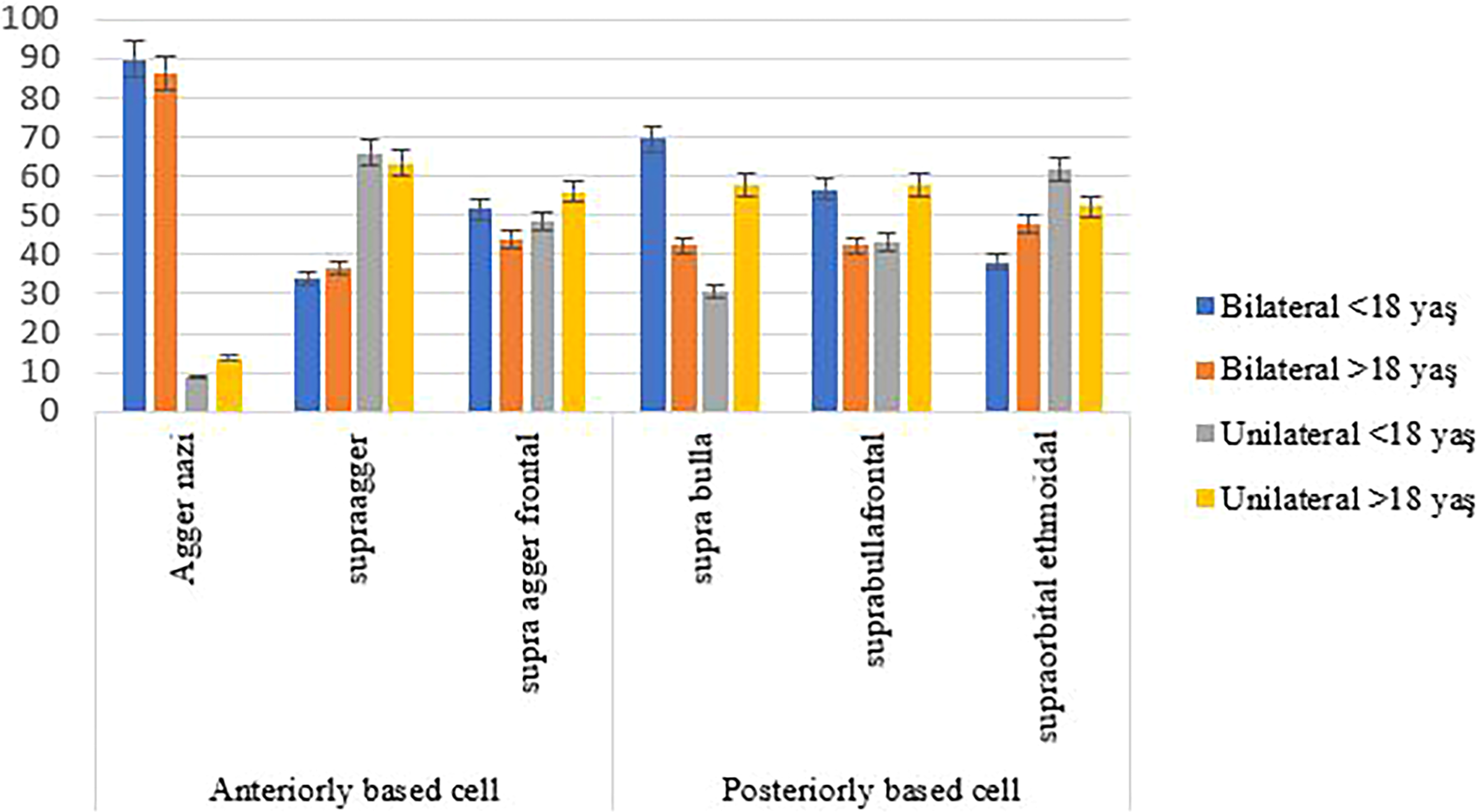
While suprabullar cells were observed bilaterally in 50 (69.44%) patients in the pediatric group and 25 (42.37%) adults, suprabullar frontal cells were observed in 34 (56.66%) pediatric patients and 22 (42.36%) adults. Supra ethmoidal cells were observed bilaterally at a rate of 38.09% (n = 8) in the pediatric group and 47.61% (n = 10) in the adult group.
Agger nasi, supra agger frontal, suprabullar, and suprabullar frontal cells were seen at a higher rate in pediatric patients than in adults, and the difference between them was statistically significant (P < 0.005). Bilaterally, the presence of agger nasi cells, the most among the anterior-based cells, and the presence of suprabullar cells, the most among the posterior-based cells, were detected.
Considering the unilateral and bilateral incidence of the cells, agger nasi cells were highly observed bilaterally in both the pediatric group (n = 71, 89.87%) and the adult group (n = 64, 86.48%) (Table 3). Supra agger cells were observed unilaterally at a high rate in both age groups (66% in the pediatric group, 63.41% in the adult group) (Fig. 2).
Distribution of cell locations.
Unilateral and bilateral distribution of cells by age group.
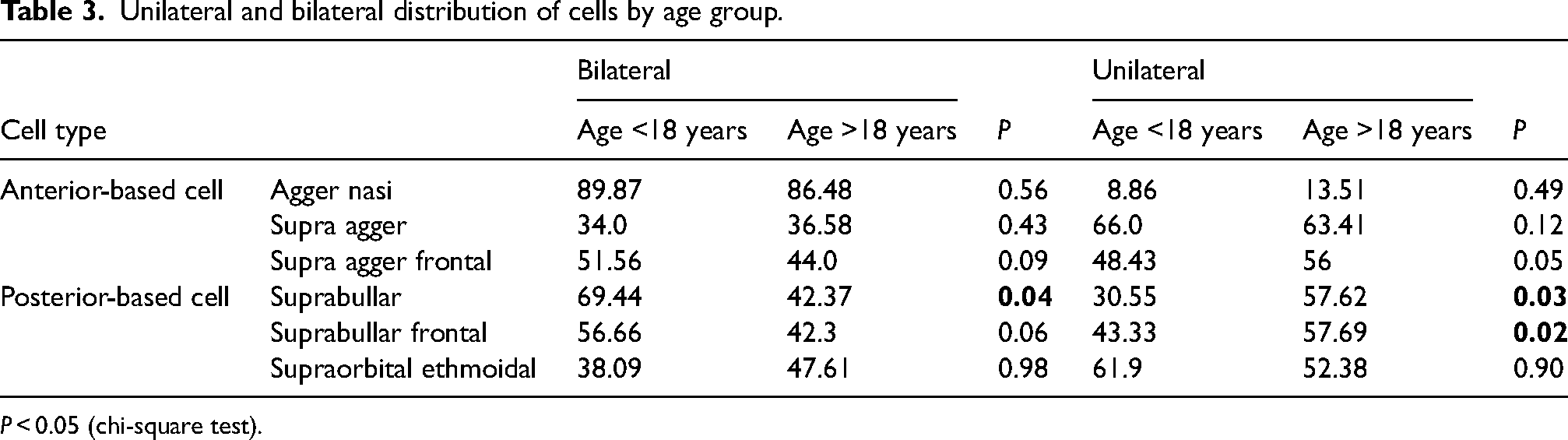
P < 0.05 (chi-square test).
Discussion
Ventilation of the frontal sinus through the natural ostium is associated with both frontal rhinosinusitis and many complications, and the dimensions of the frontal sinus ostium are critical for frontal sinus drainage (10–14). In this study, it was determined that the height, length, and width of the frontal sinus develop rapidly during adolescence, and the height and width show significant differences in children and adults, and the diameter of the frontal ostium is higher in adults.
The main result of our study is the presence of agger nasi (89.87%, bilateral), suprabullar (69.44%, bilateral) and supra agger (66.0%, unilateral), respectively, as the three most common cell groups in the pediatric group, and the presence of agger nasi (86.48%, bilateral) supra agger (66.0%, unilateral) and suprabullar frontal (57.69%, unilateral) cells, respectively, as the most common cell groups in the adult group. On the contrary, supraorbital ethmoid cells were seen bilaterally (47.61%) in adults and unilaterally (61.9%) in children. Although development of the frontal sinus continues until the age of 18 years, these frontal recess cells should be considered in surgical interventions at an early age. In addition, the combination of supraorbital ethmoid cells and suprabullar frontal cells associated with a pattern of pneumatization in both children and adults can lead to unsuccessful FESS results; therefore, proper identification of these cell groups in both preoperative imaging and intraoperative examination may be critical for long-term success in surgery at the frontal sinus exit site.
Much effort has been made to define and classify these cells, which have recently shown their effect on frontal sinus drainage, with IFAC describing the pneumatization pattern of the ethmoid and frontal sinuses (12,15). This classification system was developed as a clinical guide to provide a more anatomically accurate description of pneumatization patterns. However, possible differences in the frontal sinus between ages have not been studied in IFAC. Therefore, with age, it is extremely important to follow the cell differentiations in the frontal recess, which has such variable anatomical features. In a study on the clinical applicability and importance of IFAC, it has been reported that >65% of the residents included in the study found IFAC clinically applicable, and >70% saw it as a tool that helps in consistent communication between surgeons, and 65.6% agreed that it is necessary to understand the classification system.15 However, it was emphasized that IFAC needs to be supported by intraoperative findings and should be studied with large samples (16,17).
Investigating the frontal sinus in adults according to IFAC criteria, Sjogren et al. reported that agger nasi cells were the most commonly reported anterior-based cell (88.9%) and suprabullar cells were the most commonly reported posterior-based cell (55.8%) (18). Choby et al. reported that agger nasi cells, suprabullar cells, supra agger cells, supraorbital ethmoid cells, supra agger frontal cells, and suprabullar frontal cells were detected at rates of 96.5%, 72.0%, 30.0%, 30.0%, 28.5%, and 20%, respectively, and reported that agger nasi cells were the most seen bilaterally (19). Başer et al., who evaluated frontal recess cells in adults according to IFAC, reported that agger nasi was found bilaterally in 91.3%, supra agger in 18.0%, supra agger frontal in 5.3%, and suprabullar cells in 41.3% (15). We determined that agger nasi cells were the cell groups with the highest prevalence bilaterally for age<18 years. Our study detected other cell groups at higher rates than the literature, except for the agger nasi and suprabullar cells. Similarly, in the study by Sjogren et al., the most common IFAC cell types were found to be agger nasi, suprabullar, and supra agger cells, with rates of 88.9%, 55.8%, and 29.5%, and it has been stated that the bilateral presence of these cell groups is also higher. Similar to the literature, we also found that anterior-based agger nasi (89.7%) and posterior-based suprabullar cells (65.3%) were most common in all individuals, and the bilateral incidence of these cells was consistent with the literature.
According to the IFAC, posterior-based suprabullar frontal cells pneumatize along the skull base in the posterior region of the frontal sinus, while a supraorbital ethmoid cell is defined as a group of cells that pneumatize around, in front of, or behind the anterior ethmoid artery on the roof of the orbit (12). suprabullar frontal and supraorbital ethmoid cells may extend into the frontal sinus and occlude the frontal ostium posteriorly (19–21). Our cohort determined that supra-orbital ethmoid cells were seen in 18.8% and 19.4% of children and adults, respectively, and suprabullar frontal cells were seen in 58.8% and 46.9% of children and adults, respectively, but only suprabullar frontal cells created a significant difference between ages. In addition, the bilateral incidence of suprabullar frontal cells (56.66%) in the pediatric group and unilateral incidence in adults (57.69%) was higher.
Hyperpneumatization of the frontal bone causes an anteroposterior extension towards the outer diploes of the frontal bone, which affects the incidence of frontal cell types with age (22). In our study, while significant changes did not occur in anteriorly located cells with age, significant differences were observed in posteriorly located cells. That is, while the incidence of suprabullar cells bilaterally decreases with age, the increase in the incidence of unilateral suprabullar and suprabullar frontal cells is quite striking. Attention should be paid to these changes with age and the bilateral and unilateral differences in frontal cells.
Because the frontal cell groups have the potential to change the shape of the frontal sinus through drainage, they may predispose to iatrogenic injury with potential complications of advanced surgery, periorbital or intraorbital hematoma, intracranial hemorrhage, and epistaxis preventing cerebrospinal fluid leakage. These complications can be avoided with a thorough understanding of patient-specific variations in anatomy through preoperative imaging studies. In addition, understanding how frontal cells change with age and their localization may assist surgeons in obtaining a patent frontal ostium by performing a frontal sinusotomy.
The present study has some limitations. The most significant is that it is not multi-centered, which may cause possible local differences to be overlooked. In addition, diversifying the number of cases and age groups will make the study even more valuable. In addition, surgical follow-up is needed to better assess the clinical significance of this classification system.
In conclusion, surgery of the nasofrontal region aims to provide optimum surgical conditions by expanding the frontal recess and ostium without damaging the surrounding anatomical structures. Therefore, it is extremely important to determine how the cells in this region change with age and the localization and anatomy of the cells that can be encountered in children and young patients. The patients should be evaluated by considering the development of the frontal sinus by age, regional differences, and IFAC criteria.
Footnotes
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.