
Abstract
Background
Postpartum dyspnea is commonly observed, but its cause is often unknown.
Purpose
To investigate postpartum dyspnea, we compared lung iodine mapping (LIM) using dual-energy computed tomography (DECT) between postpartum women and women suspected of having pulmonary thromboembolism (PTE).
Material and Methods
In this retrospective study, 109 women of reproductive age (50 postpartum women, 59 women unrelated to pregnancy) underwent DECT between March 2009 and August 2020. Among the postpartum women, 23 patients were excluded due to late-onset dyspnea (n=20: >48 h after delivery) or the presence of PTE (n=3). A total of 86 patients were divided into three groups (27 postpartum women [postpartum group], 19 women with PTE [PTE group], and 40 women without PTE [non-PTE group]). Quantitation was applied to a decreased LIM value (LIM5; defined as <5 HU) and the relative value of LIM5 to whole LIM volume (%LIM5). LIM defects were classified into five patterns (0 = none, 1 = wedge-shaped, 2 = reticular/liner, 3 = diffuse granular/patchy, 4 = massive defects) based on a consensus between two readers.
Results
There were significant differences in the LIM5 and %LIM5 values among the three groups. The LIM5 and %LIM5 were largest in the PTE group, and postpartum women showed intermediate values between the non-PTE and PTE groups. Wedge-shaped defects were prominent in the PTE group, and diffuse granular/patchy defect was a typical feature in the postpartum group.
Conclusion
Postpartum women with dyspnea showed granular/patchy defects on DECT with a median quantitative value between the PTE and non-PTE groups.
Keywords
Introduction
Dyspnea is a very frequent complication in peripartum and postpartum women. During a normal pregnancy, the symptom may be associated with various diseases, including—but not limited to—physiologic dyspnea of pregnancy, respiratory tract infection, asthma, anemia, and peripartum cardiomyopathy (1).
Pregnancy itself is also a risk factor for deep venous thrombosis, and pulmonary thromboembolism (PTE) typically presents in the postpartum period with dyspnea and tachypnea. PTE and amniotic fluid embolism (AFE) are also two of the most common causes of maternal mortality (2). The etiology of AFE is related to the transfer of amniotic fluid into the maternal circulation, whereby an idiosyncratic reaction is triggered and leads to decreased cardiac output with consequent maternal collapse (3). Vasoconstriction of the pulmonary arteries and increased pulmonary vascular resistance are the primary mechanisms responsible for the cardiovascular collapse in AFE before left ventricular failure (3). However, amniotic fluid has also been shown to be present in the maternal circulation without any clinical consequences (4–6).
Dual-energy computed tomography (DECT) can provide several potential advantages over single-energy CT, including material differentiation beyond the differences in attenuation. The material differentiation of iodine, in the form of dual-energy iodine mapping, might provide relevant functional and prognostic data, beyond a simple luminal assessment of the pulmonary arteries (7). DECT depicts decreased lung iodine map (LIM) values due to pulmonary vasoconstriction or intrapulmonary clot from PTE or chronic thromboembolic pulmonary hypertension (8,9).
The aim of the present study was to investigate the qualitative and quantitative association of LIM values with postpartum dyspnea using DECT.
Material and Methods
Patient selection
This retrospective study was approved by the regional ethic review board, and the requirement for written informed consent was waived. We electronically searched for women aged 20–47 years who had undergone initial DECT obtained at 90/140 kV using first-generation dual-source CT (DSCT) without a tin filter (SOMATOM Definition; Siemens Healthcare, Forchheim, Germany) and at 100 Sn/150 kV using third-generation DSCT with a tin filter (SOMATOM Force) due to dyspnea or clinical suspicion of PTE. Imaging at 90/140 kV was performed between January 2014 and August 2016, while imaging at 100 Sn/150 kV was performed between November 2016 and April 2020.
A total of 140 women who underwent initial DECT were ultimately selected in this study (Fig. 1). Of the 140 women, 24 were excluded due to severe pulmonary co-morbidities, including pulmonary emphysema, massive pneumonia, or atelectasis (10), and 7 of the remaining 116 patients were excluded due to insufficient breath-holding during DECT scanning.
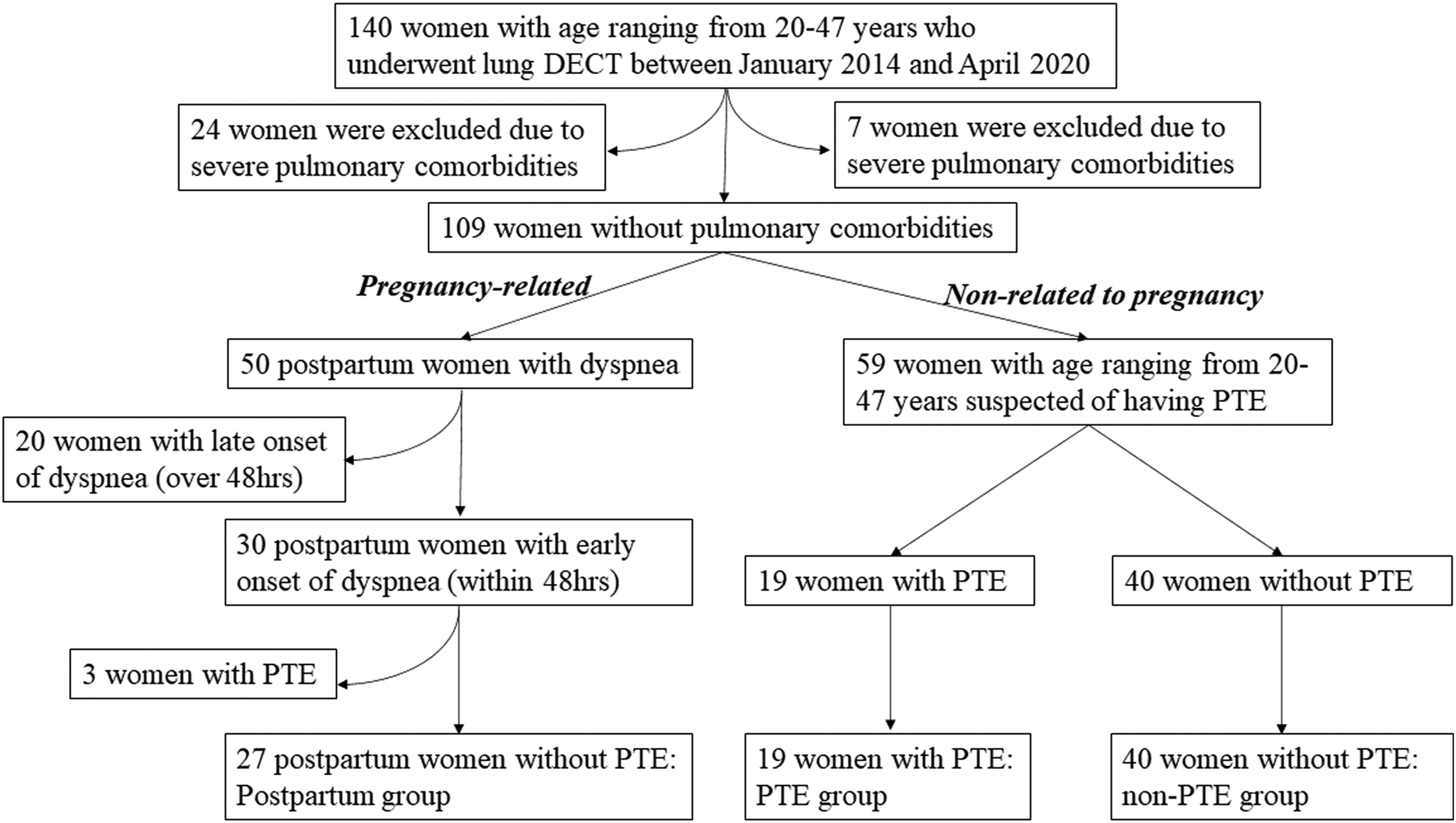
Flow diagram of patient selection.
Of the 50 postpartum women, 20 were excluded due to the late onset of dyspnea (>48 h), and 3 of the 30 postpartum women with PTE were also excluded from this study. The 59 remaining women with suspected PTE were divided into two groups based on the presence or absence of PTE (non-PTE and PTE groups). This study therefore consisted of three groups: the non-PTE group (n = 40; mean age = 38.9 years; age range = 22–47 years); the PTE group (n = 19; mean age = 39.0 years; age range = 25–46 years), and the postpartum group without PTE (n = 27; mean age = 33.3 years; age range = 24–47 years) (Fig. 1).
CT protocol
The first- and third-generation DSCT systems were equipped with two X-ray tubes and two corresponding detectors, which were oriented in the gantry with an angular offset of 90°. The first detector array (corresponding to tube A) of the first-generation DSCT system provided a field of view (FOV) of 50 cm, and the second detector array (corresponding to tube B) was restricted to a FOV of 26 cm, compared to a wide FOV of 35 cm in the third-generation DSCT system. The tube settings of the first-generation DSCT system were 80/140 kVp, while those of the third-generation DSCT system were 100 Sn/150 kVp with tin filtering. The detector collimations were set to 2 × 64 × 0.6 mm versus 2 × 196 × 0.6 mm, the gantry rotation times were 0.33 s versus 0.25 s, and the pitch values were 0.5 s versus 0.2 5 s (first-generation vs. third-generation), respectively.
DECT was started using the bolus tracking technique with the intravenous administration of a low-osmolar non-ionic iodinated contrast material (body weight <60 kg: 300 mg iodine/mL and body weight >60 kg: 350 mg iodine/ml iohexol; Omnipaque; GE Healthcare; Chicago, IL, USA) via a 20-G catheter into the antecubital vein using the dual-phase technique followed by 30 mL saline at a rate of 4 mL/s. A caudocranial scan direction was chosen to minimize streak artefacts from dense contrast material in the superior vena cava or innominate vein. Chest scanning required 10–14 s with first-generation DSCT and 4–6 s with third-generation DSCT.
LIM reconstruction
For all patients, three stacks of LIM images were semi-automatically generated: sets of 140 kVp and 80 kVp images in first-generation DSCT and sets of 150 kVp and 100 kVp images in third-generation DSCT. LIM images were generated using the lung perfused blood volume application mode of a dedicated dual-energy postprocessing software program (Syngo Dual Energy software; Siemens Healthcare). All LIM images were transferred to a workstation (AZE VirtualPlace: AZE, Tokyo, Japan) to perform three-dimensional quantification in order to evaluate the decreased LIM values among the three groups, in the range of 1–5 (LIM5) Hounsfield units (HU), and whole LIM, in the range of 1–120 HU (LIM120) (10). The relative ratios of LIM5 to LIM120 were calculated and expressed as %LIM5. Most of these LIM images were measured automatically. However, in some cases with pseudo-iodine mapping enhancement in the trachea as artifact for potential pseudo-negativity LIM, additional correction (removal) was made for tracheal pseudo-LIM enhancement.
Reference standard of PTE, LIM pattern classification, and CT measurements
Three board-certified radiologists (MO, YK, and TN) with 25, 20, and 10 years of experience, respectively, who were all experts in the field of thoracic radiology and had clinical expertise in the use of dual-energy devices, provided the reference standard for the diagnosis or exclusion of PTE in consensus, with blinded access to all participant clinical and imaging data, including the LIMs. The diagnosis of PTE was made based on the following criteria: presence of intrapulmonary clots in the pulmonary arteries on pulmonary CT angiography or with corresponding perfusion defects on LIM of DECT. The final diagnosis was made based on the reference standard, which included the combination of laboratory test results and findings of pulmonary CT angiography and DECT.
LIM defects were classified into five patterns (0 = none (Fig. 2a), 1 = wedge-shaped (Fig. 2b), 2 = reticular/liner (Fig. 2c), 3 = diffuse granular/patchy (Fig. 2d), 4 = massive defects (Fig. 2e)) based on a consensus of two readers (MO and YK). Quantitative CT measurements, including the diameters of the widest right ventricle (RV) and left ventricle (LV), were obtained at each axial CT image, because the axial RV/LV diameter ratio had the same reproducibility and accuracy compared to that in an automatically generated four-chamber view (11).
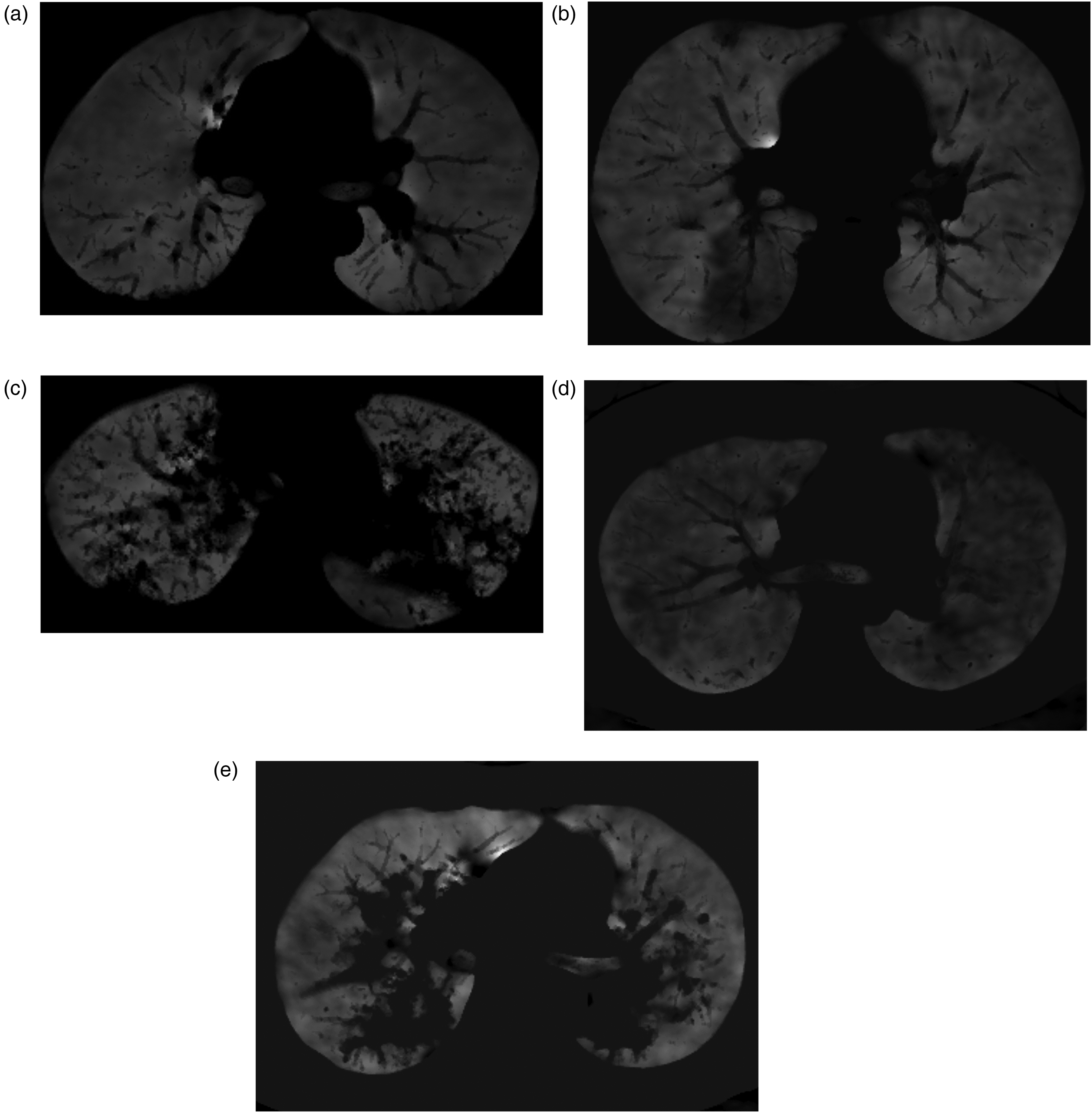
Lung iodine mapping defect patterns on DECT. (a) 0 = no defects (homogenous), (b) 1 = wedge-shaped defects in subpleural space, (c) 2 = reticular/liner defects along the interlobular septum or peribronchovascular interstitium, (d) 3 = diffuse granular/patchy defects, (e) 4 = massive defects in both lower lobes. DECT, dual-energy computed tomography.
Patients with severe pulmonary co-morbidities of pulmonary emphysema, massive pneumonia, or atelectasis were excluded from this study. However, minor plate-like atelectasis, infiltration, or a small amount of plural effusion was noted in each group, and the incidence of these conditions was also compared among the three groups.
Statistical analyses
Variables were summarized as the mean and standard deviation. All statistical analyses were performed using the SPSS software program version 20 (IBM, Armonk, NY, USA).
Categorical variables were compared using the chi-square test and the Kruskal–Wallis/Mann–Whitney U test was used among the three groups. P values <0.05 were considered to indicate statistical significance.
The interrater agreement for LIM patterns was evaluated with intraclass correlation coefficients (ICCs) to test the null hypothesis of no agreement (r = 0) (ICC <0.40 = poor/fair, ICC of 0.41–0.60 = moderate, ICC of 0.61–0.80 = good, ICC >0.80 = excellent agreement) (12).
Results
Postpartum women were significantly younger and had a larger body mass index (BMI) than those in other groups (P <0.01) (Table 1). The platelet counts and PT-INR of postpartum women were significantly lower (P <0.05) and the D-dimer value significantly higher in the PTE group than in other groups (P = 0.03), although there was no significant difference in the fibrinogen level among the groups. Echocardiography showed higher transtricuspid pressure gradient (TRPG) and estimated pulmonary artery pressure (ePAP) in the postpartum and PTE groups, which suggested increased right heart strain compared to the non-PTE group.
Patients’ characteristics and measurements of CT and LIM.
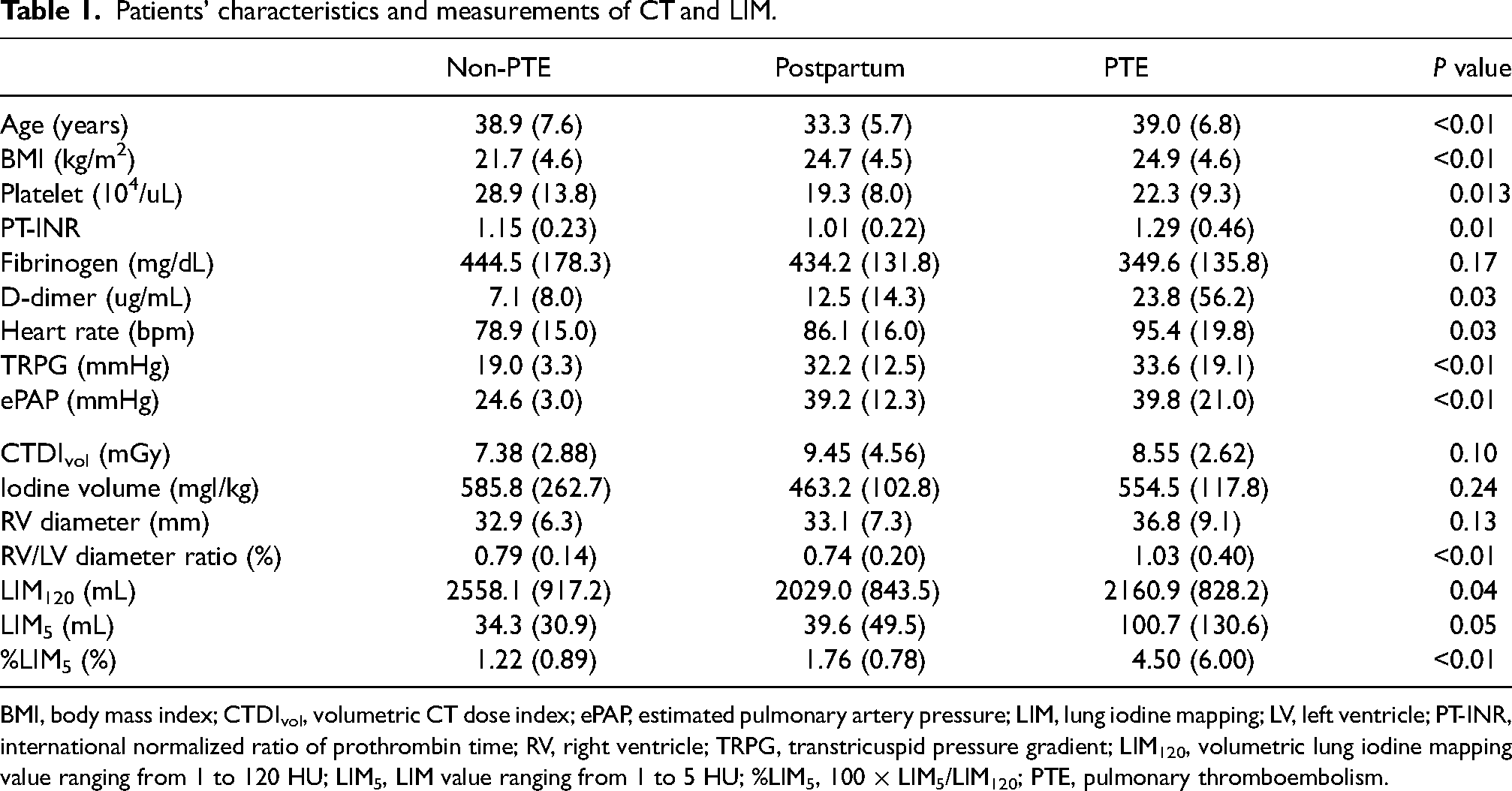
BMI, body mass index; CTDIvol, volumetric CT dose index; ePAP, estimated pulmonary artery pressure; LIM, lung iodine mapping; LV, left ventricle; PT-INR, international normalized ratio of prothrombin time; RV, right ventricle; TRPG, transtricuspid pressure gradient; LIM120, volumetric lung iodine mapping value ranging from 1 to 120 HU; LIM5, LIM value ranging from 1 to 5 HU; %LIM5, 100 × LIM5/LIM120; PTE, pulmonary thromboembolism.
The RV diameter in the PTE group was larger than in the other groups, but not to a significant degree. However, the RV/LV diameter ratio in the PTE group was significantly larger than that in the other groups (P <0.01) (Table 1). Whole LIM volumes were significantly lower in the postpartum and PTE groups than in the non-PTE group (P = 0.04). The LIM5 was significantly increased and led to a significantly higher %LIM5 value in the PTE group than in the other groups (P <0.05). Because of their slightly increased LIM5 and decreased whole LIM values of LIM120, the %LIM5 values in the postpartum group fell between those of the non-PTE and PTE groups (Table 1).
Table 2 and Fig. 3 show that there was no perfusion disturbance on lung iodine mapping in 60% of the women in the non-PTE group (P <0.01). The wedge-shaped LIM defect was a typical finding in the PTE group (P <0.01). Similar patterns were noted in both the non-PTE and postpartum groups. However, granular/patchy defects were prominent in postpartum women (P = 0.04). The inter- and intra-reader ICCs of the LIM defect patterns were fair, in the range of 0.50–0.66 (95% confidence interval = 0.33–0.78).
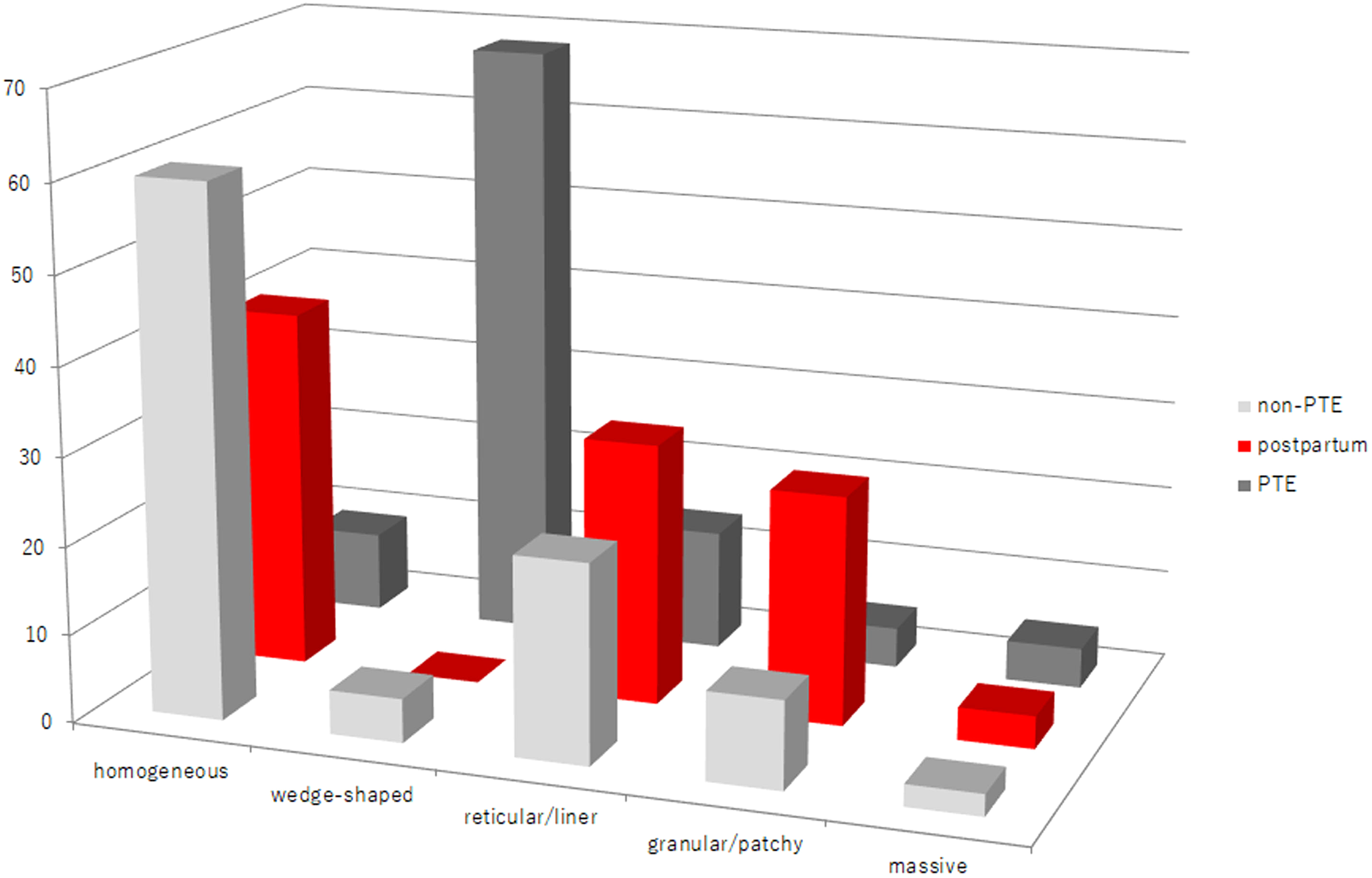
Bar graph of the distribution patterns of lung iodine map defects in each group.
LIM defect patterns and pulmonary co-morbidities.
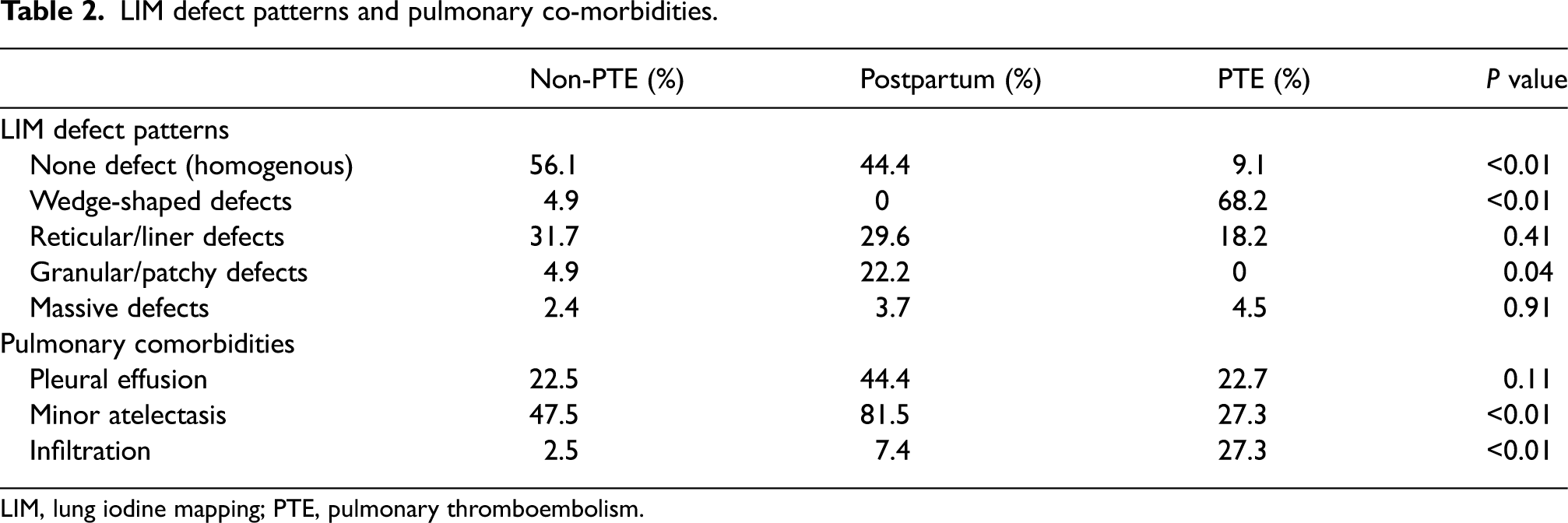
LIM, lung iodine mapping; PTE, pulmonary thromboembolism.
An additional quantitative analysis was applied to %LIM5 between the non-PTE and postpartum groups in each defect pattern using the Mann–Whitney U test, as Fig. 3 showed similar defect patterns in patients in these groups without a granular/patchy defect. There was no significant difference in the %LIM5 by defect pattern (Table 3). However, the mean %LIM5 value in postpartum women (3.17%) with granular/patchy defects was larger than that in non-PTE women (1.30%) without significance (P = 0.06). In postpartum women, the area of granular/patchy defects might be wider than that in non-PTE women.
%LIM5 between non-PTE and postpartum groups in each LIM defect pattern.
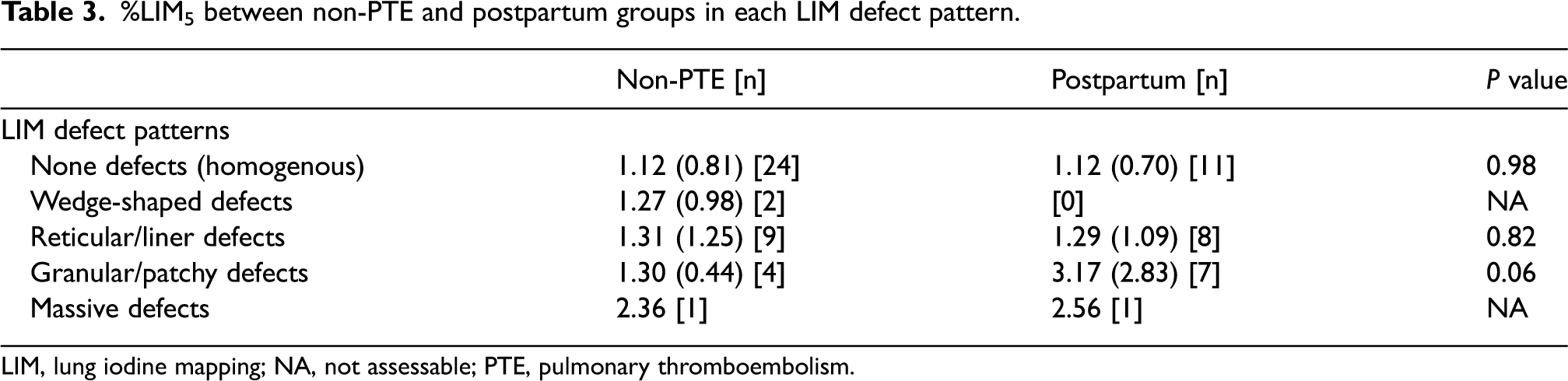
LIM, lung iodine mapping; NA, not assessable; PTE, pulmonary thromboembolism.
There was no significant difference in the radiation dose, as measured by the volumetric CT dose index (CTDIvol), among the three groups (Table 1). However, the CTDIvol in postpartum women was high because of their high BMI values.
Discussion
Dyspnea is a very frequent complaint in peripartum and postpartum women. Physiologic dyspnea of pregnancy, anemia, respiratory tract infection, bronchial asthma, and PTE are major etiologies of peripartum and postpartum dyspnea (1). Thromboembolic events frequently occur during pregnancy as this period is characterized by hypercoagulability (13). In our study, 3 of 30 (10%) postpartum women had PTE and were excluded from this study. The %LIM5 in postpartum women was an intermediate value between the values in the non-PTE and PTE groups. Fig. 3 showed a similar pattern of LIM defect in the postpartum group to that in the non-PTE group, without granular/patchy LIM defects. No perfusion disturbance (homogenous perfusion) was noted in either the non-PTE or postpartum group, because of the lack of an intrapulmonary clot burden. However, the ratio of homogenous perfusion of LIM in the postpartum group was lower than that in the non-PTE group (Table 2), as there were various causes of postpartum dyspnea, including peripartum cardiomyopathy, and AFE (1). We used a Siemens workstation based on image-data dominant reconstruction. Image-data dominant reconstruction produces LIM defects as an artifact for potential pseudo-positivity due to beam-hardening effect, unlike row-data dominant reconstruction. Wedge-shaped iodine defects are typical findings in PTE. However, interstitial edema or small plate-like atelectasis might be visualized as plate or wedge-shaped LIM defects in postpartum and non-PTE groups.
Amniotic fluid and cellular components (squames, vernix, mucin, lanugo) create pulmonary vasoconstriction and increased pulmonary vascular resistance, leading to a decreased cardiac output with consequent maternal collapse (3). However, the relevance of the detection of fetal squamous material in the pulmonary vasculature, as an indicator of AFE, is uncertain (4–6). In general, AFE is clinically diagnosed as sudden cardiovascular collapse, after exclusion of other possible causes. However, obtaining robust information about the condition is challenging because of its difficulty to diagnose. The diagnostic criteria for AFE varies from country to country, and its pathophysiology and management have all been historically hampered by a lack of uniform diagnostic criteria (14,15). Historically, the diagnosis of AFE was usually made at an autopsy, when fetal squames were found within the pulmonary vasculature. Considering the potential immunological involvement, there has been interest in the measurement of certain markers, such as complement, tryptase, and amniotic fluid, as AFE is considered to be a diagnosis of exclusion (16). Pulmonary microvascular occlusion was also evaluated using DECT in patients with sickle cell disease (17) and has been postulated to be a major pathophysiologic driver. Pulmonary microvascular occlusion on DECT without commensurate parenchymal opacities might represent early/mild sickle cell disease with acute chest syndrome. DECT also reveals pulmonary micro-thrombosis or microangiopathy with micro-thrombosis even in the absence of visible pulmonary arterial thrombosis in patients with COVID-19 pneumonia (18,19). There is no recognized or readily available diagnostic test for AFE, and a range of investigations for AFE, including hematological studies, electrocardiograms, chest X-rays, CT scans, and echocardiographs, may be required. Lung CT was reported to visualize diffuse homogeneous ground-glass shadow, suggesting non-cardiogenic or cardiogenic pulmonary edema (20), while cardiac magnetic resonance imaging was reported to show delayed linear enhancement at the mid-wall of the left ventricle as in peripartum cardiomyopathy (21). These findings were associated with delayed and severe cardiac syndrome after AFE.
Granular/patchy LIM defects in DECT might be a new and early finding of pulmonary vasoconstriction caused by the immunological response to amniotic fluid (Fig. 2d), as the immune-mediated reaction to amniotic fluid is an important factor in the development of AFE. Pulmonary arterial pressure would be expected to rise as a consequence of hypoxic vasoconstriction in the pulmonary vascular bed (22) and, indeed, in the postpartum group, echocardiography showed higher values of TRPG and ePAP equal to those in PTE group than non-PTE group (Table 1). However, granular/patchy LIM defects were also noted in the non-PTE group, but the ratio and degree of decreased LIM differed between the postpartum and non-PTE groups without significance (P = 0.06). In postpartum women with granular/patchy LIM defects, the area of the perfusion defect was large and frequent. One patient (Fig. 2d) experienced prolonged pulmonary hypertension after delivery. Amniotic fluid itself is reported to be present in the maternal circulation without any clinical consequences (4–6). However, granular/patchy LIM defects were also noted in women without PTE (Fig. 3) and were prominent in postpartum women (Table 2). In our study, postpartum women with late-onset dyspnea (>48 h) were excluded, as AFE classically shows an acute onset during labor and delivery or in the immediate postpartum period. Rare exceptions to this timing of onset have been reported as late as 48 h postpartum or after cesarean delivery, amniocentesis, or removal of the placenta, or with first and second trimester abortions (23–25).
The present study has some limitations. First, the study population was relatively small, as the target patients were fertile women and those of the same age with suspected PTE. In Japanese diagnostic criteria for AFE, its symptoms appeared during pregnancy or within 12 h of delivery (14). However, due to the small number of patients who underwent DECT within 12 h after delivery, it was necessary to raise the examination interval up to within 48 h. The second limitation is the presence of artifacts related to DECT, including beam-hardening artifacts caused by the presence of dense contrast material in the beating heart or superior vena cava, as well as cardiac motion artifacts and focal iodine defects along the periphery of the lung (26). We did not prove the presence of amniotic fluid material in the maternal pulmonary circulation in this study, because it was difficult to take lung tissue from the mother immediately after delivery. Further evaluations might be needed in order to investigate the relationship between amniotic fluid and perfusion disturbance of granular/patchy defect appearance on DECT. Finally, DECT carries risks related to the use of contrast material and radiation exposure. In this study, there were no significant differences in the radiation dose of CTDIvol among the three groups, with the dose in the range of 7.0–9.0 mGy (Table 1), and these values did not exceed the provincial diagnostic reference level for the chest (27). Thoracic DECT is reported to be feasible without any additional dose (28); however, we must pay attention to the patient's radiation exposure.
In conclusion, postpartum women with dyspnea not related to PTE showed granular/patchy defects on DECT with slightly decreased lung perfusion compared to women in the non-PTE group. Further evaluations will be needed to investigate the cause of a granular/patchy LIM defect-appearance on DECT in postpartum women without pulmonary emphysema or PTE.
Footnotes
Acknowledgments
We gratefully acknowledge the work of previous members of Yamaguchi University Hospital and present members of the National Hospital Organization, Kanmon Medical Center.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received the following financial support for the research, authorship, and/or publication of this article: The corresponding author (M.O.) received Grants-in-Aid for Scientific Research from Japan Society for Promotion of Science to investigative amniotic fluid embolism using dual energy CT. The other authors state that they have not received any funding for this work.