
Abstract
Background
In patients with an acute aortoceliac angle, the diagnostic catheter often fails to enter the common hepatic artery.
Purpose
To retrospectively evaluate the impact of aortoceliac angle on the implantation of a port-catheter system via a femoral approach for hepatic arterial infusion chemotherapy (HAIC) in patients with advanced hepatocellular carcinoma (HCC).
Material and Methods
A total of 399 patients with advanced HCC underwent percutaneous implantation of a port-catheter system for HAIC. Among these patients, 383 underwent successful implantation via a femoral artery approach (success group). In 16 patients, port-catheter systems were implanted via a subclavian artery approach (failure group) after failure of the initial attempt via the femoral artery due to failed catheter tip fixation to the gastroduodenal artery. We statistically analyzed aortoceliac angle, ostial celiac stenosis, sex, age, weight, height, and body mass index (BMI) between groups.
Results
The average aortoceliac angle, weight, and BMI were significantly different between the two groups (P < 0.001, P = 0.02, P < 0.001, respectively). Among them, only the aortoceliac angle was a significant risk factor in logistic regression analysis. The smaller the aortoceliac angle, the more often the femoral approach failed (P < 0.001, odds ratio = 0.817, 95% confidence interval = 0.752–0.887). There were no significant differences in ostial celiac stenosis, sex, or age between the two groups (P = 0.549, 0.056, 0.173, and 0.773, respectively).
Conclusion
For patients with an acute aortoceliac angle, the femoral approach is likely to fail. A subclavian artery approach should be preferentially considered for percutaneous implantation of a port-catheter system in such patients.
Introduction
Of patients with hepatocellular carcinoma (HCC), 20% have portal vein tumor thrombosis (PVTT) at initial diagnosis. For advanced HCC with PVTT, treatment with sorafenib or other systemic drugs is currently recommended as the standard of care, but the efficacy of such treatments is still limited (1). Transarterial radioembolization (TARE) is another recommended locoregional treatment for HCC, but it is technically complicated, costly, and limited to bilobar disease or main portal vein invasion (2). Repeated hepatic arterial infusion chemotherapy (HAIC) via an implanted-port catheter system has been considered to be an alternative treatment option for advanced HCC with PVTT (3,4). HAIC using an arterial port system is theoretically more effective for HCC than systemic chemotherapy (3,4). HAIC allows a high concentration of anticancer drugs to be delivered locally to hypervascular tumors, thereby keeping systemic concentrations of chemotherapeutic agents low due to the first-pass effect (5). Many studies have reported that HAIC is a useful modality for patients with advanced HCC (3,5–9). HAIC is widely used in Asia, especially in Japan and the Republic of Korea (3,10).
For percutaneous implantation of hepatic arterial infusion port-catheter systems, several arteries, including the brachial, subclavian, femoral, and hypogastric arteries, have been used as percutaneous access routes, among which the subclavian and femoral arteries are most frequently selected (11). In patients with an acute aortoceliac angle, the diagnostic catheter often fails to enter the common hepatic artery or is easily dislodged when using the femoral approach. Previous studies compared the success rates and complications of the subclavian and femoral approaches (12), but, to the best of our knowledge, no study has specifically focused on the impact of the aortoceliac angle (the angle between the celiac axis and abdominal aorta) during implantation via a femoral artery approach.
The aim of the present study was to retrospectively evaluate the impact of the aortoceliac angle on port-catheter system implantation for HAIC via a femoral approach.
Material and Methods
The institutional review board (IRB) of our institution approved this retrospective review of patient medical and imaging records. The need for informed consent was waived by the IRB. Between January 2008 and November 2018, 399 patients with advanced HCC were enrolled in this study, and all were treated with HAIC using a percutaneous hepatic arterial port-catheter system via the celiac trunk. The patients who had a hepatic arterial port-catheter system via the superior mesenteric trunk were excluded. All patients were refractory or not candidates for other locoregional treatments, such as radiofrequency ablation or transcatheter arterial chemoembolization (TACE). All tumors were diagnosed based on characteristic findings on ultrasonography, computed tomography (CT), conventional angiography, or magnetic resonance imaging (MRI) (13), as well as serum tumor markers (a-fetoprotein or protein induced in vitamin K absence or antagonist II [PIVKA-II]) or biopsy. The decision to perform HAIC was made by hepatologists and an interventional radiologist after consultation based on CT and MRI.
In 16 (4%) patients, the port-catheter systems were implanted via the left subclavian artery (failure group) (Fig. 1) after unsuccessful attempts of implantation via the femoral artery due to catheter tip fixation failure in the gastroduodenal artery. Another 383 (96%) patients underwent successful implantation of a port-catheter system via the femoral artery during the same period (success group) (Fig. 2).
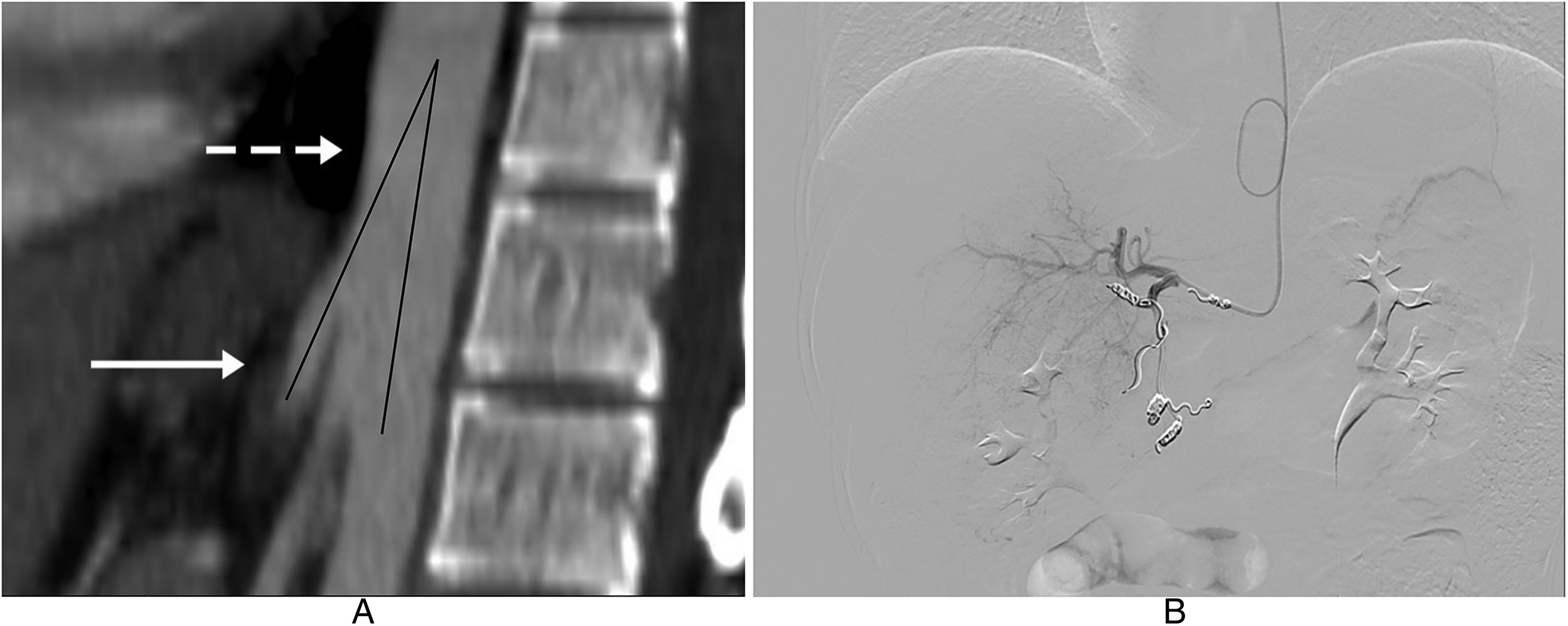
Representative image of the failure group. (a) Multiplanar reconstruction CT image shows an acute angle (16.7°, black line) between the celiac axis (solid arrow) and the abdominal aorta (dashed arrow). (b) Final digital subtraction angiography shows successful implantation of the infusion-port system via a subclavian approach.
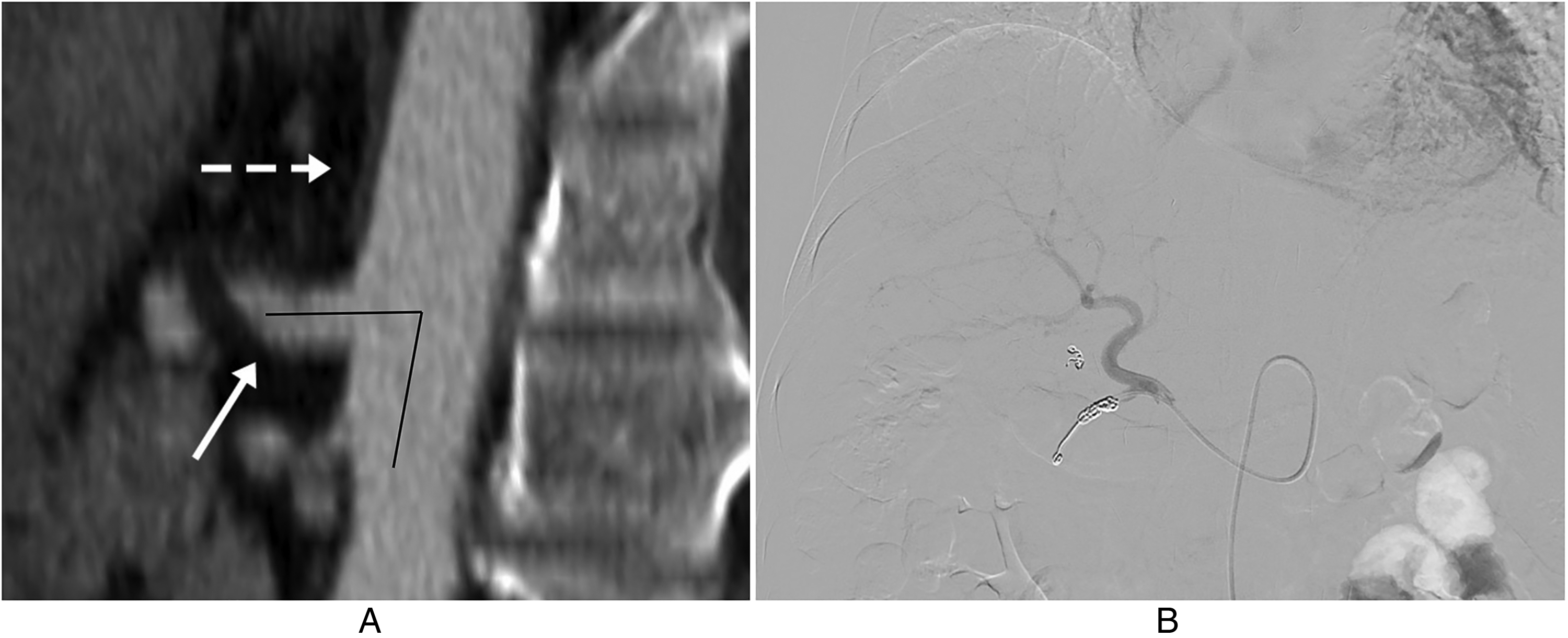
Representative image of the success group. (a) Multiplanar reconstruction CT image shows a nearly perpendicular angle (79.4°, black line) between the celiac axis (solid arrow) and the abdominal aorta (dashed arrow). (b) Final digital subtraction angiography shows successful implantation of the infusion-port system via a femoral approach.
Procedures
All procedures were performed in a dedicated vascular interventional suite equipped with digital subtraction technology by two interventional radiologists who each had >7 years of experience in the field of interventional radiology. A femoral approach was initially attempted for all patients. After the common femoral artery was punctured with an 18-G Angiocath needle, a 0.035-inch guidewire (Terumo, Japan) was inserted. A 5-Fr catheter (Radifocus Introducer II; Yashiro, Terumo, Tokyo, Japan) without introducing sheath placement was inserted over the guidewire, and celiac and superior mesenteric arteriography were performed to precisely evaluate arterial anatomy. The right gastric and accessory left gastric arteries were embolized with microcoils (Tornado; Cook, Bloomington, IN, USA) to prevent reflux of anticancer drugs into the stomach during HAIC. Using the catheter-exchange method, a port catheter (CELSITE; B. Braun Medical, Center Valley, PA, USA) with one side hole was inserted via the common femoral artery. If the port catheter was placed through the celiac artery, the fixed catheter tip technique was applied, and anchoring at the gastroduodenal artery was achieved by placing microcoils (Vortex Microcoil and Interlocking Detachable Coil; Boston Scientific, Watertown, MA, USA) (14,15). If the tip was not located in the gastroduodenal artery despite several attempts, the procedure was changed to a left subclavian approach. Failure was defined as when the port catheter was unable to enter the gastroduodenal artery while the guidewire was sufficiently inserted into the gastroepiploic artery or when the port catheter was immediately dislodged after removal of the guidewire. After puncture of the subclavian artery, a 0.035-inch guidewire was inserted into the aorta under fluoroscopy. Then, a 5-Fr cobra catheter (Terumo) was inserted into the descending thoracic aorta and advanced selectively into the celiac artery. The port catheter was then fixed to the gastroduodenal artery using the method mentioned above (16,17). In all patients in both groups, a side hole of approximately 1 × 2 mm was created using scissors at the point that all hepatic arteries were visualized, approximately 5 cm from the end of the in-dwelling catheter.
Clinical parameters
The aortoceliac angle was examined on multiplanar reconstruction (MPR) CT imaging, including both long axes of the aorta and celiac axis ostium at the sagittal plane (Aquarius iNtuition Viewer 4.4; Terarecon, San Mateo, CA, USA). Ostial celiac stenosis was evaluated on CT MPR images. Stenosis was defined as luminal narrowing >50% in the shortest diameter. Catheter dislodgement was evaluated using arteriography and contrast-enhanced cone-beam CT, which were performed to evaluate the distribution of contrast and function of the implanted port on the day after implantation. Data on sex, age, height, weight, and body mass index (BMI) were collected from electronic medical records.
Statistical analysis
All statistical analyses were performed with SPSS 18.0 software (SPSS, Chicago, IL, USA), and P values <0.05 were considered statistically significant. The two groups were compared with Student's t-test or the Mann–Whitney U test for continuous data and with the chi-square test or Fisher's exact test for categorical data. To derive the result of correcting the interaction between factors influencing femoral approach success, logistic regression analysis was performed on the factors showing statistically significant differences between the two groups. The validity of the aortoceliac angle for prediction was estimated using receiver operating characteristic (ROC) curves, optimal cutoff values, area under the ROC curve (AUC), sensitivity, and specificity with 95% confidence intervals (CI).
Results
The success group consisted of 383 patients (318 men, 65 women; mean age = 56.4 ± 10.1 years), and the failure group consisted of 16 patients (11 men, 5 women; mean age = 55.6 ± 13.0 years). The subclavian approach succeeded in all patients in whom the femoral approach failed. Table 1 shows the distribution of age and anthropometric parameters between the success group and the failure group. The distribution of sex (P = 0.173) and age (P = 0.784) of the two groups were not significantly different. The success group was heavier than the failure group (P = 0.02). The mean aortoceliac angles of the success and failure groups were 61.9° ± 22.5° (range = 11.2°–136.0°) and 20.8° ± 11.8° (range = 8.4°–56.4°), respectively. There were statistically significant differences in the average aortoceliac angle between the two groups (P < 0.001). CT MPR images demonstrated ostial celiac stenosis in 18 patients in the success group. In the failure group, one patient had ostial celiac stenosis. Statistically significant differences in ostial celiac stenosis were not observed between the success group and failure group (P = 0.549). In the logistic regression analysis using weight, BMI, and aortoceliac angle, which were statistically significant factors that showed a significant difference between the two groups, femoral approach success was related only to the aortoceliac angle (P < 0.001, odds ratio = 0.817, 95% CI = 0.752–0.887) (Table 2).
Comparison of the femoral and subclavian approach groups.
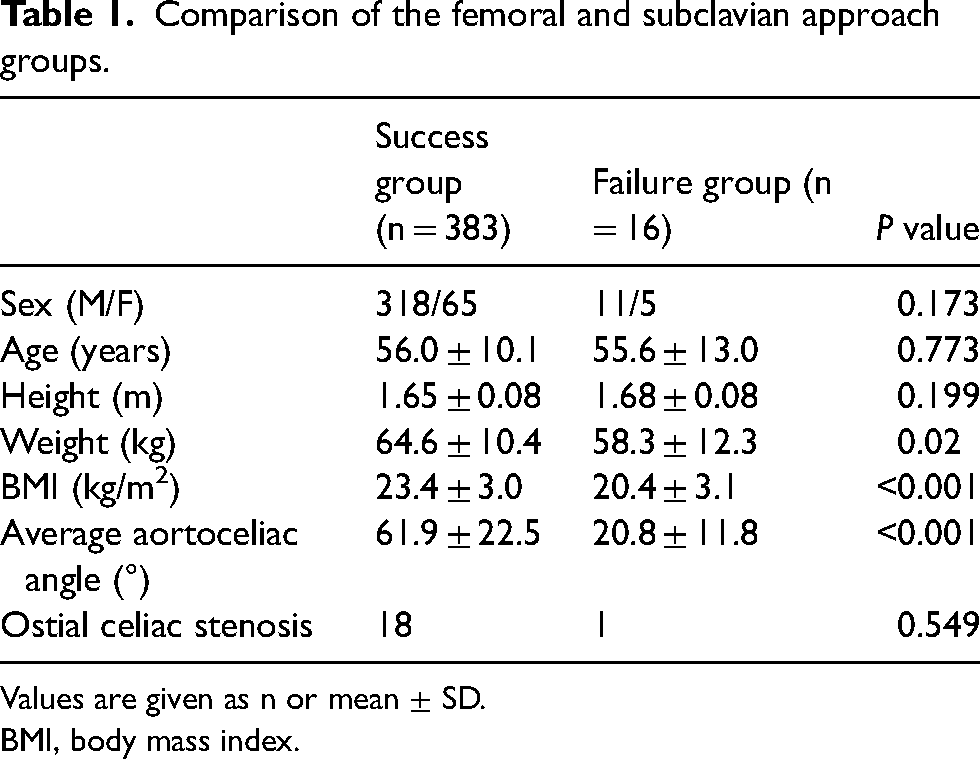
Values are given as n or mean ± SD.
BMI, body mass index.
Logistic regression analysis of predictors of femoral approach success.
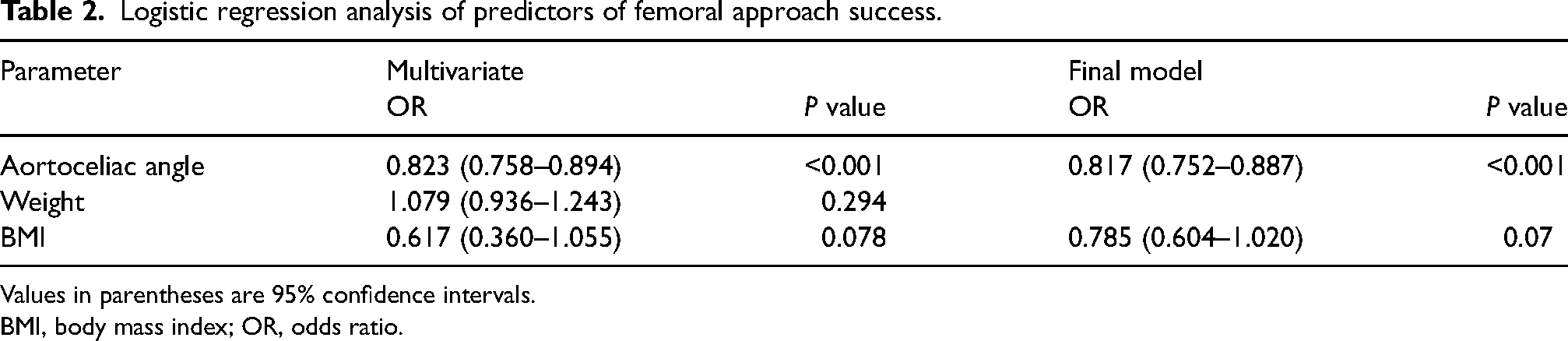
Values in parentheses are 95% confidence intervals.
BMI, body mass index; OR, odds ratio.
ROC curve analysis showed that the optimal cutoff point of the aortoceliac angle was 34.7° with a sensitivity of 91.1%, specificity of 93.7% (Fig. 3), and an AUC of 0.961.
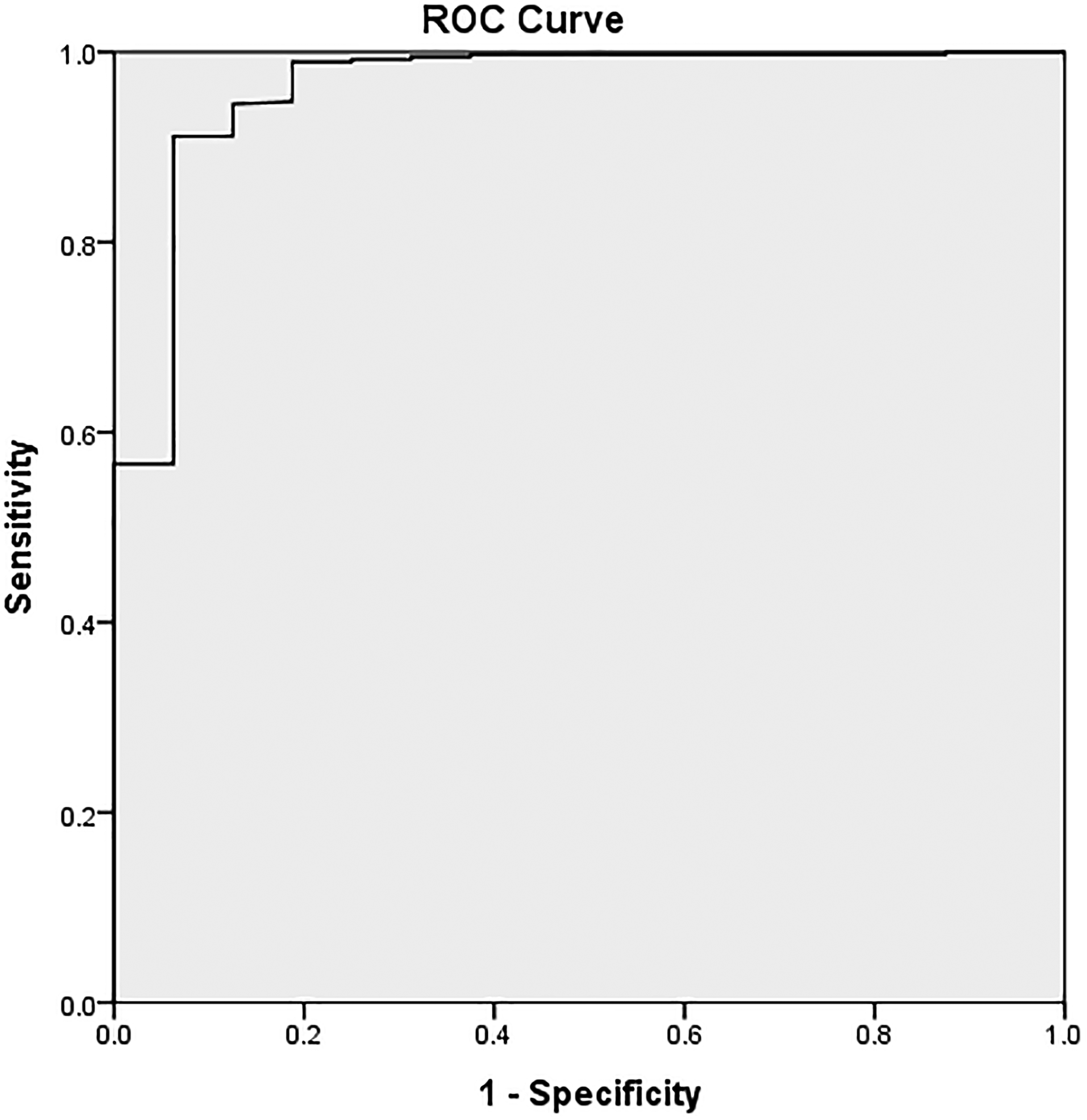
Receiver operating characteristic curve of aortoceliac angle for prediction of the need for a subclavian artery approach. The best cutoff point for the aortoceliac angle was 34.7°, with a sensitivity of 91.1%, specificity of 93.7%, and area under the curve of 0.961.
Discussion
This study was initiated to find factors affecting femoral approach because the procedure time was too long when the femoral approach failed during percutaneous implantation of a hepatic arterial infusion port-catheter system. In our experience, if the aortoceliac angle is small, the fixation of the catheter is difficult, which is statistically explained in this study.
HAIC using an arterial port system is theoretically more effective for HCC than systemic chemotherapy (3,4). HAIC allows a high concentration of anticancer drugs to be delivered locally to hypervascular tumors, thereby keeping systemic concentrations of chemotherapeutic agents low due to the first-pass effect (5). Many studies have reported that HAIC is a useful modality for patients with advanced HCC (3,5–9). HAIC is widely used in Asia, especially in Japan and the Republic of Korea (3,10).
When percutaneous implantation of a hepatic arterial infusion port-catheter system is performed, the left subclavian and femoral artery approaches are the most commonly used vascular access route (11). The femoral approach is technically easier than the left subclavian approach due to its superficial location and less tortuous anatomy, and it does not pose a risk of cerebral infarction, a serious complication of the subclavian approach. For this reason, several HAIC-related studies inserted ports using a femoral approach (5,8,14). In our hospital, a femoral approach was first attempted to prevent complications. However, in some patients, the femoral approach failed to fix the catheter despite several attempts, so a subclavian approach was then used. It is very important that the indwelling catheter be well maintained in the gastroduodenal artery during implantation of a port-catheter system for HAIC. If the catheter is not fixed to the gastroduodenal artery, the port-catheter system may dislodge after the procedure. If patients who are poor candidates for a femoral approach can be identified before the procedure, procedure time and radiation exposure can be reduced. However, the cause of femoral approach failure was poorly understood, so this study was conducted to explore the issue. In this study, the average aortoceliac angle in the failure group was significantly more acute than in the success group (P < 0.001). And in the logistic regression analysis, the aortoceliac angle was significantly associated with femoral approach success.
Therefore, the acute aortoceliac angle can be considered a major cause of technical failure in the implantation of port-catheter systems via a femoral approach.
Despite its several disadvantages, the subclavian approach should be considered in patients with an acute aortoceliac angle. It is important to review CT or MR images and choose an appropriate approach before the procedure. In response to this study, our institution's protocol was revised to the initial use of the subclavian approach in patients with an aortoceliac angle of <30°.
The main limitation of this study is the small number of patients in the failure group. Larger studies may provide a more accurate aortoceliac angle cutoff value for approach selection.
In conclusion, for patients with acute aortoceliac angle undergoing port-catheter system implantation for HAIC, the femoral approach is likely to fail. A left subclavian artery approach should be preferentially considered in these patients for stable fixation of the catheter tip to the gastroduodenal artery.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.