
Abstract
Background
Ultrasound-guided percutaneous thermal ablation has become an alternative treatment for small hepatocellular carcinoma (HCC). Recent evidence suggests that fusion imaging (FI) may improve the feasibility and efficacy of thermal ablation for HCC, while the clinical evidence remains limited.
Purpose
To compare FI versus ultrasound-guided thermal ablation for HCC.
Material and Methods
Relevant cohort or randomized controlled trials were found by searching Medline, Web of Science, Cochrane Library, and Embase. The pooling of results was performed using a random-effects model incorporating heterogeneity.
Results
In this meta-analysis, 15 studies involving 1472 patients (1831 tumors) for FI-guided ablation and 1380 patients (1864 tumors) for ultrasound-guided ablation were included. Pooled results showed that compared to conventional HCC ablation guided by ultrasound, the FI-guided procedure showed a similar technique efficacy rate (risk ratio [RR] = 1.01, 95% confidence interval [CI] = 1.00–1.02, P = 0.25; I2 = 30%). However, FI-guided tumor ablation was associated with a lower incidence of overall complications (RR = 0.70, 95% CI = 0.50–0.97, P = 0.03; I2 = 0%). Moreover, patients receiving FI-guided tumor ablation had a lower risk of local tumor progression during follow-up than those with ultrasound-guided ablation (RR = 0.61, 95% CI = 0.47–0.78, P < 0.001; I2 = 13%). Subgroup analysis according to FI strategy, imaging techniques in controls, and tumor diameter showed consistent results (p for subgroup difference all >0.05).
Conclusion
FI-guided thermal ablation may be more effective and safer than ultrasound-guided ablation for patients with HCC.
Introduction
For early hepatocellular carcinomas (HCC), percutaneous thermal ablation is widely accepted as an effective and mini-invasive treatment (1). Technically, percutaneous thermal ablation includes radiofrequency ablation (RFA) and microwave ablation (MWA) (2). For HCC with diameters <3 cm, percutaneous thermal ablation has been shown to confer similar therapeutic efficacy to surgical resection (3,4). During the procedure of percutaneous thermal ablation for HCC, ultrasound is the conventionally preferred real-time imaging modality to guide the needling position, track tumor lesions during hepatic, respiratory movement, and avoid the injury of vital organs (5). Moreover, optimized ultrasound guidance is necessary to confirm the immediate efficacy of the treatment and reduce the incidence of local tumor progression (LTP) during follow-up (6,7). However, not all HCC lesions were with adequate visibility on conventional ultrasound, such as those with small size (diameter <2 cm), with the isoechoic feature, or in difficult locations within the body (8,9). Although contrast-enhanced ultrasound (CEUS) has been suggested to overcome some shortcomings of conventional ultrasound in guiding the ablation of HCC for tumors with inadequate blood supply, the application of CEUS was restricted (10).
With the development of digital and three-dimensional (3D) imaging techniques in recent years, fusion imaging (FI) has emerged as a more accurate and efficient tool to support mini-invasive procedures, including percutaneous ablation for HCC lesions (11,12). By combining real-time ultrasound or CEUS images with high-resolution images, such as computed tomography (CT), magnetic resonance imaging (MRI), or 3D ultrasound (3DUS), FI has been suggested to confer more efficiencies than conventional ultrasound in visualizing the target lesion, determining the ablation edge, and evaluating the therapeutic efficacy of percutaneous ablation for HCC (13–15). However, the clinical evidence of the potential superiority of FI-guided thermal ablation to ultrasound-guided ablation remains limited. A few head-to-head comparative studies have been performed. However, these studies have limited sample sizes, and a summarized study with meta-analysis is needed (16–30). Accordingly, we performed a systematic review and meta-analysis in this study to compare the efficacy and safety of FI versus ultrasound-guided thermal ablation for HCC.
Material and Methods
This study adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 2020) guideline (31,32) and the Cochrane Handbook for Systematic Reviews and Meta-analyses (Handbook for Systematic Reviews and Meta-analysis) (33). Approval from the Institutional Review Board was not required as this is a meta-analysis.
Literature search
We obtained studies by searching several databases including Medline, Web of Science, Cochrane Library, and Embase with a combined keyword strategy: (i) “hepatocellular” OR “liver” OR “hepatic”; (ii) “carcinoma” OR “cancer” OR “tumor” OR “malignancy” OR “malignant” OR “neoplasm”; (iii) “ablation” OR “radiofrequency” OR “thermal ablation” OR “microwave ablation” OR “RFA”; and (iv) “fusion” OR “fusion imaging.” The included studies were published in English and involved human particiants. To complement this process, we hand-screened the citations of the related original and review articles. Literature searches were last conducted on 30 December 2022.
Selection of studies
The PICOS criteria were used for study inclusion.
P (patients): patients with a confirmed diagnosis of HCC who were planned to receive percutaneous thermal ablation;
I (intervention or exposure): ablation guided by FI, including CT/MRI or 3DUS fusion with ultrasound;
C (control): ablation guided by conventional ultrasound or CEUS;
O (outcomes): reported at least one of the following outcomes, which included the technique efficacy rate (TER), incidence of complications, and risk of LTP during follow-up. This study defined technique effectiveness as the complete destruction of the macroscopic tumor as determined by imaging immediately after the procedure (4). Complications were defined according to the criteria of the original studies. In addition, LTP was defined as an incompletely treated tumor that continues to grow or a new tumor (or satellite tumors) that grows at the original site (34).
S (study design): cohort studies or randomized controlled trials (RCTs) published as full-length articles in peer-reviewed journals.
The following studies were excluded: preclinical studies; review articles; editorials; meta-analyses; studies that did not include patients with HCC; studies without an intervention of FI-guided thermal ablation; studies without a control ultrasound-guided ablation; and studies that did not report any of the above outcomes. Studies with the largest sample sizes were included in the meta-analysis if multiple studies with overlapped patients were retrieved.
Data collection and study quality assessment
Two independent authors searched, collected, and assessed the data. Discussions with the corresponding author were used to resolve disagreements. The data collected were as follows: (i) author, year, location, and study design; (ii) participant characteristics, such as diagnosis, patient number, tumor number, mean age, sex, and mean diameters of the tumors; (iii) details of intervention and control procedures; (iv) variables adjusted or matched between groups; and (v) follow-up durations and outcomes reported. An assessment of study quality was conducted according to the Newcastle-Ottawa Scale (NOS) (35). Based on this scale, each study was rated using three broad criteria: selection of the study groups; the comparability of the groups; and the ascertainment of the outcome of interest. The total score was in the range of 1–9, and a higher score indicated better study quality. The Cochrane Risk of Bias Tool was used to determine the quality of the included RCTs (33) according to the following aspects: assigning random sequences; concealing allocations; blinding participants and personnel; blinding outcomes assessors; incomplete outcomes data; and selective outcome reporting.
Statistical methods
In the present study, the outcome of categorized variables was presented as risk ratio (RR) and 95% confidence interval (CI) (36). An evaluation of the extent of heterogeneity between studies was conducted by performing Cochrane's Q test and estimating the I2 statistic, as explained previously (36,37). An I2 > 50% indicates heterogeneity. The results were pooled using a random-effects model that considered possible between-study heterogeneity (33). For studies including multiple intervention groups of different strategies for FI (e.g. CT/MRI-US and 3DUS-US), the control groups with ultrasound-guided ablation were equally split and included as independent comparisons to overcome a unit-of-analysis error, according to the instruction of Cochrane's Handbook (33). Whenever possible, predefined subgroup analyses were performed according to the different strategies for FI, ultrasound techniques in control (ultrasound or CEUS), and mean diameters of the tumors. A median of the continuous variable was selected as a cutoff for defining subgroups. To determine whether publication bias exists, funnel plots were constructed and visually examined for symmetry (38). In addition, for the purpose of testing for publication bias, Egger's regression analysis was conducted (38). RevMan (version 5.1; Cochrane Collaboration, Oxford, UK) and Stata were used for the statistical analysis. P < 0.05 indicates statistical significance.
Results
Study retrieval
As shown in Fig. 1, after a search of electronic databases, 675 articles were retrieved, and 544 remained after duplications were removed. Among the 544 titles and abstracts screened for the meta-analysis, 491 were excluded due to their non-compliance with the criteria of the meta-analysis. Of the remaining 53 studies, 38 were subsequently excluded due to the reasons listed in Fig. 1 after full texts were read by two authors independently. As a result, 15 studies were enrolled in the meta-analysis (16–30).
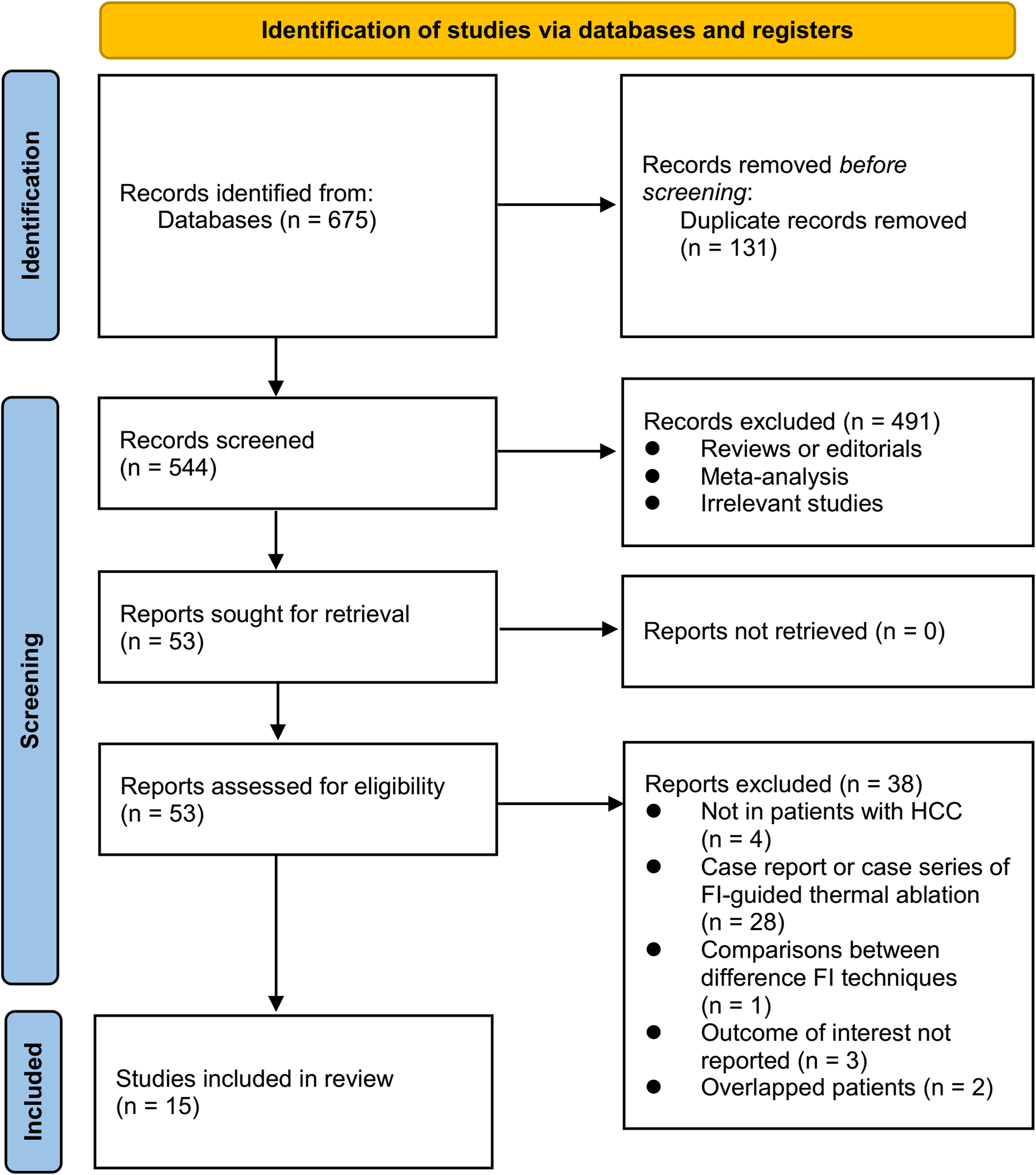
Diagram illustrating the process of searching databases and identifying studies.
Study characteristics
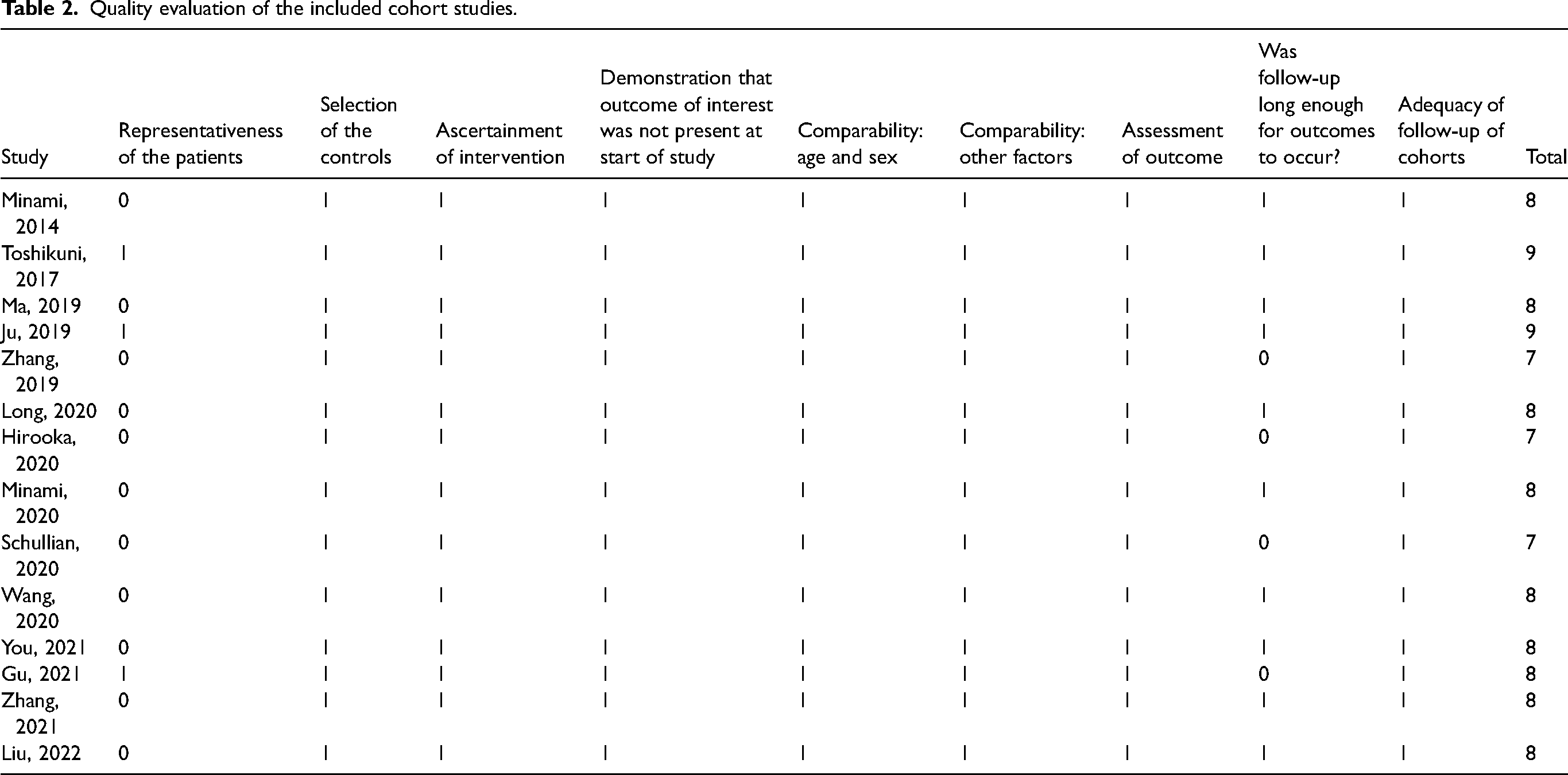
Table 1 summarizes the characteristics of the studies included in the meta-analysis. Overall, one RCT (18), three prospective cohort studies (17,19,27), and 11 retrospective cohort studies (16,20–26,28–30) were available. Since one study included two comparisons of different FI techniques with ultrasound (CT/MR-CEUS vs. CEUS and 3DUS-CEUS vs. CEUS) (18), these datasets were included independently in the meta-analysis. Accordingly, 16 comparisons (datasets) were available for this meta-analysis, involving 1472 patients (1831 tumors) for FI-guided ablation and 1380 patients (1864 tumors) for ultrasound-guided ablation. These studies were published between 2014 and 2022, and were performed in Japan, China, and Austria. All the studies included patients with HCC who were allocated to an intervention group of patients with FI-guided percutaneous thermal ablation and a control group of patients with ultrasound (conventional ultrasound or CEUS) guided ablation. The number of included patients was in the range of 28–839 in the included studies. The mean age of the included patients was in the range of 52–73 years. The mean diameter of the tumors was in the range of 14–41 mm. As for the ablation procedures, RFA was used in eight studies (16,17,22,24–28), MWA was used in one study (21), and RFA or MWA was used in the remaining six studies (18–20,23,29,30). The median follow-up durations were 8–66 months, and variables such as age, sex, Child-Pugh Score, etiology, tumor size, location, and so on were matched between patients with FI and ultrasound-guided ablation. For the cohort studies (16,17,19–30), the included studies received a NOS of 7–9 stars, which indicates good study quality (Table 2). For the RCT (18), the details of random sequence generation were reported, but not for the details of allocation concealment. The study was blinded to the outcome assessment but to the patient.
Characteristics of the included studies.
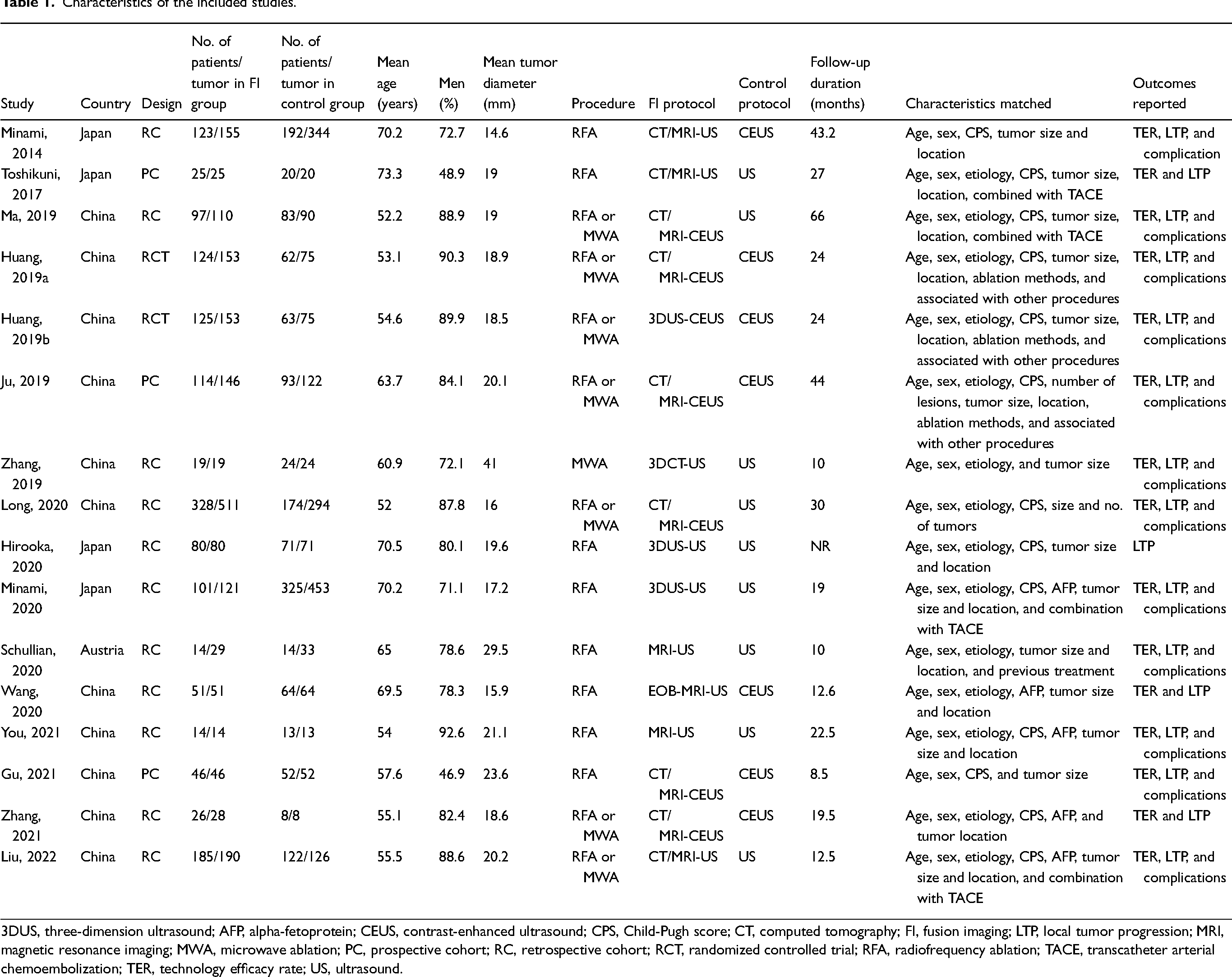
3DUS, three-dimension ultrasound; AFP, alpha-fetoprotein; CEUS, contrast-enhanced ultrasound; CPS, Child-Pugh score; CT, computed tomography; FI, fusion imaging; LTP, local tumor progression; MRI, magnetic resonance imaging; MWA, microwave ablation; PC, prospective cohort; RC, retrospective cohort; RCT, randomized controlled trial; RFA, radiofrequency ablation; TACE, transcatheter arterial chemoembolization; TER, technology efficacy rate; US, ultrasound.
Quality evaluation of the included cohort studies.
Meta-analysis results
Pooled results of 15 comparisons from 14 studies (16–21,23–30) indicated that compared to conventional HCC ablation guided by ultrasound, FI-guided procedure showed similar TER (RR = 1.01, 95% CI = 1.00–1.02, P = 0.25) (Fig. 2a) with mild heterogeneity (p for Cochrane's Q test = 0.13, I2 = 30%). Sensitivity analyses by excluding one dataset at a time showed consistent results (RR = 1.00 or 1.01, P all >0.05). However, evidence from 12 studies (16,18–25,27,28,30) showed that FI-guided tumor ablation was associated with a lower incidence of overall complications (RR = 0.70, 95% CI = 0.50–0.97, P = 0.03) (Fig. 2b) with no significant heterogeneity (p for Cochrane's Q test = 0.62, I2 = 0%). Similarly, omitting one dataset also did not significantly change the results (RR = 0.65–0.77, P all <0.05). Moreover, a meta-analysis with 14 studies suggested that patients receiving FI-guided tumor ablation had a lower risk of LTR during follow-up compared to those with ultrasound-guided ablation (RR = 0.61, 95% CI = 0.47–0.78, P < 0.001) (Fig. 2c) with mild heterogeneity (p = 0.31, I2 = 13%). The results were consistent for sensitivity analysis by excluding one dataset sequentially (RR = 0.56–0.66, P all <0.05). Subgroup analysis according to the difference of FI strategy, imaging techniques in controls, and tumor diameter showed consistent results for the meta-analyses of TER, the incidence of complications, and the risk of LTP during follow-up (P for subgroup difference all >0.05) (Table 3).
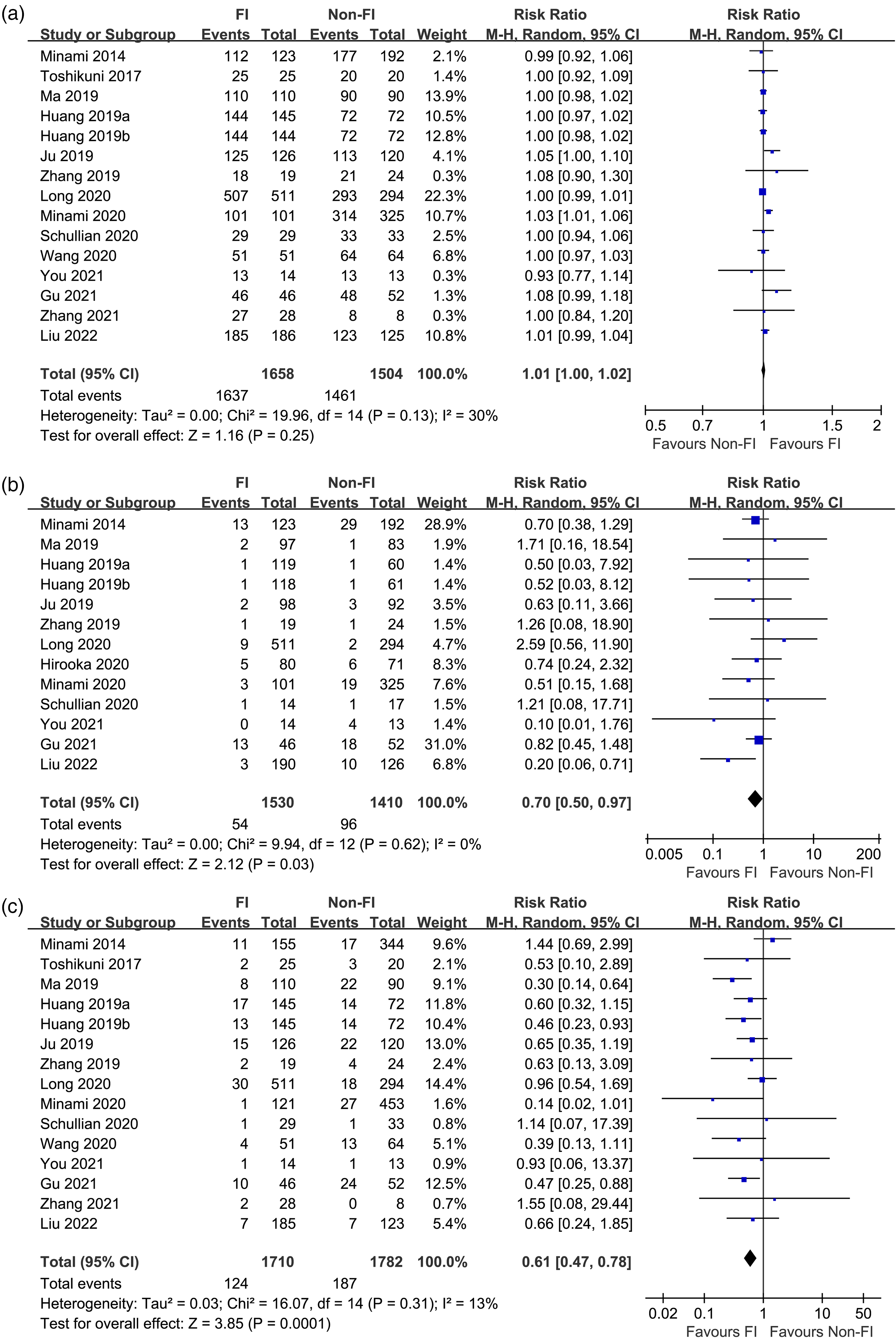
Forest plots comparing the feasibility, safety, and efficacy of FI versus ultrasound-guided percutaneous thermal ablation for HCC: (a) forest plots for the meta-analysis of TER; (b) forest plots for the meta-analysis of the incidence of complications; and (c) forest plots for the meta-analysis of the risk of LTP during the patients’ follow-up. FI, fusion imaging; HCC, hepatocellular carcinoma; LTP, local tumor progression; TER, technique efficacy rate.
Subgroup analysis.
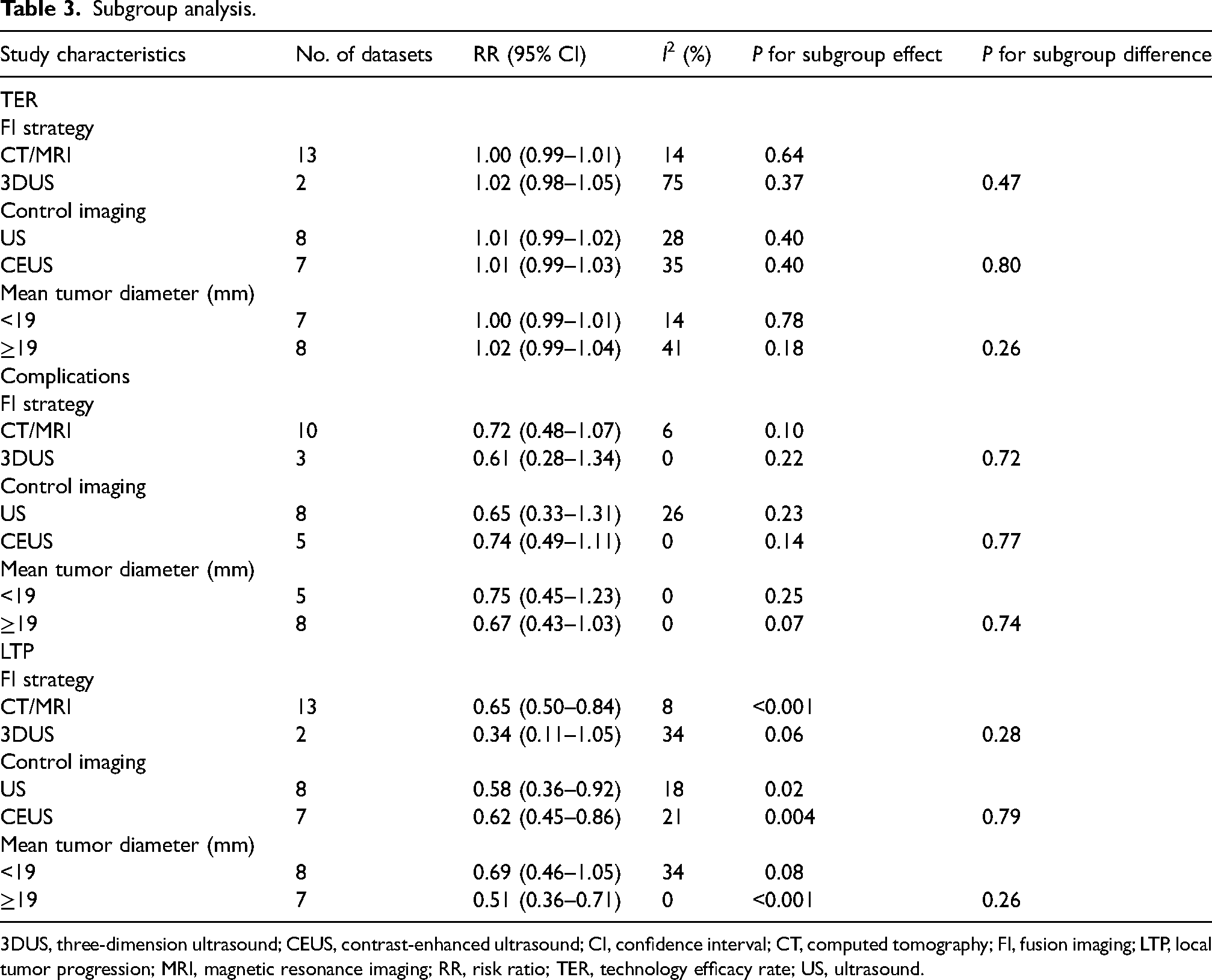
3DUS, three-dimension ultrasound; CEUS, contrast-enhanced ultrasound; CI, confidence interval; CT, computed tomography; FI, fusion imaging; LTP, local tumor progression; MRI, magnetic resonance imaging; RR, risk ratio; TER, technology efficacy rate; US, ultrasound.
Publication bias
The funnel plots for the meta-analyses of TER, the incidence of complications, and the risk of LTP during follow-up are shown in Figs. 3a–c. There are low publication bias risks based on the plots’ symmetry for these meta-analyses. Moreover, Egger's regression tests did not reveal any significant publication bias (P values all >0.10).
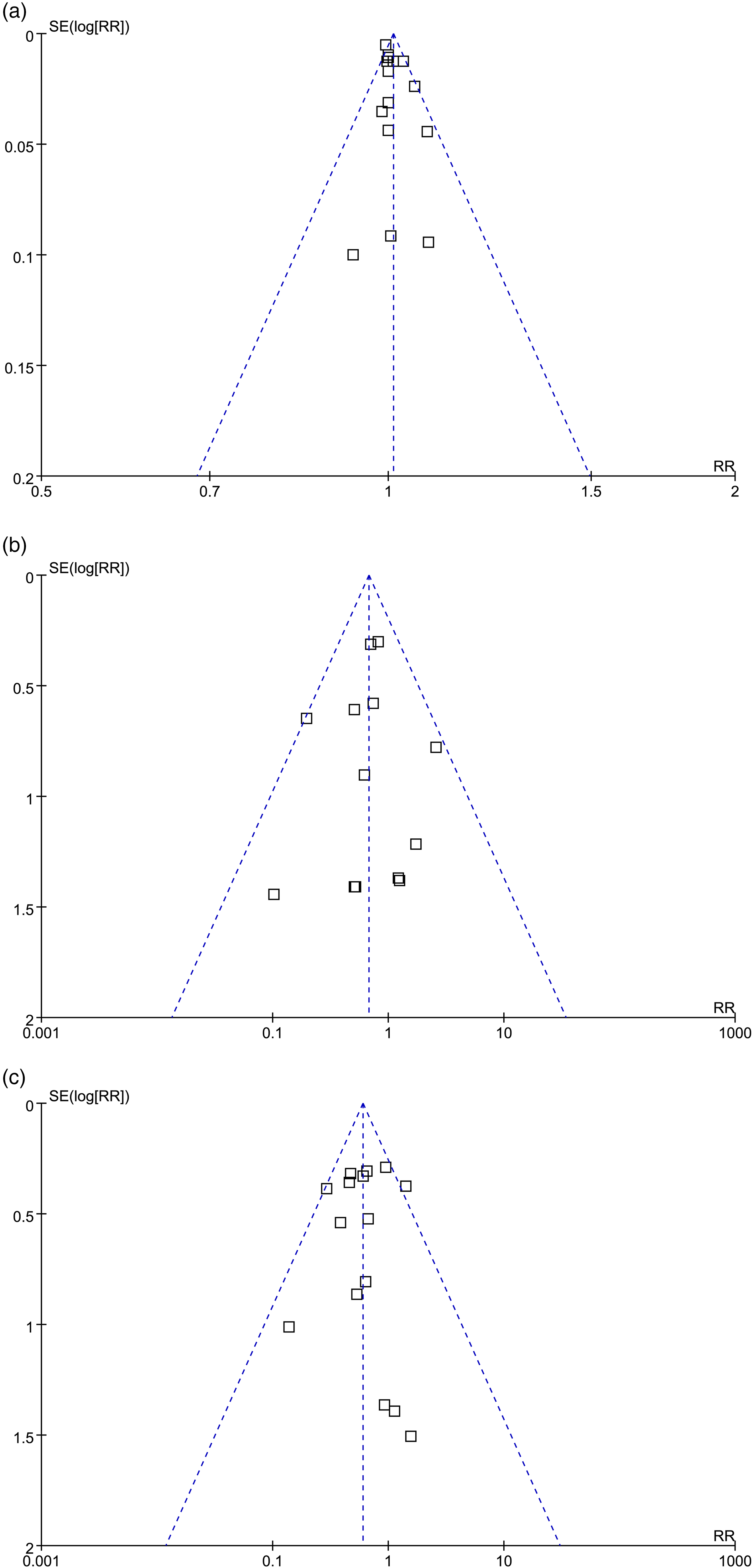
An analysis of the publication bias of the meta-analyses based on funnel plots: (a) funnel plots for the meta-analysis of TER; (b) funnel plots for the meta-analysis of the incidence of complications; and (c) funnel plots for the meta-analysis of the risk of LTP during follow-up of the patients. LTP, local tumor progression; TER, technique efficacy rate.
Discussion
In this systematic review and meta-analysis, we pooled the results of 15 available studies, and the results showed that compared to percutaneous thermal ablation guided with ultrasound or CEUS, FI-guided thermal ablation for HCC had a similar TER. However, FI-guided thermal ablation was associated with a lower incidence of complications and a reduced risk of LTP in patients with HCC during follow-up. The results were further validated in sensitivity analyses by excluding one study at a time and in subgroup analyses according to the different strategies in FI, control images, and mean diameter of the tumors. Taken together, although large-scale RCTs are needed to validate these findings, the results of the meta-analysis indicate that guided thermal ablation may be more effective and safer than ultrasound-guided ablation for patients with HCC.
To the best of our knowledge, only one previous meta-analysis evaluated the possible role of FI-guided RFA for patients with HCC (39). This meta-analysis included only six relevant studies published before April 2021, with a total of 1168 patients with HCC. Although this study showed a similar TER for FI and ultrasound-guided thermal ablation for HCC, it failed to indicate a superiority of FI-guided ablation to ultrasound-guided ablation (16–30). Compared to this previous meta-analysis, our study has several strengths in methodology. First, an extensive literature search was performed in four commonly used electronic databases, which retrieved 15 up-to-date, relevant studies. The overall sample size of this meta-analysis is much larger than the previous one (2852 vs. 1168), which may be adequate to achieve significant results for the differences in safety and efficacy between the two imaging-based ablation strategies. Second, although one of the studies was an RCT, the others were all cohort studies that matched the baseline characteristics between patients allocated to FI or ultrasound-guided procedures, thereby minimizing the potential confounding effects of these factors on the outcome. In addition, this meta-analysis summarized and reported three outcomes, which showed a reduced incidence of complications and a decreased risk of LTP in the FI-guided group despite similar TER, indicating the superiority of FI-guided ablation to ultrasound-guided ablation in safety and efficacy. Finally, multiple subgroup analyses showed that the results were consistent for CT/MRI and 3DUS based FI, in comparison to conventional ultrasound or CEUS-guided ablation and in studies with HCC tumor lesion <19 mm and ≥19 mm. These results further validated the robustness of the findings. Collectively, the results of the meta-analysis support the use of FI-guided thermal ablation for patients with HCC, particularly for those with difficult tumors under conventional ultrasound-guided ablation.
There are several potential advantages of FI compared to conventional ultrasound imaging as the guidance for percutaneous thermal ablation for HCC. First, by combining multiple imaging modalities with real-time ultrasound, FI could theoretically increase the visualizability of the HCC lesions, which have poor conspicuity on conventional ultrasonography. Early studies showed that FI based on CT/MRI-US could identify HCC lesions that had poor conspicuity on grayscale ultrasonography or CEUS, suggesting the benefits of FI in locating the HCC lesions and determining the position for needling (40,41). In addition, during the procedure, the use of CT/MR-US-based FI has been demonstrated to be feasible for evaluating RFA and enables intraoperative treatment evaluation by measuring the ablation margin accurately without needing contrast-enhanced CT (42). Accordingly, immediate evaluation of the therapeutic efficacy could be achieved by FI, and supplemental ablation sessions could be performed, if necessary, which may be an important reason for the reduced LTP following FI-guided ablation. In addition, by incorporating CT with contrast-enhance or 3DUS, FI could provide further imaging information regarding the relative locations of adjacent vital structures, which may be helpful in avoiding organ injury and severe complications during the ablation (34). Finally, in addition to increasing tumor detection, FI techniques improve the confidence of the operator as well as reduce operating time, which is also an important reason for the use of FI-guided ablation in patients with HCC (43). However, it has to be mentioned that FI is still in the development stage, and it has not been possible to perfectly resolve the inherent image distortion between ultrasound and CT/MR images. Efforts are needed to determine the optimized FI strategies for percutaneous ablation of HCC lesions.
The present study has some limitations. First, only one of the included studies was a RCT, and the others were all observational studies. We could not exclude the potential influences of the unmatched confounding factors on the outcome of the meta-analysis. Therefore, large-scale RCTs are needed to validate the findings of the meta-analysis. Moreover, studies were performed mostly in China and Japan. Studies from other countries are needed to confirm these results. Finally, as mentioned previously, the optimal FI strategy for guiding the thermal ablation of HCC remains to be developed in future studies.
In conclusion, the results of the meta-analysis demonstrate that FI-guided thermal ablation may be more effective and safer than ultrasound-guided ablation for patients with HCC. Although large-scale RCTs are needed to validate these findings and determine the long-term survival benefits of FI-guided ablation for patients with HCC, these findings support the use of FI as the guiding imaging for thermal ablation of HCC lesions.
Footnotes
Authors' note
Jiankui Luan is co-corresponding author and his information is stated as follows: Jiankui Luan, Department of Medical Imaging, Laizhou People's Hospital, 1718 Wuli Street, Laizhou City, PR China, Email: lzsszsjj@vip.163.com.
Availability of data
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding author.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Research project of Qingdao University Medical Group Co., Ltd. (grant number YLJT20222031).