
Abstract
Background
Some peripheral small cell lung cancers (pSCLCs) and benign lung tumors (pBLTs) have similar morphological features but different treatment and prognosis.
Purpose
To determine the significance of marginal vessels in differentiating pSCLCs and pBLTs.
Material and Methods
A total of 57 and 95 patients with pathological confirmed nodular (≤3 cm) pSCLC and pBLT with similar morphological features were enrolled in this study retrospectively. The patients' clinical characteristics and computed tomography (CT) features of tumors and marginal vessels (vessels connecting with tumors) were analyzed and compared.
Results
Compared with pBLTs, pSCLCs had a larger diameter (P = 0.001) but lower enhancement (P = 0.015) and fewer had calcification (P = 0.013). Compared with pBLTs, more lesions had proximal (70.2% vs. 22.1%) and distal (59.6% vs. 4.2%) marginal vessels in pSCLCs (each P < 0.0001). In addition, in pSCLCs, the numbers of proximal (1.3 ± 1.4 vs. 0.3 ± 0.6), distal (2.4 ± 3.1 vs. 0.1 ± 0.5), and total (3.6 ± 3.5 vs. 0.4 ± 1.0) marginal vessels were all more than those in pBLTs (each P < 0.001). Receiver operating characteristic curve analysis revealed the positive distal marginal vessel sign had the highest specificity (95.8%), and the number of total marginal vessels had the best performance in discriminating pSCLC from pBLT (cutoff value = 1.5, AUC = 0.80, 95% CI = 0.72–0.89, sensitivity = 70.2%, and specificity = 91.6%).
Conclusion
For peripheral solid nodules similar to pBLTs but without any calcification, the possibility of pSCLC should be considered if they have multiple marginal vessels (≥2), especially the distal ones.
Introduction
Lung cancer was the leading cause of global cancer death in 2020 (1). Among lung cancers, small cell lung cancer (SCLC) is the most common primary neuroendocrine malignancy and accounts for approximately 15% (2). It is characterized by rapid growth and greater propensity for early development of widespread metastases (3). Therefore, although SCLC is not very common in primary lung cancers, it contributes to the extremely poor prognosis. Patients with SCLC have a median overall survival (OS) time of 16 months (4) and the five-year OS rate is only 7% (5). Early diagnosis and treatment of SCLC are somewhat helpful for improving its survival rate (6,7), and computed tomography (CT) examination has been shown to be efficient for its early detection and diagnosis (8). The central SCLC usually has consistent CT features (9,10), while the diagnosis of the peripheral SCLC (pSCLC) has been a challenge.
On CT images, pSCLC is mainly characterized by solid nodules, which should be differentiated from non-small cell lung cancer, inflammatory lesion, and benign lung tumor (BLT). Previous studies revealed that the pSCLCs usually manifest as round or lobulated nodules with homogeneous density, smooth margin, and homogeneous enhancement, but without significant spiculation, pleural indentation, or internal necrosis (10–14). However, peripheral benign lung tumors (pBLTs), such as common sclerosing pneumocytomas and pulmonary hamartomas, also frequently showed similar features (15,16). Therefore, the CT findings of pSCLCs and pBLTs have many similarities, which lead to the former being easy to be misdiagnosed when they are first detected. In view of the significant differences in the treatment and prognosis of pSCLCs and pBLTs, it is necessary to further reveal their differences to improve diagnosis.
In our previous study, it was found that only sex, density homogeneity, bronchial cutoff, hilar lymph node enlargement, and emphysema were independent factors for differentiating pSCLCs and pBLTs (14). Except for these differences, both had a high degree of similarity in morphology. Thus, for those nodules without significant CT characteristics, further research is needed to reveal their differences, but there are no reports in this aspect so far. Peripheral SCLCs, as one type of peripheral lung cancer, usually originated from the bronchial mucosa and grew along the submucosa layers (10,17); it was easier to interrupt the lumen of bronchi. Meanwhile, the parallel pulmonary artery was stretched or encased by the tumor in the early stage but was interrupted as the tumor grew (18). Therefore, the pSCLC was closely related to the bronchovascular bundle, and the vessels around the nodules may provide clues for differentiating diagnosis.
In clinical practice, we have observed pSCLCs to frequently have vessels connecting with them on thin-section CT images, but this feature was rare for pBLTs. In view of the potential relationship between lesions and adjacent vessels, we hypothesized that the marginal vessels may provide additional information for further differentiating pSCLCs and pBLTs. The marginal vessels connected with nodules were thoroughly studied and compared, and the results may provide a new basis for the diagnosis and differential diagnosis of pSCLC.
Material and Methods
Patients
This study was approved by the Institutional Review Board of the First Affiliated Hospital of Chongqing Medical University. The requirement for informed consent was waived for this retrospective study. Between July 2012 and August 2021, patients with pSCLC and pBLT confirmed by pathological examination after operation or biopsy were consecutively enrolled in this study. All patients underwent chest CT examinations before operation or therapy. The inclusion criteria were as follows: (i) the lesions were located in a subsegment or more distal area; and (ii) the lesion diameters were ≤3 cm. The exclusion criteria were as follows: (i) the lesions had typical benign calcification and/or fat component (19); (ii) the lesions had an irregular shape, spiculation, spinous process, pleural indentation, or significant hilar and/or mediastinal lymph node enlargement; (iii) there were other lesions around the nodules, and the features of vessels could not be well evaluated; and (iv) CT images were of poor quality and the features of nodules could not be well evaluated. Finally, 57 of 82 patients with pSCLCs and 95 of 115 patients with pBLTs were enrolled in the present study (Fig. 1). In the 95 pBLTs, there were 60 (63.2%) pulmonary hamartomas, 34 (35.8%) sclerosing pneumocytomas, and 1 (1.0%) pulmonary cavernous hemangioma.
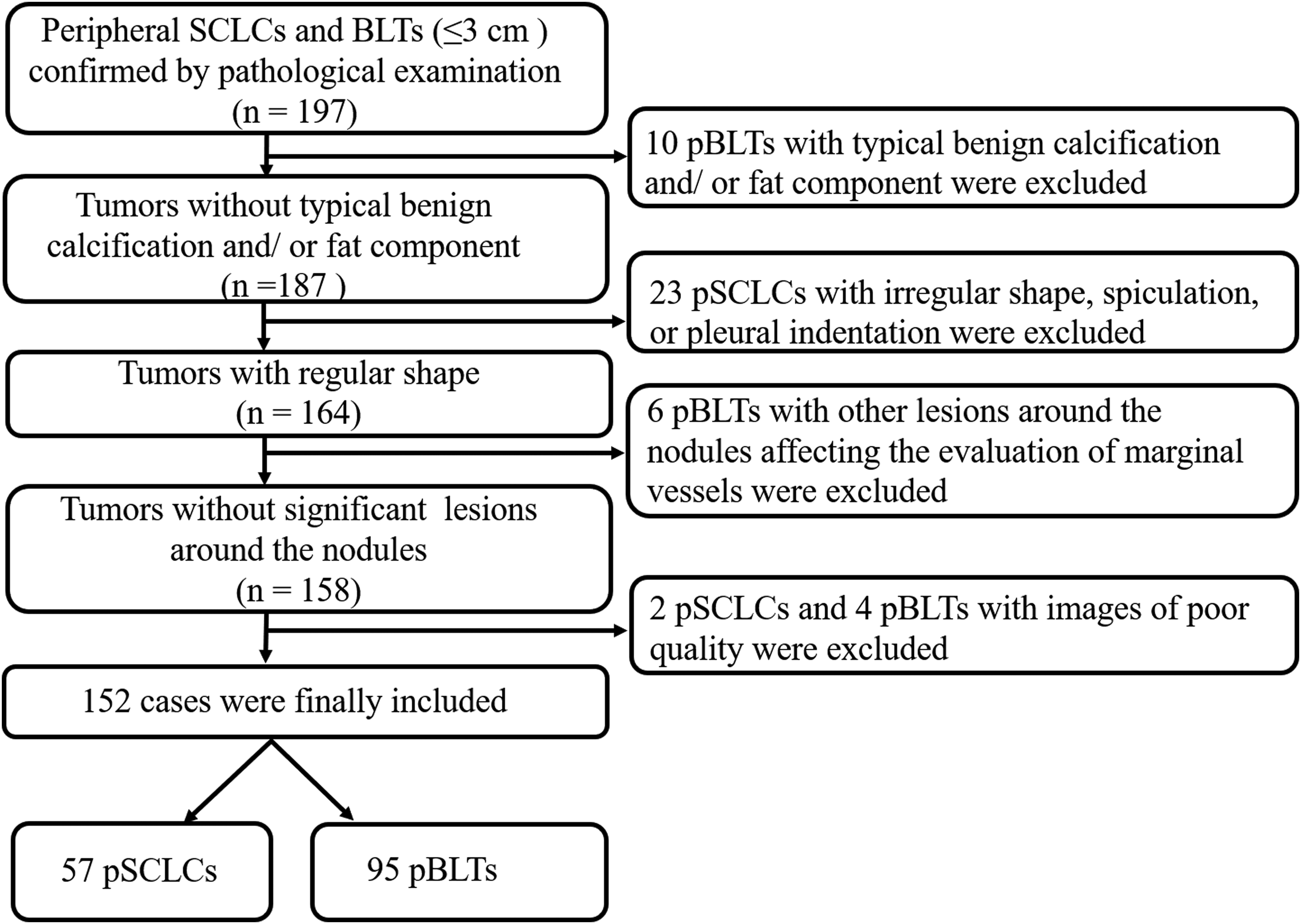
Flow chart of inclusion and exclusion criteria for eligible peripheral SCLCs and BLTs. BLT, benign lung tumor; SCLC, small cell lung cancer.
Clinical characteristics
The clinical data of all patients, including sex, age, and smoking history, were obtained in the electronic medical record system.
CT protocol
All patients were examined using one of the CT scanners (SOMATOM Definition Flash; Siemens Healthineers, Erlangen, Bavaria, Germany or Discovery CT750 HD; GE Healthcare, Milwaukee, WI, USA) with the following settings: tube voltage = 120 kVp; reference tube current = 40–100 mAs (using automatic tube current modulation techniques); rotation time = 0.5 s; pitch = 1.0; collimation = 0.6 mm; and reconstructed slice thickness and interval = 1 mm. Upon CT examination, patients were placed in the supine position with both hands near the head. Image acquisition was performed from the level of the thoracic inlet to a level inferior to the costophrenic angle. All patients underwent plain CT scanning and 110 patients (44 with pSCLCs and 66 with pBLTs) underwent contrast enhanced CT scans with a total of 80–100 mL of non-ionic iodinated contrast material (Iopamidol, 320 mg/mL; Shanghai Bracco Sine Pharmaceutical Co., Ltd., Shanghai, PR China) at an injection rate of 3.0 mL/s, followed by 50 mL of saline solution via a power injector. The automatic bolus tracking method was used to detect the ascending aorta with a threshold of 150 Hounsfield units (HU) followed by a delay of 6 s before scanning. Images were obtained with mediastinal (width = 350–450 Hounsfield units [HU]; level = 40–60 HU) and lung (width = 1200–1500 HU; level = -400–-600 HU) window settings.
Image analysis
CT data were independently reviewed on a picture archiving and communication system (PACS) workstation (Carestream Vue PACS Philips (China) Investment Co., Ltd, Shanghai, PR China). The presence of pSCLC and pBLT was determined by two radiologists (with 15 and 10 years of experience in chest CT, respectively) who were blinded to the clinical data and pathological results. Data analysis was mainly based on axial and multiplanar reconstruction (MPR) images, volume-rendering (VR) image as a supplement was used to confirm the results on two-dimensional images through three-dimensional display. In view of the natural high contrast between pulmonary vessels and lung tissue, the lung window (window width = 1500 HU, window level = −600 HU) of the plain chest scan or enhanced thin CT images were selected to observe and evaluate the vessels connected with the tumor. When the interpretations of the two radiologists differed, the discrepancies were resolved by consensus.
The following CT features of the tumors were evaluated: size (the mean of the longest diameter and the perpendicular diameter on axial CT images); lobulation (yes/no); density homogeneity (yes/no); calcification (yes/no); ΔCT value (peak CT value on contrast-enhanced CT scan – CT value on plain CT scan); and numbers of proximal, distal, and total vessels connected with tumor. The positive marginal vessel sign indicates there are proximal and/or distal blood vessels connected with the tumor. The proximal marginal vessels refer to the vessels that connect with the nodule on its hilum side and are cut off by tumor; only their proximal segments can be seen. The distal marginal vessels refer to the vessels that connect with the nodule on its pleura side; only their distal segments can be seen (Fig. 2).

Illustration of marginal vessels. (a) There are multiple vessels around the tumor (T), a vessel (a) on the hilum (H) side is cut off by the tumor and only its proximal segment can be displayed, which is seen as the proximal marginal vessel; (b, c) two vessels connect with the tumor on its pleura side, only their distal segment can be displayed, which are seen as the distal marginal vessels. For those vessels, only their (d) ending or (e) edge connect with the tumor, they are not seen as marginal vessels. (b) Axial and (c) volume-rendering images from the same patient show a tumor has one proximal marginal vessel (arrowhead) and multiple distal marginal vessels (arrows). (d) Volume-rendering image from another patient shows a tumor without any marginal vessel but two (arrows) running along its surface.
Statistical analysis
The patients’ clinical data and the CT features of tumors and number of marginal vessels were statistically analyzed with the software package SPSS version 22.0 (IBM Corp., Armonk, NY, USA). The intraclass correlation coefficient (ICC) was used to assess the inter-observer agreement of continuous variables, including the number of proximal and distal marginal vessels. Inter-observer agreement based on ICC was classified as poor (ICC < 0.50), moderate (0.50 ≤ ICC < 0.75), good (0.75 ≤ ICC < 0.90), or excellent (ICC ≥ 0.90) (20). Continuous variables were expressed as means ± standard deviations or median (range), and categorical variables were expressed as number and percentage. To compare the differences in the variables between different tumors, the independent t-test was used for patient ages, ΔCT value, and number of total marginal vessels; the Mann–Whitney U test was used for tumor size, and number of the proximal and distal marginal vessels; the Pearson chi-square test was used for sex, smoking history, and frequencies of tumor with positive marginal vessel sign. Receiver operating characteristic (ROC) analysis was performed to evaluate the performance of positive marginal vessel sign, proximal marginal vessel sign, and distal marginal vessel sign, and numbers of proximal, distal, and total marginal vessels in differentiating pSCLC from pBLT, respectively. The best cutoff value of the ROC curve was determined, respectively, where the Youden index reached the maximum value. A P value <0.05 was considered to be statistically significant.
Results
Patients’ clinical characteristics
The patients’ clinical characteristics are shown in Table 1. A total of 57 pSCLCs and 95 pBLTs were included in this study. Compared with patients with pBLTs, men (77.2% vs. 34.7%), smokers (71.9% vs. 24.2%), and older individuals (63.1 ± 8.2 years vs. 53.4 ± 10.5 years) were more common in cases with pSCLCs (each P < 0.0001).
Patients’ clinical characteristics.
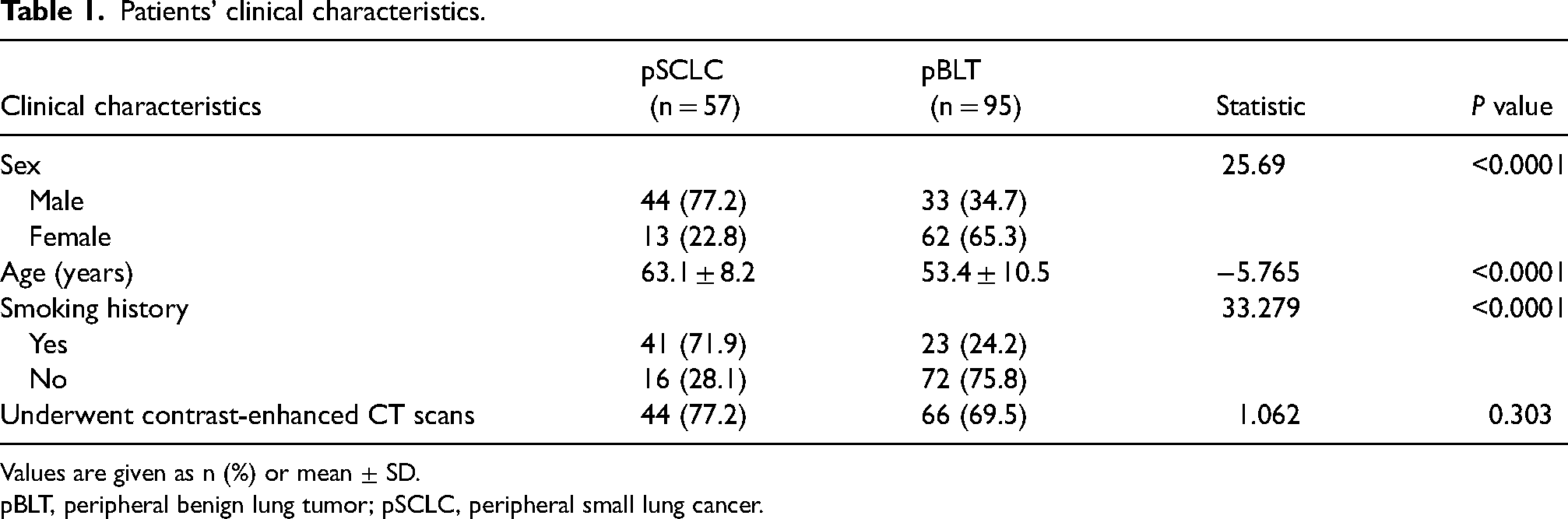
Values are given as n (%) or mean ± SD.
pBLT, peripheral benign lung tumor; pSCLC, peripheral small lung cancer.
Inter-observer agreement
The agreement was good for the number of proximal marginal vessels (ICC = 0.806, 95% CI = 0.732–0.859) and distal marginal vessels (ICC = 0 .826, 95% CI = 0.768–0.870).
Comparison of the CT features of tumors and their marginal vessels
The CT features of tumors and their marginal vessels are shown in Table 2. Compared with pBLTs, pSCLCs had a larger diameter (P = 0.001) but lower enhancement (P = 0.015), and fewer had calcification (P = 0.013). All the calcifications detected in pBLTs were single and spotted. In pSCLC, the proportions of tumors with positive marginal vessel sign, proximal marginal vessels, and distal marginal vessels were all significantly higher than those in pBLT (each P < 0.0001). In addition, in pSCLCs, the numbers of proximal, distal, and total marginal vessels were all higher than those in pBLTs (each P < 0.001) (Figs. 3 and 4). There were 17 (29.8%) cases of pSCLCs and 11 (11.6%) cases of pBLTs with marginal vessels composed of pulmonary veins (P = 0.005).
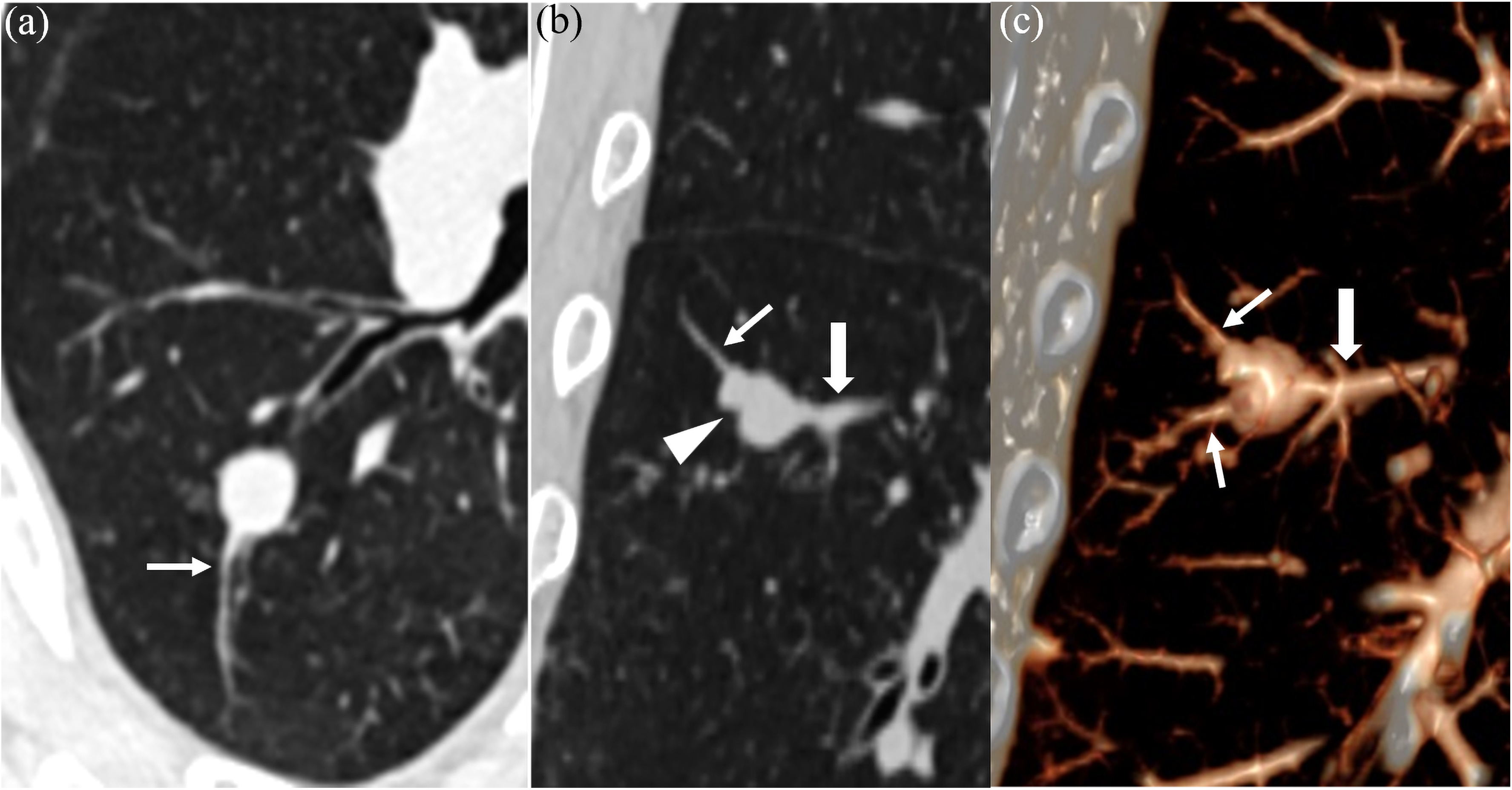
A 63-year-old man has a pSCLC with positive marginal vessel sign. (a) Axial, (b) coronal, and (c) volume-rendering images show an oval nodule with smooth margin, homogeneous density, and lobulation sign (arrowhead) has one proximal vessel (thick arrow) and two distal vessels (thin arrows) connecting it. pSCLC, peripheral small cell lung cancer.
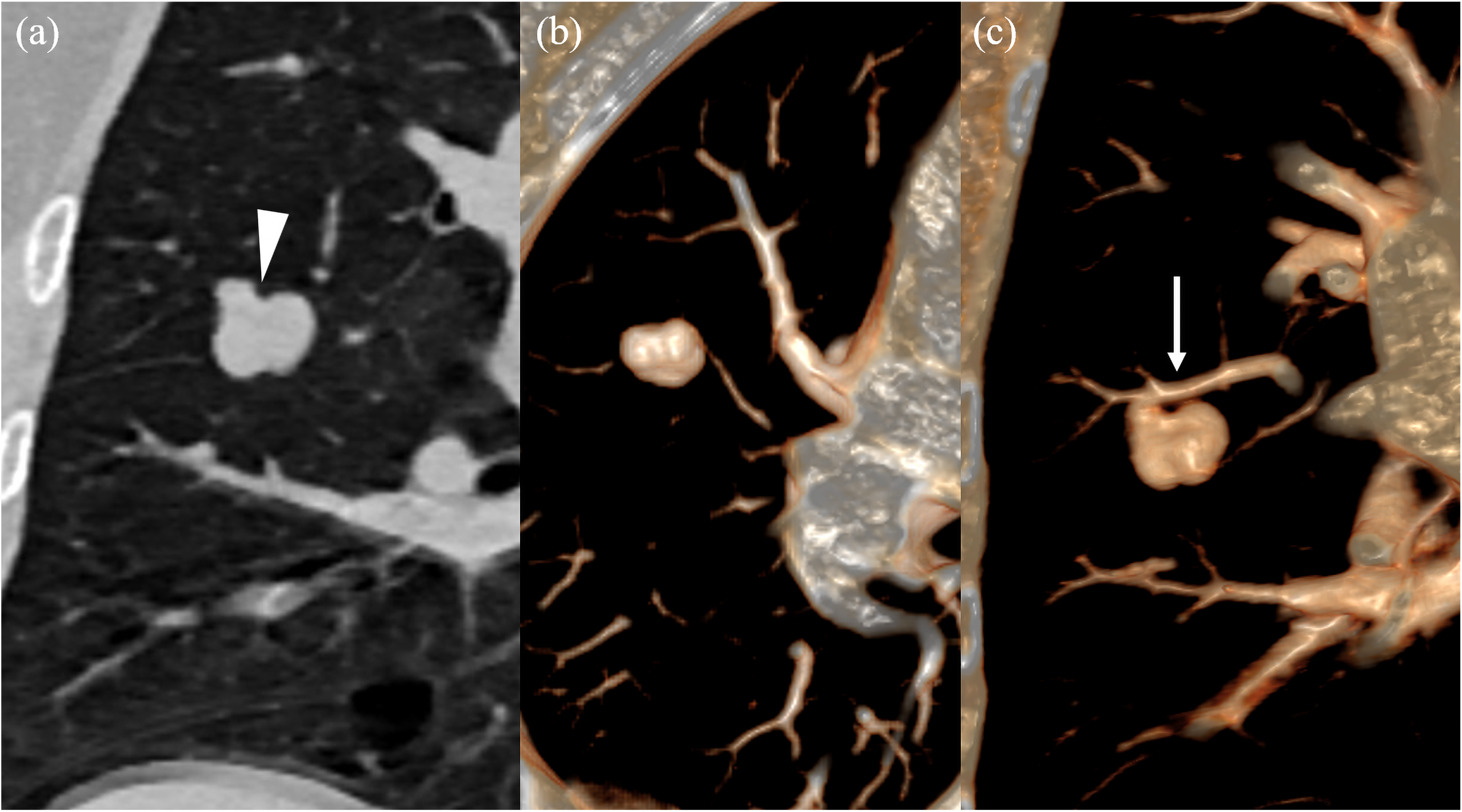
A 53-year-old woman has a pulmonary hamartoma without marginal vessel sign. (a) The coronal image shows a nodule in the right upper lobe with lobulation sign (arrowhead), smooth margin, and homogeneous density. (b, c) The volume-rendering images indicate there is no vessel connecting with (b) the nodule, but one (arrow) runs along (c) the nodule margin.
Comparison of the CT features and marginal vessels of tumors.
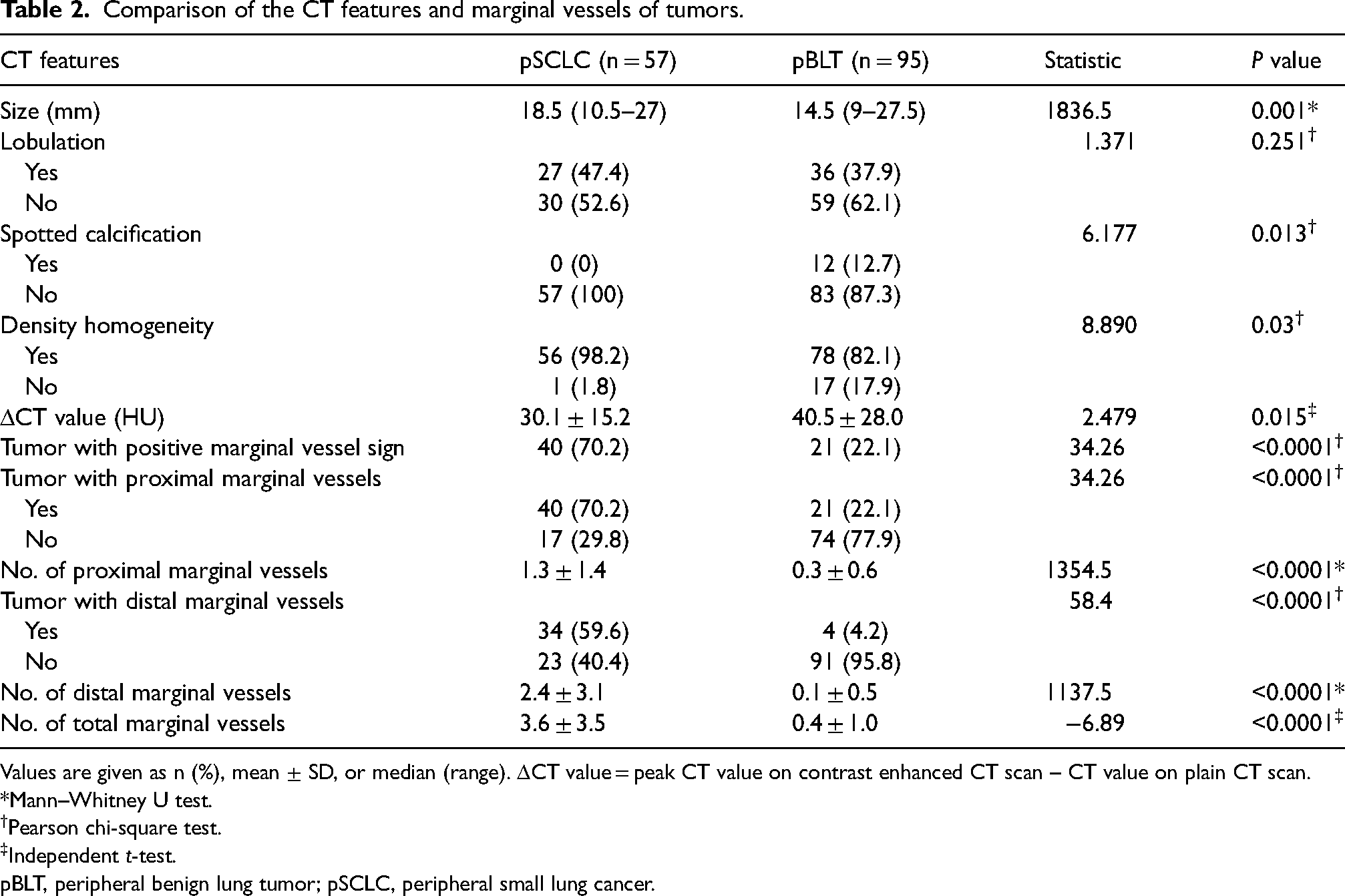
Values are given as n (%), mean ± SD, or median (range). ΔCT value = peak CT value on contrast enhanced CT scan – CT value on plain CT scan.
*Mann–Whitney U test.
Pearson chi-square test.
Independent t-test.
pBLT, peripheral benign lung tumor; pSCLC, peripheral small lung cancer.
ROC analysis was performed to evaluate the performance of positive marginal vessel sign, proximal marginal vessel sign, distal marginal vessel sign, and numbers of proximal, distal, and total marginal vessels in differentiating pSCLC from pBLT, respectively. The area under the curve (AUC), sensitivity, specificity, and the best cutoff value of ROC curves are shown in Table 3. It is revealed that the positive distal marginal vessel sign had the highest specificity (95.8%), and the number of total marginal vessels had the best performance in discriminating pSCLC from pBLT. The optimal cutoff value for number of total marginal vessels was 1.5, with an AUC of 0.80 (95% CI = 0.72–0.89, sensitivity = 70.2%, and specificity = 91.6%) (Fig. 5).
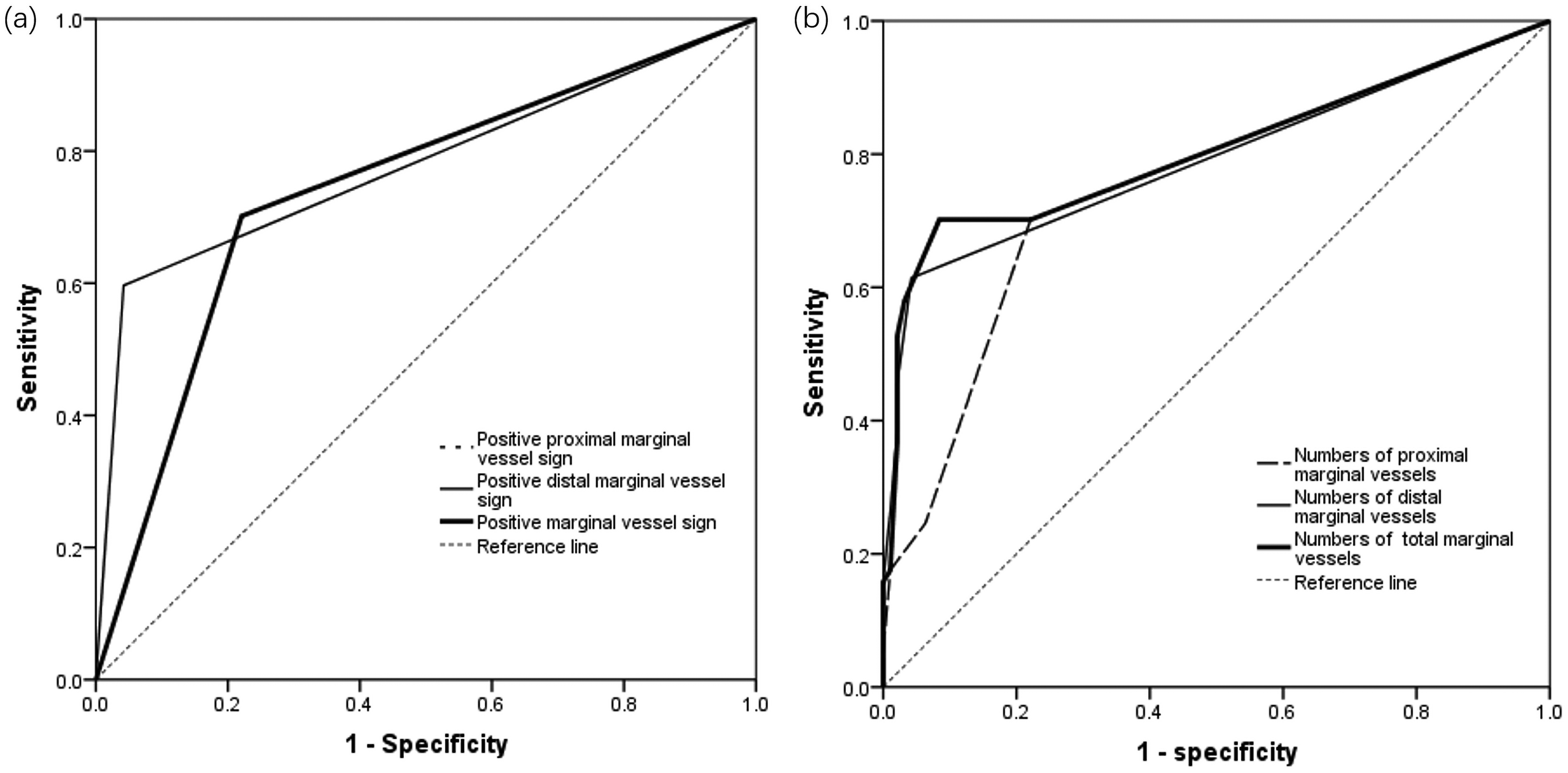
(a) ROC curves of the pSCLC predictive model established by the positive proximal (dotted line) and distal (thin solid line) marginal vessel sign, and positive marginal vessel sign (thick solid line), respectively. The dotted line and thick solid line are coincident. (b) ROC curves of the pSCLC predictive model established by the numbers of proximal (dotted line), distal (thin solid line), and total (thick solid line) marginal vessels, respectively. pSCLC, peripheral small cell lung cancer; ROC, receiver operating characteristic.
Performance of marginal vessel sign in differentiating pSCLC from pBLT.
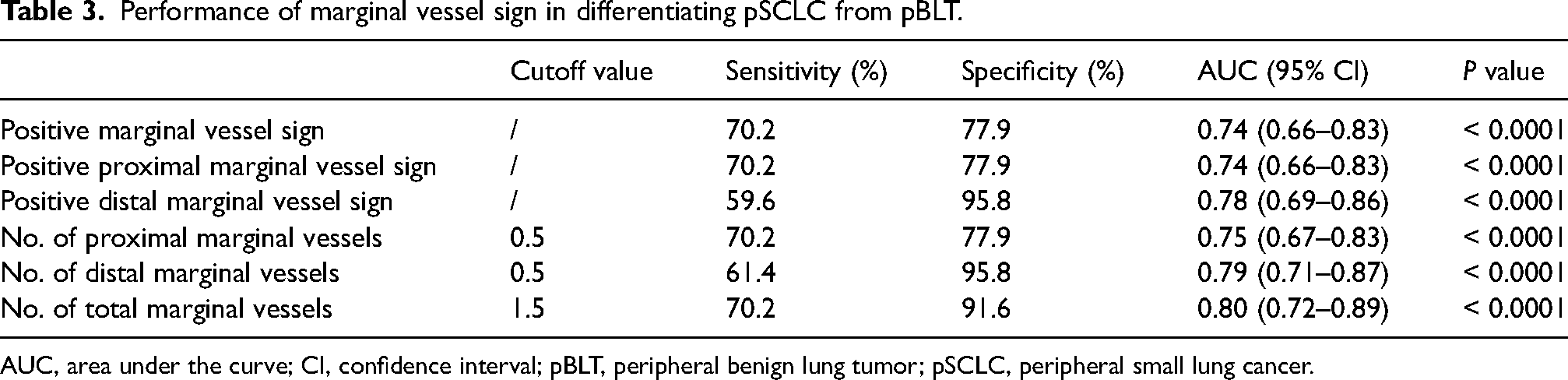
AUC, area under the curve; CI, confidence interval; pBLT, peripheral benign lung tumor; pSCLC, peripheral small lung cancer.
Discussion
When pSCLCs are small, their malignant signs, such as spiculation and pleural indentation, are not obvious due to the rapid growth. In this case, their CT manifestations are very similar to those of pBLTs. A previous study revealed that the number of vessels surrounding nodules could help to discriminate benign and malignant lesions; the lung cancers usually had more vessels surrounding them (21). In the present study, the proportion of nodules with a positive marginal vessel sign and the number of marginal vessels in pSCLCs were all significantly higher than those in pBLTs, which was consistent with the previous result. Thus, the marginal vessel of nodules could also be used as a potential indicator for differentiating pSCLC and pBLT with similar morphological features.
These significant differences of marginal vessel sign in pSCLCs and pBLTs may be closely related to the different origins of lesions. The SCLC usually originates from the bronchial mucosa and grows along the submucosa layers (10,17), and the pulmonary artery and bronchi are usually paralleled, thus the growth of pSCLC may affect not only the bronchi but also the paralleled pulmonary vessels. In contrast, the commonly detected sclerosing pneumocytoma are mainly composed of epithelial cells (type II pneumocytes) aligned in different directions and accompanied by proliferation and reaction of other components (22,23), and the hamartoma usually originates from mesenchyme (24). Thus, it can be seen that they do not directly originate from bronchi, so these lesions are less closely related to the surrounding vessels. However, in this study, 22.1% of pBLTs still had marginal vessels, especially the proximal ones, which may be due to the adjacent vessels being compressed and the border between them being unclear along with the tumor growth. ROC analysis suggests that evaluating the distal marginal vessel is more valuable for differentiating pSCLCs and pBLTs, while a positive proximal marginal vessel sign may not be an ideal indicator.
ROC analysis indicated that the number of total marginal vessels had a higher predictive value than that of proximal or distal ones in distinguishing pSCLC from pBLT; the best cutoff value was 1.5 with a higher specificity of 91.6%. It indicated that the number of total marginal vessels ≥2 favored the diagnosis of pSCLC over pBLT. This finding suggested the marginal vessel should be comprehensively evaluated for nodules without significant CT features. However, the sensitivity of total marginal vessels for predicting pSCLC was relatively low. The reason for this deficiency may be that some pSCLCs originate from distal bronchi (especially those located in the subpleural zone) so that the smaller marginal vessels cannot be easily detected and identified on CT images. Therefore, other CT features need to be considered for improving their diagnosis.
Lobulation sign was usually more common in lung malignancies; however, in the present study, it was not different between pSCLCs and pBLTs. It indicated that this sign was of limited value in differentiating them. Calcification was more frequently found in benign lesions (19), and the present results revealed that single spotted calcification was only detected in pBLTs. Thus, any calcification in the nodule may be an indicator of pBLTs rather than pSCLCs. However, the calcification only presented in some of pBLTs, and most pSCLCs and pBLTs cannot be differentiated by using this sign only. On enhanced images, the enhancement degree of pBLTs was higher than that of pSCLCs. This may be explained by the fact that the vascular bed of SCLC is composed of smaller vessels, so the tumor has less blood volume during the arterial phase (25); in addition, pathological findings indicate that necrosis is frequent and often extensive in SCLC (26). This feature should be considered in differentiating.
In addition to CT features, clinical features also need to be considered when differentiating them. Sclerosing pneumocytoma occurs predominantly in women (27), whereas pulmonary hamartoma is 2–3 times more common in men than in women (28). In the present study, men were more common among patients with pSCLC than among those with pBLT, while men accounted for 47.5% of the patients with pulmonary hamartoma. This discordance may be due to the small sample size. SCLC is known to be strongly associated with smoking history (29); the smokers among the patients with pSCLC were significantly more common than those among cases with pBLTs in the present study. In smokers, lung cancer could not be easily ruled out even though the nodules had a regular shape and smooth margin. However, regular nodules with a smooth margin were usually considered to be benign lesions in non-smokers. Therefore, regarding the nodules without significant CT features, marginal vessels should be carefully evaluated for determining the possibility of pSCLC, especially in the low-risk group.
The present study has some limitations. First, it was a retrospective study, and some bias may exist. Second, the sample sizes of pSCLCs were relatively small because only those with smaller size, regular shape, and smooth margin were selected. Third, because this was a retrospective study, some cases had no enhanced CT data; whether it could provide valuable information for the differential diagnosis should be verified in further studies. Fourth, in this study, the number and type of blood vessels connected with nodules were evaluated subjectively, thus discrepancy still existed even though MPR and VR images were used. Fifth, there was a selection bias in our study, because we only focused on the discrimination between pathologically confirmed pSCLCs and pBLTs, rather than pSCLCs and benign nodules; thus the results of the study cannot be directly used to distinguish pSCLCs from various benign nodules.
In conclusion, more pSCLCs have a marginal vessel sign and the pSCLCs have more marginal vessels compared with pBLTs. Thus, the tumor marginal vessel sign can be seen as a potential marker for differentiating pSCLC from pBLT with similar CT manifestations, and is a valuable supplement of the common morphological indicators. For peripheral solid nodules suspected of being pBLTs but without any calcification, the possibility of pSCLC should be considered if there are multiple marginal vessels (≥2), especially the distal ones, and the follow-up interval should be shortened, if necessary.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Joint Project Chongqing Science and Technology Commission and Chongqing Public Health Commission (grant number 2022MSXM050).