
Abstract
Background
Vestibular neuritis (VN) is a disorder manifesting as acute, isolated, spontaneous vertigo. There are few comprehensive studies on the changes in related functional and structural brain regions.
Purpose
To evaluate alterations in spontaneous neural activity, functional connectivity (FC), and gray matter volume (GMV) in patients with VN.
Material and Methods
A total of 24 patients with VN and 22 age- and sex-matched healthy controls underwent resting-state functional magnetic resonance imaging (rs-fMRI) and three-dimensional T1-weighted anatomical imaging. We calculated the amplitude of low frequency fluctuation (ALFF), regional homogeneity (ReHo), and degree centrality (DC) to discern local brain abnormalities. The most abnormal brain region was selected as the region of interest (ROI) for FC analysis based on ALFF and ReHo values after Bonferroni correction. Voxel-based morphometry (VBM) was used to assess differences in GMV.
Results
Patients with VN, compared to healthy controls, showed increased ALFF (P < 0.001), ReHo values (P = 0.002, <0.001), and DC (P = 0.013) in the left lingual gyrus and right postcentral gyrus. FC analysis demonstrated enhanced connectivity between the left lingual gyrus and the left superior frontal gyrus, and decreased connectivity with the right insula gyrus, right and left supramarginal gyrus (P = 0.012, 0.004, <0.001, 0.014). In addition, GMV was reduced in the bilateral caudate (P = 0.022, 0.014).
Conclusions
Patients with VN exhibit abnormal spontaneous neural activity and changes in ALFF, ReHo, DC, GMV, and FC. Understanding these functional and structural brain abnormalities may elucidate the underlying mechanisms of VN.
Keywords
Introduction
Vestibular neuritis (VN) is a condition characterized by acute, prolonged vertigo. It is the second leading cause of peripheral vestibular vertigo, being benign paroxysmal positioning vertigo (BPPV) (1,2). Patients with VN predominantly present with spontaneous vertigo and often experience severe nausea, vomiting, and unsteadiness. These symptoms can last anywhere from a few hours to several days. Simultaneously, patients with VN frequently demonstrate spontaneous nystagmus, both horizontal and rotary (3). The etiology of VN is believed to be either viral or vascular ischemic in origin, with recent studies indicating a preference for the former, i.e. the reactivation of latent type 1 herpes simplex virus (4). Despite some advancements in understanding the clinical features and etiology of VN, the related changes and mechanisms of brain function remain unclear.
In recent years, with the advances in neuroimaging techniques, related research has been gradually applied to patients with VN (1). Magnetic resonance imaging (MRI), due to the high image resolution, fine tissue contrast as well as multi-functionalities, has been widely applied to diagnose VN (5,6). Based on high-resolution MRI measurements of the internal auditory canal, a previous study identified superior vestibular nerve (SVN) atrophy and a smaller ratio of SVN/inferior vestibular nerve on the symptomatic side (5). Helmchen et al. (7) demonstrated decreased functional connectivity (FC) of the intraparietal sulcus near the supramarginal gyrus on the contralateral side of the lesion in the acute stage. Despite some progress in the clinical and imaging features of VN, few studies have systematically investigated the related changes in functional and structural brain regions.
The application of resting-state functional MRI (rs-fMRI) and voxel-based morphometry (VBM) in VN provides new research approaches to investigate the altered structural and functional alterations of the brain regions. The rs-fMRI has advantages due to its ease in signal acquisition and proficiency in identifying the functional areas in different populations (8), and spontaneous low-frequency fluctuations can be measured through blood oxygen level-dependent (BOLD) signals (9). Currently, several methods, such as amplitude of low frequency fluctuation (ALFF), regional homogeneity (ReHo), and degree centrality (DC), have been proposed to characterize the local dynamics of the rs-fMRI signal. For the voxel level, the present study considered that the ALFF, ReHo, and DC voxelwise metrics parameters represent a progressive relationship: ALFF describes the activity intensity of a single voxel; ReHo reveals the relationship of this voxel among the nearest voxels; and DC portrays the importance of this voxel in the whole-brain voxel (10). Previous research on rs-fMRI revealed local brain abnormalities in patients who had a transient ischemic attack. This was done using three local metrics: ALFF, ReHo, and DC (10). Seed-based FC analysis is a model-based method that depends on the proper selection of a seed or region of interest (ROI) and reveals a linear correlation between the selected seed region and whole-brain voxels (8,11,12). Li et al. confirmed decreased ALFF and ReHo values in the right precuneus and cuneus in patients with postural perceptual dizziness (PPPD). After ALFF analysis, abnormal regions were selected as seeds to further explore changes showing decreased FC between the precuneus, cuneus, and left precentral gyrus (13). In addition, the major advantages of rs-fMRI studies indicate their suitability for the investigation of acute VN, because it does not require a task to be carried out by the patients. Several studies have utilized rs-fMRI to investigate patients with VN. These studies have highlighted the value of understanding the FC between different brain networks. Specifically, they explored the connectivity within resting-state networks, the interregional functional connectivity, and the brain responses of patients with chronic VN (7,14,15). Currently, related VBM studies have been gradually applied to peripheral vestibular deficits, such as BPPV, vestibular migraine (VM), persistent PPPD, and VN (16–20), and confirmed that the structural changes in gray matter volume (GMV) were related to functional compensation (21,22). However, whether local brain abnormalities in patients with VN differ from those in healthy controls (HCs) remains unknown, and previous studies did not systematically investigate the functional and structural brain abnormalities in patients with VN.
Therefore, the aim of the present study was to investigate the spontaneous functional abnormalities and structural difference changes in patients with VN using ALFF, ReHo, DC, seed-based FC, and VBM, which might yield meaningful insights into patients with VN and help to reveal the structural and functional mechanisms of this disease.
Material and Methods
Participants
This study was approved by our institutional ethics committee, and each patient provided written informed consent before the MRI procedures were conducted. Between May and December 2020, 30 patients with VN and 26 age- and sex-matched HCs without any history of neurological or psychiatric diseases were recruited. All patients with VN and HCs were right-handed. The patients with VN, who were in the acute phase, were evaluated by a clinical neurologist with 10 years of experience. Patients with BPPV, PPPD, VM, chronic dizziness, tumor-related neurological symptoms, epilepsy, or a history of psychiatric disease were excluded. MRI was further performed in all participants to exclude white matter hyperintensity, lacunes, focal lesions, cerebral ischemic stroke, and severe cerebral stenosis. MRI of the brain was performed when the patient had unprecedented symptoms or did not recover within 1 to 2 days using various examination sequences, such as rs-fMRI, three-dimensional (3D) T1 high-resolution imaging, T2-fluid attenuated inversion recovery, diffusion-weighted imaging, and magnetic resonance angiography. During MRI, we also excluded individuals who could not complete the entire examination or whose head motion was >2.0 mm. Finally, 24 patients with VN (8 men, 16 women; mean age = 45.0 ± 13.6 years; age range = 17–63 years; time in education = 6–23 years; mean time in education = 13.5 ± 4.9 years) and 22 HCs (5 men, 17 women; mean age = 44.1 ± 13.6 years; age range = 20–63 years; time in education = 7–22 years; mean time in education = 13.9 ± 5.2 years) were enrolled in the study.
MRI acquisition
All participants were examined with a 3.0-T MRI scanner (Signa EXCITE HDxt; GE Healthcare, Waukesha, WI, USA) with an eight-channel phase array head coil while maintaining a supine and head-first position. During image acquisition, all participants were instructed to relax, keep their eyes closed, and stay awake. Furthermore, the individuals were fixed in place using foam padding to reduce head movement, and earplugs were utilized to minimize scanner noise. The rs-fMRI examination was performed using an echo-planar imaging sequence with the following parameters: TR = 2000 ms; TE = 30 ms; flip angle = 90°; field of view (FOV) = 240 × 240 mm; voxel size = 3.0 × 3.0 × 4.0 mm; slice interval = 0 mm; number of slices = 32; number of excitations (NEX) = 1; 200 volumes; and scan time = 6 min 40 s. Sagittal T1 high-resolution imaging was achieved using a 3D magnetization prepared rapid gradient echo sequence with the following parameters: TR = 7.8 ms; TE = 3.0 ms; flip angle = 15°; FOV = 256 × 256 mm; voxel size = 1.0 × 1.0 × 1.0 mm; slice interval = 0 mm; number of slices = 188; NEX = 1; and scan time = 4 min 10 s.
Data processing
The rs-fMRI data were processed using DPABI 5.1 software (23) on the MATLAB 2013b platform (MathWorks, Natick, MA, USA). The data preprocessing included the following: (i) converting the fMRI image and structural image data from a DICOM to a NIFTI format; (ii) removing the first 10 time points because of the possible instability of the initial MRI signal; (iii) choosing the middle 32nd slice as the reference slice to correct for differences in the image acquisition time; (iv) realigning head motion correction to ensure the accuracy of the position information and to remove more than 2.0 mm head translation in any direction and 2.0° head rotation; (v) normalizing by diffeomorphic anatomical registration and exponential Lie algebra using a new segment on 3D T1-weighted images: spatial normalization to the Montreal Neurological Institute (MNI) space using diffeomorphic anatomical registration and exponential Lie algebra (DARTEL) to solve the differences in brain deformation among different individuals and spatial positions, with a resampled voxel size of 3 × 3 × 3 mm3; (vi) spatial smoothing with a Gaussian kernel of 6 mm full-width at half maximum (FWHM); (vii) using linear regression for detrending; (viii) regression: nuisance covariates regression includes the 24 head motion parameters, white matter signal, and cerebrospinal fluid (CSF) signal, which were used to remove the interference signal; and (ix) filtering the band-pass ranges of 0.01–0.08. Furthermore, the three voxelwise metric parameters and seed-based FC were applied to the preprocessed fMRI data.
ALFF calculation
The preprocessing for the ALFF calculation does not require filtering; the time courses of each voxel were transformed into the frequency domain using a fast-Fourier transform algorithm, and the power spectrum was obtained. The average square root at each frequency of the power spectrum across 0.01–0.08 Hz was calculated as the ALFF value, and each individual's ALFF value was then divided by the global mean ALFF for group comparison.
ReHo calculation
The preprocessing for the ReHo calculation does not require spatial smoothing. The ReHo calculation was performed using Kendall's coefficient of concordance to measure the synchronicity of the time courses between a core voxel and its 27 nearest neighbors in the current study. The ReHo value of each voxel was then divided by the global mean ReHo of each individual for standardization purposes. Furthermore, spatial smoothing was subsequently performed.
DC calculation
The preprocessing for the ALFF calculation does not require spatial smoothing. DC is defined as the sum of weights from the edges connecting to a node for the weighted graph. The correlation matrix threshold was set to r = 0.6. The threshold was used to eliminate counting voxels with low temporal correlation. Weighted DC was obtained for each voxel, and the weighted DC of each voxel was further divided by the global mean weighted DC.
Seed-based FC analysis
The brain regions with the largest abnormalities in the ALFF and ReHo value group comparisons were selected as ROIs to calculate the whole brain and its FC (peak MNI coordinate, radius = 5 mm). The resulting correlation coefficients were normalized into Z values using Fisher's Z-transformation.
VBM analysis
Structural data were processed using the VBM8 toolbox installed in SPM8 (Wellcome Department of Imaging Neuroscience, University College London, London, UK) based on MATLAB. First, we converted structural image data from DICOM to the NIFTI format and then checked the image quality. The 3D structural image was segmented into gray matter, white matter, and CSF based on the VBM8 template toolbox. The DARTEL template was used for spatial normalization into the MNI space and inspatial position, and the images were resampled to 1.5-mm isotropic voxels. Finally, spatial smoothing was performed with an 8-mm FWHM Gaussian kernel.
Statistical analysis
The related clinical parameters of age and sex between patients with VN and HCs were analyzed using SPSS version 22 software (IBM Corp., Armonk, NY, USA). Two-sample t-tests were used to examine the differences in age and education level, and the chi-square test was used to evaluate the difference in sex. The differences were considered statistically significant when P <0.05.
Rs-fMRI parameters were analyzed using a statistical module in SPM12. Differences in ALFF, ReHo, DC, seed-based FC, and GMV between patients with VN and HCs were analyzed using a two-sample t-test . Covariates including age, sex, and education level were regressed out. The results were corrected for familywise error (FWE) during group comparisons. A Pearson correlation analysis was used to assess local brain abnormalities and duration of the vertigo. P <0.001 and Cluster P <0.05 were considered statistically significant. The results were presented using xjview and MRIcron.
Results
Clinical data
In total, 30 patients with VN and 26 HCs without any history of neurological or psychiatric diseases were recruited. Six patients with VN (cerebral ischemic stroke = 2, meningeoma = 1, head motion >2 mm = 3) and four HCs (claustrophobic = 1, obvious multiple infarcts = 1, head motion >2 mm = 2) were excluded. Ultimately, the study included 24 patients with VN and 22 HCs. Age, sex, and level of education did not significantly differ between patients with VN and HCs (P = 0.830,0.425, 0.763). In the group of patients with VN, the duration of vertigo was distributed as follows: 13 patients experienced vertigo for <1 day; eight patients had vertigo lasting between 1 day and 1 week; and three patients reported vertigo persisting for >1 week.
Changes in ALFF, ReHo, and DC values in patients with VN and HCs
Compared with HCs, the patients with VN exhibited increased ALFF values in the left lingual gyrus (P <0.001). The left lingual gyrus, right lingual gyrus, and right postcentral gyrus showed increased ReHo values in patients with VN compared to HCs (P <0.001, 0.002, <0.001). Meanwhile, the left lingual gyrus showed increased DC values (P = 0.013). The local brain abnormalities of ALFF, ReHo, and DC information are summarized in Table 1 and Fig. 1a–c.
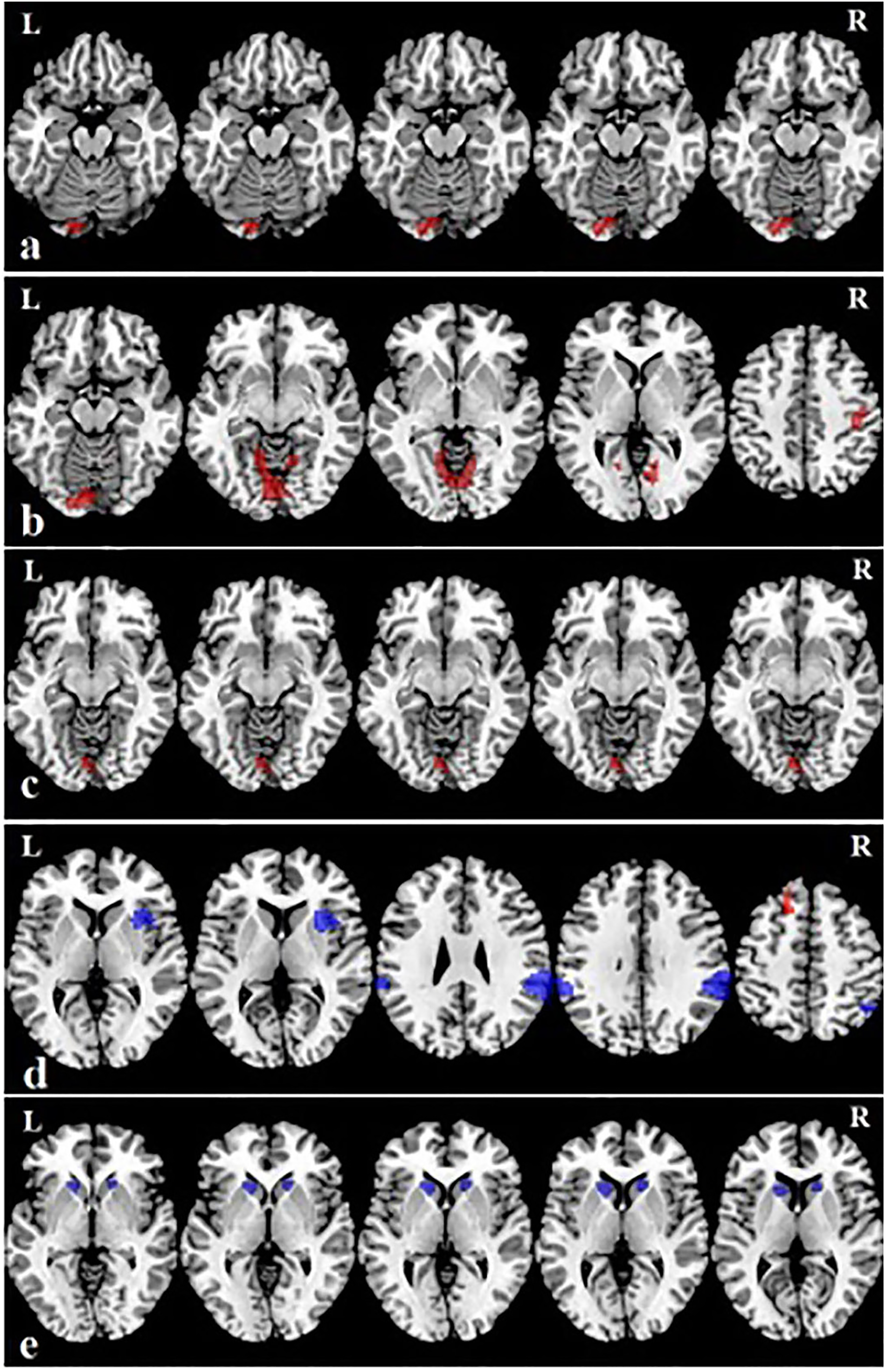
Red indicates increased brain regions or connectivity, whereas blue indicates decreased connectivity. (a) ALFF showed an increase in left lingual gyrus. (b) ReHo showed increased activity in the left lingual gyrus, right postcentral gyrus, and right lingual gyrus. (c) Degree centrality showed an increase in left lingual gyrus. (d) The region of the left lingual gyrus showed increased ReHo and ALFF values simultaneously and was selected as the region of interest for calculation. Seed-based FC analysis showed increased FC between the left lingual gyrus and the left superior frontal gyrus and decreased FC between the left lingual gyrus and right insula gyrus, right supramarginal gyrus, and left supramarginal gyrus; (e) voxel-based morphometry analysis showed reduced gray matter volume in both the right and left caudate. ALFF, amplitude of low frequency fluctuation; FC, functional connectivity; ReHo, regional homogeneity.
Regions showing local brain abnormalities of ALFF, ReHo, and DC in patients with VN and HCs.
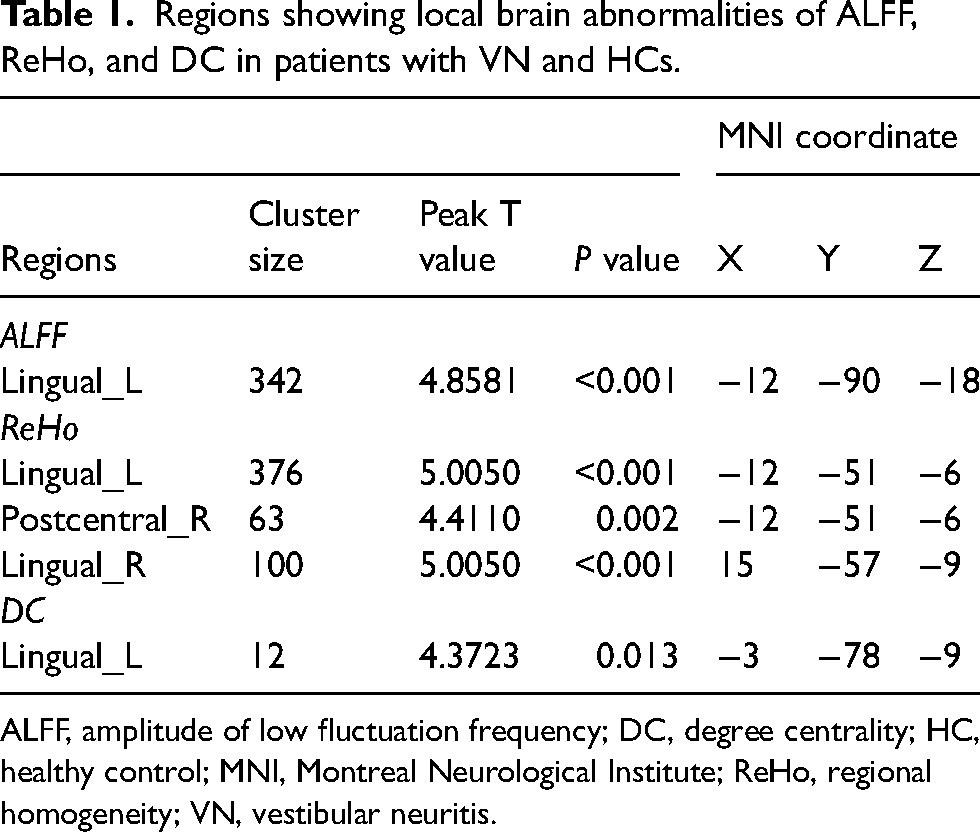
ALFF, amplitude of low fluctuation frequency; DC, degree centrality; HC, healthy control; MNI, Montreal Neurological Institute; ReHo, regional homogeneity; VN, vestibular neuritis.
Seed-based FC analysis
From the resulting fMRI analyses, we selected the left lingual gyrus in which the ALFF and ReHo values were increased simultaneously in patients with VN as the seed coordinate in the connectivity analyses. The seed-based FC analysis showed increased FC between the left lingual gyrus and the left superior frontal gyrus and decreased FC between the left lingual gyrus and the right insula gyrus, right supramarginal gyrus, and left supramarginal gyrus (P = 0.012, 0.004, <0.001, 0.014). The voxelwise seed-based FC analysis results are summarized in Table 2 and Fig. 1d.
Regions showing FC analysis in patients with VN and HCs.
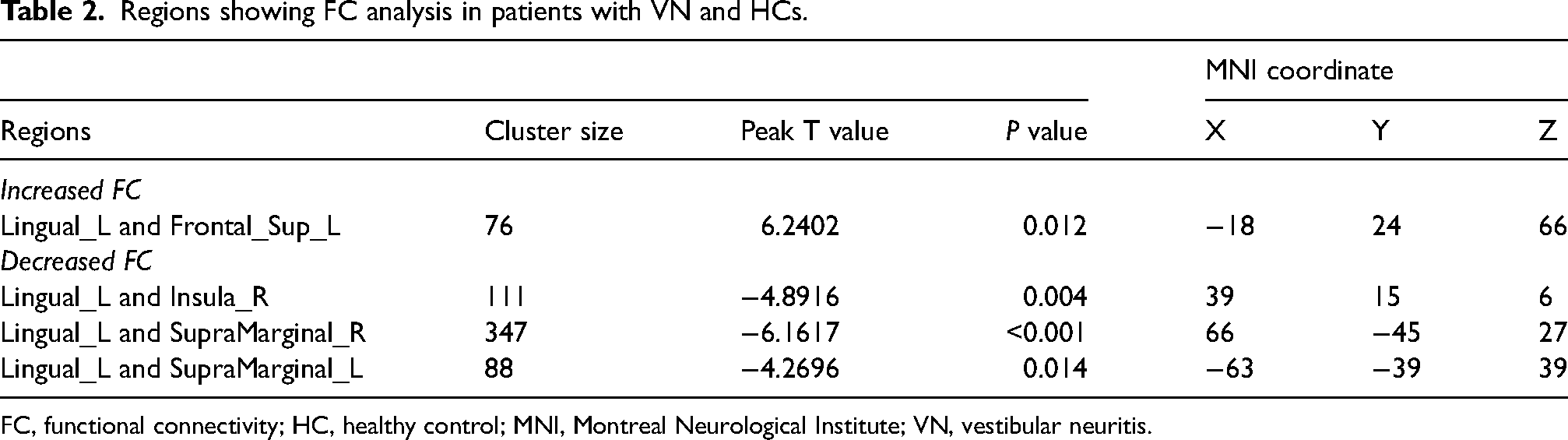
FC, functional connectivity; HC, healthy control; MNI, Montreal Neurological Institute; VN, vestibular neuritis.
VBM analysis
Compared with the HCs, patients with VN showed a reduced GMV in the right caudate gyrus and left caudate gyrus (P = 0.022, 0.014). No associated brain regions with increased GMV by FWE were corrected. The results of the VBM analysis are summarized in Table 3 and Fig. 1e.
Regions showing gray matter volume in patients with VN and HCs.
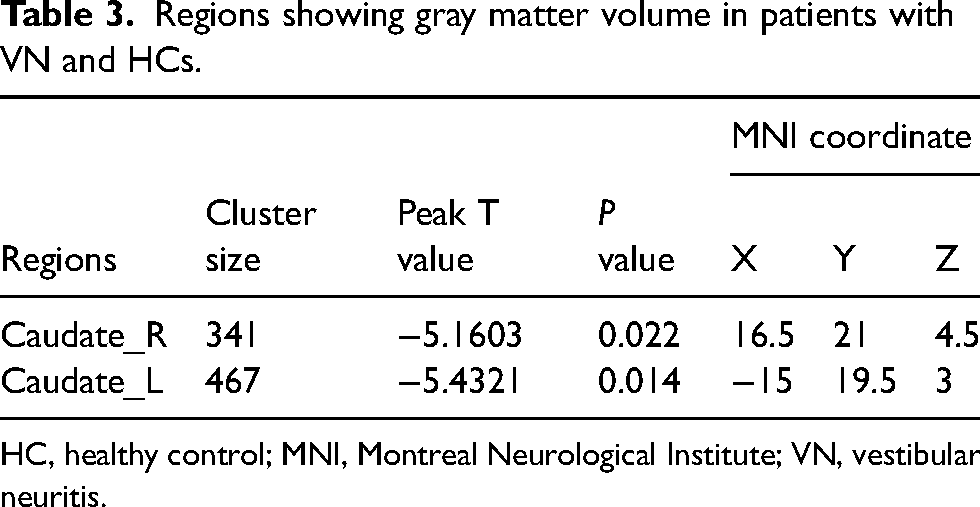
HC, healthy control; MNI, Montreal Neurological Institute; VN, vestibular neuritis.
Correlation analyses between local brain abnormalities and duration of the vertigo
No significant correlation was found between local brain abnormalities and duration of the vertigo in patients with VN.
Discussion
In this study, local brain functional alterations in patients with VN were assessed using three local metrics (ALFF, ReHo, and DC) and seed-based FC analysis through rs-fMRI. The study found that increased ALFF values were observed in the left lingual gyrus, while increased ReHo values were observed in the left lingual gyrus, right lingual gyrus, and right postcentral gyrus. In addition, reduced GMV was observed in the bilateral caudate gyrus. These results suggest that VN is associated with local brain abnormalities in patients, which may aid in understanding the brain functional mechanism underlying this condition.
Our findings showed increased ALFF, ReHo, and DC in the left lingual gyrus and increased ReHo in the right postcentral gyrus and lingual gyrus, which indicated increased spontaneous neuronal activity within the local brain region (24–26). The lingual gyrus is part of the occipital cortex and is located in the visual network. Its function is defined as visual spatial image and episodic memory extraction to synthesize visual information and form conscious perception, which helps to process visual information processing. Related research also confirmed that the lingual gyrus communicates with the cerebral cortex and plays a role in the perception of facial emotion, visual attention, and visual judgment (27–29). Patients with VN usually showed spontaneous, dominantly horizontal-torsional nystagmus and increased intensity when they looked in the direction of the fast phase of nystagmus (30,31). The intensity of nystagmus increased, which increased spontaneous neuronal activity, so the ALFF value increased in the left lingual gyrus. Related studies confirmed that patients with VN exhibited a vestibulo-ocular reflex, caloric responsiveness, and postural sway (32). These enhanced functional activities further increased neuronal activity in the lingual gyrus. Furthermore, a bilingual gyrus with increased ReHo indicates more local synchronization of the BOLD signal, which plays an important role in the brain network in patients with VN. The increased neuronal activity of the lingual gyrus reflects the integration function of visual information in the brains of patients, which is likely an adaptive change in response to repeated vertigo processes (33). DC reflects the role and position of voxels in the brain network. An increased DC value was observed in the left lingual gyrus, indicating the heightened importance of this region in the brain with VN. Finally, the results of this study were related to laterality, and the left lingual gyrus simultaneously showed increased ALFF, ReHo, and DC values. However, the right lingual gyrus only showed increased ReHo values, and the cluster size was much smaller than the side. This fact may be caused by the complex interplay between the lesion side and stimulation side of the individual (14,34).
Moreover, we also found increased ReHo values in the right postcentral region. The postcentral region, a region of the parietal lobe, is a component of the sensorimotor cortex and sensorimotor network (32). An increase in ReHo values in the postcentral region might result in patients with VN exhibiting acute gait unsteadiness, as they are able to activate the associated sensorimotor brain regions.
Previous studies confirmed that ReHo and ALFF increased simultaneously in some brain regions, suggesting that the brain activity of neurons in these regions was locally homogeneous (35). Therefore, based on comparisons of the ALFF and ReHo values between groups, the left lingual gyrus was selected for seed point coordination. Compared with the HCs, patients with VN showed decreased FC between the left lingual and right insula gyri and bilateral supramarginal regions. Related research has found cortical hypertrophy in regions of the insular and lingual gyrus based on a VBM analysis of patients with VN (18). Cortical atrophy would indicate the dominance of afferent connections receiving peripheral sensory input in the area (19,21). On the contrary, this hypertrophy, in turn, affects FC between the vestibular circuit and the right insula, and decreased FC between the lingual and insula gyri. Previous studies have reported that the posterior insular cortex is often regarded as an integrator of visual and vestibular motor information, and the processing of visual and vestibular information in patients with VN is affected by unilateral vestibular failure (36) and related decreased FC. The supramarginal gyrus is involved in a variety of cognitive functions, such as visual attention and imagery. Messina et al. confirmed structural abnormalities of the supramarginal gyrus in patients with migraine (37). Zhe et al. also demonstrated reduced supramarginal volume in patients with VM and suggested that the supramarginal gyrus might be involved in general pain processing or in pain response (16). The insular cortex is considered a critical cortical region of the pain network and plays a vital role in the development and regulation of pain (38). It directly or indirectly participates in the perception, coding, and regulation of pain. As indicated above, decreased FC between the left lingual and insula reflects the reduced FC between the lingual and supramarginal regions to some extent.
Of course, we also found increased FC between the left lingual and left superior frontal gyrus in this study. Klingner CM proposed that patients with VN often display an imbalance in vestibular tone. This imbalance results in bilateral information deviation and spontaneous nystagmus (15). Such manifestations necessitate a marked improvement in the ability to process spatial orientation information. The superior frontal gyrus plays an important role in executive function. Therefore, the increased FC between the lingual and superior frontal gyrus is simultaneously reflected by the increased activity in brain regions responsible for the processing of vestibular information and integration of multisensory information (39).
A previous longitudinal analysis showed brain structural changes in patients with VN after vestibular compensation (18). Moreover, Helmchen et al. confirmed that an increase in GMV was related to an improvement in vestibular function and central vestibular compensation (19). In our study, we also found abnormalities in brain regions. Compared with the HCs, patients with VN showed reduced GMV in the bilateral caudate. The most likely reason for the difference proven in a previous study was the longitudinal analysis, which reflects the processing of the vestibular compensation mechanism. The caudate, as a part of the striatum, is an important part of the brain's learning and memory system. It also influences body movement regulation, sensory conduction processes, and the mechanisms that regulate pain conduction. Previous reports have shown that the caudate is critically associated with the severity of cognitive decline (40). Decreased GMV suggests that patients with VN may have learning imitation and memory disorders.
The present study has some limitations. First, the relatively small sample size may introduce bias in the comparative evaluations. Further analyses with a larger sample of patients with VN are needed to examine brain functional activity. Second, this study lacked a dizziness handicap inventory, Montreal Cognitive Assessment, and/or Mini-mental State Examination Analysis and relevant clinical indicators for patients with VN.
In conclusion, we used rs-fMRI to investigate the brain activity of patients with VN and analyzed both the functional and structural brain data. Our results suggest that patients with VN exhibit abnormal neuronal activity intensity and extensive brain functional abnormalities in various regions. In addition, our FC analysis showed that the brain networks in patients with VN adapt to repeated vertigo processes, particularly between the visual, pain, and executive networks. We also observed reduced GMV, which further indicates abnormalities in brain function in patients with VN.
Footnotes
Acknowledgments
The authors thank Professors Yu Dexin and Wang XiZhen for their assistance with the research and Dmytro Pylypenko for the English revision of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.