
Abstract
Background
The diagnostic impact of deep learning computed tomography (CT) reconstruction on intracranial aneurysm (IA) remains unclear.
Purpose
To quantify the image quality and diagnostic confidence on IA in craniocervical CT angiography (CTA) reconstructed with DEep Learning Trained Algorithm (DELTA) compared to the routine hybrid iterative reconstruction (HIR).
Material and Methods
A total of 60 patients who underwent craniocervical CTA and were diagnosed with IA were retrospectively enrolled. Images were reconstructed with DELTA and HIR, where the image quality was first compared in noise, signal-to-noise ratio (SNR), and contrast-to-noise ratio (CNR). Next, two radiologists independently graded the noise appearance, arterial sharpness, small vessel visibility, conspicuity of calcifications that may present in arteries, and overall image quality, each with a 5-point Likert scale. The diagnostic confidence on IAs of various sizes was also graded.
Results
Significantly lower noise and higher SNR and CNR were found on DELTA than on HIR images (all P < 0.05). All five subjective metrics were scored higher by both readers on the DELTA images (all P < 0.05), with good to excellent inter-observer agreement (κ = 0.77–0.93). DELTA images were rated with higher diagnostic confidence on IAs compared to HIR (P < 0.001), particularly for those with size ≤3 mm, which were scored 4.5 ± 0.6 versus 3.4 ± 0.8 and 4.4 ± 0.7 versus 3.5 ± 0.8 by two readers, respectively.
Conclusion
The DELTA shows potential for improving the image quality and the associated confidence in diagnosing IA that may be worth consideration for routine craniocervical CTA applications.
Keywords
Introduction
Intracranial aneurysm (IA) is a local bulge or dilation in the cerebral artery, typically occurring at weak points of the vessel wall that outpunch under the pressure of blood flow (1). The rupture of IA accounts for nearly 85% (2,3) of non-traumatic subarachnoid hemorrhage (SAH), which is associated with high morbidity and mortality rates. Unfortunately, the risk of incidental IAs is often hard to assess, given that most IAs are silent and asymptomatic until rupture (4). Prompt identification, counseling, and timely management of the underlying IA, therefore, would be of obvious clinical value.
For diagnosis, routine surveillance, or procedural planning of IA, computed tomography angiography (CTA) is one of the first modalities of choice in the clinical setting, owing to its excellent spatial and contrast resolution. Over the past decade, iterative reconstruction (IR) algorithms have been widely used in CT and showed superior performance over the classical filtered-back projection methods in a variety of applications, where the delineation of vascular structure was also largely improved (5–7). Lately, with the rapid development of artificial intelligence, deep learning-based reconstructions (DLRs) emerged and have shown great potential in suppressing the image noise while keeping the image texture. Growing evidence has been found for applying DLRs in head CT, abdominal CT, chest CT, and cardiac CTA (8–12). However, only a few studies investigated the application of DLR in head or craniocervical CTA (13,14). Chuluunbaatar et al. (13) evaluated the performance of different reconstruction algorithms in head CTA, where the DLR was found capable of reducing the noise by 33.68%, improving the contrast-to-noise ratio (CNR) by 44.86%, and delivering a more favorable depiction of small vessels as compared to hybrid IR (HIR). Huang et al. (14) demonstrated that the application of DLR in head CTA allows for a reduction of 37.5% in contrast medium dose and 41% in radiation dose without compromising the image quality. Though these studies have proved the value of DLR in improving image quality, the cohort under investigation was formed in the general sense. Moreover, the diagnostic impact on specific abnormalities remains unclear.
In this retrospective study, we assessed the image quality and diagnostic confidence on IA in craniocervical CTA images that were reconstructed using a novel DEep Learning Trained Algorithm (DELTA; United Imaging Healthcare, Shanghai, PR China) for a cohort of patients with known IAs. Previous investigations have provided clinical evidence of DELTA in liver and chest CT applications (15,16). It was hypothesized in this study that CTA images reconstructed using the DELTA algorithm would be able to provide superior image quality and improve confidence in diagnosing IAs over the current routine HIR techniques.
Material and Methods
Patient enrollment
This study was approved by the institutional review board. Owing to the retrospective nature of the study, written informed consent was waived.
Fig. 1 shows the flow chart of case collection and study design. In our institution, the craniocervical CTA protocol was used for the diagnosis and following up of IA. In total, 65 patients who took a craniocervical CTA between November 2022 and April 2023 and were diagnosed with IA were enrolled in this study. Demographic and histopathological information was obtained from the medical records. Excluding the cases lacking the CT raw data, which were necessary for additional reconstruction, the final set consisted of 60 patients (male:female ratio = 1.5:1.0; mean age = 67.7 ± 13.9 years; age range = 36–89 years), six of whom were further confirmed with DSA during surgery at our hospital while the diagnosis of the remaining patients had to rely on the CTA alone.
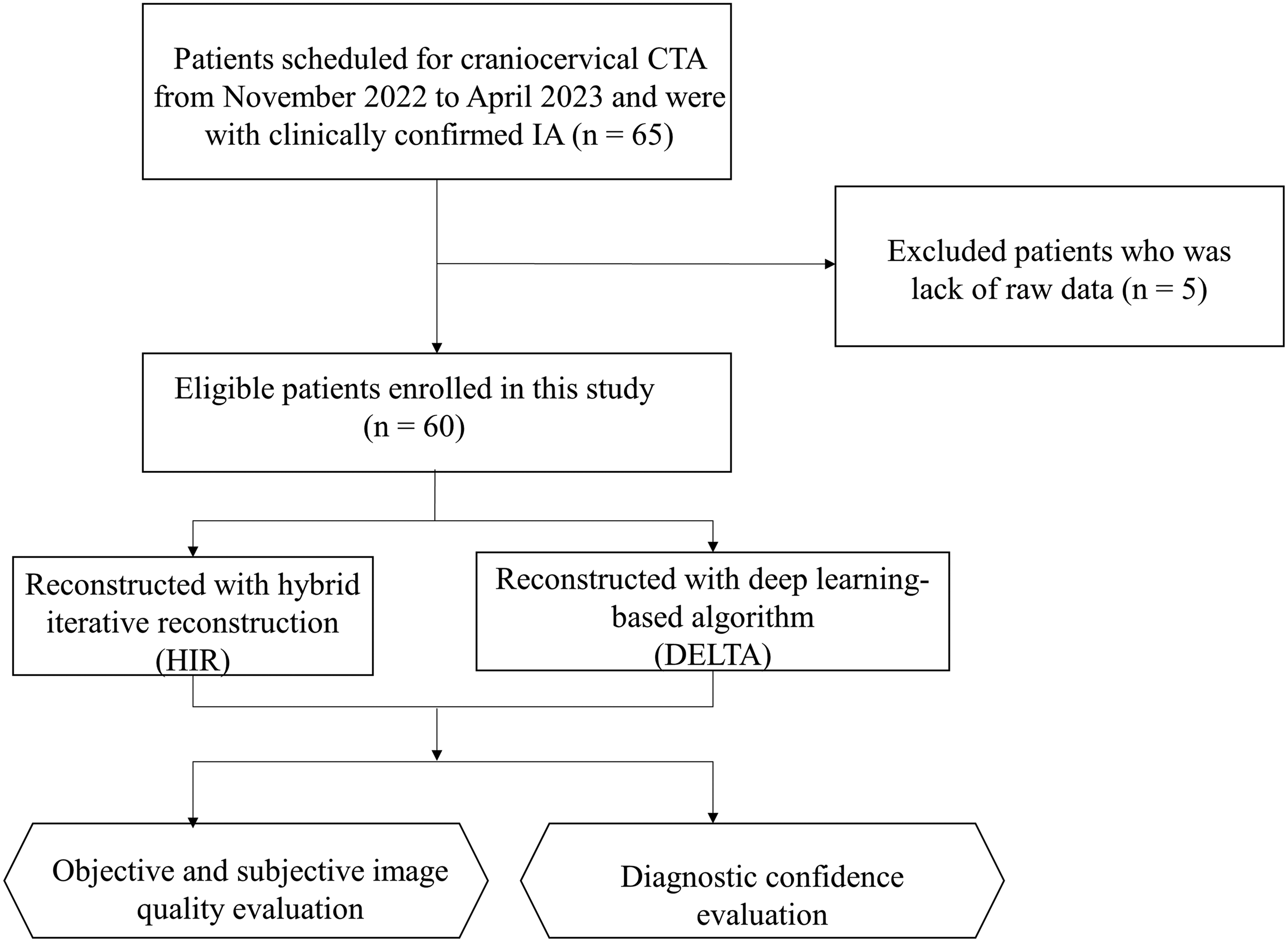
Flow chart of patient enrollment and study design.
CTA protocol and image reconstruction
All the craniocervical CTA examinations were performed on a 320-row CT scanner (uCT960+; United Imaging Healthcare, Shanghai, PR China). The acquisition was conducted in helical mode with the following parameters: tube voltage = 100 kVp; auto-modulated tube current with a reference of 157 mAs; rotation time = 0.5 s; longitudinal collimation = 80 mm; and pitch = 0.89.
A total of 60 mL of iodinated contrast medium (Lobitridol, 350 mg I/Ml; XENETIX) was intravenously injected with a flow rate of 5.0 mL/s, followed by 30 mL of saline solution at the same rate. A region of interest (ROI) for bolus-tracking was placed on the descending aorta with a triggering threshold of 120 Hounsfield units (HU). The acquisition time was approximately 3–4 s. For all enrolled cases, the volume CT dose index (CTDIvol) and the dose length product (DLP) were in the range of 4.86–8.88 mGy and 225.47–399.76 mGy cm, respectively.
DELTA reconstruction was applied to the CT raw data in addition to the original HIR (KARL 3D; United Imaging Healthcare, Shanghai, PR China), with a slice thickness of 1.0 mm, slice increment of 0.5 mm, and a matrix size of 512 × 512 pixels. Then, a total of 120 resulting image sets (HIR: n = 60; DELTA: n = 60) were transferred to the clinical workstation (uWS-CT; United Imaging Healthcare, Shanghai, PR China) for objective and subjective analysis.
Image quality evaluation
Objective image quality, including the noise, signal-to-noise ratio (SNR), and contrast-to-noise ratio (CNR), were measured by two radiologists with four and six years of experience in neuroradiology, respectively, where each measurement was performed using a circular ROI three times and averaged. The radiologist with four years of experience was also asked to measure the size of IAs, which defined the largest diameter.
Fig. 2 shows the positioning of the ROIs. The ROI for IA was placed on the plane of the largest diameter for each case. The ROIs for the arteries were set to half to two-thirds in diameter of the corresponding lumen and placed on the center of the vertebral artery (VA), the basilar artery (BA) trunk, the cavernous segment of the internal carotid artery (ICA), and the first segment of middle cerebral artery (MCA) trunk, while avoiding the vessel wall and any calcification plaques that may present. An additional circular ROI of 100 mm2 placed on the white matter of the cerebellar hemisphere was defined as the background. The ROIs were first placed on the HIR images and then copied-pasted to the DELTA images.
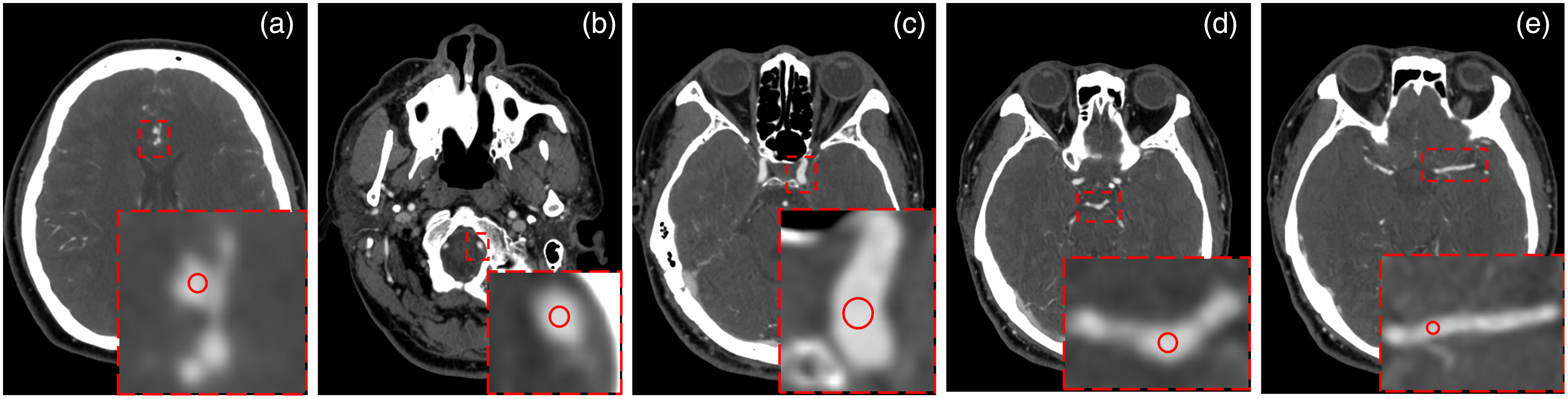
Positioning of the regions of interest for measuring the objective image quality (window W/L = 550/150 HU) on: (a) intracranial aneurysm; (b) vertebral artery; (c) cavernous segment of the internal carotid artery; (d) basilar artery trunk; and (e) the first segment of middle cerebral artery, respectively.
Noise was calculated by the standard deviation (SD) of the CT value (in HU) within the ROI. SNR and CNR were calculated with:


Two more radiologists, with 20 and 12 years of experience in neuroradiology, respectively, and blinded to the reconstruction methods and all patient information except the diagnostic report on IA, were invited to grade the subjective image quality in an independent manner, including the noise appearance, arterial sharpness, small vessel visibility, conspicuity of calcifications that may present in the arteries, and the overall image quality. To minimize the subjective bias, the image sets of two reconstruction algorithms were mixed and presented in a random order. The grading was performed using a modified 5-point Likert scale system suggested by previous studies (14,17), where 1 = unacceptable and 5 = excellent. A score ≥3 was deemed diagnostically acceptable.
The reconstructed images were displayed in a preset window width/level of 300/45 HU on the clinical workstation, which was freely adjustable during the reading. Multi-planar reconstruction (MPR), maximum intensity projections (MIP), and volume rendering (VR) images were reproduced each time by the readers as needed, where the processing, except the automatic vessel extraction for generating the VR, was manual and largely up to the reader's experience and preference.
Diagnostic confidence evaluation
For each confirmed IA with known location and size, the same readers who performed subjective image quality assessment were invited to independently rate the diagnostic confidence on a scale of five, with 5 points denoting the highest certainty (definite) and 1 point the poorest (cannot be determined). The image quality on those with a score ≥3 was considered sufficient for clinical diagnosis, otherwise, additional DSA and following up were recommended.
As a subgroup analysis, the diagnostic confidence was further investigated per size group, which was classified as sizes ≤3 mm, 3–<7 mm, and ≥7 mm.
Statistical analysis
All statistical analyses were performed using SPSS version 27.0 (IBM Corp., Armonk, NY, USA). Quantitative variables were expressed as mean ± SD or median (interquartile range [IQR]) as appropriate and were tested for normality using the Kolmogorov-Smirnov test. For data with normal distribution, the Student's t-test was used, otherwise the Wilcoxon signed-rank test was used. Categorical variables were expressed as numbers and percentages, where the difference was analyzed using the chi-square test. A two-tailed P < 0.05 was considered statistically significant. The intraclass correlation coefficient (ICC) and Cohen's Kappa analysis were used to test the inter-observer agreement in objective analysis and subjective scores, respectively, where an ICC or κ value of ≤0.20, 0.21–0.40, 0.41–0.60, 0.61–0.80, and≥0.81 indicated poor, fair, moderate, good, and excellent agreement, respectively (18).
Results
Patient characteristics
The patient characteristics and the diagnostic results of IAs are listed in Table 1. In terms of the location of IA, it was found most common in ICAs (58.82%) and MCAs (22.06%). In terms of the size of IA, 24 (35.29%) were measured as ≤3 mm. No aneurysms with calcifications or thrombus were observed.
Characteristics of patients and IAs.
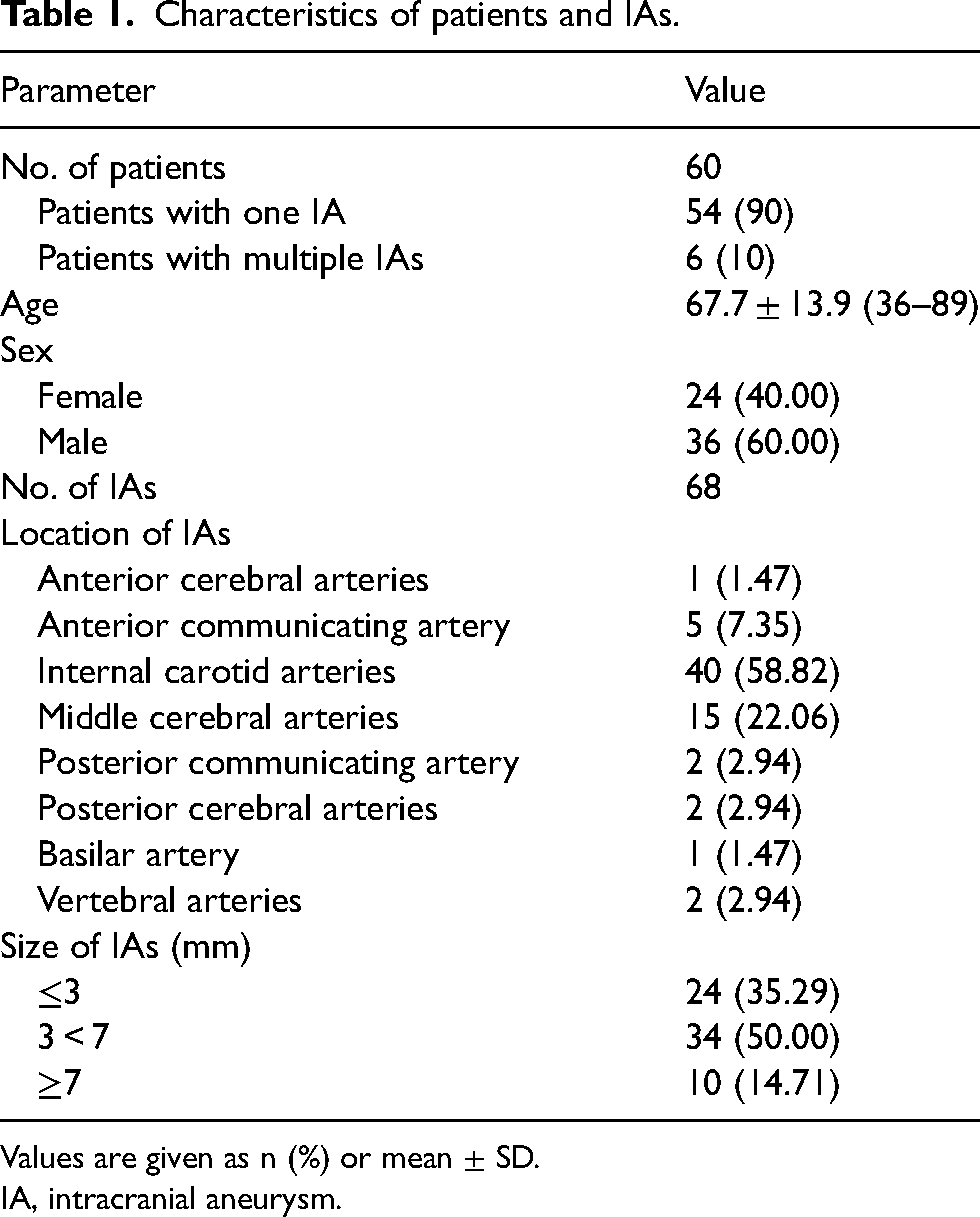
Values are given as n (%) or mean ± SD.
IA, intracranial aneurysm.
Objective image quality
The median size of IAs was 3.6 mm (IQR = 3.0–5.0 mm) on both HIR and DELTA images, with no significant difference observed (P > 0.05). The image noise, SNR, and CNR on four arteries (VA, BA, ICA, and MCA) and IAs are summarized in Table 2. Compared to HIR, DELTA performed better on suppressing image noise (all P < 0.05), leading to a significantly superior SNR and CNR on all ROIs according to both readers (all P < 0.001). The inter-observer agreement for all objective measurements was excellent, with an ICC value up to 0.97, 0.92, and 0.96 for HIR and 0.95, 0.93, and 0.90 for DELTA regarding noise, SNR, and CNR, respectively.
Objective image quality assessment of HIR and DELTA images.
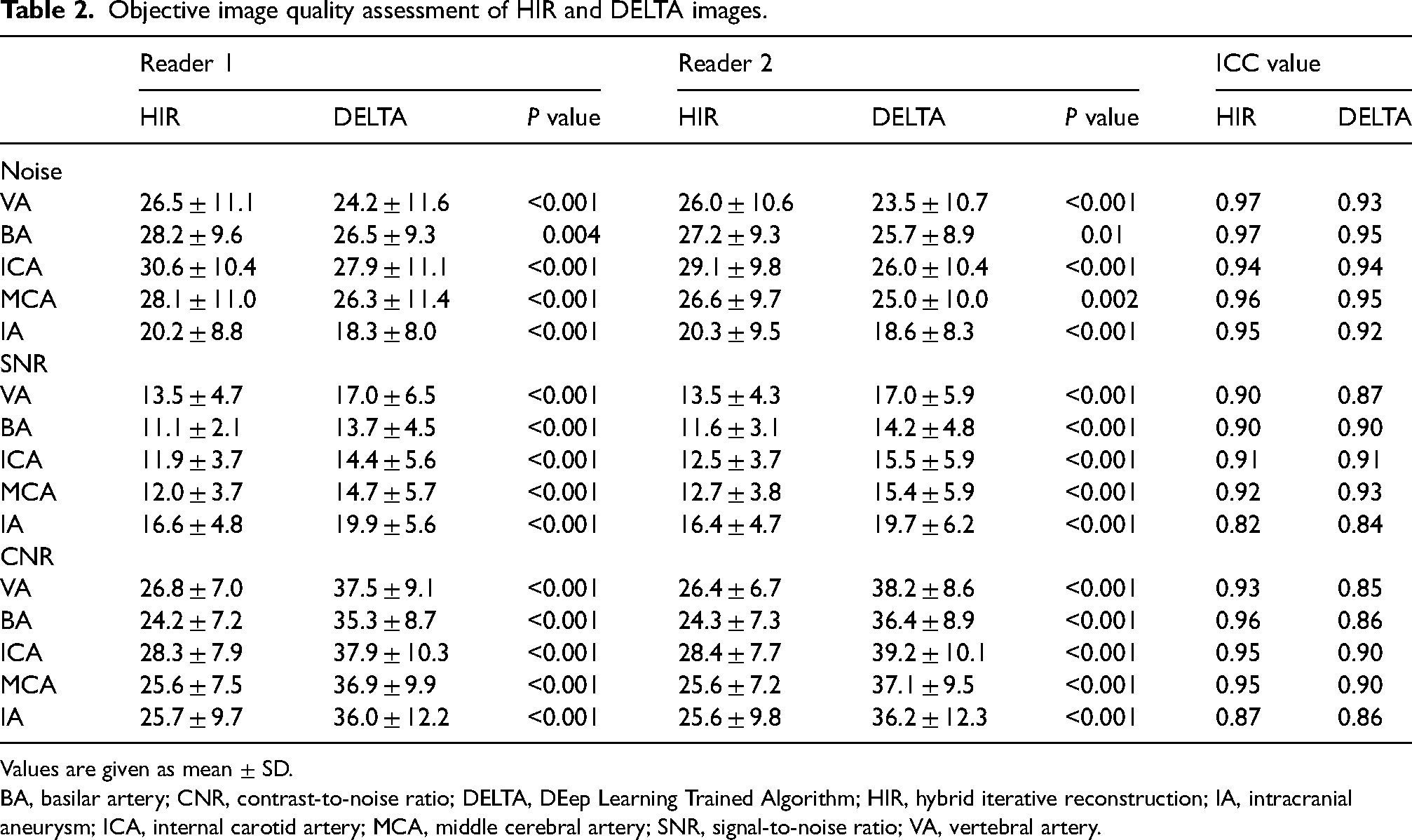
Values are given as mean ± SD.
BA, basilar artery; CNR, contrast-to-noise ratio; DELTA, DEep Learning Trained Algorithm; HIR, hybrid iterative reconstruction; IA, intracranial aneurysm; ICA, internal carotid artery; MCA, middle cerebral artery; SNR, signal-to-noise ratio; VA, vertebral artery.
Subjective image quality
Table 3 summarizes the subjective image quality scores. Of note is that the scores of conspicuity referred to the calcifications that may be present in the arteries, rather than within the IA, which was not found in the cases under investigation. For both readers, the scores of five subjective image quality metrics were all significantly higher on DELTA than those on HIR (all P < 0.05). The inter-observer agreement for all subjective ratings ranged from good to excellent, with kappa values in the range of 0.73–0.96 for HIR and 0.77–0.93 for DELTA.
Subjective image quality scores of HIR and DELTA images.
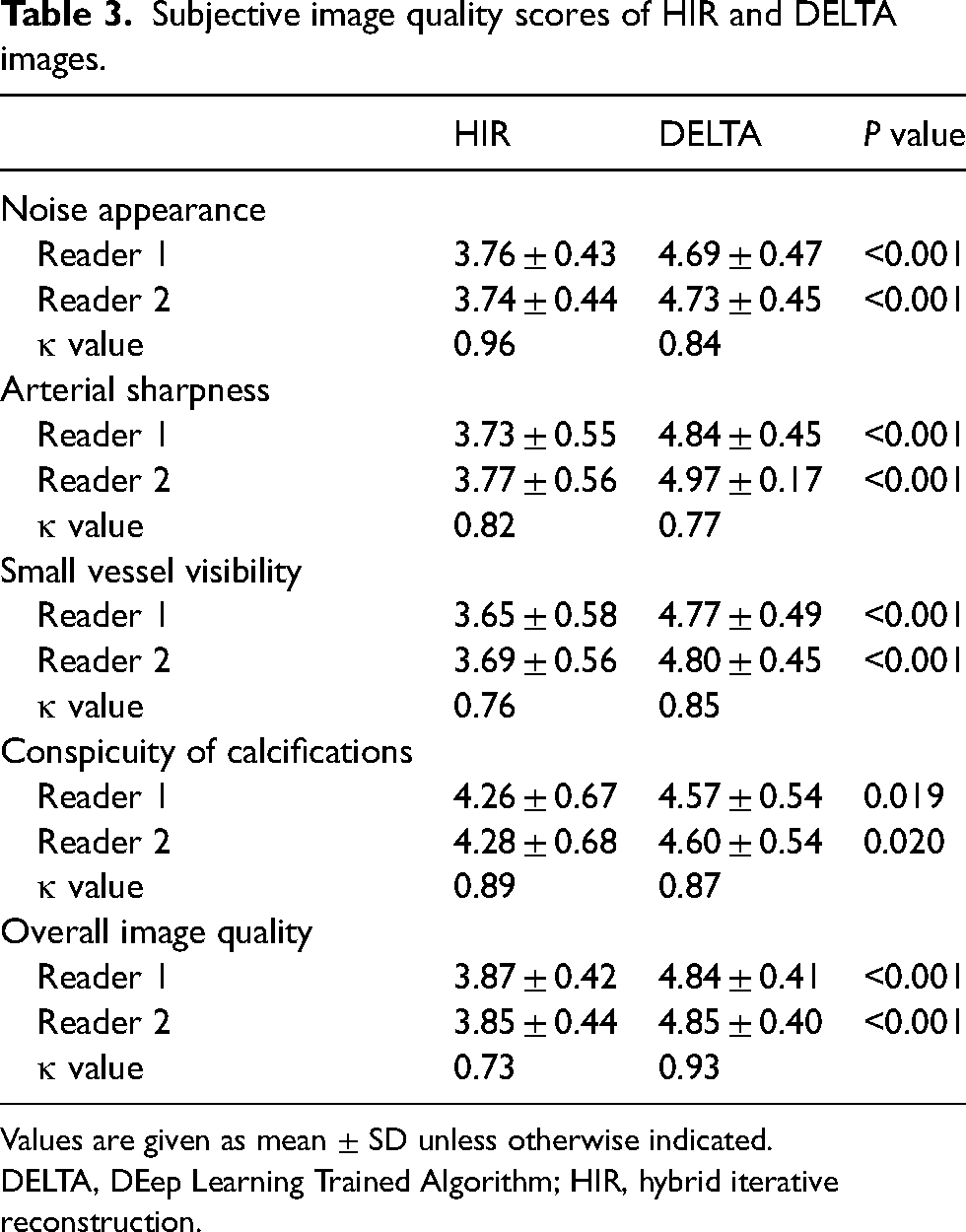
Values are given as mean ± SD unless otherwise indicated.
DELTA, DEep Learning Trained Algorithm; HIR, hybrid iterative reconstruction.
Among all metrics, the improvement of the subjective score seemed to be most profound on the small vessel visibility, where the mean scores for HIR and DELTA by two readers were 3.65 ± 0.58 versus 4.77 ± 0.49 and 3.69 ± 0.56 versus 4.80 ± 0.45 (both P < 0.001), respectively. As shown in Fig. 3, DELTA images provided sharper arterial boundaries and improved the visibility of small arterial details on both proximal and distal sides compared to HIR images, offering a more complete characterization of the vasculature without increasing the overall iodine medium dose.
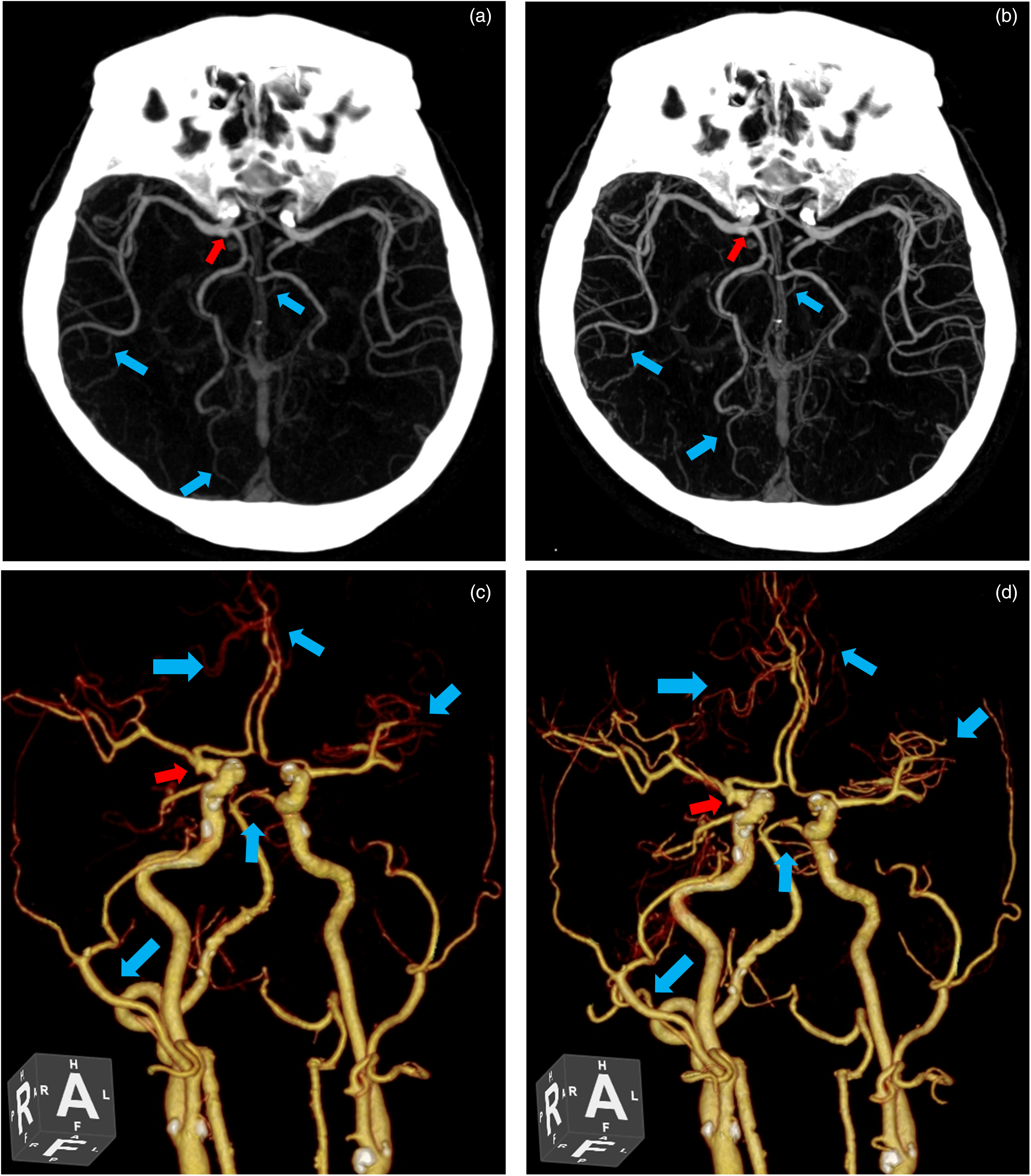
Craniocervical CTA of a 75-year-old man with an aneurysm in the right carotid terminus (red arrow): (a) maximum intensity projection of the HIR and (b) the DELTA images; and (c) volume rendering of the HIR and (d) the DELTA images. Compared to HIR, DELTA improved the visibility of small arterial details on both proximal and distal ends with reduced image noise (blue arrows). The image quality of HIR and DELTA was graded 3 and 5, respectively, by both radiologists. CTA, computed tomography angiography; DELTA, DEep Learning Trained Algorithm; HIR, hybrid iterative reconstruction.
Diagnostic confidence
Table 4 summarizes the diagnostic confidence scores. Both radiologists showed higher diagnostic confidence on average with the DELTA images than with HIR images, where the mean scores were 4.57 ± 0.61 versus 3.78 ± 0.94 and 4.54 ± 0.63 versus 3.76 ± 0.83 for the two readers (both P < 0.001), respectively. The inter-observer agreement was excellent, with a kappa value up to 0.85 on HIR images and 0.83 on DELTA images.
Diagnostic confidence score of HIR and DELTA images.
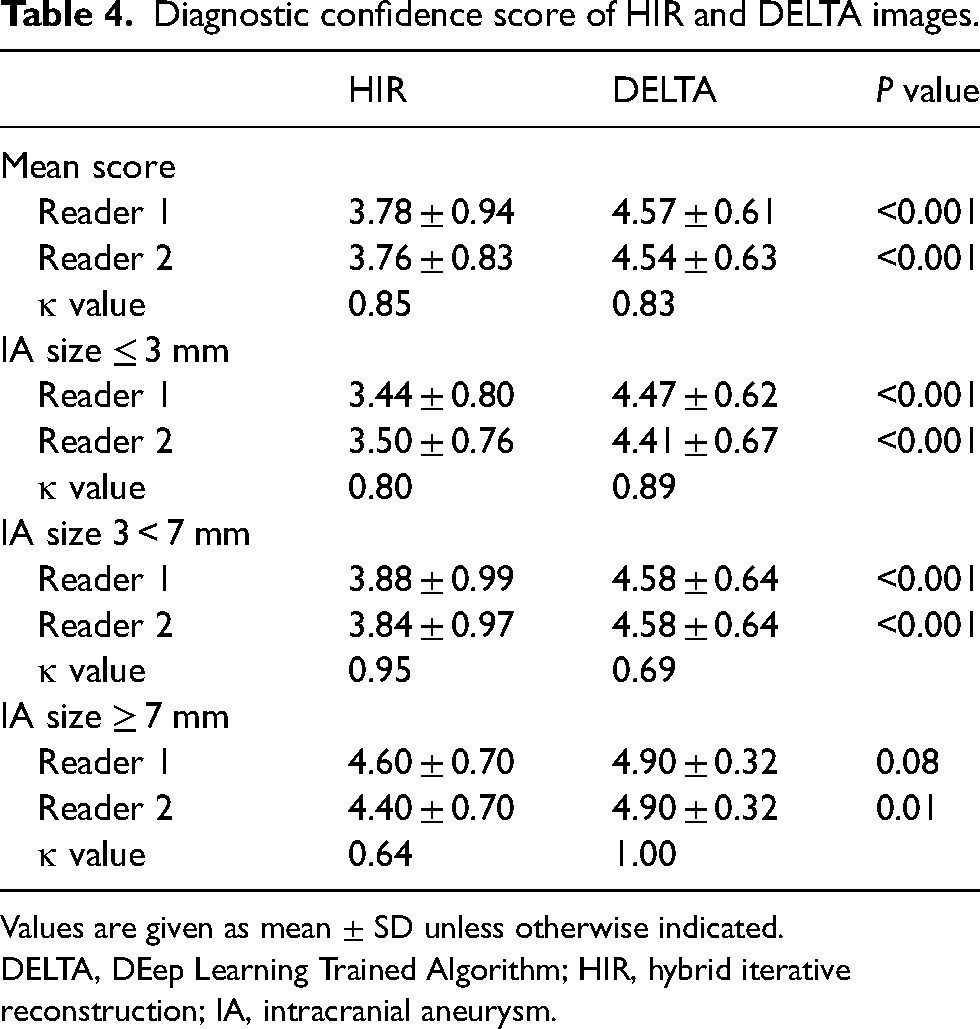
Values are given as mean ± SD unless otherwise indicated.
DELTA, DEep Learning Trained Algorithm; HIR, hybrid iterative reconstruction; IA, intracranial aneurysm.
For IAs in all three size groups, the DELTA images received significantly higher diagnostic confidence scores compared to the HIR images by both readers, with significant difference observed (all P < 0.001) except for IAs with a size ≥7 mm by reader 1 (P = 0.08). The improvement of diagnostic confidence, therefore, seemed to be most profound in IAs with a size ≤3 mm, where the mean scores for HIR and DELTA were 4.5 ± 0.6 versus 3.4 ± 0.8 and 4.4 ± 0.7 versus 3.5 ± 0.8 by the two readers (both P < 0.001), respectively, which was logical, owing to the superior vessel delineating ability and improved image quality of DELTA. An example case is shown in Fig. 4, where the left ICA aneurysm with size <2 mm was hardly detectable on the HIR images for the blurred boundary and the poor contrast with surrounding tissues, but sufficiently clear on the DELTA images owing to the sharp delineation of boundary and high contrast. Therefore, both radiologists showed an increase in diagnostic confidence, from score 2 on the HIR image to score 4 on the DELTA image.
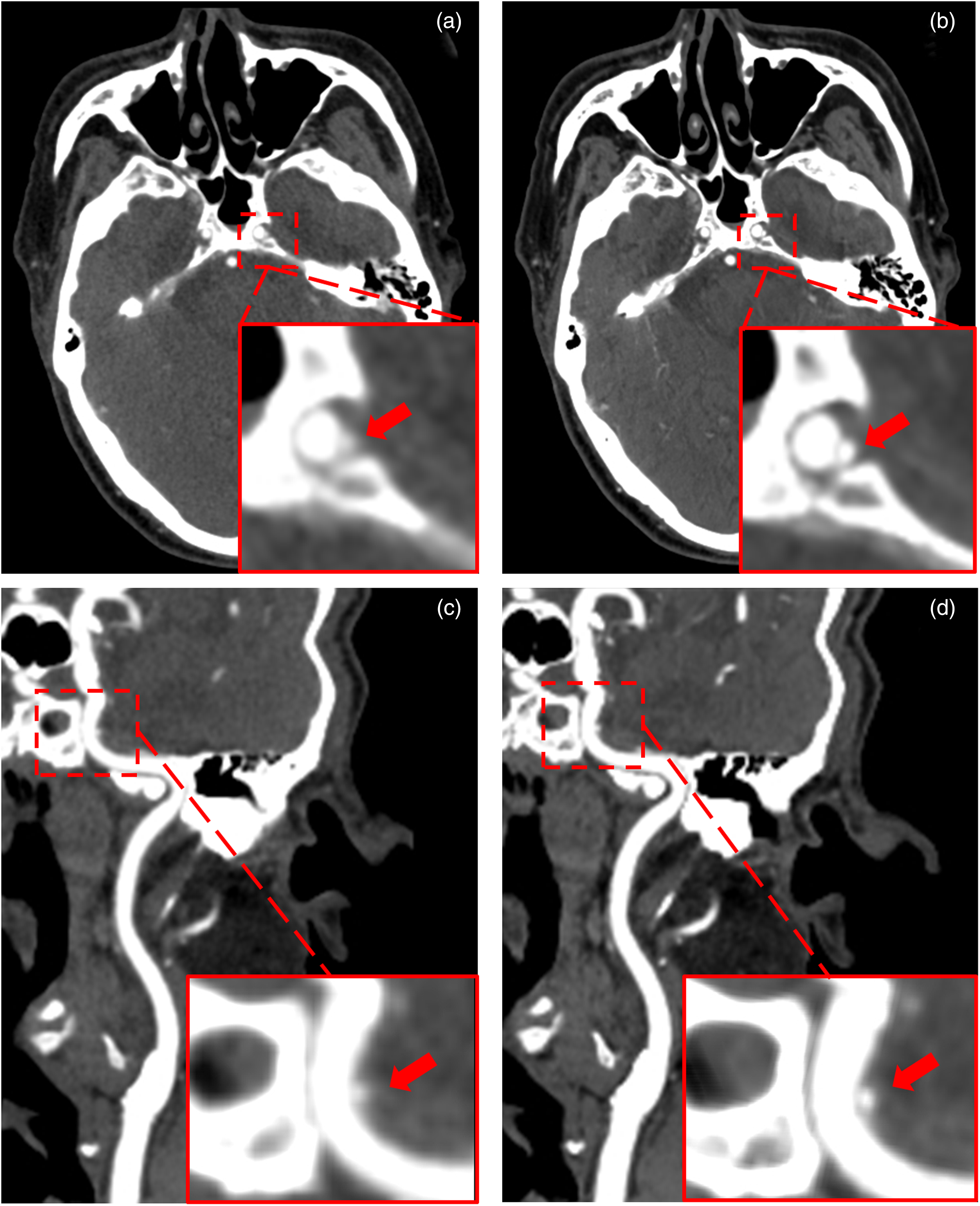
Craniocervical CTA of an 83-year-old man with a tiny aneurysm (size < 2 mm) in the left internal carotid artery (red arrow): (a) the HIR and (b) DELTA image on the axial plane; and (c) curved planer reformation of the HIR and (d) the DELTA images. The diagnostic confidence was grade 2 and 4 by both radiologists for the HIR and the DELTA images, respectively (window W/L = 550/150 HU). CTA, computed tomography angiography; DELTA, DEep Learning Trained Algorithm; HIR, hybrid iterative reconstruction.
An overview of the distribution of the diagnostic confidence was illustrated in Fig. 5. For both readers, four IAs with score 2 on the HIR images were raised to score ≥3 on the DELTA images. All IAs on DELTA images were scored ≥3 and were considered sufficient for clinical diagnosis. In addition, the proportion of IAs with a high score (≥4) enlarged from 54.4% (37/68) to 94.1% (64/68) and from 58.8% (40/68) to 92.7% (63/68) by the two readers, respectively.
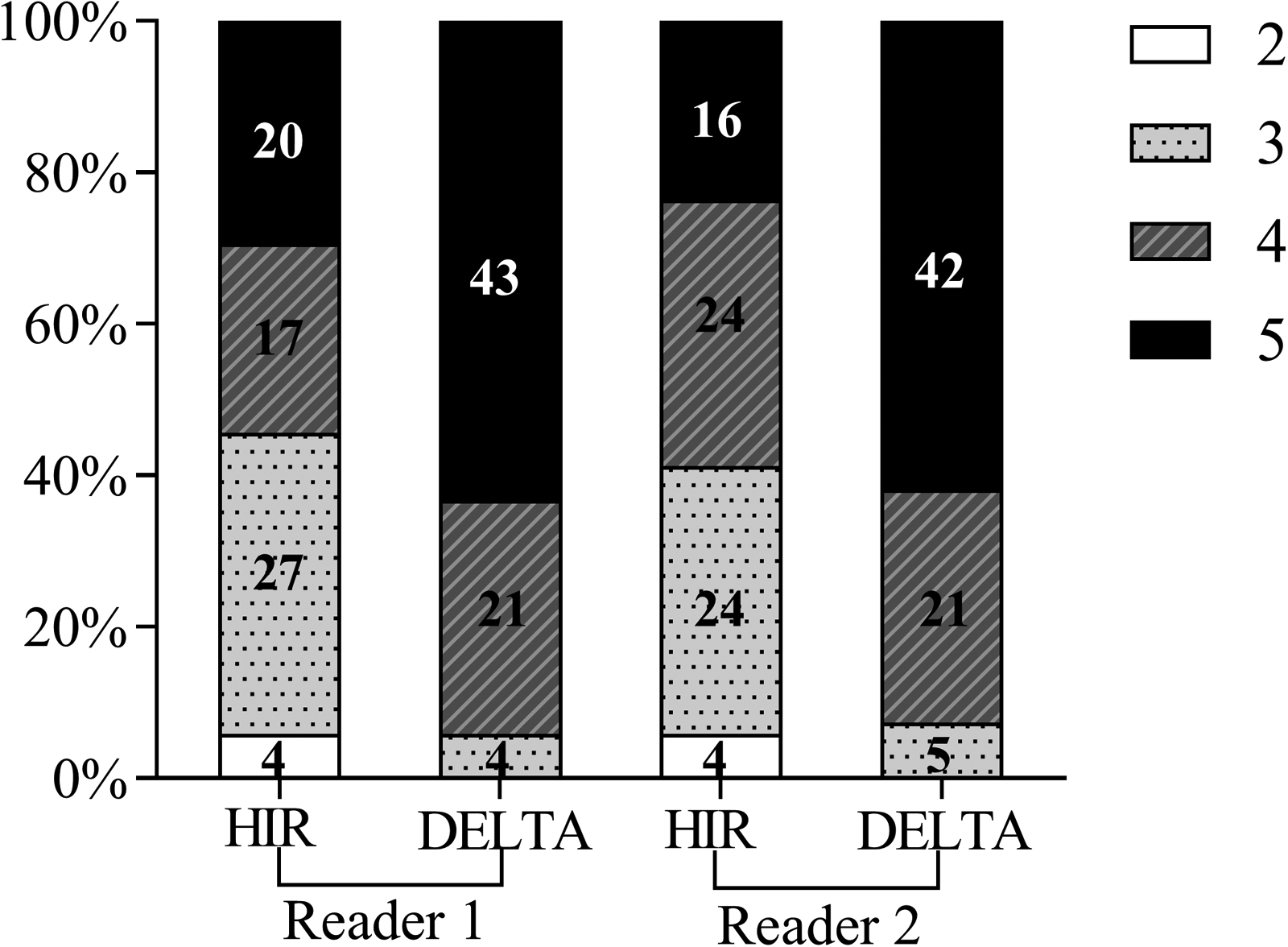
Distribution of diagnostic confidence by two radiologists on HIR and DELTA images. DELTA, DEep Learning Trained Algorithm; HIR, hybrid iterative reconstruction.
Discussion
In this study, we evaluated the performance of DELTA in craniocervical CTA on image quality and diagnostic confidence of intracranial aneurysms. Results revealed that DELTA images yielded significantly lower image noise and higher SNR and CNR than HIR images. All five subjective image quality metrics were scored higher on DELTA images than on HIR images by both radiologists. In addition, higher average diagnostic confidence on DELTA images was found, especially for IAs with a size ≤3 mm.
DLR has shown the potential to outperform current reconstruction algorithms in recent years (12). Previous studies have demonstrated the clinical value of DELTA in liver and chest CT (15,16). Cao et al. (15) reported that low-dose chest CT with DLR improved image quality and lung nodule detectability compared to low-dose HIR. Zeng et al. (16) demonstrated that, apart from the image quality, half-dose enhanced liver CT with DELTA was comparable to routine-dose images with HIR in lesion detectability, where the sensitivity and specificity were 81.9% versus 83.7% and 89.1% versus 86.3%, respectively. They also added in the discussion that, for visualization of abnormal findings, no remarkable difference was observed in the distribution of subjective scores for liver lesions, gallstones, or hepatic calcifications between the low-dose images with DELTA and the routine-dose images with HIR. Our results revealed that the DELTA improved the visibility of small vessels, so it may benefit the diagnosis of SAH-related vasospasm or the observation of collaterals in the setting of ischemic stroke, which would be interesting for investigation in the future.
Due to the lack of DSA in the majority of the enrolled cases, where the patient may have chosen for various reasons to follow up on the indication of IA at other institutions, it was not possible to conduct a complete detection test for evaluating the diagnostic accuracy within the present investigation. Fortunately, the detection of IA, for its distinctive morphological exhibition, depends mostly on the stage of development, and the chance of misdiagnosis should be rather low once it has reached a considerable size. In comparison, it is more challenging to determine whether it poses an imminent risk or resides in a critical position that requires timely surgical intervention. In this perspective, the value of the DLR algorithm, rather than revealing IAs that would have been missed on the current HIR images, has been reflected in its ability to depict a more complete and more detailed intracranial vasculature with suppressed image noise and improved lesion conspicuity, which was the reason for having scored superior diagnostic confidence.
How to effectively keep the radiation dose as low as reasonably achievable has also been an ongoing topic for CTA. However, striking a balance between dose reduction and acceptable levels of diagnostic accuracy was a more significant issue. In our institution, although a routine craniocervical CTA protocol was used, a lower dose was found than previously reported (14,19) (CTDIvol: 7.61 ± 0.51 vs. 9.67 ± 1.14 mGy), suggesting the potential to further reduce radiation dose while maintaining diagnostic image quality in future research.
Management options for patients with IAs may include surveillance, placement of a flow diverter or other intrasaccular device, coil embolization, and surgical clipping. The recommended options depend on a variety of patient and IA characteristics. In cases where patients have undergone coil embolization or surgical clipping, beam-hardening, and metal artifacts due to the coils or clips generally preclude visualization of the IA and may even adversely affect the image quality of the adjacent parent artery. It was essential to minimize the artifacts for better diagnosis. Although the performance of DELTA in removing metal artifacts was not investigated in this study, we did find that DELTA was able to suppress the artifacts to some extent in a few postoperative patients, especially in the anterior and posterior fossae. Therefore, joining the DLR with metal artifact correction might be an interesting topic worth further investigation.
The present study has some limitations. First, the investigation was conducted only in the routine dose setting that we believed to be most relevant in practice, although the DLR algorithm has been proven powerful for low-dose CT. Second, the DELTA algorithm was only one implementation of the DLR algorithms, for which the reproducibility of the findings remained of interest to further explorations. Third, we in this study focused only on IA while other observations of the craniocervical region were also involved in the diagnostic process, on which the impact of DELTA could be even more profound, such as on non-vascular areas where noise is the most dominating factor. Fourth, the impact of the display window (W/L) is not trivial in diagnosing the IA, where the measured size of the aneurysm may be slightly different under a different window setting. Finally, bias due to the different image appearance of the two algorithms remained inevitable and must be considered when interpreting the subjective results.
In conclusion, the DELTA was found potentially capable of improving the image quality and the associated confidence in diagnosing intracranial aneurysm, particularly for those with a size ≤3 mm compared to the currently used HIR, and may be worth considering adopting in routine craniocervical CTA applications.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: TW and GZ are employees of United Imaging Healthcare. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Key Projects of Shanghai Jiading District Health Commission (grant nos. 2020-ZD-04) and the Key Discipline Construction Project of Jiading District Health System (grant nos.2020-jdyxzdzk-02).