
Abstract
Background
In children and young adults, tumors in the chest and thoracic wall exhibit a wide variety of types, making it challenging to differentiate between benign and malignant cases before invasive histopathological examination.
Purpose
To evaluate the utility of apparent diffusion coefficient (ADC) for discriminating malignant thoracic masses in children and young adults.
Material and Methods
This retrospective study included chest magnetic resonance imaging (MRI) scans in patients aged <30 years. Patients' age and sex, tumor location (mediastinum or thoracic wall), tumor size, MR characteristics including necrosis or hemorrhage, and ADC values were assessed.
Results
Malignant masses were found in older patients (mean age = 18.0 ± 8.1 vs. 10.6, ± 9.1 years; P = 0.008), had lower mean ADC values (0.765 ± 0.298 vs. 2.051 ± 0.855 × 10−3 mm2/s; P < 0.001), and showed more internal hemorrhage (6/12 vs. 17/86; P = 0.031) compared to benign masses. Univariate and multivariate regression analyses also showed significant differences in age, tumor size, and ADC values. In the diagnostic performance analysis, age (area under the receiver operating characteristic curve [AUC] = 0.723, 95% confidence interval [CI] = 0.624–0.809; P = 0.004) and ADC mean value (AUC = 0.941, 95% CI = 0.874–0.978, P < 0.001) were significant. The optimal cutoff values were 13 years for age (sensitivity = 83.3%, specificity = 61.6%) and an ADC mean of 1.196 × 10−3 mm²/s (sensitivity = 100%, specificity = 86.1%) for discriminating malignant from benign thoracic masses.
Conclusion
When evaluating thoracic masses in children and young adults, older age and lower ADC values help identify malignancy.
Introduction
In children and young adults, mediastinal and thoracic wall masses show a wide spectrum of histopathological characteristics. With the mediastinum being the most common location of thoracic masses in children, mediastinal masses can range from non-vascular to vascular tumors, including congenital lesions, inflammation, and benign and malignant tumors (1). In comparison, thoracic wall masses are relatively uncommon and include vascular, peripheral nervous, osseous, cartilaginous, or adipose lesions that can benign or malignant (2). This multitude of characteristics possibly makes initial diagnosis difficult. Some lesions share similar characteristics but can be benign or malignant depending on cellular differentiation (3–5). Even though an exact diagnosis must eventually be made, initial discrimination of malignancy is important for expedient treatment.
Magnetic resonance imaging (MRI) is a non-invasive diagnostic method with excellent soft tissue differentiation. Diffusion-weighted imaging (DWI) is an MRI technique used to detect the free movement of water in tissue microstructures that provides valuable information for differentiating malignant masses (6,7). The apparent diffusion coefficient (ADC) can be calculated from a series of diffusion MR images at different b-values. Previous studies on lung cancer, mediastinal masses (8,–14), pleural lesions (15,16), and thoracic wall lesions (6,17) reported low ADC values in malignant lesions. However, there are few studies about the utility of ADC for differentiating thoracic masses that include both mediastinal and thoracic wall lesions in children.
The aim of the present study was to identify imaging factors that could differentiate malignant masses in chest MRI including both mediastinal and thoracic wall lesions in children and young adults and to evaluate whether ADC values could be used to effectively discriminate malignancy.
Material and Methods
Patients and clinical data
We included all consecutive chest MRI scans performed at our institution between January 2000 and December 2023 from patients aged 29 years and younger. Patients were classified into the benign or malignant mass group based on pathology or clinical follow-up.
Clinical data, including age, sex, and pathologic diagnosis, were retrospectively collected from electronic medical records and pathology reports of our institution. The final diagnoses of thoracic masses were based on histopathological examination for all malignant lesions and some benign lesions. Clinical course, including follow-up imaging studies recorded in electronic medical records, was also used to diagnose benign lesions.
MRI acquisition
Chest MRI was performed using either a 1.5-T or 3.0-T system with numerous machines. MRI studies varied in sequence during the 23 years covered in this study. However, most studies consisted of axial, coronal, and sagittal T1- and T2-weighted images, in-and-out phase images or T1-fat-saturated images, and DWI with several b-values. The b-values used in DWI were in the range of 3–10 for each patient. Chest MRI examinations were performed using a 1.5-T scanner in 44 patients and a 3.0-T scanner in 54 patients. Two b-values were used in 13 cases, three b-values in 45 cases, four b-values in eight cases, and 10 b-values in 32 cases. The maximum b-value was 800–1500. ADC maps were automatically created based on calculations made using diffusion images.
For patients who had multiple chest MRI scans, only the initial examination before treatment or surgery was included in the analysis. We included MRI studies with and without contrast enhancement. We excluded cases with no available DWI, severe artifacts in DWI, or no mass lesion. Lipomas were not included in this study because of their classic appearance on conventional MR and the fat-saturated pulse that was used on DWI.
Radiologic analysis
Two radiologists (HJL and ML with 5 and 19 years of experience in pediatric MRI, respectively) from our institution reviewed the images in consensus to define the boundaries of the region of interest (ROI), excluding the necrotic or hemorrhagic portions within the lesion. Tumor location was classified as either the mediastinum or the thoracic wall. The tumors were classified based on the location of their center. There was no case of lung lesions. Tumor size was defined as the longest diameter of the lesion in multiplanar imaging, including axial, coronal, and sagittal planes. The MR images were also reviewed for the cystic or necrotic component and the presence of hemorrhage in the tumor. To measure ADC values, maximum ROIs were drawn in the lesion excluding the necrotic or hemorrhagic portion. We obtained the mean value of ADC (ADCmean), minimum value of ADC (ADCmin), and maximum value of ADC (ADCmax) simultaneously.
Statistical analysis
Statistical analyses were performed using SPSS version 25 (IBM Corp., Armonk, NY, USA) and MedCalc version 18.6 (MedCalc Software, Ostend, Belgium). Continuous variables were rounded to the nearest tenths and categorical variables were summarized as frequencies and percentages. To compare continuous variables, a normality test using the Shapiro–Wilk test and t-test was performed. To compare categorical variables, the chi-square test or Fisher's exact test was performed. Logistic regression analysis was used to find relevant variables indicating malignancy. An area under the receiver operating characteristic curve (AUC) analysis was performed to assess diagnostic ability. For continuous variables, the best cutoff points were determined based on Youden's index. Statistical significance was defined with a two-sided P value < 0.05.
Ethics statement
This retrospective study was conducted in accordance with the ethical guidelines of the Declaration of Helsinki using patient data and MRI images. The present study protocol was reviewed and approved by the Institutional Review Board of our institution (approval no. 4-2021-0631) and the requirement for informed consent was waived.
Results
Patients, tumor pathology, and MR protocols
Among the 138 consecutive chest MRI studies performed during the study period, 40 exams were excluded due to chemotherapy status (n = 8), lack of DWI (n = 22), severe artifacts in DWI (n = 3), no mass lesion (n = 5), and lipoma diagnosis (n = 2). Finally, 98 patients (51 boys/men, 47 girls/women; age range = 0–29 years; mean age = 11.5 ± 9.2 years) with 98 chest MRI studies were included.
In this study, a total of 48 mediastinum masses and 50 thoracic wall masses were examined. In mediastinum masses, eight were malignant tumors and 40 were benign lesions. The malignant lesions of mediastinum were malignant germ cell tumor (n = 4), lymphoma (n = 2), neuroblastoma (n = 1), and thymic adenocarcinoma (n = 1). The benign lesions of mediastinum were mature teratoma (n = 7), ganglioneuroma (n = 6), lymphangioma (n = 5), bronchogenic cyst (n = 3), thymic hyperplasia (n = 4), normal thymus (n = 3), schwannoma (n = 2), pulmonary sequestration (n = 2), leiomyoma (n = 2), thymoma (n = 1), lymphadenitis (n = 1), ganglioneuroblastoma (n = 1), congenital pulmonary airway malformation (n = 1), hematoma (n = 1), and duplication cyst (n = 1). In thoracic wall tumors, four were malignant tumors and 46 were benign lesions. The thoracic wall malignant lesions were dermatofibrosarcoma (n = 4). The benign lesions of thoracic wall were hemangioma (n = 8), lymphangioma (n = 16), benign vascular tumor (n = 5), neurofibroma (n = 4), osteochondroma (n = 3), neurogenic tumor (n = 2), aneurysmal bone cyst (n = 1), angiolipoma (n = 1), fibrous dysplasia (n = 1), mature teratoma (n = 1), pilomatricoma (n = 1), proliferative myositis (n = 1), chronic osteomyelitis (n = 1), and venolymphatic malformation (n = 1).
Group comparison between the benign and malignant masses
The clinical and radiologic characteristics of the two groups are summarized in Table 1. Mean age was older in the malignant group (18.0 ± 8.1 vs. 10.6 ± 9.1 years; P = 0.008). Sex percentage did not differ between the malignant and benign groups.
Clinical and radiologic features compared between benign and malignant masses in the thorax.
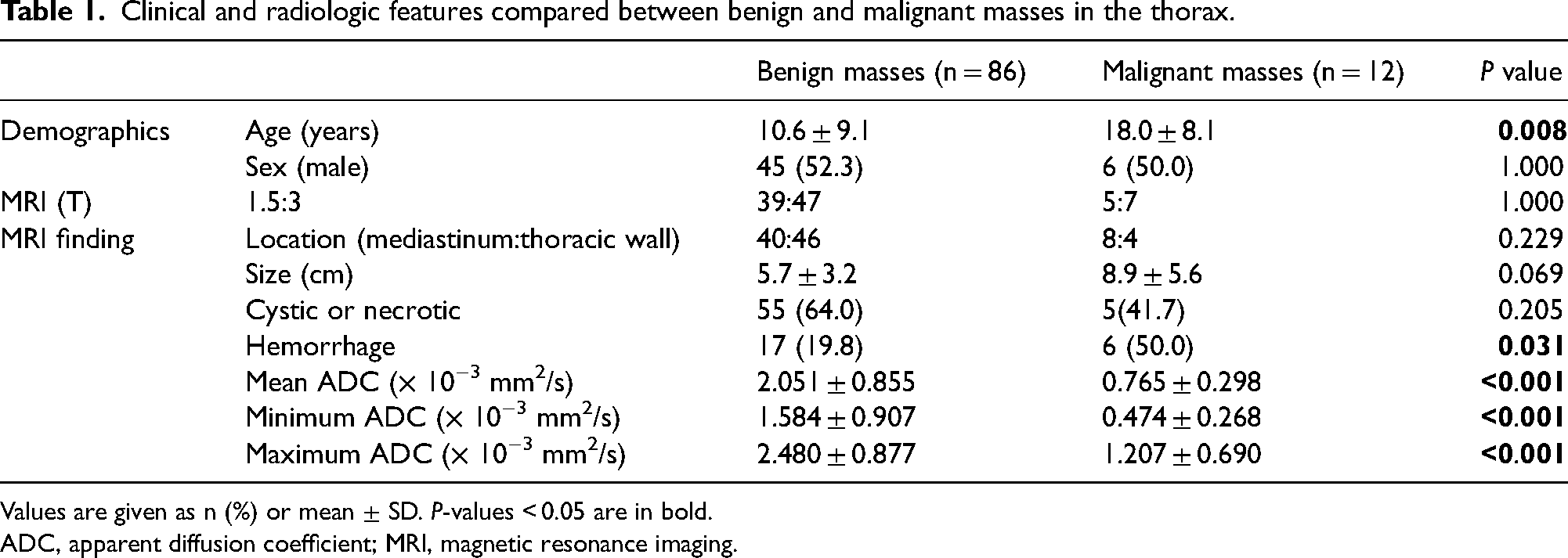
Values are given as n (%) or mean ± SD. P-values < 0.05 are in bold.
ADC, apparent diffusion coefficient; MRI, magnetic resonance imaging.
There was no difference in MR strength (1.5 T vs. 3.0 T) between the benign and malignant groups (Table 1). Of the 98 cases, 48 were located in the mediastinum and 50 in the thoracic wall. Hemorrhage was more commonly observed in malignant masses (50% [6/12] vs. 19.8% [17/86]; P = 0.031). The tumor location (mediastinum or thoracic wall), tumor size, and presence of a cystic or necrotic portion were not different between the two groups. On the ADC analysis, there was no case of ADC calculations failing. The ADC values were lower in the malignant group for all mean, minimum, and maximum values (all P ≤ 0.001).
We also performed a subgroup comparison regarding tumor location (Fig. 1). Among masses located at the mediastinum, malignant masses were larger in size than benign masses (12.2 ± 3.5 vs. 5.5 ± 3.0 cm; P < 0.001). Hemorrhage was also more common in malignant tumors (75% [6/8] vs. 17.5% [7/40]; P = 0.003). However, age, sex, and presence of cystic portion were not different between benign and malignant masses in mediastinal tumors. Among masses located at the thoracic wall, more malignant masses were observed in older patients (23.3 ± 6.5 vs. 8.9 ± 8.6 years; P = 0.002), had a smaller size (2.5 ± 0.6 vs. 5.8 ± 3.4 cm; P < 0.001), and showed fewer cystic or necrotic portions (0% [0/4] vs. 67.4% [31/46]; P = 0.017). However, sex and presence of hemorrhage were not different between benign and malignant masses in thoracic wall tumors. In ADC analyses, malignant masses had lower ADC mean values than benign masses for both mediastinal (0.681 ± 0.322 vs. 2.041 ± 0.808 × 10−3 mm2/s; P < 0.001) and thoracic wall (0.933 ± 0.161 vs. 2.059 ± 0.902 × 10−3 mm2/s; P < 0.001) tumors (Figs. 1–3).
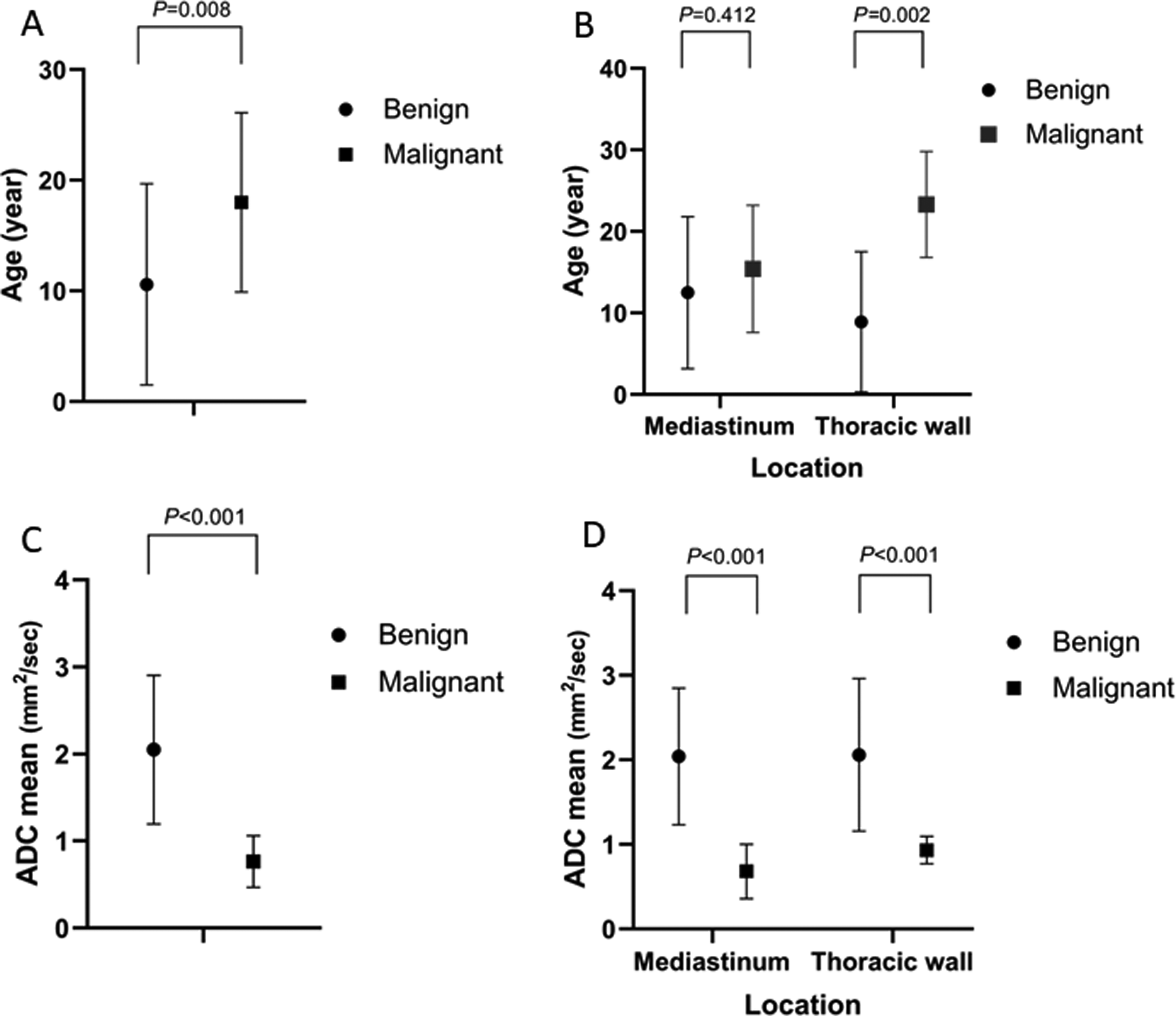
Comparison of radiologic factors differentiating malignant and benign masses in chest MRI. (a, b) The graphs show the mean values and their range of standard deviation of (a) patient's age and subgrouped by (b) tumor location in benign and malignant masses in chest MRI. Malignant masses were more common in older patients for all tumors (18.0 ± 8.1 vs. 10.6 ± 9.1 years; P = 0.008) and in thoracic wall tumors (23.3 ± 6.5 vs. 8.9 ± 8.6 years; P = 0.002). (c, d) The graphs show the mean values and their range of standard deviation of (c) the apparent diffusion coefficient (ADCmean) and subgrouped by (d) tumor location in benign and malignant masses in chest MRI. ADCmean was lower in malignant masses than in benign masses of all tumors (mean = 0.765 ± 0.298 vs. 2.051 ± 0.855 × 10−3 mm2/s; P < 0.001). In the subgroup analysis by location, ADCmean was lower in mediastinal tumors (0.681 ± 0.322 vs. 2.041 ± 0.808 × 10−3 mm2/s; P < 0.001) and in thoracic wall tumors (0.933 ± 0.161 vs. 2.059 ± 0.902 × 10−3 mm2/s; P < 0.001). ADC, apparent diffusion coefficient; AUC, area under the receiver operating characteristic curve; MRI, magnetic resonance imaging.
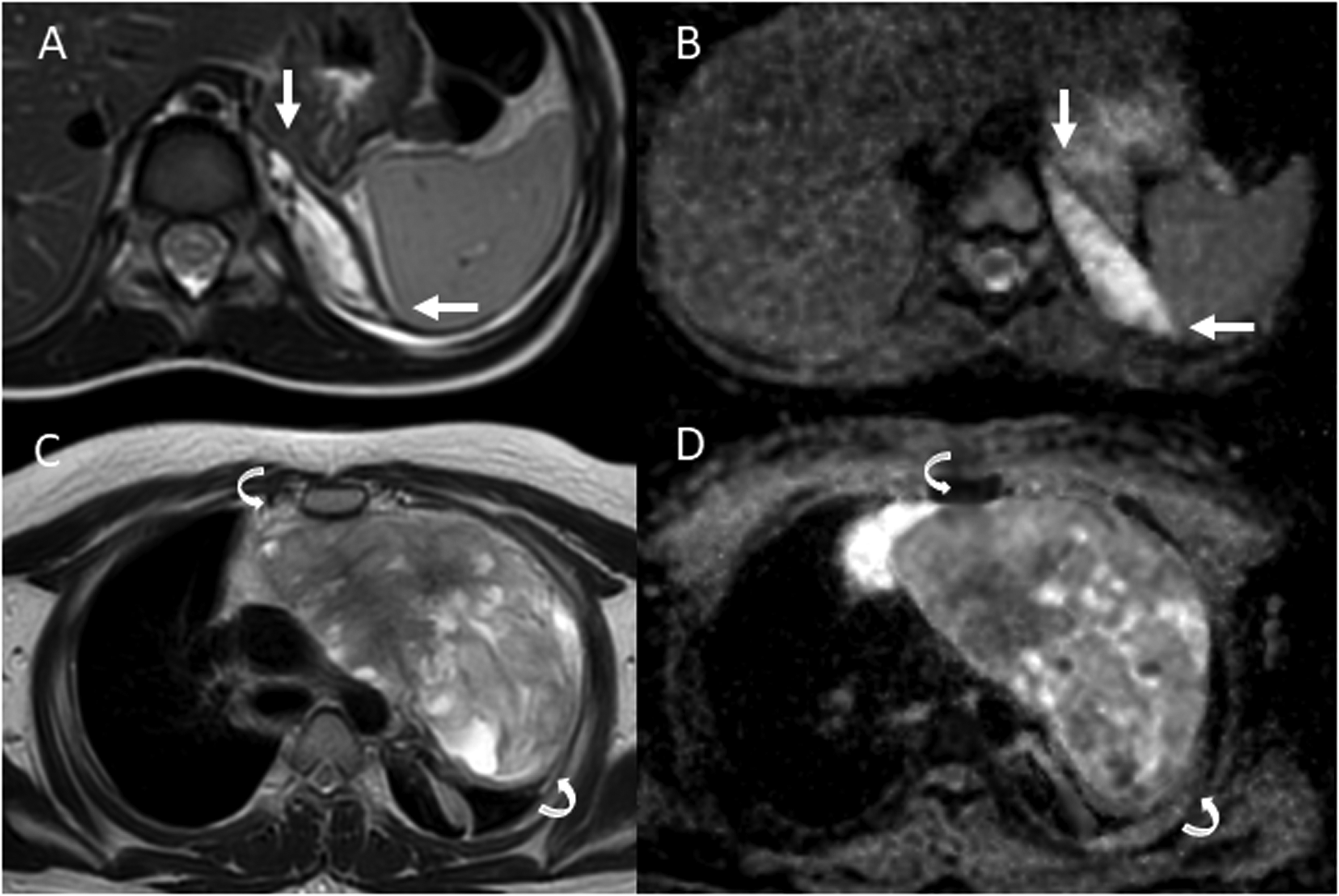
Representative cases of benign and malignant masses in the mediastinum tumors. (a, b) A 2-year-old boy with a benign mass (arrows) at the left posterior mediastinum. The mass was 4.2 cm and the chest MRI image shows (a) T2 high signal intensity and (b) high mean ADC value of 2.355 × 10−3 mm2/s. The pathological diagnosis was pulmonary sequestration. (c, d) A 14-year-old boy with a malignant mass (curved arrows) at the anterior mediastinum. The mass was huge as 20.1 cm and the chest MRI image shows (c) heterogeneous T2 intermediate to high signal intensity and (d) low mean ADC value of 1.073 × 10−3 mm2/s. The pathological diagnosis was a yolk sac tumor.
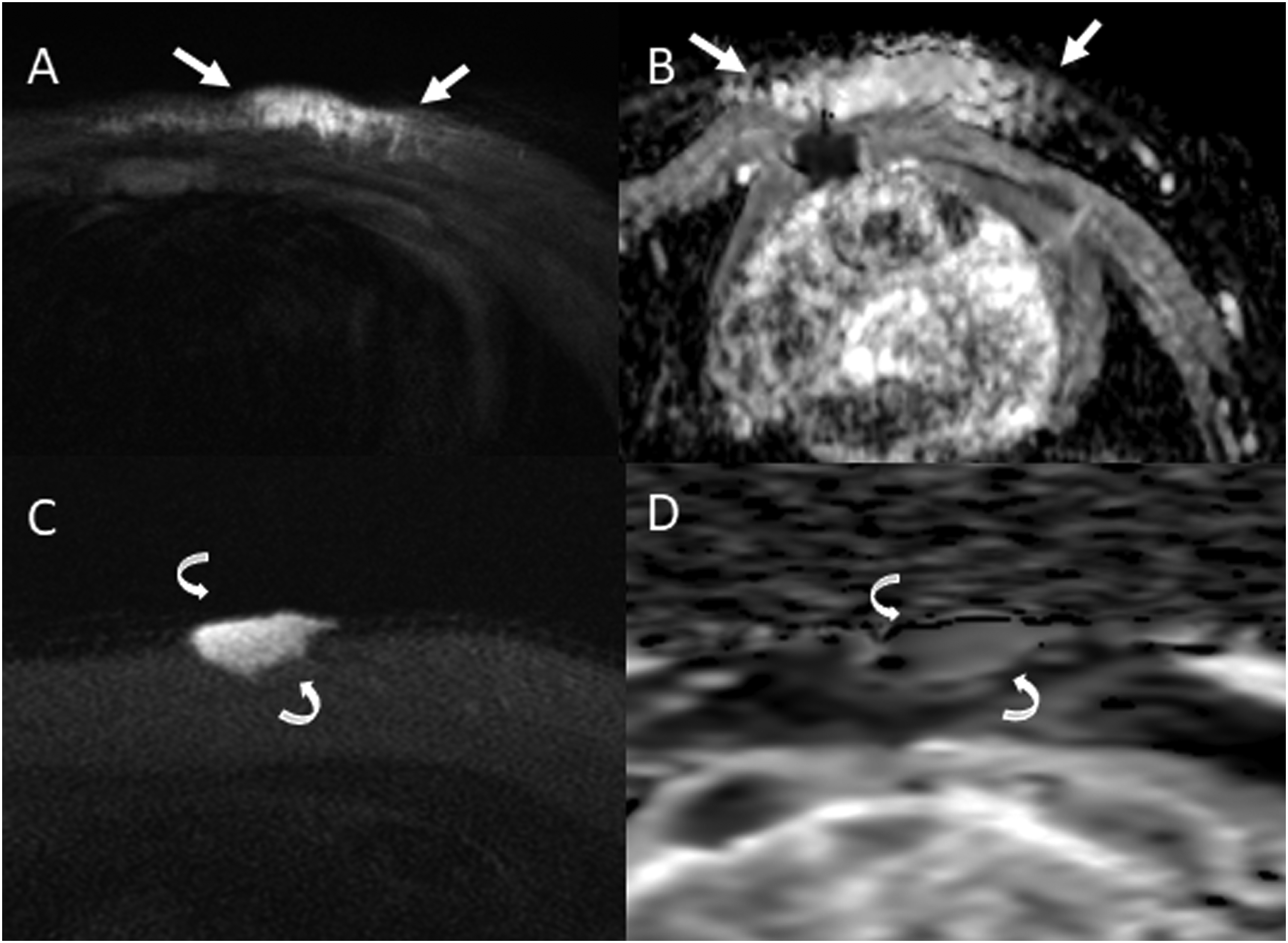
Representative cases of benign and malignant masses in the thoracic wall tumors. (a, b
Logistic regression analysis
In the univariate analysis, age, tumor size, and ADC values were statistically significant factors implying malignancy (Table 2). Due to the high correlation between the three ADC values (mean, minimum, and maximum), we selected ADCmean for the multivariate analysis. In the multivariate analysis using forward conditional logistic regression, age (odds ratio [OR] = 1.194, 95% confidence interval [CI] = 1.019–1.400; P = 0.029), tumor size (OR = 1.489, 95% CI = 1.035–2.141; P = 0.032), and ADC mean (OR = 0.007, 95% CI = 0.000–0.174; P = 0.003) were the significant factors indicating malignancy.
Logistic regression analyses of thoracic masses for diagnosing malignant masses.
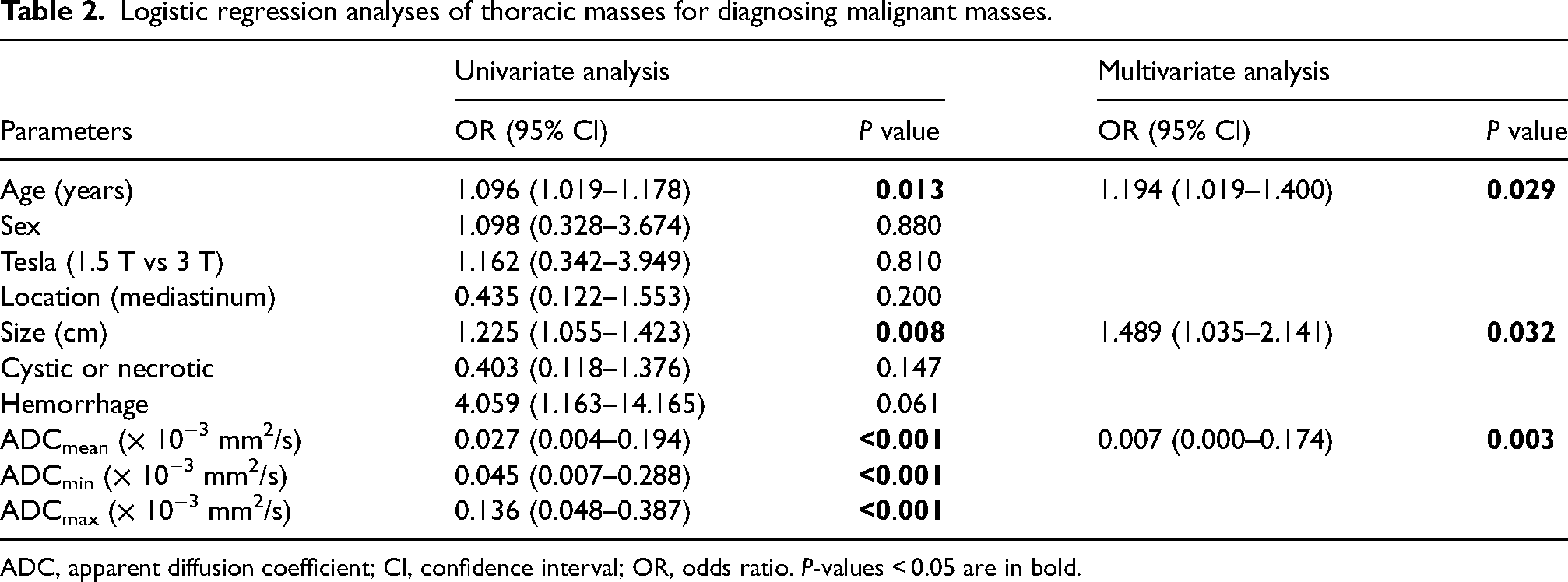
ADC, apparent diffusion coefficient; CI, confidence interval; OR, odds ratio. P-values < 0.05 are in bold.
Diagnostic performance
In the AUC analysis, age (AUC = 0.723, 95% CI = 0.624–0.809; P = 0.004) and ADCmean (AUC = 0.941, 95% CI = 0.874–0.978; P < 0.001) showed good discrimination for malignancy (Table 3). In a pairwise comparison of the ROC curves, the ADCmean value showed a higher diagnostic value than that of age (difference between areas = 0.218, 95% CI = 0.055–0.380; P = 0.009) and size (difference between areas = 0.292, 95% CI = 0.061–0.523; P = 0.013). Using the Youden index, determined cutoff values were age 13 years showing a sensitivity of 83.3% and specificity of 61.6%, and ADCmean of 1.196 × 10−3 mm2/s showing a sensitivity of 100% and specificity of 86.1% (Fig. 4).
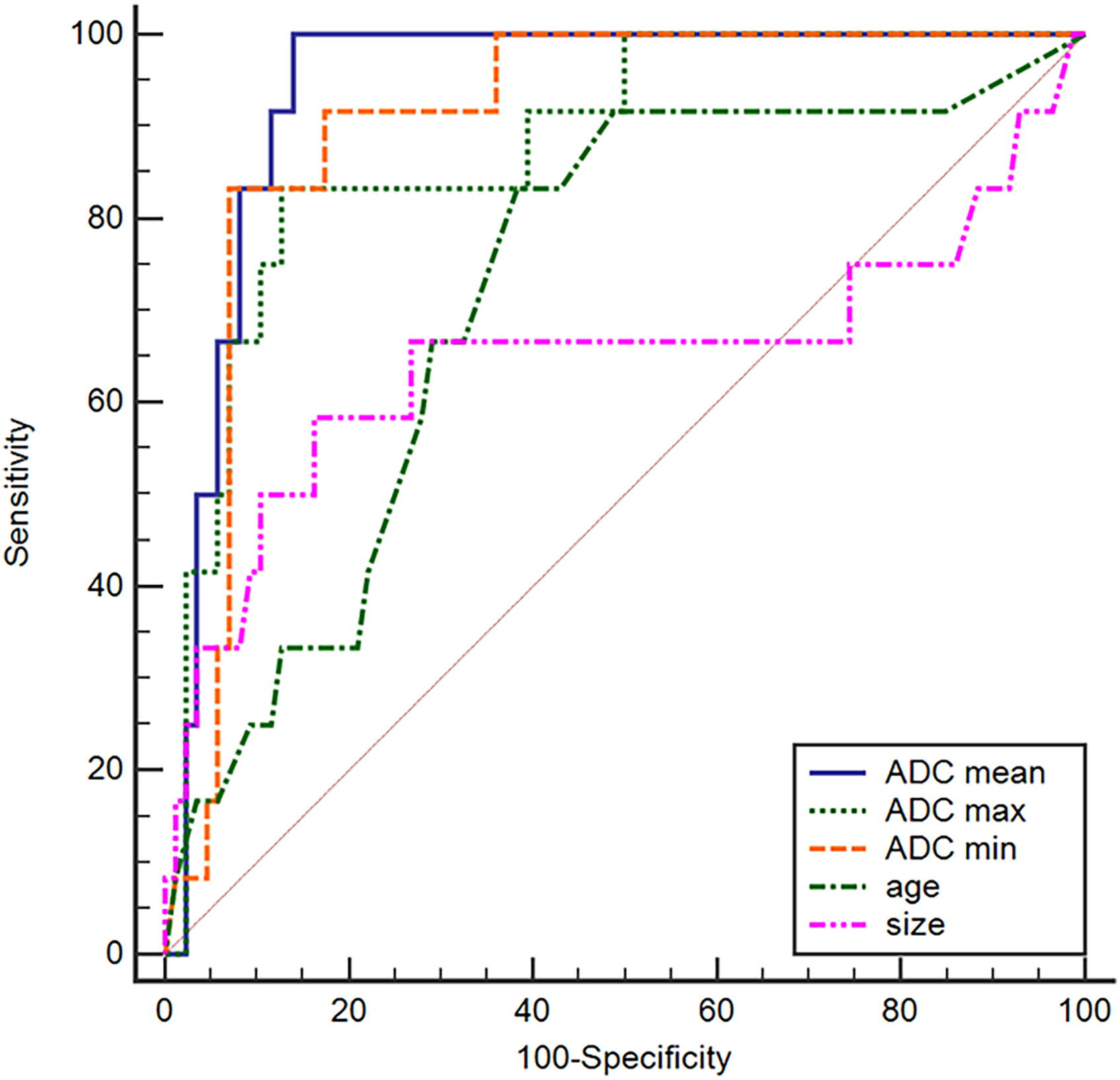
The receiver operating characteristic curve analysis for age, tumor size, and ADC values for differentiating malignant masses in chest MRI. The diagnostic performance of the mean ADC value (ADCmean) was higher than that of age (P = 0. 009) or size (P = 0.013). ADC, apparent diffusion coefficient; MRI, magnetic resonance imaging.
Diagnostic performances of age, tumor location, tumor size, and minimum ADC value (ADCmin) for differentiating malignant masses in chest MRI.
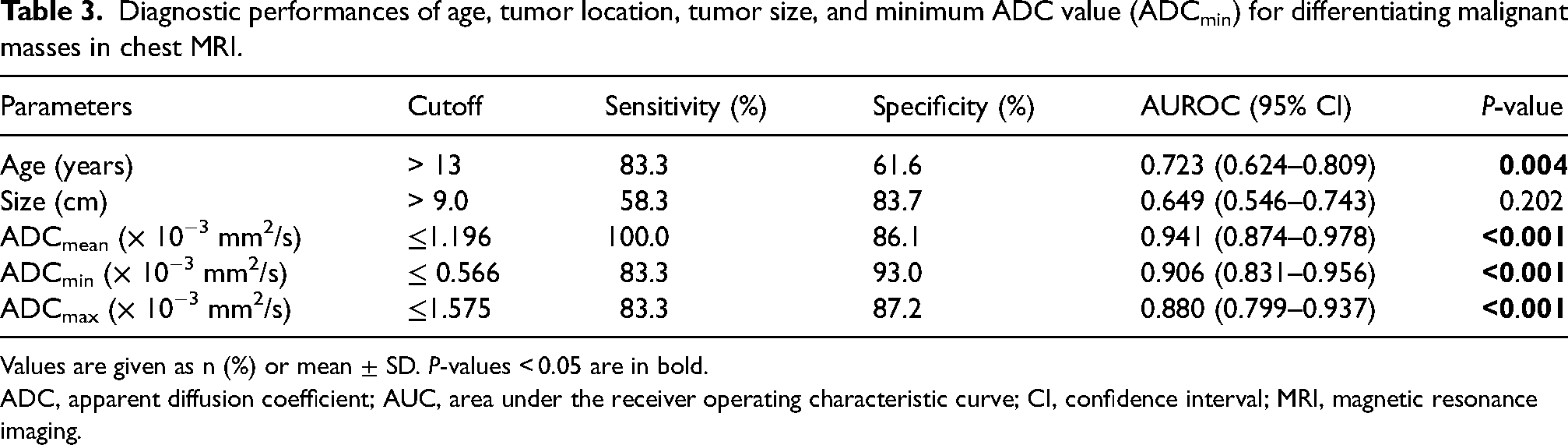
Values are given as n (%) or mean ± SD. P-values < 0.05 are in bold.
ADC, apparent diffusion coefficient; AUC, area under the receiver operating characteristic curve; CI, confidence interval; MRI, magnetic resonance imaging.
Discussion
There are a variety of chest tumors involving the mediastinum and/or thoracic wall in children and young adults. Chest MRI is useful for evaluating lesion extent and characteristics, but little is known about the utility of ADC for discriminating benign and malignant masses in these patients. Our study showed that older age and low ADCmean value can differentiate malignant masses in mediastinum and thoracic wall. Age older than 13 years and low ADCmean value with a cutoff of 1.196 × 10−3 mm2/s were good discriminators of malignancy.
Age and tumor location are effective clinical information when evaluating thoracic masses in children and young adults. If there is a mediastinal tumor, we need to further classify its location to the anterior, middle, and posterior mediastinum and a differential diagnosis can be made according to patient age (1,3). Lymphoma, the most common malignancy in the anterior and middle mediastinum, usually occurs in adolescents and young adults. Germ cell tumors, which are another common tumor in the anterior mediastinum, show a bimodal age distribution in infancy and adolescence. Neurogenic tumors, including neuroblastoma, are common in the posterior mediastinum and usually occur in children aged under 3 years. However, there are many other differential diagnoses, including congenital lesions, and a broad disease spectrum from benign to malignant can be observed for germ cell tumors and neurogenic tumors when evaluating mediastinal tumors. Thoracic wall tumors are less common in children and malignancies are mostly bone tumors that can also happen across all age groups (2,18). Osteosarcoma and Ewing sarcoma are common at adolescence and skeletal metastasis is rare but can still develop at any age.
Our study showed that age above 13 years was associated with malignancy. However, tumor location was not a significant factor. The clinical meaning of age could differ according to a tumor's location and characteristics. In our study population, we included congenital lesions such as lymphangioma in the benign category, which are usually diagnosed at a young age as palpable lesions in the thoracic wall. This could affect the results of our study. Therefore, having information on only age and tumor location might have limited value when differentiating benign and malignant masses among thoracic tumors in children and young adults.
Tumor size showed discrepant results according to the tumor location in our study. Malignant tumors were larger in mediastinal tumors, but smaller in thoracic wall tumors in our patients. Previous studies also showed that a large mass in the mediastinum indicates malignancy (3). For instance, if a mass larger than 5 cm is in the anterior mediastinum, malignancies such as malignant germ cell tumors or lymphomas are highly suspected. In addition, if the posterior mediastinal mass is large enough to invade other organs, malignant neurogenic tumors such as neuroblastoma are highly suspected (1,3,19). However, malignant tumors were smaller than benign tumors in thoracic wall masses, which is probably because thoracic wall masses are easily palpable and discovered early even when they are small.
In our research, ADC values were a significant factor indicating malignancy in the chest MRI of pediatric and young adult patients, both for mediastinal and thoracic wall masses. ADC values including ADCmean, ADCmin, and ADCmax were all significant factors indicating malignancy. Our results suggest an ADCmean of 1.196 × 10−3 mm2/s as the cutoff value. Malignant lesions show low ADC values due to the restricted movement of water molecules from increased cellularity, cellular pleomorphism, and disorganized neoangiogenesis (8,9,11,13). Most previous studies have focused on adults, and research on pediatric patients has been conducted on a small number of cases, limiting its clinical applicability. Mediastinal tumors and thoracic wall tumors require different differential diagnoses depending on age and location, making it necessary to analyze pediatric and adult cases separately.
Several studies showed low ADC values in malignant mediastinal tumors in adults; however, the suggested cutoff values had a wide range of 1.2–2.5 × 10−3 mm2/s (8,10,–12,13). Only one study discussed the ADC in pediatric mediastinal lesions (11). This past study was performed on 24 pediatric patients aged 5 months to 16 years and the suggested cutoff value was 1.2 × 10−3 mm2/s, which was similar to our cutoff value for ADCmin.
There are few studies about the ADC value for thoracic wall masses in children. The reported cutoff value for general soft tissue tumors in adults was 1.18–1.45 × 10−3 mm2/s (20,21). A recent study also showed that a cutoff ADC value for predicting malignancy was 1.058 × 10−3 mm2/s for bone tumors and 1.198 × 10−3 mm2/s for soft-tissue tumors in adults (22). However, only one study focused on the meaning of the ADC in pediatric musculoskeletal tumors (23). They evaluated the ADC value in 44 pediatric patients including 10 malignancies and the suggested cutoff value was 1.03 × 10−3 mm2/s with a sensitivity of 90% and specificity of 91%.
Our study included the largest number of patients of children and young adults and demonstrated excellent diagnostic performance of ADC values in diagnosing malignant thoracic masses, consistent with prior studies. These findings are expected to improve diagnostic accuracy in distinguishing benign from malignant tumors in ambiguous cases. In addition, in cases where a biopsy is performed, targeting areas with lower ADC values may help enhance the diagnostic accuracy of the biopsy.
The present study has some limitations. As this was a retrospective study based on data collected at a single center, patient selection might be biased and the number of patients insufficient. Moreover, chest MRI scans were attained with non-standardized sequences, especially the ADC map, which was obtained using diverse b-values performed on both 1.5-T and 3.0-T scanners during the 20-year study period. Because of this broad variability, we could not perform subgroup analyses based on different b-values. However, this heterogeneity of the MRI sequences may be a strength in terms of generalizing our findings, as it reflects the many situations that can come up in actual clinical practice. ADC values were gained by drawing ROIs on mass lesions and these ROIs can vary depending on the reviewer. Measurement variability was not examined in this study. However, we drew ROIs on what was judged to be the largest lesion area on consensus, so any differences might be negligible. We also could not evaluate the additional diagnostic values of the ADC in thoracic masses. Further study is needed for this topic. Lastly, we focused only on mediastinal and thoracic wall masses in children and young adults. However, tumors can also arise in other thoracic areas, such as the large airways or diaphragm. Future studies that include these areas would provide a more comprehensive understanding of thoracic masses in children.
In conclusion, chest MRI including DWI can help evaluate thoracic masses in pediatric and young adult patients. Age older than 13 years and low ADC values (ADCmean less than 1.196× 10−3 mm2/s) are significant factors indicating malignancy in this study population.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.