
Abstract
Background
Carotid artery stenting (CAS) is an interventional management in preventing ischemic stroke caused by carotid artery stenosis. After the treatment with CAS, in-stent restenosis caused by neointimal hyperplasia may develop.
Purpose
This study aims to obtain a better determination of neointimal hyperplasia using superb microvascular imaging (SMI), which provides a high-quality visualization of the endoluminal lesions, and to compare these results with B-mode and Doppler ultrasound (US).
Material and Methods
A total of 106 patients who underwent CAS in our interventional radiology unit between 2018 and 2020 were retrospectively analyzed. In total, 44 patients whose procedure images and post-procedural follow-up Doppler US and SMI data could be accessed were included.
Results
There were nine patients who had in-stent restenosis. One patient had no velocity increase; however, on SMI the measurements showed in-stent restenosis both in area and diameter. The other eight patients had a stenosis degree in the range of 50%–79% on Doppler US. Five patients had in-stent restenosis, both in Doppler US and SMI, by area and diameter measurements. Two patients underwent digital subtraction angiography (DSA).
Conclusion
We suggest that using SMI with duplex sonography improves detecting neointimal hyperplasia and in-stent restenosis. With SMI, better visualization of the stent lumen may improve the patient selection for DSA.
Introduction
Carotid artery stenting (CAS) is less-invasive interventional management in preventing ischemic stroke caused by carotid artery stenosis compared to carotid artery endarterectomy (CEA). Controlled trials have shown that both treatment methods have similar outcomes in preventing ischemic stroke (1,2). After CAS, restenosis may develop, and the restenosis rates in 2 years of follow-up after CEA and CAS are found to be 6.3% and 6%, respectively (3,4).
In-stent restenosis is caused by neointimal hyperplasia induced by the vessel trauma and chronic inflammation, which started at the placement of the stent (5). Neointimal hyperplasia can be seen as a hypoechoic thin layer inside the stent wall by B-mode ultrasound (US); however, it can be missed by radiologists using conventional B-mode carotid US. Superb microvascular imaging (SMI) is a new technique that provides high-quality visualization of the endoluminal lesions (6–8).
The aim of the present study was to obtain a better determination of neointimal hyperplasia using SMI and compare the results using B-mode US and Doppler US velocity criteria.
Material and Methods
A total of 106 patients who underwent CAS in our interventional radiology unit between 2018 and 2020 were retrospectively analyzed. In total, 44 patients whose procedure images and post-procedural follow-up Doppler US and SMI data could be accessed were included in this study. Patients were informed about the treatment and post-treatment process. Approval was obtained from the Ethics Committee at Ankara Diskapi Yildirim Beyazit Training and Research Hospital Ethics Committee (reference no. 136/13). Written consent was obtained from all patients.
Self-expandable stents (Carotid Wallstent; Boston Scientific, Marlborough, MA, USA) and anti-embolic protection devices (SpiderFX; Medtronic, Dublin, Ireland or Emboshield NAV6; Abbott, IL, USA) were used in all procedures.
Patient demographics
The age range of the patients was 46–87 years (mean age = 67 years). Patient characteristics are shown in Table 1.
Baseline patient characteristics (n = 44).
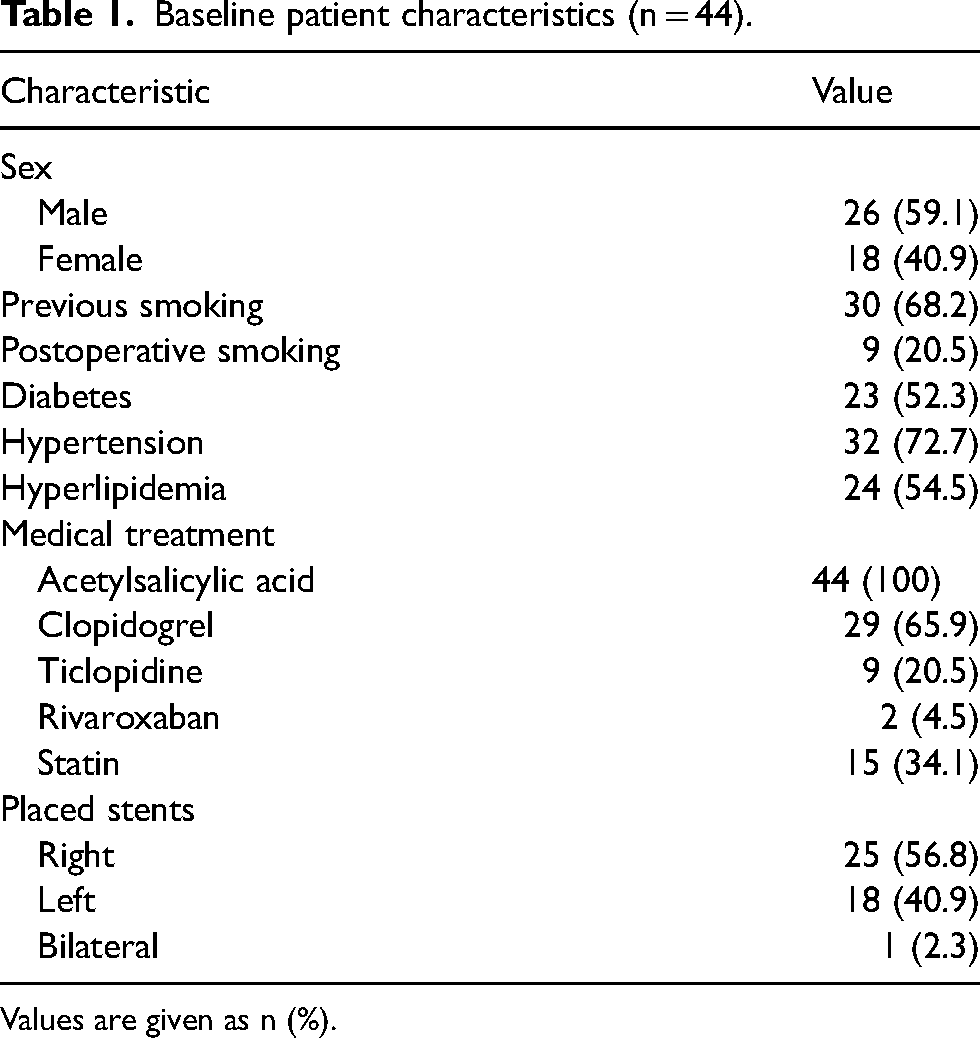
Values are given as n (%).
Ultrasound examination
B-mode imaging, Doppler velocity measurements, and SMI were performed using an Aplio 500 ultrasound device (Toshiba Medical Systems, Tokyo, Japan), using a 6–12 MHz linear array transducer in all patients.
Doppler velocities were obtained with appropriate angle correction and classified according to the criteria used by Lal et al., which are shown in Table 2 (9).
Doppler velocity criteria* used by Lal et al.
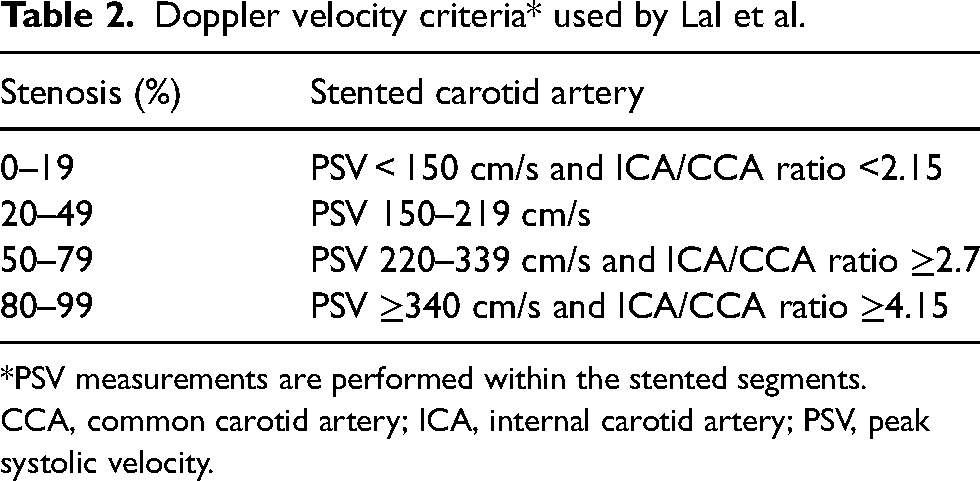
*PSV measurements are performed within the stented segments.
CCA, common carotid artery; ICA, internal carotid artery; PSV, peak systolic velocity.
The imaging studies were performed by two experienced radiologists. The common carotid artery (CCA), the internal carotid artery (ICA), and the placed stent were examined for neointimal hyperplasia and in-stent restenosis. B-mode US, color Doppler US, and SMI were used to determine neointimal hyperplasia; velocity measurements were obtained for restenosis (Fig. 1). Suspected cases were studied for in-stent restenosis with SMI, both using area and diameter measurements.
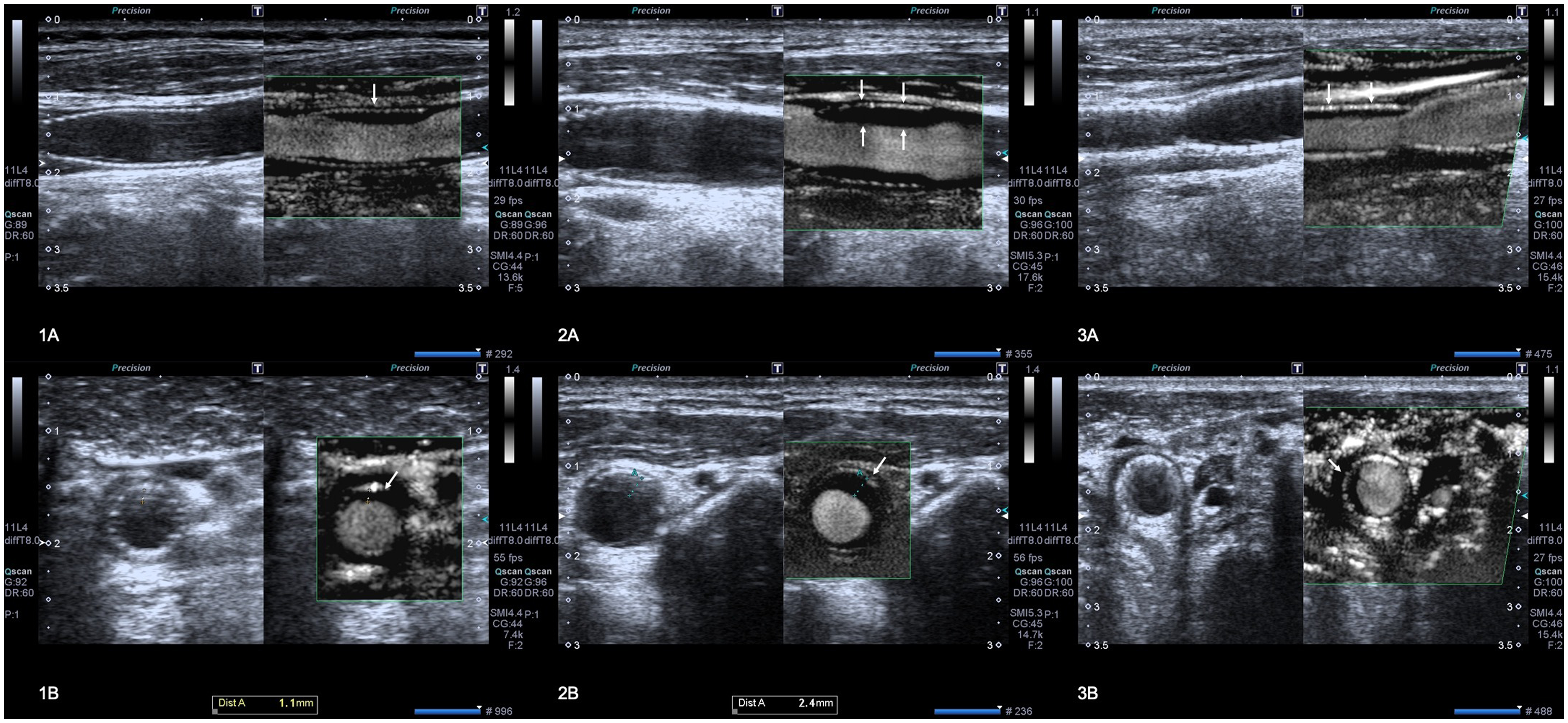
(1A, 2A, 3A) Longitudinal and (1B, 2B, 3B) axial B-mode and SMI images of carotid artery stents. Neointimal hyperplasia is seen as a hypoechoic layer between the arterial flow and the stent wall (arrows). SMI, superb microvascular imaging.
In native carotid arteries, intima-media thickness <1 mm is considered normal (10). However, there is no study to define the minimum rate of neointimal hyperplasia in the literature. Therefore, measumerements <0.5 mm were not considered for neointimal hyperplasia in this study.
Superb microvascular imaging
Both blood flow and tissue motion can produce ultrasonic Doppler signals. To remove motion artifacts, Doppler techniques use a wall filter causing loss of slow blood flow signals. On the contrary, SMI applies a multidimensional filter to separate low-flow signals from overlapping tissue motion, resulting in high resolution on vascular examinations. SMI offers two modes: color and monochrome. In our study, we opted for the monochrome mode because it eliminates background information, enabling a focused view of blood flow. This mode can be presented in a twin-view alongside the B-mode image. During patient examinations, we decreased the color box width and increased the color gain to optimize SMI image quality, until the flash artifacts could not be seen and optimal visualization of blood flow was achieved (11).
Digital subtraction angiography (DSA)
To establish the correlation between the data obtained from Doppler US and SMI, angiography remains the gold standard. In our institution, we use the threshold value of 80%–99% stenosis degree, as described by Lal et al. (9). Therefore, we were only able to correlate the results of two patients using DSA.
Results
All the patients were examined for neointimal hyperplasia in both the CCA and ICA portions of the stent. The results are shown in Table 3.
The measurements of the neointimal hyperplasia of both CCA and ICA portions of the stent.
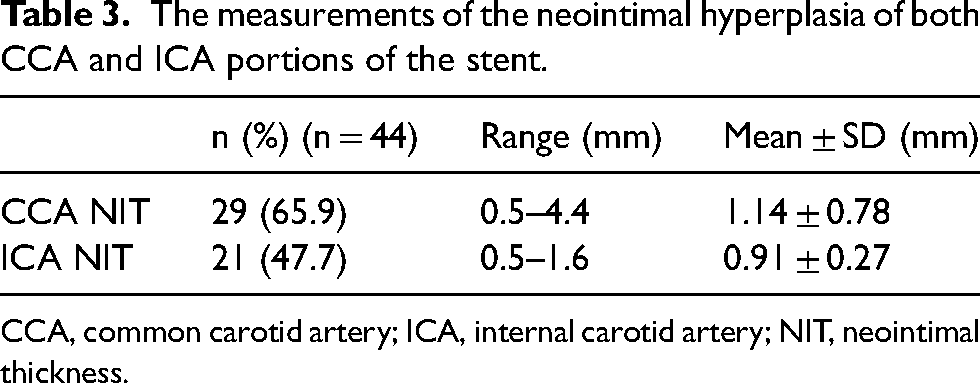
CCA, common carotid artery; ICA, internal carotid artery; NIT, neointimal thickness.
The initial results showed there were nine patients who had in-stent restenosis. One patient had no velocity increase; however, in SMI the measurements showed in-stent restenosis in both area and diameter. In this case, stenosis primarily affected the CCA portion of the stent and the ICA portion had only minimal neointimal hyperplasia. Other eight patients had a stenosis degree in the range of 50%–79% according to the Doppler velocity criteria used by Lal et al. Five patients had in-stent restenosis in both Doppler US and SMI by area and diameter measurements (Fig. 2). The Doppler and SMI measurements of these patients are listed in Table 4.
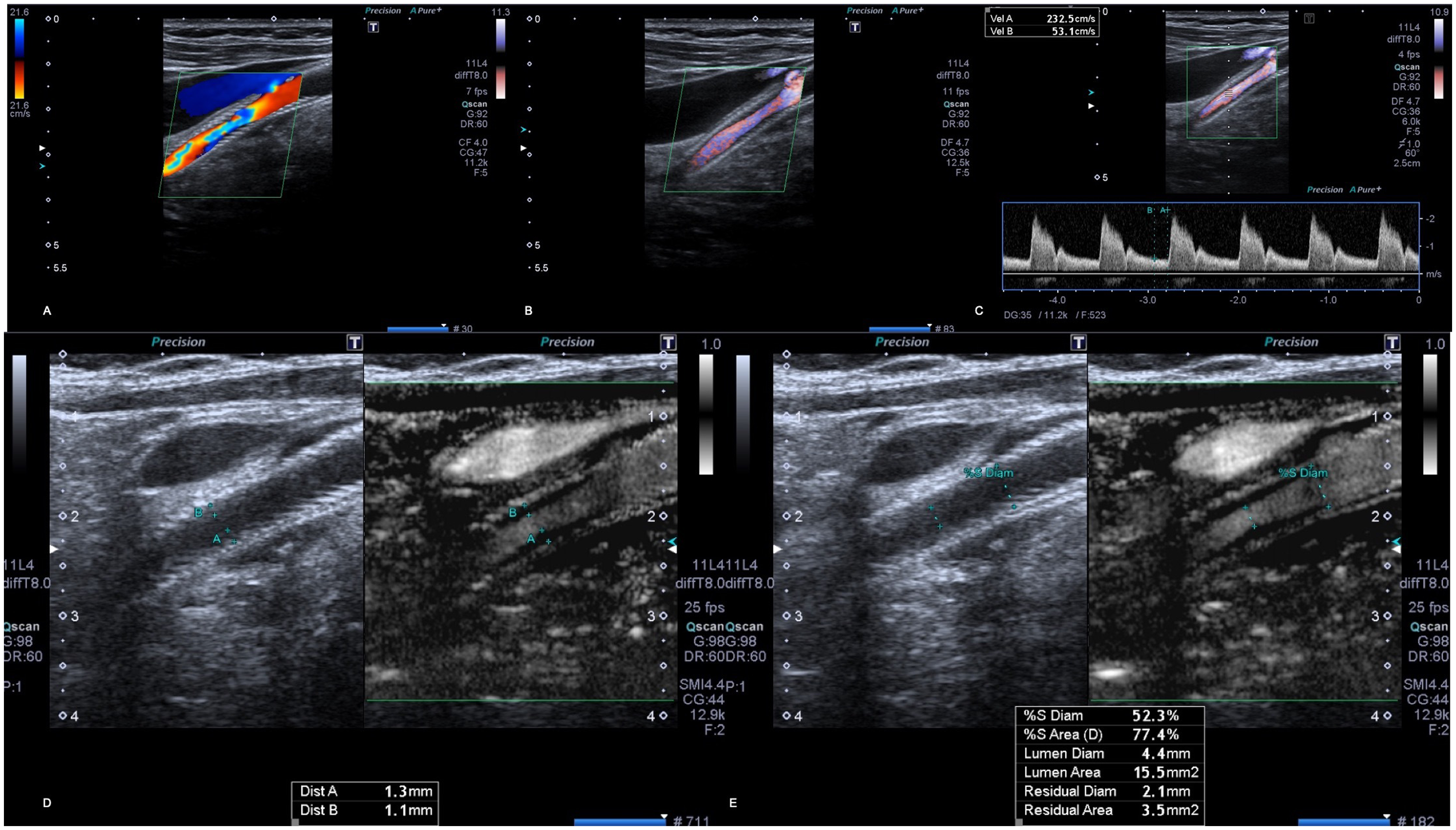
Color Doppler US and SMI scans of a patient with carotid artery stent. PSV measurements obtained from the area suspected of restenosis where color Doppler US showed aliasing artifact. (A–C) Velocity increase was detected consistent with 50%–79% stenosis (PSV/EDV = 232/53 cm/s). (D) With SMI, anterior wall neointimal hyperplasia of 1 mm thickness and posterior wall neointimal hyperplasia of 1.3 mm thickness are shown. (E) The diameter stenosis of 52% and area stenosis of 77% are measured using SMI. EDV, end-diastolic volume; PSV, peak systolic velocity; SMI, superb microvascular imaging; US, ultrasound.
Patients with in-stent restenosis.
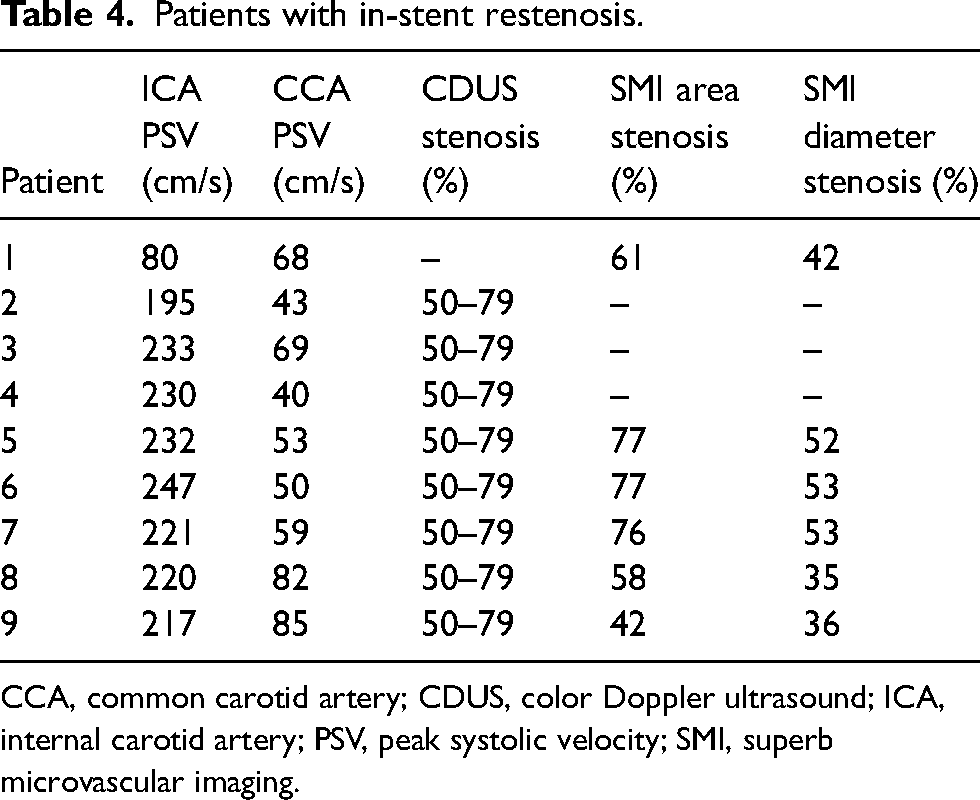
CCA, common carotid artery; CDUS, color Doppler ultrasound; ICA, internal carotid artery; PSV, peak systolic velocity; SMI, superb microvascular imaging.
Two patients underwent DSA and due to the >70% degree of in-stent restenosis, endovascular treatment with a new stent placement was performed (Figs. 3 and 4).
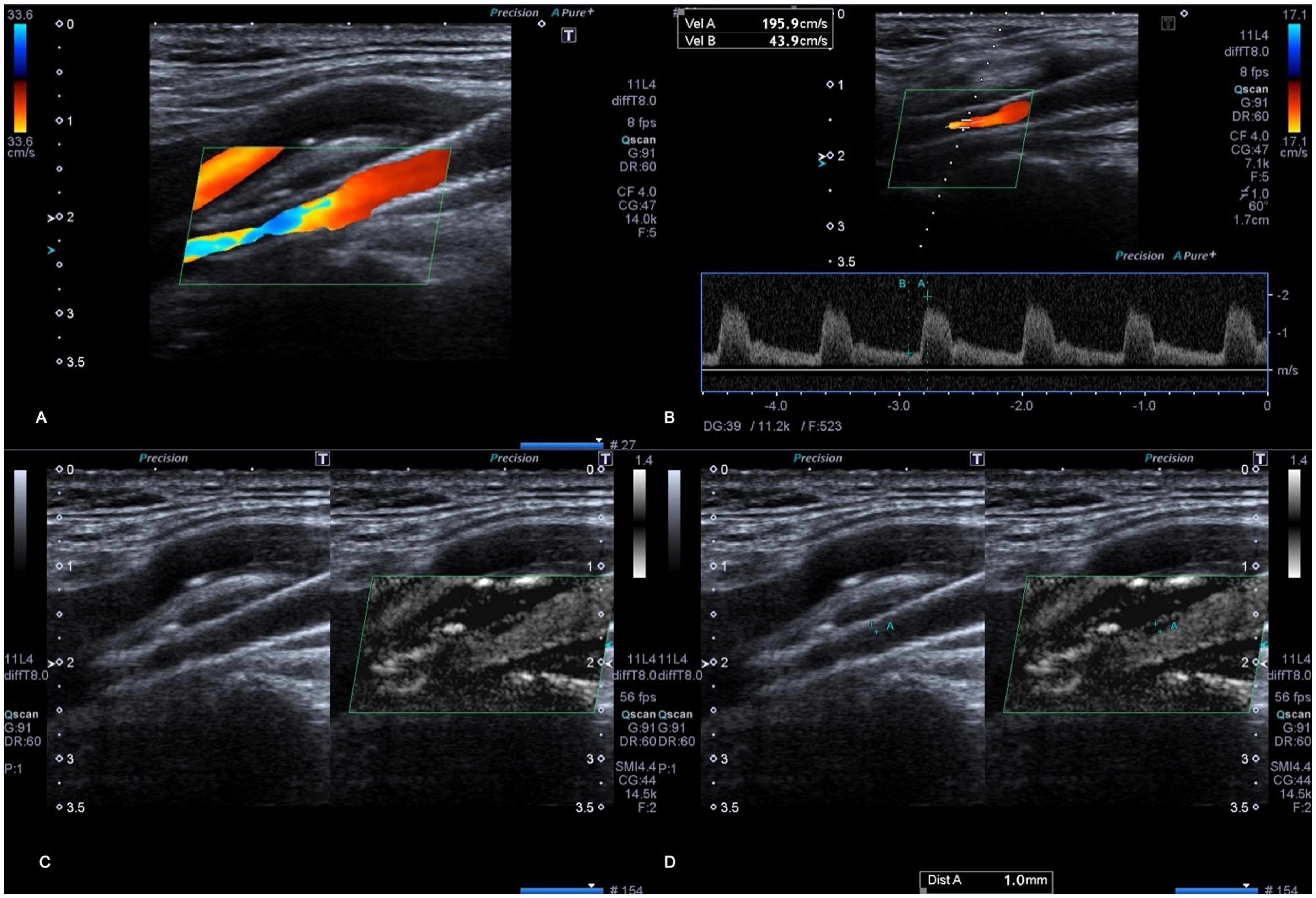
Color Doppler US, velocity measurements, and SMI images of a patient with carotid artery stent. (A) Color Doppler US showed an aliasing artifact that was suspected of restenosis. (B) The increase of PSV confirmed the in-stent restenosis. (C, D) SMI showed an anterior wall neointimal hyperplasia with a thickness of 1 mm. PSV, peak systolic velocity; SMI, superb microvascular imaging; US, ultrasound.
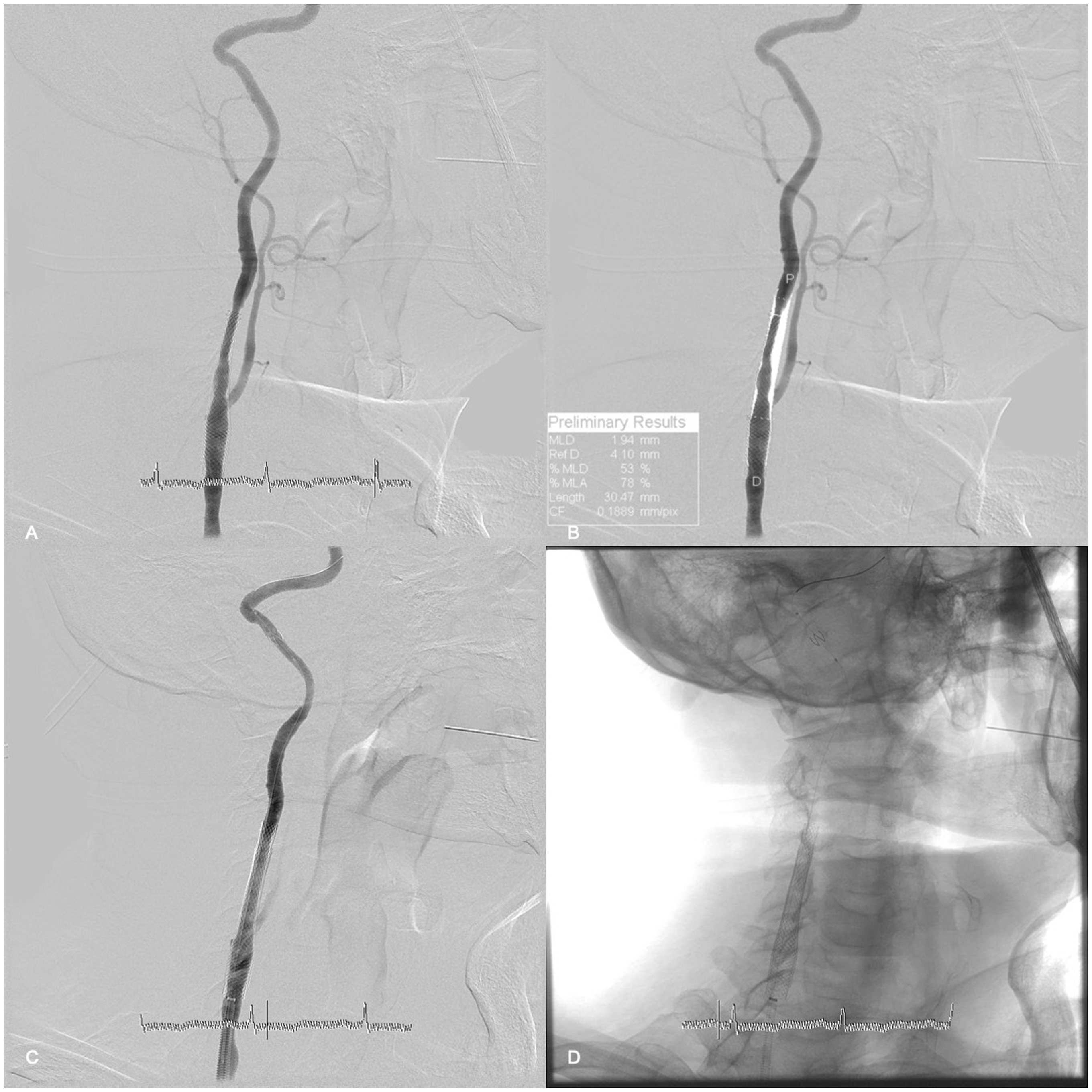
(A, B) DSA images of the patient in Fig. 3 after 1 year of US control. The patient's angiography was delayed by 1 year due to the COVID-19 pandemic. The in-stent restenosis degree increased during that time; therefore, the patient underwent re-stent placement. (C, D) Postprocedural DSA images can be seen. DSA, digital subtraction angiography; SMI, superb microvascular imaging; US, ultrasound.
Discussion
After stent placement to the carotid vessels, the healing process has started immediately. According to Willfort-Ehringer et al., the healing process of carotid stent is divided into three phases (12). The first phase is unstable, which presumes that a thrombotic layer covers the inner surface of the stent and diminishes nearly to zero until the first month. The second phase is the growth of neointima and can be seen on B-mode US as a hypoechogenic layer between the stent wall and the lumen of the vessel. The growth of neointima is a physiological response triggered with vessel trauma by placement of the stent. It is assumed to start between the first and third postoperative months. If the growth of neointima is severe, due to individual factors such as smoking and diabetes, it can lead to neointimal hyperplasia (12,13). In-stent restenosis may develop during this period. It is suggested that this period is completed more or less after 12 months (12). The third phase is characterized by a stable neointima that represents the integration of the stent wall and the vessel.
Detecting neointimal hyperplasia and follow-ups are essential because they could lead to in-stent restenosis (5,12,13). The follow-up of CAS patients includes B-mode and Doppler US with velocity measurements in most centers. There have been many velocity criteria suggested to determine in-stent restenosis (14). Referring to these velocity criteria, the patients are selected for DSA and further intervention. However, there is no consensus about the restenosis velocity criteria in the literature. Due to the gold standard of diagnosing in-stent restenosis using DSA, some patients undergo unnecessary angiography.
SMI is a new Doppler imaging technique that allows the identification of low velocities of blood flow and obtains images similar to contrast-enhanced US. This technique uses an algorithm that purifies the luminal visualization by eliminating motion artifacts and noise background without lowering the frame rate (8,15). In recent studies, SMI has mostly been used for detecting endoleaks in endovascular aneurysm repair, intraplaque neovascularization, vascularity of thyroid nodules, and breast malignancies (7,8,16,17). SMI can also detect neovascularization in native carotid artery plaques; there have been many studies that show this technology is useful to determine whether the plaque is vulnerable (7,18). B-mode US is sufficient to examine and detect the carotid plaques; however, the thickness and length of the plaque, as well as the ulcerations, are defined better with SMI.
In-stent restenosis, especially after 2 years postoperatively, may occur due to plaque in-growth rather than neointimal hyperplasia. This long-term complication is associated with the use of single-layer carotid stents that inadequately insulate the plaque underneath the stent (19,20). As a result, the atheromatous plaque starts to grow inside the stent between the stent structure. Tekieli et al. presented a case report of an in-stent restenosis developing due to plaque in-growth diagnosed using intravascular ultrasound (19). With this version of SMI technology, distinguishing whether the restenosis is triggered by neointimal hyperplasia or plaque in-growth is challenging, as this technology lacks the ability to provide histological data revealing the fibrous cap, which is characteristic of atheromatous lesions. In our study, we successfully diagnosed in-stent restenosis using SMI. However, we anticipate that further enhancements in SMI technology may enable us to discern whether the cause of in-stent restenosis is neointimal hyperplasia or plaque in-growth.
Several studies in the literature examine whether stent design influences restenosis rates (21,22). However, in our study, all patients were treated with the Carotid Wallstent (Boston Scientific, Marlborough, MA, USA). As a result, we were unable to investigate the impact of stent design on restenosis rates within the scope of this study.
To date, this is the first study that uses SMI to detect neointimal hyperplasia and in-stent restenosis in carotid stents. Because of the clear visualization of the stent lumen, hypoechoic lesions on the stent wall that cannot be easily identified in B-mode US can be determined using SMI. We suggest that using SMI with duplex sonography improves detecting neointimal hyperplasia and determining the patients suspected of having in-stent restenosis. With SMI technology, better visualization of the stent lumen may improve the patient selection for DSA.
The present study has some limitations. These include the low numbers of cases with in-stent restenosis, the absence of comparison with intravascular ultrasound, and contrast-enhanced ultrasound images due to the lack of contrast agent in our institution. In addition, we could not obtain DSA images from all patients with in-stent restenosis because the stenosis degrees did not require angiography. Due to these limitations, further studies may be required.
In conclusion, with SMI technology we may be able to detect neointimal hyperplasia better than B-mode ultrasound, obtain better intraluminal images, and more accurately diagnose in-stent restenosis.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.