
Abstract
Background
Knees with anterior cruciate ligament (ACL) injury have distinct knee bone morphology. However, the correlation between ACL injury and morphology of the proximal tibiofibular joint has not been investigated.
Purpose
To compare proximal tibiofibular joint morphology in patients with injured and intact ACLs to aid in predicting and preventing ACL injuries.
Material and Methods
A total of 50 patients with ACL injury and 50 individuals without structural knee damage (revealed by magnetic resonance imaging [MRI]) were included in this study. In the anteroposterior knee radiographs, the length between the proximal end of the fibular head and the medial and lateral tibia joint line were measured. In the axial knee MRI scans with the most proximal part of the fibular head, the distance calculation was performed between the most anterior point of the tibia plateau (MATP) and the most anterior point of fibular head (MAFH).
Results
The mean length from the proximal end of the fibular head and the medial and lateral tibial joint lines was 8.7 ± 2.8 mm and 13.2 ± 2.6 mm in the ACL-injured group, and 6.5 ± 2.8 mm and 11.1 ± 2.4 mm in the control group. The length for both medial and lateral sides was significantly greater in the ACL-injured group. The length between the MATP and MAFH was significantly larger in the ACL-injured group than the control group.
Conclusion
A large distance between the proximal end of the fibular head and the tibial joint line and knees with posterior fibular head placement would be another anatomic risk factor of ACL injury.
Introduction
Knees with anterior cruciate ligament (ACL) injuries share certain morphological characteristics (1–8). Recently, soft tissue of the lateral knee is a major issue for the stabilization of the knee joint (9–12). Although anterolateral ligament (ALL) existence is still controversial (9), it seems that lateral knee soft tissue, such as the lateral joint capsule, the iliotibial band, and the fibular collateral ligament, plays an important role in the stabilization of the knee (12,13). It is widely known that the shape of the intercondylar notch on the femur shows a strong correlation with the incidence of ACL injury (1,8). One of the most famous anatomical parameters that correlates with ACL injury is known as the notch width index. ACL injury occurs in knees with a small intercondylar notch on the femur (1,8). A large posterior tibial slope is also a high-risk factor for ACL injury (2,8). However, the usefulness of knee shape for the prevention or prediction of ACL injury has not been studied in depth (1,2,4). The bony shape of the knee can be evaluated easily with X-ray, computed tomography (CT), or magnetic resonance imaging (MRI). If strong risk factors for ACL injury can be identified based on knee bone shape, the incidence of ACL injury could be predicted, making prevention more feasible. The fibular head is the only bone structure that exists among the lateral aspects of the knee (12). However, not many studies have evaluated its shape. In addition, the relationship between fibular head or proximal tibiofibular joint morphology and the incidence of ACL injury has not been well investigated.
The aims of the present study were to evaluate fibular head and proximal tibiofibular joint morphology and to reveal the correlation between that morphology and the incidence of ACL injury. It was hypothesized that some differences in the morphology of the fibular head or proximal tibiofibular joint would be found between knees with and without ACL injury.
Material and Methods
The ACL injury group consisted of 50 patients with ACL injury who had been treated with ACL reconstruction (26 men, 24 women; mean age = 26.2 ± 8.7 years). All participants were recreational athletes. The dominant leg side was not taken into consideration.
The control group consisted of 50 age- and sex-matched patients (25 men, 25 women; mean age = 28 ± 9.5 years) with knee pain with no structural damage (meniscus, ligament, and articular surface) confirmed by MRI.
The exclusion criteria were as follows: age >50 years; previously injured knee; contralateral knee injury; and Kellgren-Lawrence (K-L) grade II or more severe knee osteoarthritis. Informed consent was obtained from all patients. Approval was obtained from the ethics committee (reference no. KH2201).
X-ray evaluation
In the anteroposterior (AP) knee X-ray image, the distance between the proximal end of the fibular head and the medial and lateral tibia joint line was measured. The tibial joint line was defined as the line perpendicular to the tibial bone shaft and tangential to the medial or lateral tibia plateau. The line tangential to the proximal end of the fibular head and parallel to the tibial joint line was determined, and the length between the line and medial or lateral tibial joint line was regarded as the proximal end of the fibular head and the medial and lateral tibia joint line length (Fig. 1).
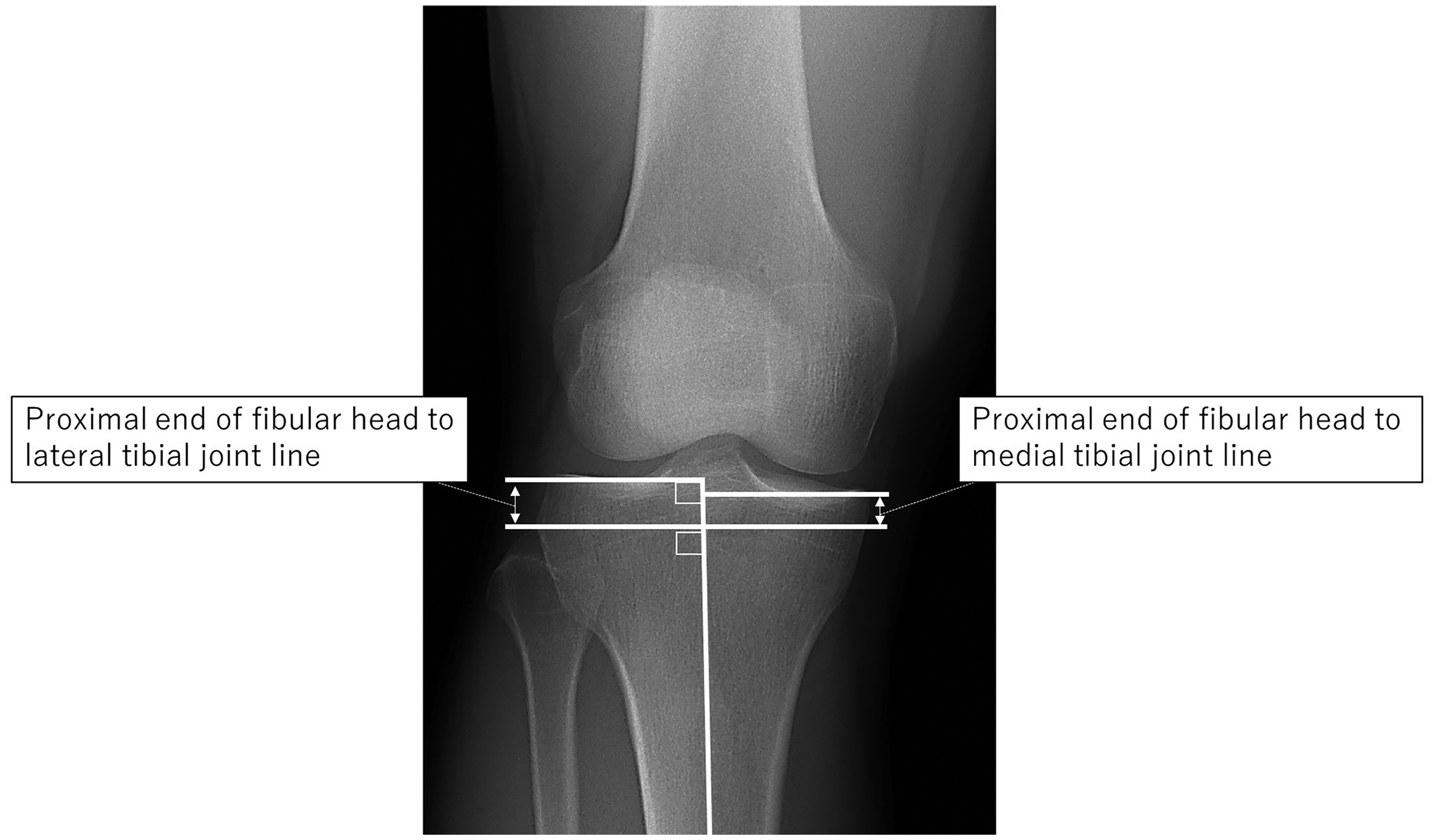
X-ray evaluation of the length between the proximal end of the fibular head and the tibial joint line. In the AP knee X-ray, the length between the tibial joint lines (perpendicular line to the tibial bone shaft and tangential to the medial or lateral tibial articular surface) and the proximal end of the fibular head (parallel line to the tibial joint line and tangential to the proximal end of fibular head) was measured. AP, anteroposterior.
MRI evaluation
In the axial image of knee MRI including the most proximal fibular head, the AP and mediolateral (ML) length of the tibia plateau was measured (3). The connecting line of the medial and lateral tibial plateau's posterior condyle was determined first; based on the line, the outer rectangle was determined on the tibia plateau. This rectangle's AP and ML lengths were regarded as the tibial AP and ML lengths. The length from the most anterior lesion of the tibia plateau (MATP) and the most anterior lesion of the fibular head (MAFH) was measured. The ratio of MAFH/tibial plateau AP length was calculated (Fig. 2).
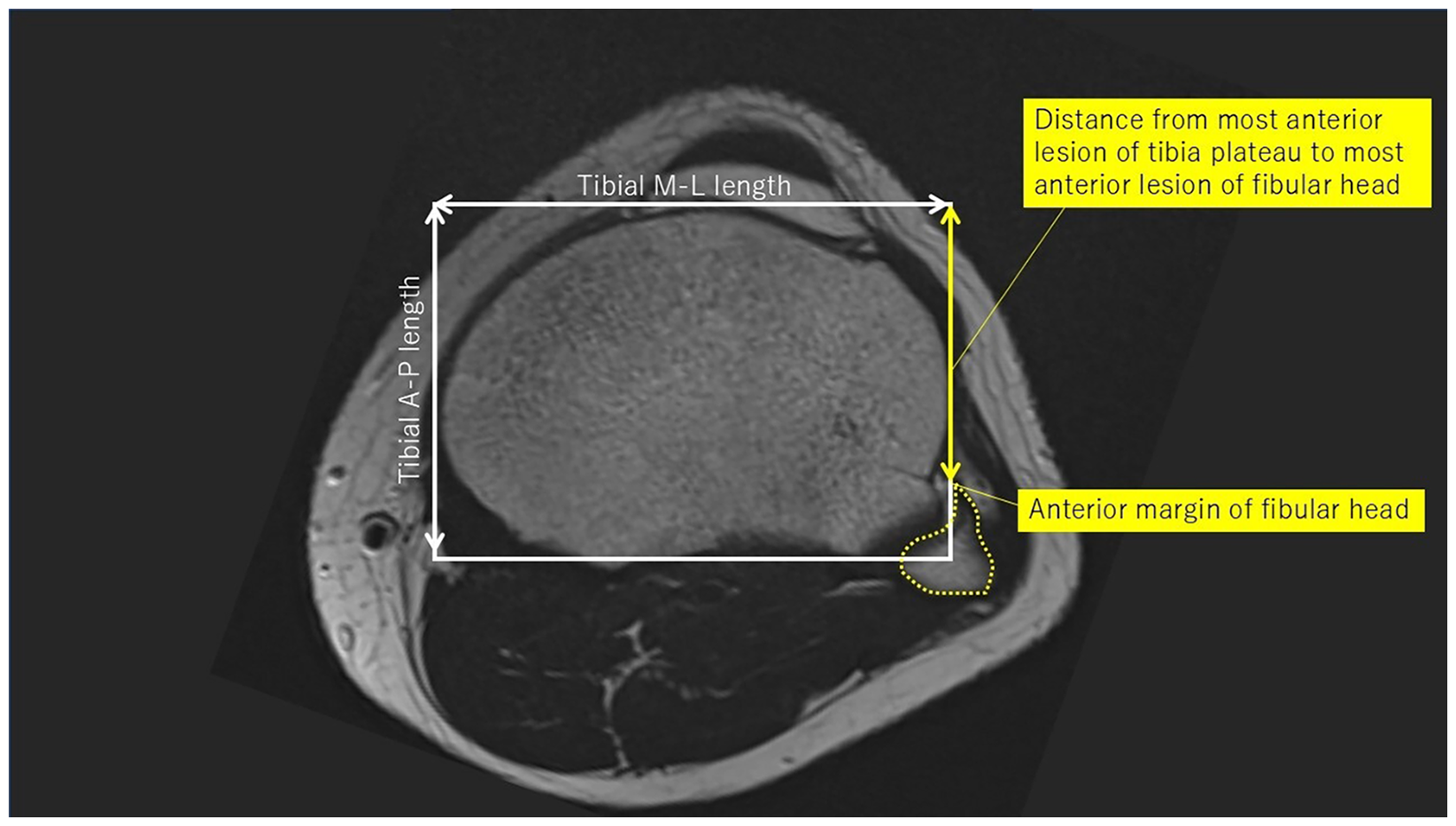
MRI evaluation of the tibia plateau and proximal tibiofibular joint shape. In knee MRI including the most proximal fibular head, the AP and ML lengths of the tibia plateau were measured. The distance between the most anterior point of the tibia plateau (MATP) and the most anterior point of the fibular head (MAFH), and the ratio between the MAFH/AP length of tibia plateau were measured. AP, anteroposterior; ML, mediolateral; MRI, magnetic resonance imaging.
Statistical analysis
Considering the sample size was not large, the non-parametric Mann–Whitney U-test was used for the statistical analysis to compare the following parameters between the ACL injury and control groups (P < 0.05 was considered significant):
The length between the proximal end of the fibular head and the medial and lateral tibial joint lines. The length between the proximal end of the fibular head and the medial and lateral tibial joint lines normalized by ML length of tibia plateau. AP and ML lengths of the tibia plateau. The length between the MATP and MAFH and the ratio.
The F-test was performed for the evaluation of data distribution.
Inter- and intra-observer reliability (ICC 1 and 2) was calculated with the length between the fibular head and the medial and lateral tibial joint lines.
To calculate the sample size, G*Power 3 software was used (test family = t-test; statistical test = two independent means; types of power analysis = priori; power = 0.95). The calculated sample size was 35 for each group.
Results
X-ray evaluation
The mean length from the proximal end of the fibular head and the medial and lateral tibial joint lines was 8.7 ± 2.8 mm and 13.2 ± 2.6 mm in the ACL injury group, and 6.5 ± 2.8 mm and 11.1 ± 2.4 mm in the control group, respectively. The length for both the medial and lateral sides was significantly greater in the ACL injury group (P < 0.05) (Fig. 3a). The F-test showed no significant group difference of data distribution (the length from the proximal end of the fibular head and the medial and lateral tibial joint lines). When these lengths were normalized by the tibia plateau ML length, this difference did not change and the ACL injury group still showed a significantly larger value than control group (P < 0.05) (Fig. 3b). For the distance between the fibular head and the medial and lateral tibial joint lines, ICC 1 and 2 were 0.84 and 0.86, and 0.8 and 0.88, respectively.
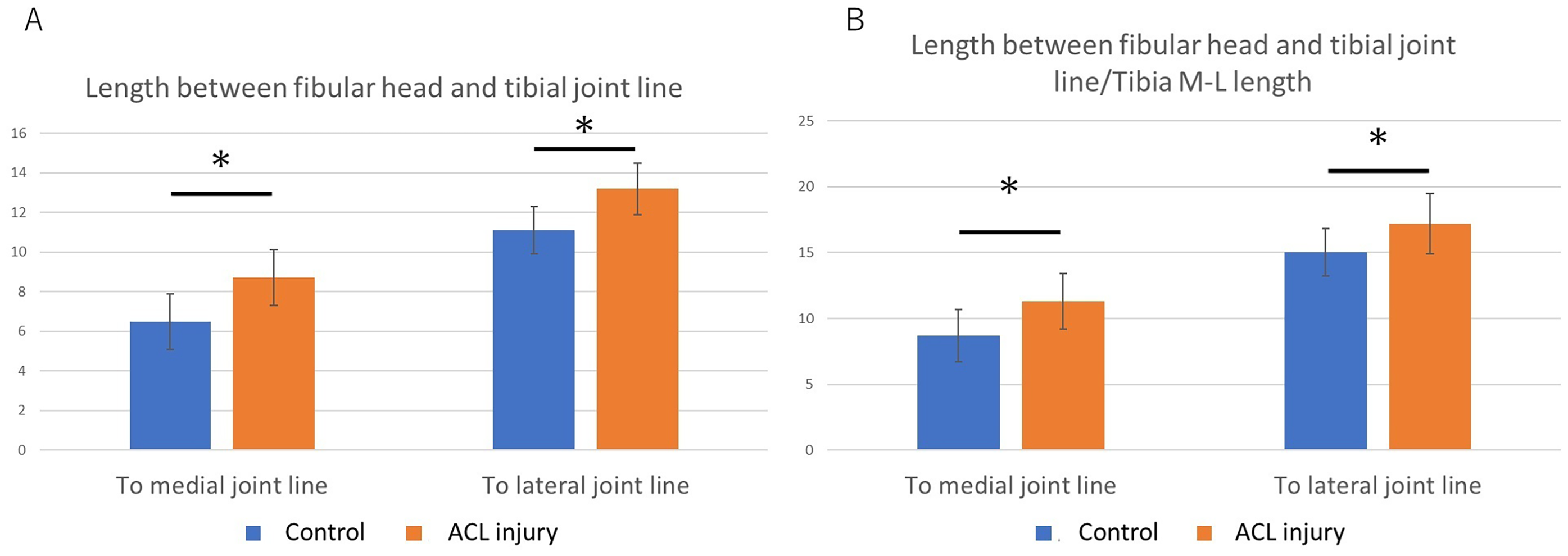
Comparison of the length between the proximal end of the fibular and tibial joint line between the ACL injury and control groups. (A) The lengths between the proximal end of fibular and tibial joint lines (medial and lateral) were significantly longer in the ACL injury group. (B) These results did not change when the length was normalized by the ML length of tibia plateau. ACL, anterior cruciate ligament. ML, mediolateral.
MRI evaluation
The AP and ML length of the tibia was 52.5 ± 4.6 mm and 74.7 ± 6.5 mm in the ACL injury group, and 50.9 ± 4.8 mm and 74.5 ± 4.6 mm in the control group, respectively. Both the length between the MATP and the MAFH and the ratio between the length between the MATP and MAFH /AP length of the tibia plateau were significantly larger in the ACL injury group than in the control group (P < 0.05) (Table 1).
Comparison of tibiofibular joint shape between ACL injury and control groups.
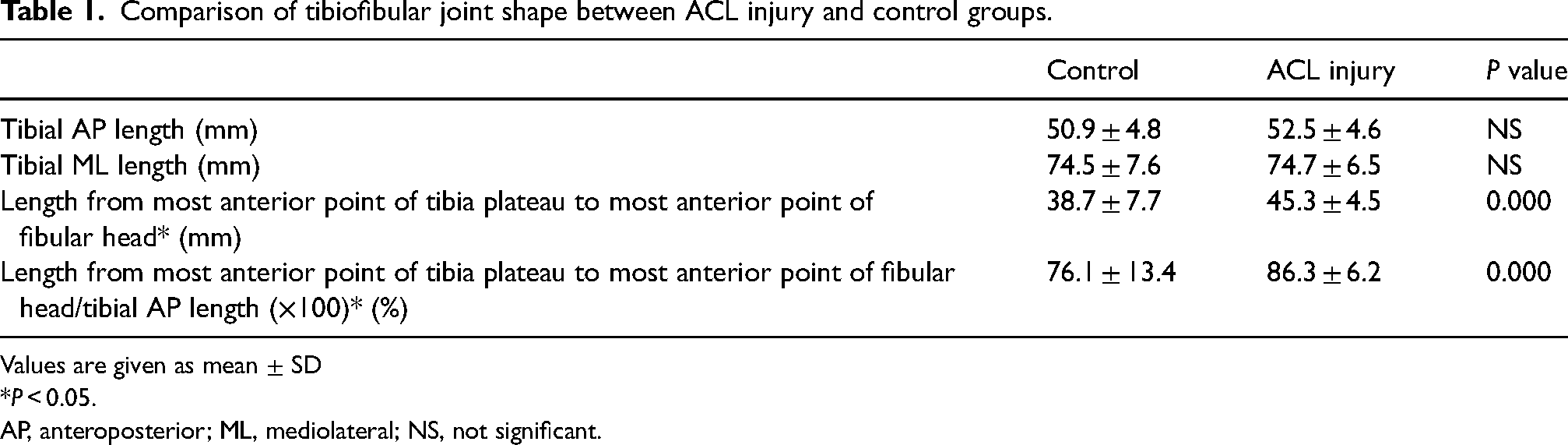
Values are given as mean ± SD
*P < 0.05.
AP, anteroposterior; ML, mediolateral; NS, not significant.
Discussion
The morphology of the fibular head and proximal tibiofibular joint differed significantly between the ACL injury and control groups. The length between the proximal end of the fibular head and the tibial joint line was significantly longer in the ACL injury group. In the ACL injury group, the fibular head was located significantly more posteriorly than in the control group. Measuring proximal tibiofibular joint morphology in individuals with pre-ACL injury as part of medical screening could aid in predicting and preventing ACL injuries.
The proximal tibia and fibular head form the proximal tibiofibular joint (12,14–17). Several characteristics of the fibular head anatomy have been reported (18–22). The fibular collateral ligament, popliteofibular ligament, and biceps femoris tendon attach to the fibular head and are believed to contribute to knee stabilization. The popliteus tendon runs just posterior to the fibular head (19,23). The knee joint capsule and the tibiofibular joint capsule surround the fibular head (12). Several knee stabilizers attach to and surround the fibular head and proximal tibiofibular joint, making the lateral knee structure and ACL injury subjects of significant interest (9,11,13,19). However, few reports have existed on fibular head or proximal tibiofibular joint morphology. Although it has been rarely reported that the proximal tibiofibular joint instability becomes a cause of posterolateral knee pain (18,24), the relation between proximal tibiofibular joint morphology and knee instability has not been well investigated. The length between the proximal end of the fibular head and the tibial joint line was significantly longer in the ACL injury group in this study. A key mechanism may be that the extended running distance of the lateral knee soft tissue contributes to increased lateral knee laxity, potentially leading to ACL injury. In the present study, the fibular head or the proximal tibiofibular joint was located more posteriorly in the ACL injury group than in the control group. Earlier studies reported that proximal tibiofibular joint dislocation leads to anterior knee instability (13,23,24). The fibular head or proximal tibiofibular joint may play a role in joint stabilization, acting as the “lateral wall” of the knee. A posteriorly positioned fibular head or proximal tibiofibular joint appears to be associated with knee rotational instability and may contribute to ACL injury.
The present study has some limitations. First, not healthy participants were included as the control group. Owing to the limited sample size, age- and sex-matched controls were used in this study; however, level of physical activity or body size would also influence knee morphology, and those should be matched in future research. Second, only Japanese individuals were included in this study. Third, the sample size was not large. Fourth, a two-dimensional evaluation was performed in this study. As the fibular head or proximal tibiofibular joint has a three-dimensional complicated morphology (25), a three-dimensional evaluation should be performed in future research.
In conclusion, this study found significant differences in fibular head or proximal tibiofibular joint morphology between the ACL injury and control groups. A significantly greater distance between the proximal end of the fibular head and the tibial joint line, along with a more posterior positioning of the fibular head or proximal tibiofibular joint, was observed in the ACL injury group. Assessing the morphology of these structures may aid in predicting and preventing ACL injuries.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.