
Abstract
Background
Hip dysplasia (HD) involves abnormal acetabular development, resulting in reduced femoral head coverage, labral tears, and cartilage injury. Machine learning (AI) advancements have enabled reproducible radiographic measurements for HD, such as lateral center edge angle (LCEA), Tonnis, and extrusion index. Moreover, incorporating 3D magnetic resonance imaging (MRI) alongside 2D MRI enhances diagnostic capabilities.
Purpose
To correlate advanced MRI-assessed labral and cartilage injuries with validated AI-generated radiographic measurements.
Material and Methods
This study enrolled 139 patients (age range = 16–68 years) with HD, comprising a total of 156 hips. All patients had 2D and 3D MRI scans, four-view X-rays, and AI-generated radiographic measurements using a commercial AI program that utilized bony landmarks to generate measurements. Labral reconstructions were obtained for each hip, and a multi-reader study was conducted. Inter-reader (ICC) analysis and Spearman correlations were calculated.
Results
The predominant location for the largest labral tear was anterosuperior (133/156, 90%), and paralabral cysts were observed in 53/156 (34%) cases. No statistically significant correlations were found between the length of labral tears and radiographic measurements. However, statistically significant correlations were observed between paralabral cysts and femoral head coverage, extrusion index, LCEA, and Tonnis measurements.
Conclusion
AI-generated radiographic measurements in HD exhibited weak correlations with advanced MRI findings, likely due to the condition's complex pathophysiology.
Introduction
Hip dysplasia (HD) is characterized by structural abnormalities of the acetabulum causing under coverage of the femoral head (1). HD usually presents with hip pain and/or instability in both adult and pediatric populations. If left untreated, it can lead to premature osteoarthritis and internal soft tissue damage due to improper mechanics and stress overload at the joint (2). Labral tears have been classified as similar to meniscal injuries of the knee arthroscopically and can occur with untreated HD (3). Recent research has shown that labral tear severity in patients with HD could correlate positively with symptom duration, preoperative pain severity, acetabular cartilage damage, and incidence of paralabral cysts (4). Thus, labral tear extent could serve as tools to gauge the prognosis of patients with HD. Common conservative treatment options for HD include physical therapy and lifestyle modifications, although surgical options such as periacetabular osteotomy and hip arthroplasty are indicated in more advanced disease states (5).
A wide range of radiographic measurements are used to assist in the initial diagnosis and assessment of HD, including lateral center edge angle (LCEA), Tonnis, extrusion index, and others (6). Among these parameters, LCEA is most commonly used. Definitions of different radiographic parameters used for HD diagnosis and used in this study are included in Table 1 (5,7–10).
Explanation of radiographic measurements in the study used to determine the severity of HD.
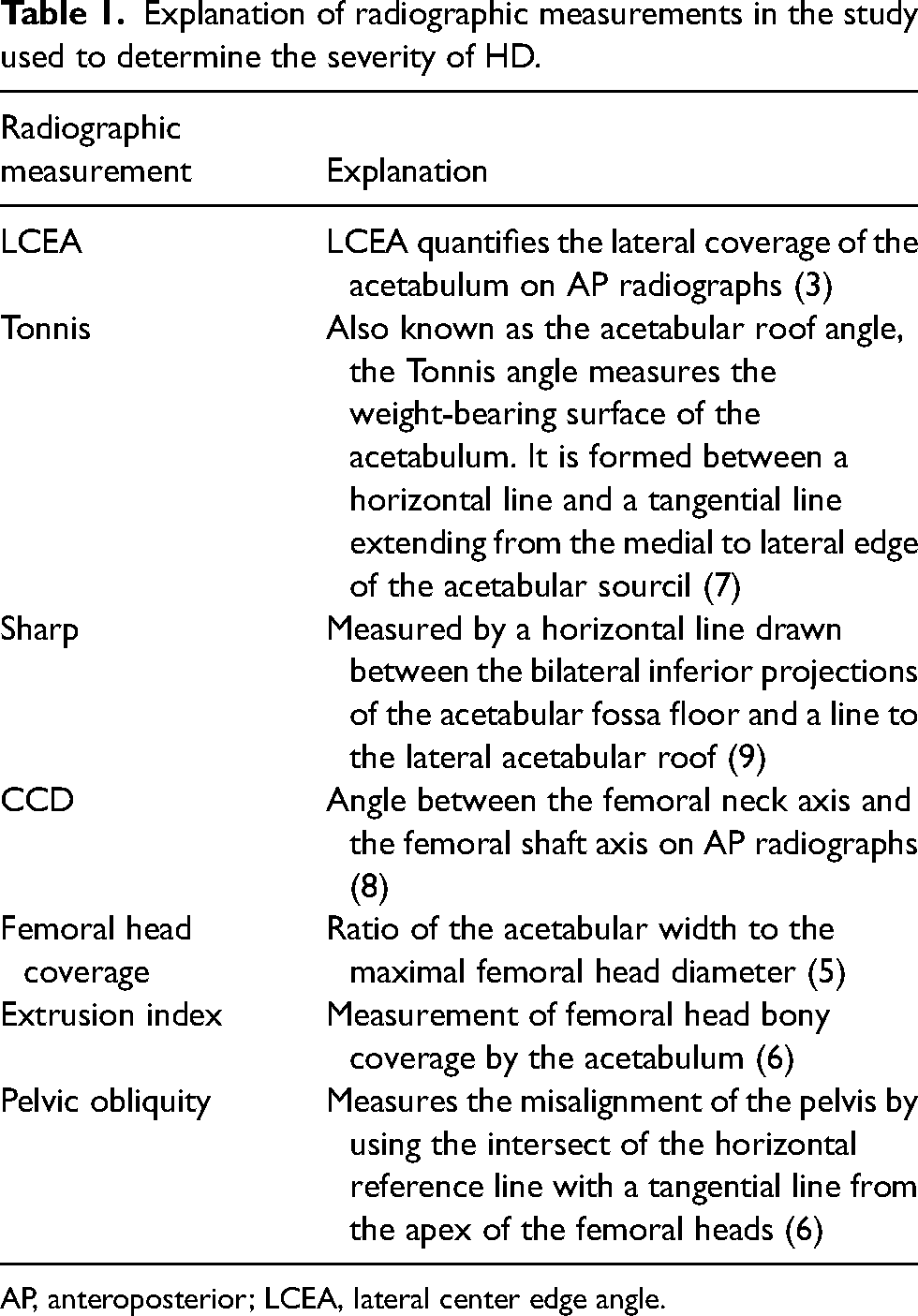
AP, anteroposterior; LCEA, lateral center edge angle.
It is time consuming to routinely measure the above outlined radiographic parameters. Fortunately, recent advancements in machine learning (AI) software have enabled reproducible and automated generation of radiographic measurements. These measurements can be used to aid in the radiographic interpretation and automated report generation in the clinical note, which has potential to enhance the workflow for both radiologists and treating physicians. Furthermore, usage of such software programs would eliminate inherent reader variance and allow for the standardized and consistent generation of needed radiographic measurements. The AI program used in this study is a hip measurement tool validated in a European study and Conformite Europeenne (CE) certified (ImageBiopsy Lab Inc., Vienna, Austria) (11).
Magnetic resonance imaging (MRI) is obtained for assessing internal and external hip soft tissues, especially the labrum, hyaline cartilage, synovium, and regional muscles (12,13). In addition, 3D MRI used in concordance with 2D MRI has been shown to enhance the evaluation of labrum and cartilage lesions of HD (11). 3D MRI opens opportunities to measure the extent of labral tears with labrum specific reconstructions with a higher degree of accuracy, not possible on traditional 2D MRI (14). Although stability of tears is best assessed on arthroscopy (4), measurement of labral tears is possible on 3D MRI reconstructions (15). Such quantitative markers along with degree of cartilage loss may predict the prognosis of such patients. MRI and MR arthrogram exhibit high accuracy of labral tear detection and with 3D MRI; it is expected to be even better (16,17). However, to the authors’ knowledge, there is lack of information regarding correlations between these reproducible and accurate AI-generated radiographic measurements and internal derangement findings on 3D MRI.
The aim of the present study was to assess the correlations between 3D advanced MRI findings and AI-derived radiographic hip measurements with the hypothesis that longer labral tears and higher-grade cartilage damage seen on 3D MRI would correlate with AI-generated radiographic HD measurements that indicate higher grades of hip dysplasia.
Material and Methods
Approval from the institutional review board was obtained for this cross-sectional study and for the retrospective use of a patient database from an institutional hip preservation clinic. The longitudinally maintained hip preservation database consists of radiographic images, 2D and 3D MRI scans, and surgical notes. All patients in the database had given informed consent for the future use of their data.
Patients
A total of 314 patient records with a final diagnosis of HD were screened for inclusion in the study from a consecutive series of patients who visited the institutional hip preservation clinic. The inclusion criteria for the study were ages 14–100 years, all genders, hip MRI performed at our institution with 2D and 3D MRI protocols on 1.5-T and 3-T magnets, and with a final diagnosis of HD based on intraoperative findings and electronic health record follow-ups. The exclusion criteria included the presence of avascular necrosis of the hip (AVN), osteoarthritis (OA), lack of 3D MRI, implants, and arthroplasty. Ultimately, 156 hips from 139 patients were included in the study. Nine of these hips did not show any labral injury on 3D MRI and were excluded from the final analysis (Fig. 1). Of the 139 patients, 90 ultimately underwent surgery for their HD. Of the 90 surgical patients, 76 had labral injuries indicated on their surgery reports. Of these 76 patients, 75 patients underwent intraoperative repair of their labrum.
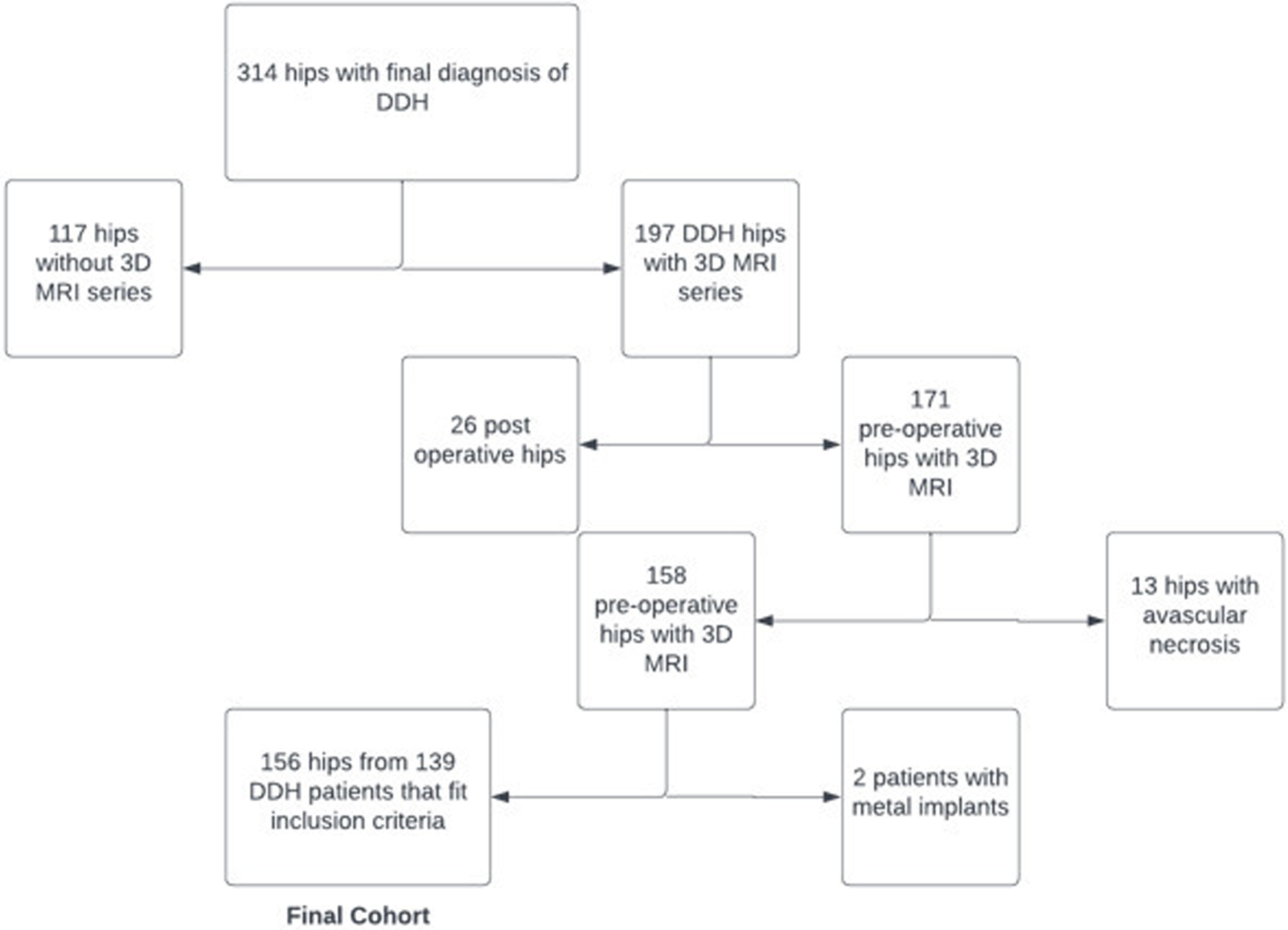
Representation of how the final cohort for the study was obtained. A total of 156 hips from 139 patients with DDH fit the inclusion criteria from a total pool of 314 hips with a diagnosis of DDH. DDH, developmental dysplasia of the hip.
MRI protocol
All scans were performed on 1.5-T and 3-T scanners using a cardiac multichannel coil. Multiplanar 2D MRI sequences in fat-suppressed and non-fat-suppressed contrasts were available (parameters were as follows: TR = 3000–3500 ms; TE = 36–42 ms; slice thickness = 3.0–3.5 mm; interslice gap = 10%; fat-suppression = frequency-selective fat suppression). 3D MRI was obtained using the following parameters: TR = 1100 ms; TE = 40–42 ms; voxel = 0.8–0.9 mm; interslice gap = 0%, sagittal isotropic acquisition with multiplanar reconstructions available in picture archiving system).
HIPPO: an AI measurement tool
The AI measurement tool used in the study, “HIPPO” (ImageBiopsy Lab Inc., Vienna, Austria) automatically measures radiographic parameters on AP weight-bearing radiographs using anatomical landmarks (11). The algorithm has been validated by a previous study, where measurements made by trained manual readers were compared with the measurements made by the AI algorithm. It was shown that the AI algorithm demonstrated good to excellent agreement with the manual readers as measured by intraclass correlation coefficient (ICC) (11). The parameters measured included LCEA, Tonnis angle, Sharp angle, caput-collum-diaphyseal (CCD) angle, femoral head coverage, extrusion index, and pelvic obliquity. The data are then processed through the software and downloaded onto an Excel document (Windows 11; Microsoft, Redmond, WA, USA). An example of the AI measurements is shown in Fig. 2.
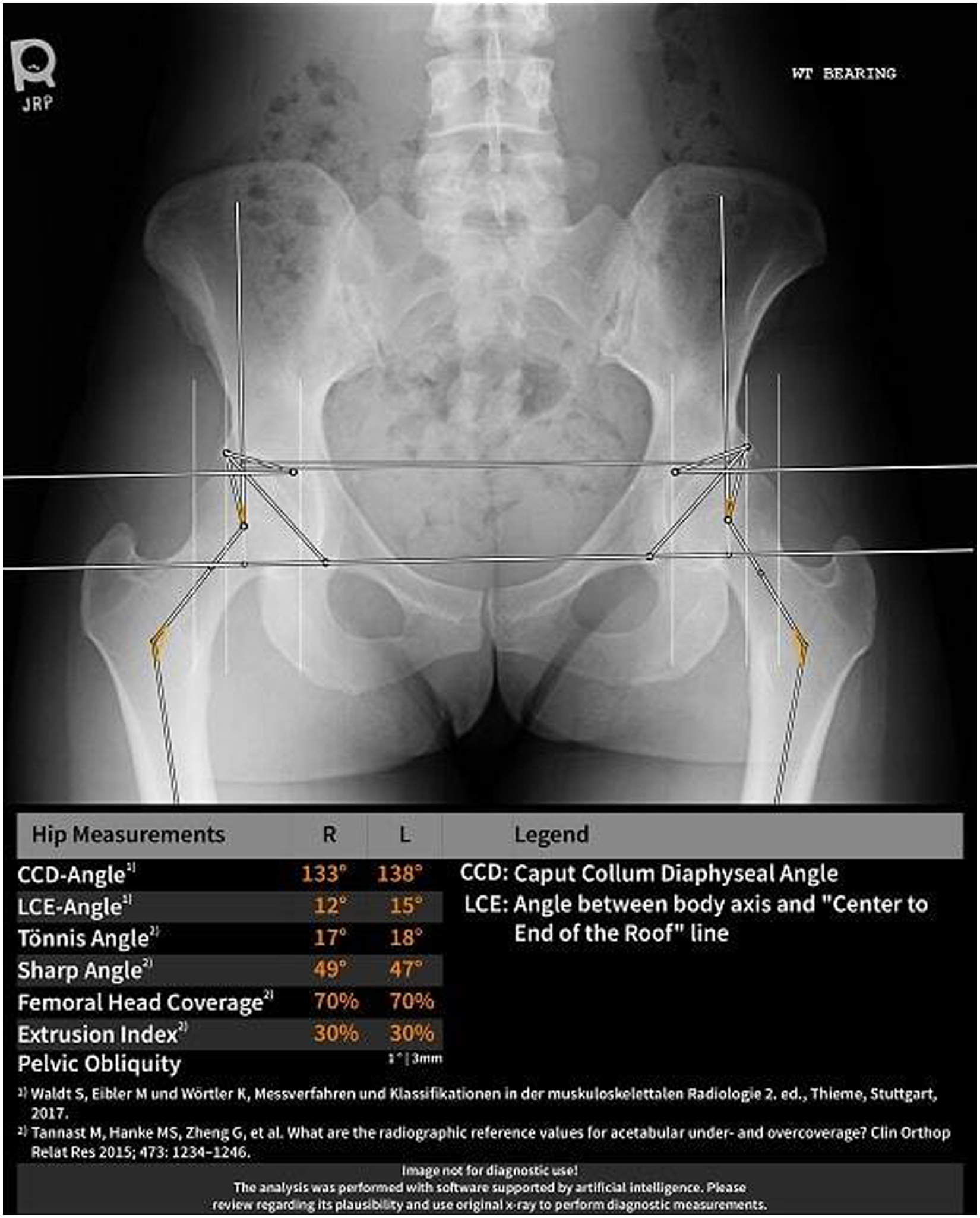
Example HIPPO output. This figure shows an example of the reports that HIPPO produces.
3D MRI reconstructions and measurements
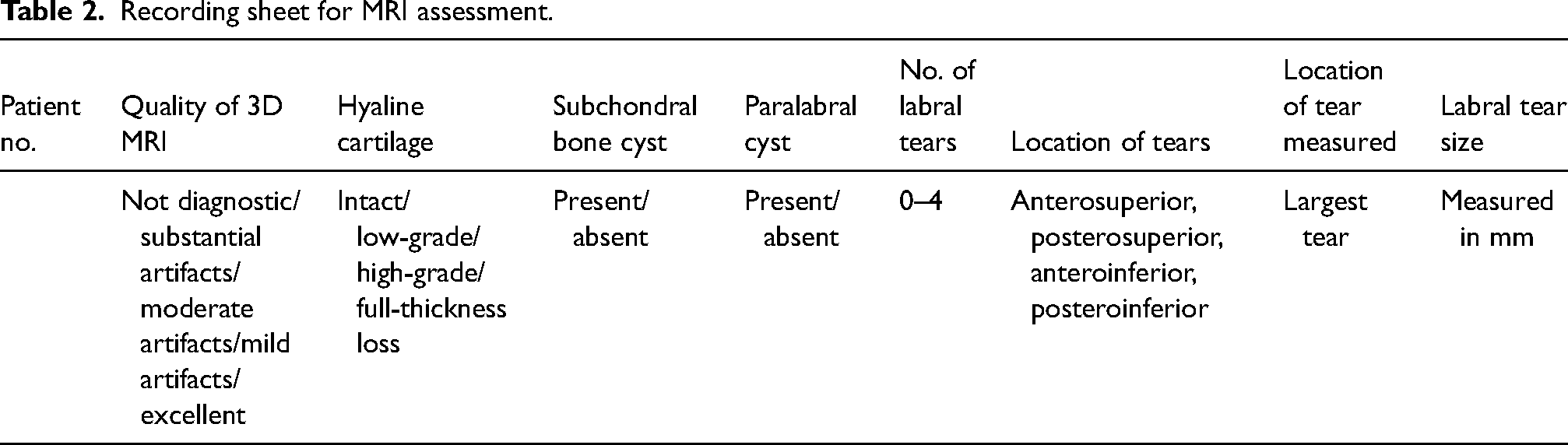
A senior musculoskeletal (MSK) radiologist initially evaluated all cases using both 2D MRI and 3D MRI, mimicking routine practice. The senior radiologist and medical student evaluated the quality of imaging on a scale of 1–5 (5 being the best quality) and labral and cartilage lesions on Isite PACS (Philips, Best, the Netherlands) using a scoring sheet (Table 2). Then, using independent software (Aquarius intuition; Terarecon, Durham, NC, USA), 3D reconstructions were created along the largest labral tear identified and were saved to the same PACS as a set of processed images. The senior MSK radiologist trained three other MSK fellowship-trained experienced readers on the measurement protocols on 10 images, which also formed part of the final dataset. The labral tear lengths were subsequently independently recorded by all three readers from the 3D reconstructions created, blinded to each other's measurements and clinical or surgical findings.
Recording sheet for MRI assessment.
Statistical analysis
Descriptive statistics were used for patient demographics and body mass index (BMI). Spearman's rank correlation coefficients were reported with corresponding 95% confidence intervals for all variables of interest. Correlation coefficients were interpreted as follows: negligible = 0–0.1; weak = 0.1–0.39; moderate = 0.4–0.69; strong = 0.7–0.89; and very strong = 0.9–1. The ICC was also performed to ascertain the level of agreement between the three readers for labral tear length. All analyses were conducted using R version 4.1.1 (R Core Team, Vienna, Austria). The jitter plot for the Sharp angle versus the number of labral tears is included in Fig. 3. Comparison of the distribution of femoral head coverage values, LCEA, and Sharp angles in patients with and without paralabral cysts are included in Figs. 4–6.
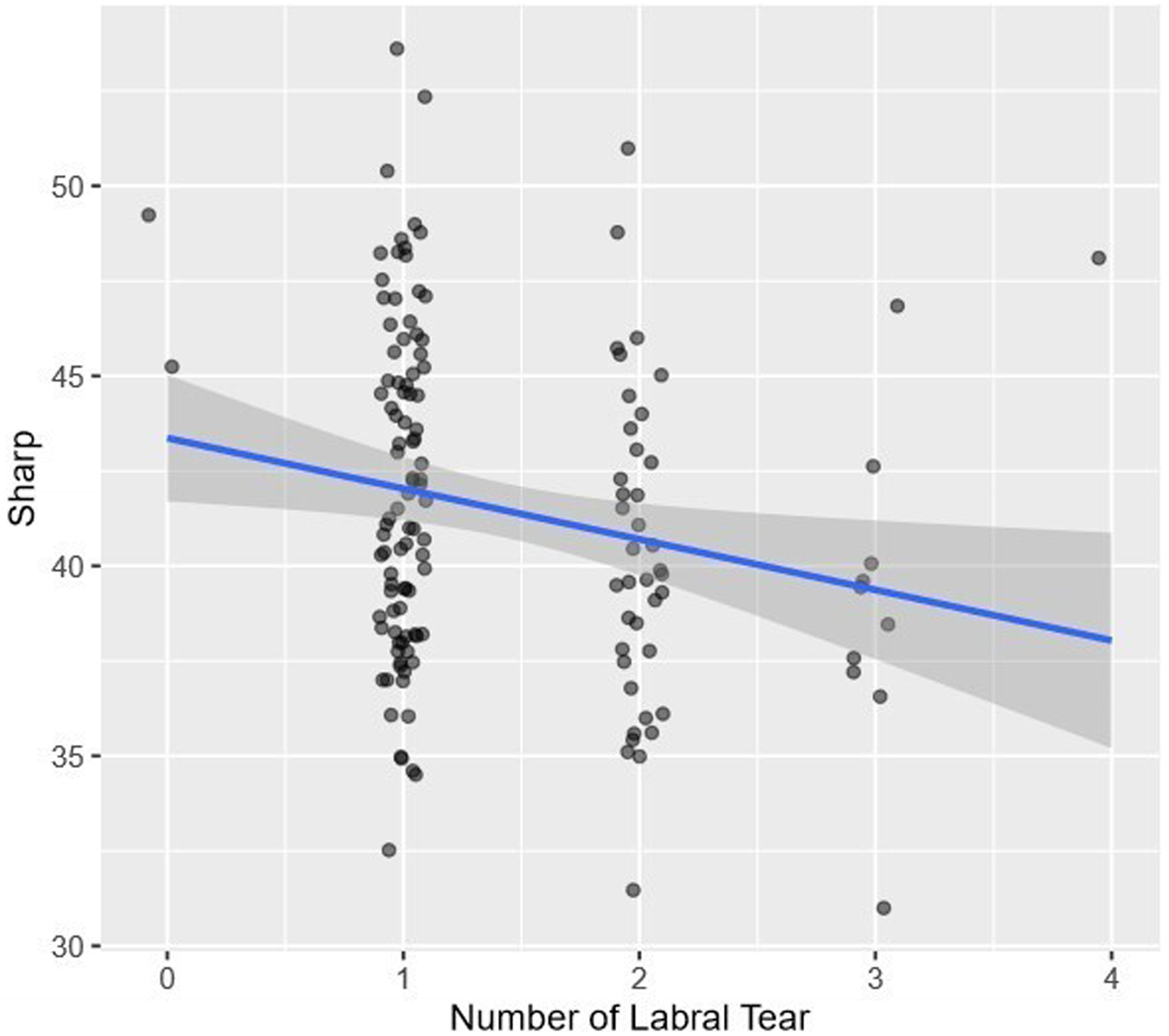
Jitter plot of the Sharp angles of patients vs. the number of labral tears.
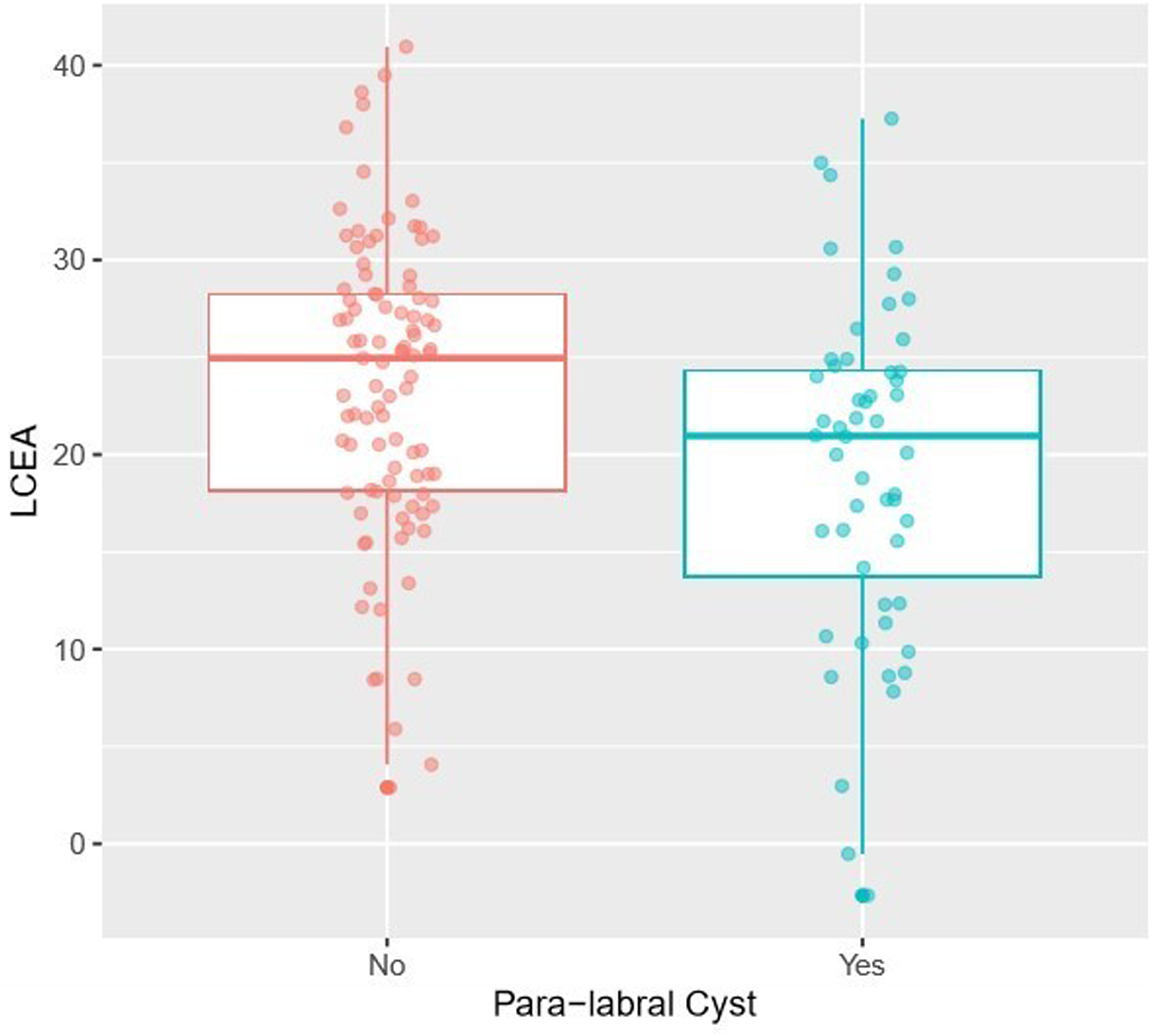
Comparison of the distribution of LCEA values in patients with and without paralabral cysts.
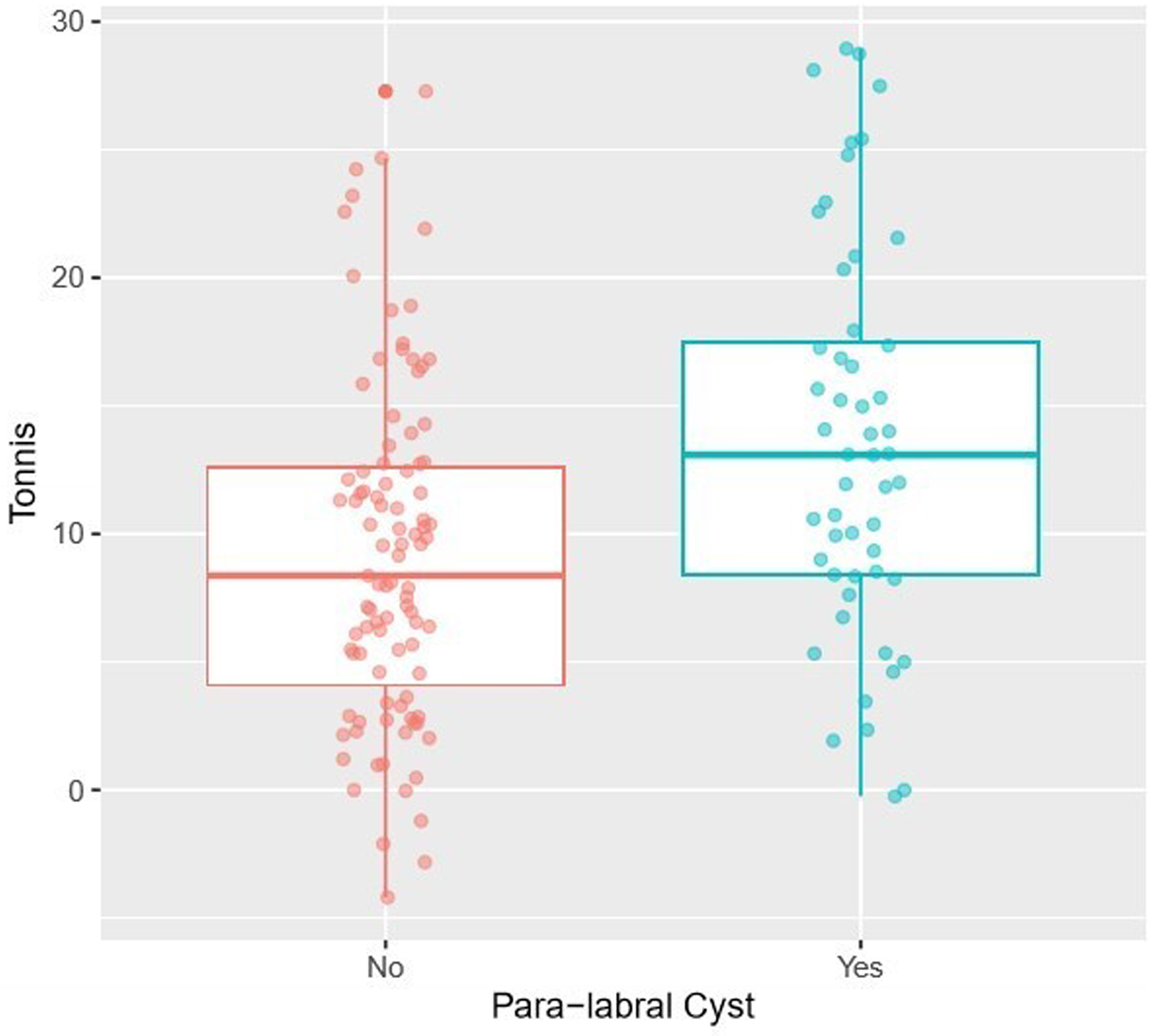
Comparison of the distribution of Tonnis angle values in patients with and without paralabral cysts.
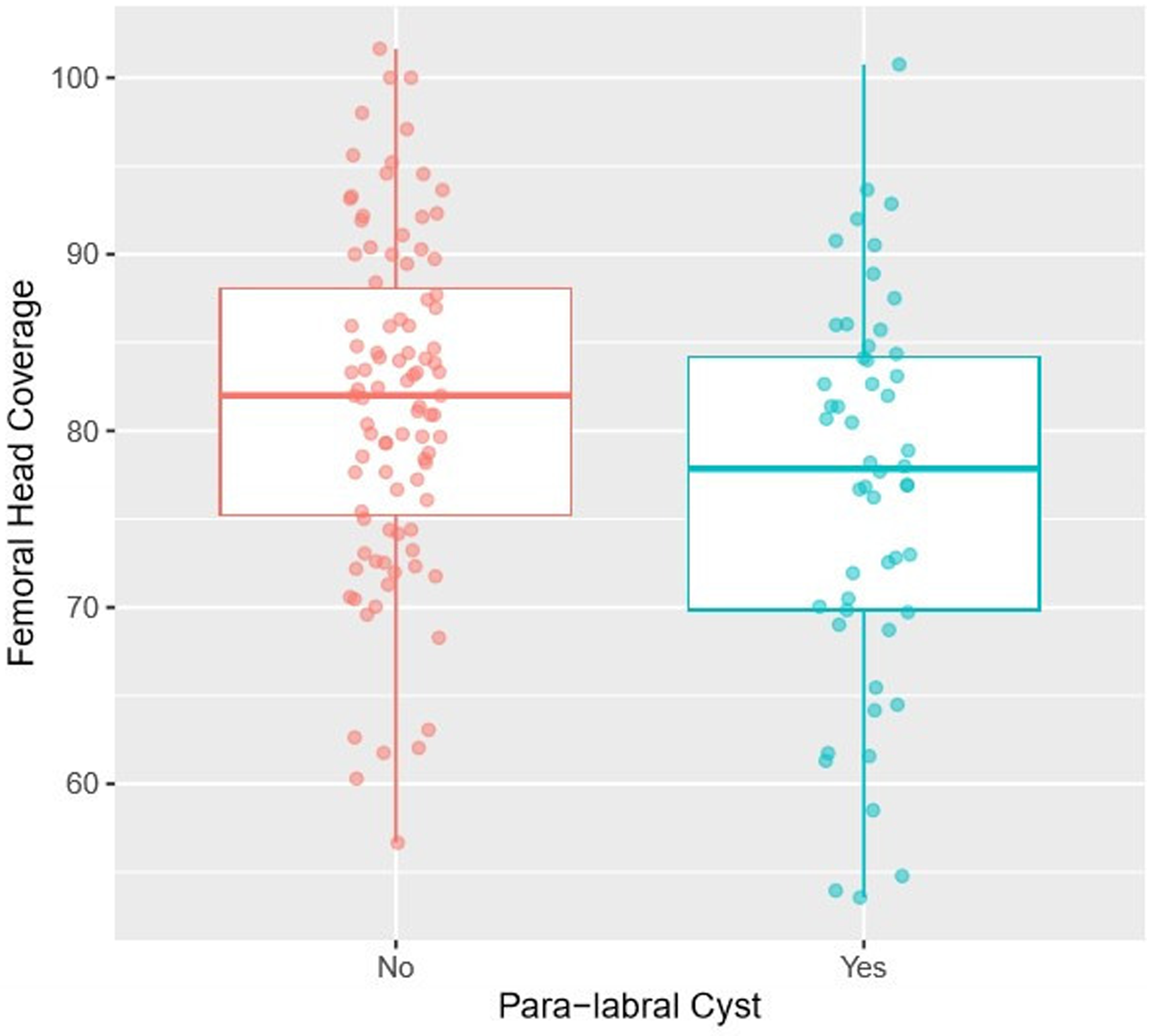
Comparison of the distribution of femoral head coverage values in patients with and without paralabral cysts.
Results
Patients
A total of 156 hips from 139 consecutive patients diagnosed with HD (age range = 16–68 years, men and women) were included. Table 3 shows a full breakdown of patient demographics.
Patient demographics.
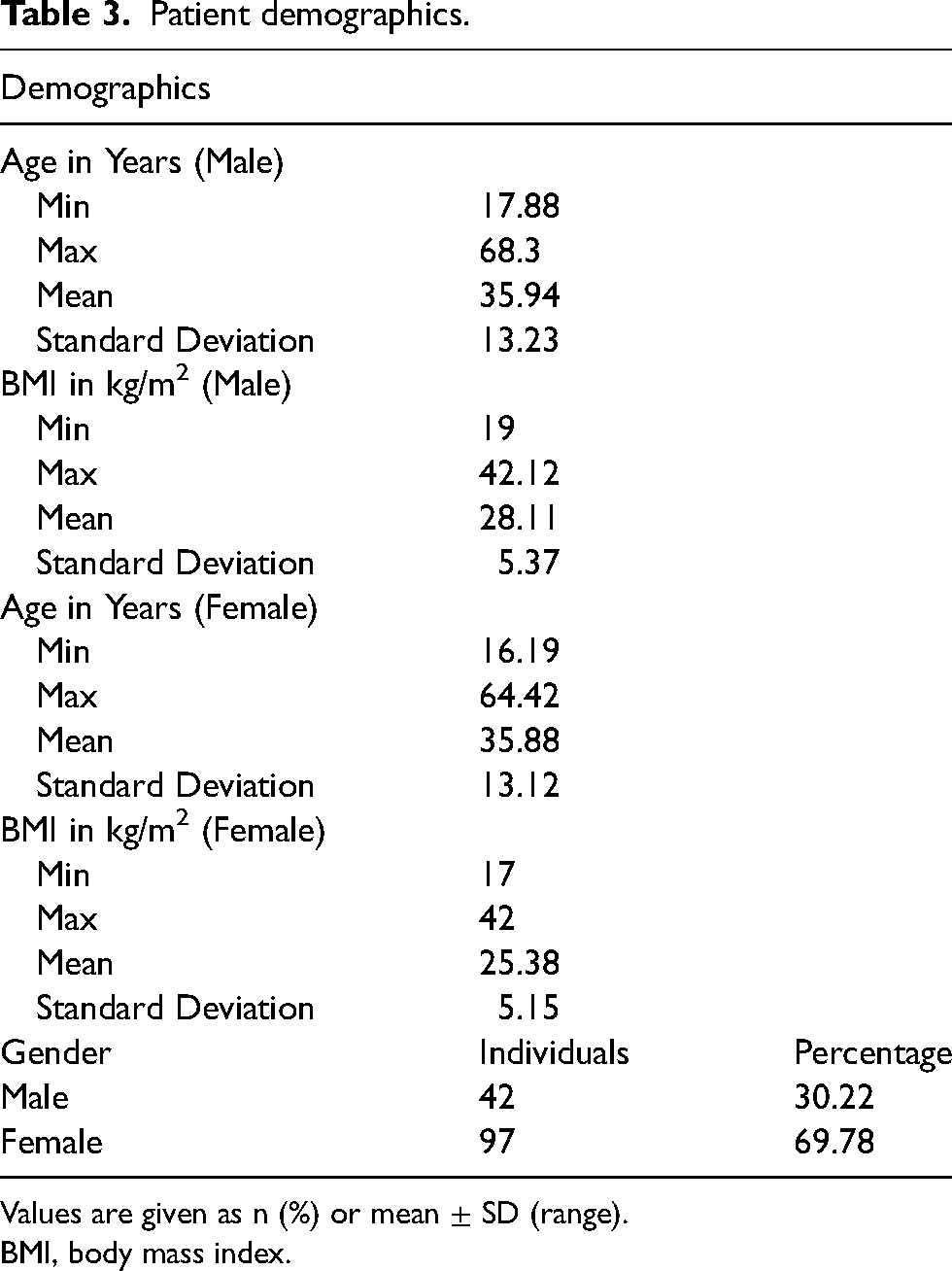
Values are given as n (%) or mean ± SD (range).
BMI, body mass index.
Hip MRI
In total, 122 hips had intact cartilage, 10 had low-grade, six had high-grade, and 18 had full-thickness cartilage loss. The majority of 3D hip MRI scans were of good to excellent quality (20/156 3D MRI scans with a quality of 3, 55/156 3D MRI scans with a quality of 4, and 76/156 3D MRI scans with a quality of 5). Representative MRI scans of two patient cases are included in Figs. 7 and 8.
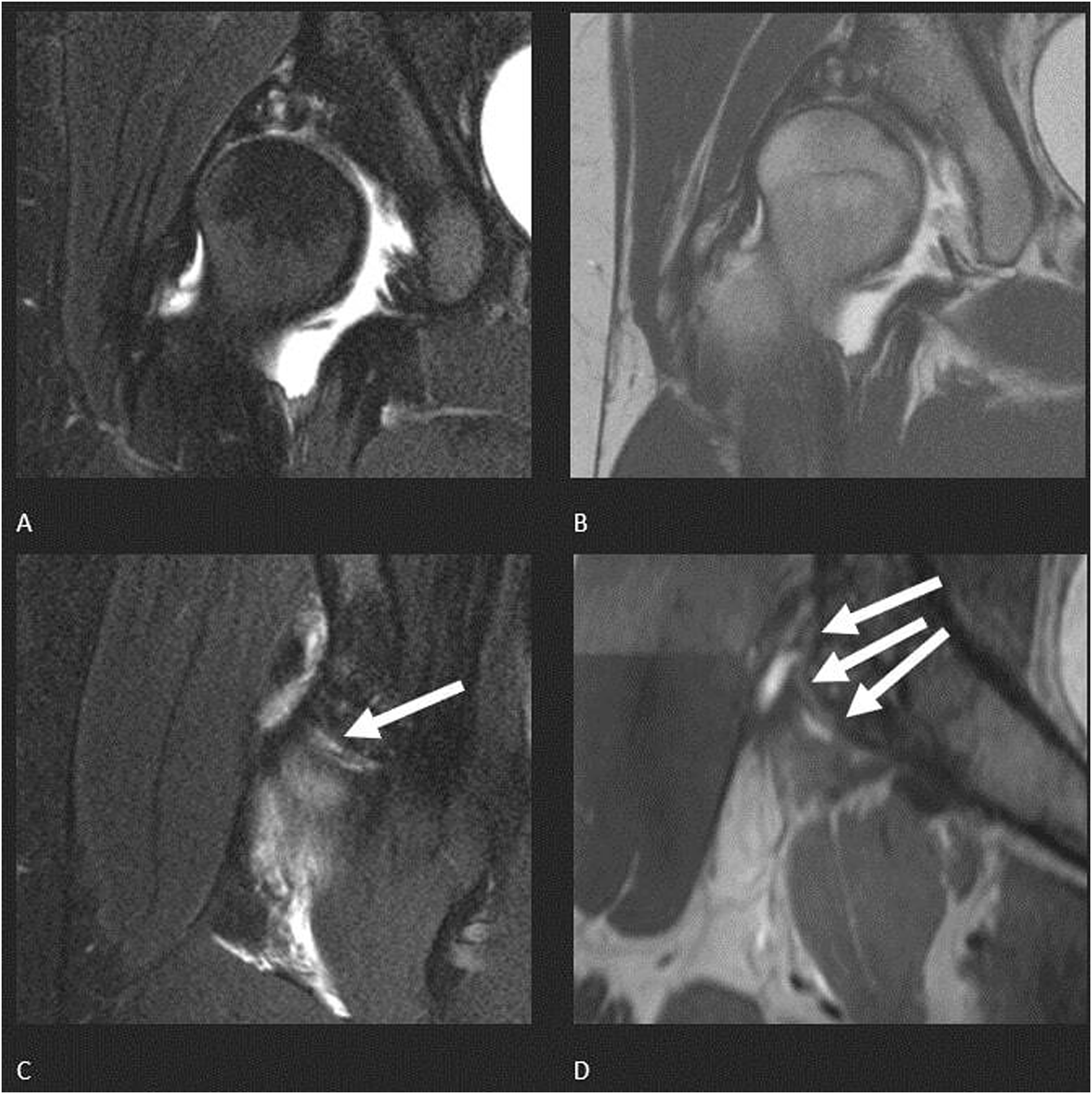
A 21-year-old woman with severe right HIP with grade IV cartilage injury and labral tears in the anterosuperior and anteroinferior quadrants. The anterosuperior labral tear was larger and was measured. The 3D MRI quality was excellent. (a, b) 3D MRI show grade IV cartilage defects with subchondral cysts and labral tears. (c) 2D MRI and (d) corresponding 3D MRI reconstruction show labral tear measurement of 19 mm (arrows). HD, hip dysplasia; MRI, magnetic resonance imaging.
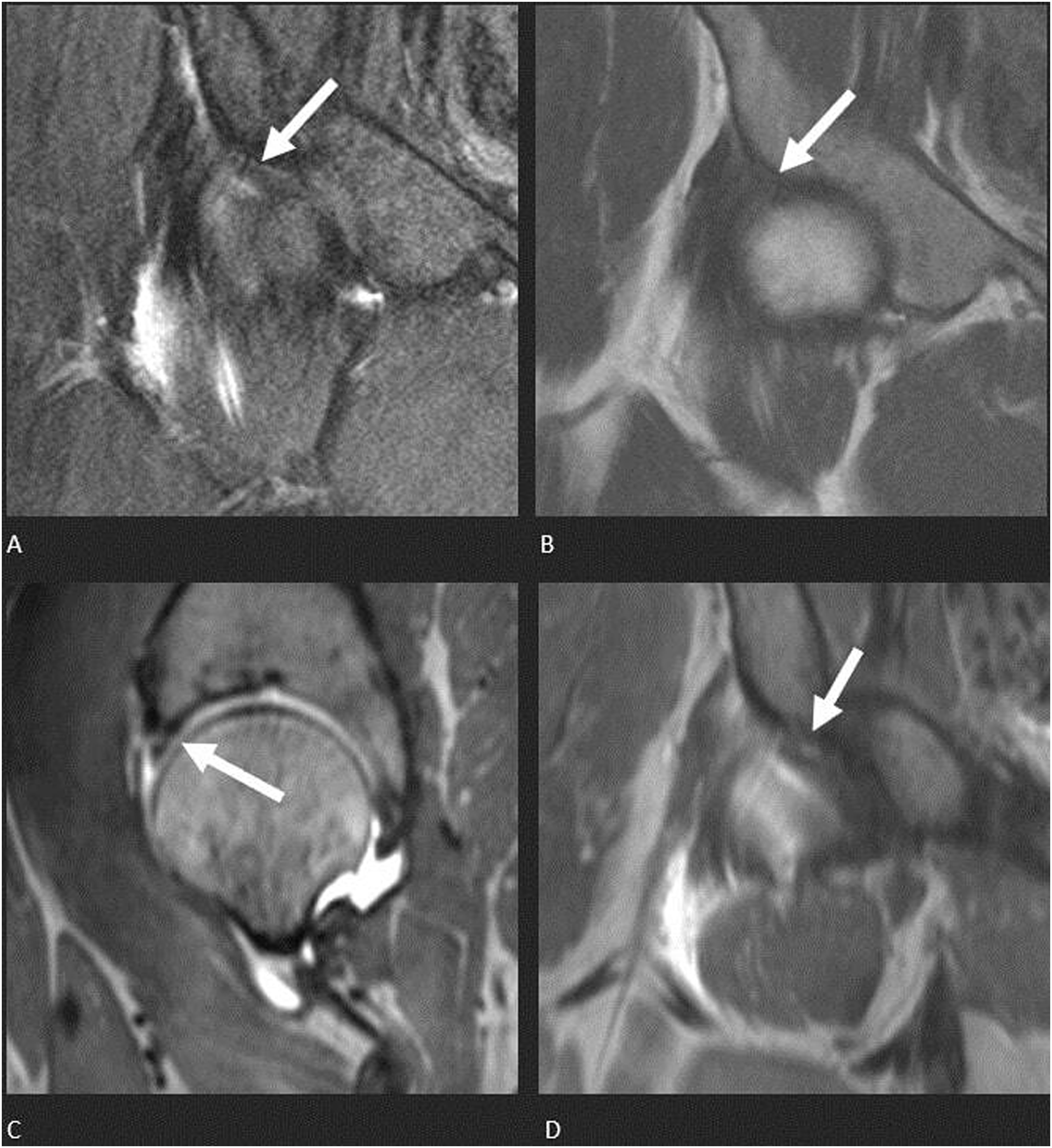
A 34-year-old woman with one anterosuperior labral tear measured at 4.93 mm on 3D MRI (white arrows). The 3D MRI quality was excellent. (a, b) 3D MRI shows no cartilage damage or cysts. (c, d) 2D MRI and corresponding 3D MRI reconstruction of the anterosuperior labral tear outlined with arrows measuring 5 mm. MRI, magnetic resonance imaging.
3D hip MRI measurements
The minimum labral tear length observed was 3.5 mm and the maximum labral tear length was 31.17 mm. The mean labral tear length was 15.38 ± 5.57 mm. Table 4 shows a full breakdown of the MRI findings.
MRI findings.
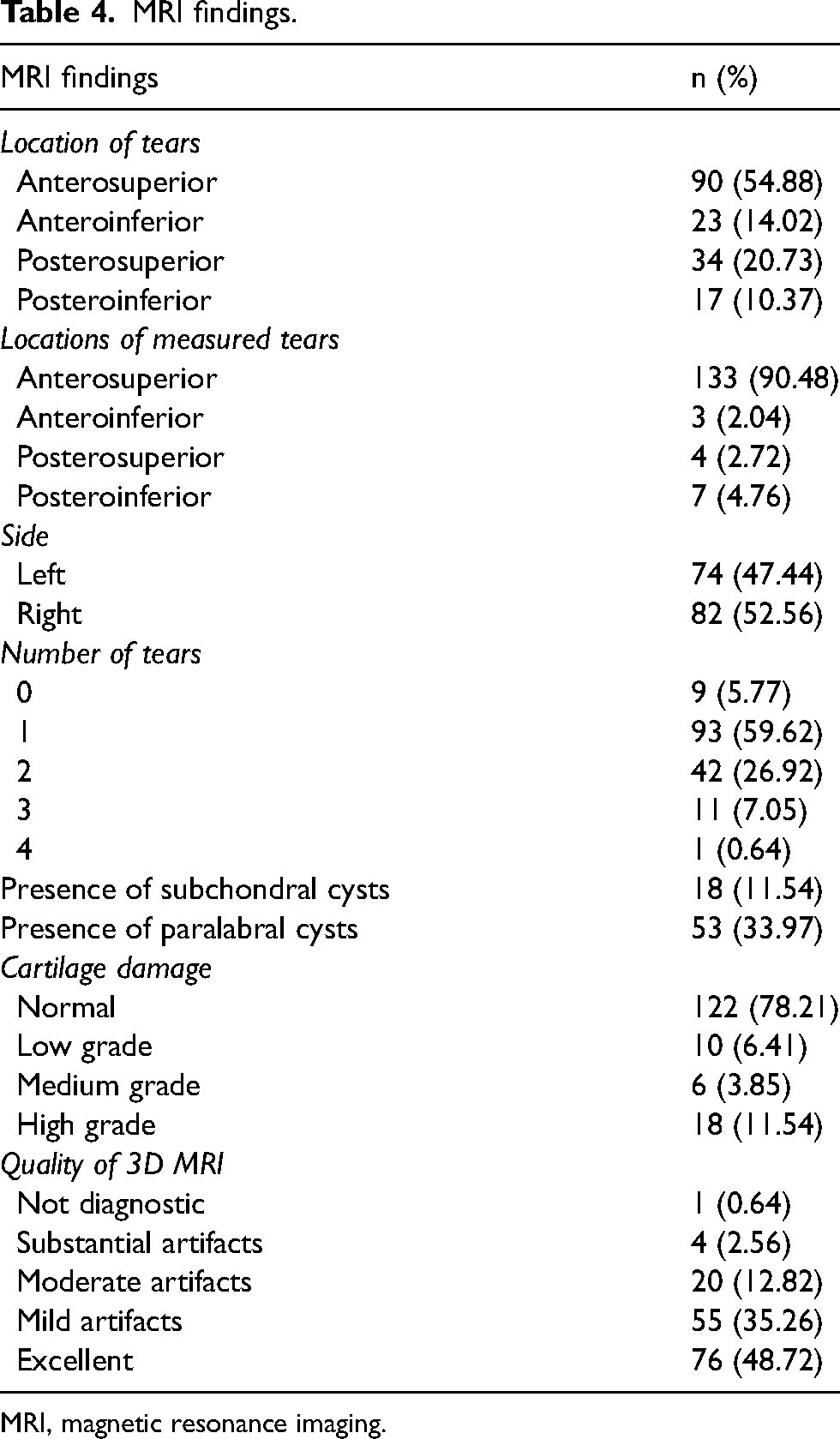
MRI, magnetic resonance imaging.
Inter-reader analysis
The ICC was 0.66 for the labral tear lengths between the three readers, which equates to a moderate inter-reader correlation. The Bland–Altman plots for reader 1 versus reader 2, reader 2 versus 3, and reader 1 versus 3 are included in Fig. 9.
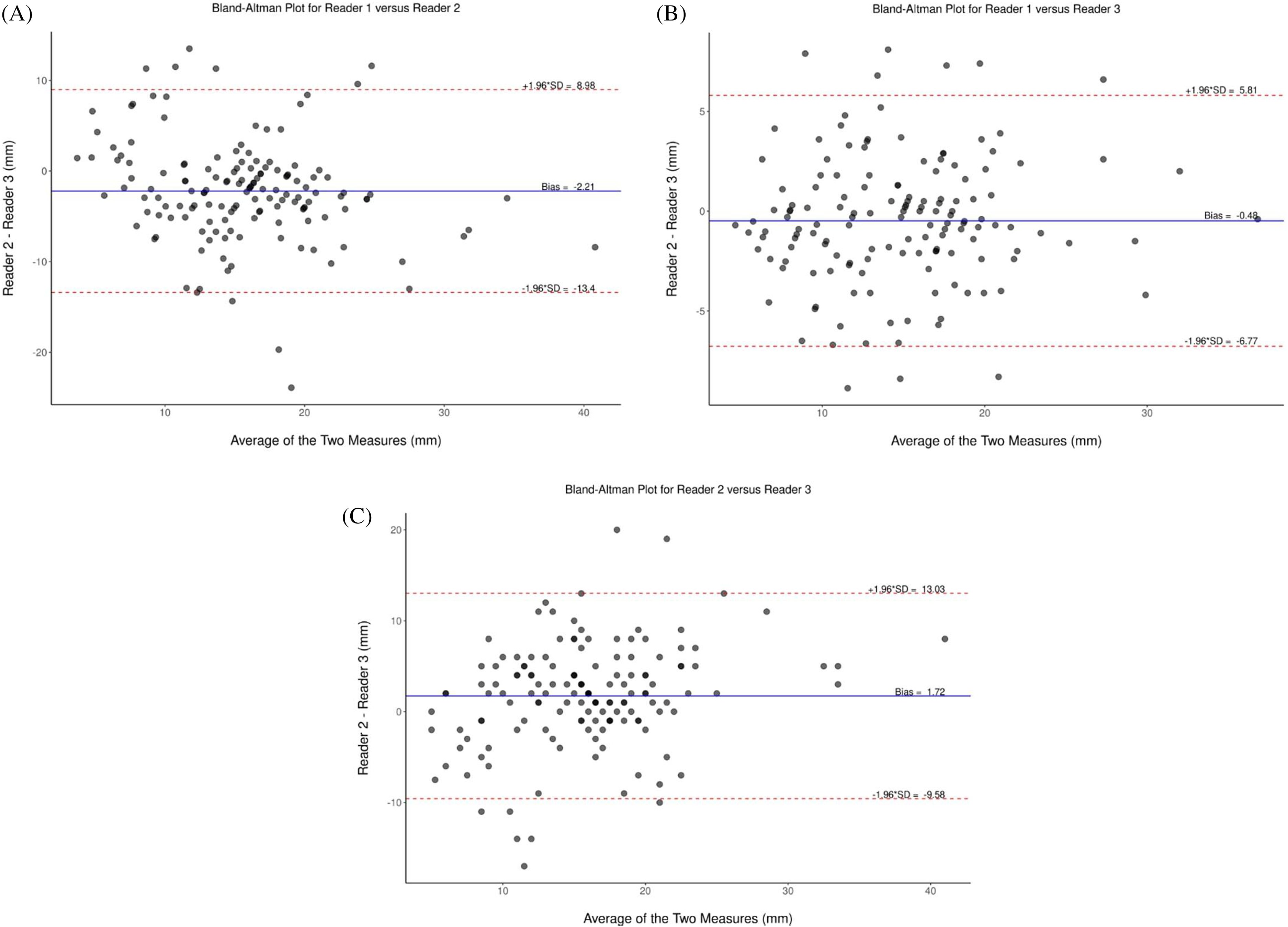
Bland–Altman plots for (a) reader 1 vs. reader 2, (b) reader 1 vs. reader 3, and (c) reader 2 vs. reader 3.
3D MRI versus HIPPO
There were statistically significant correlations between paralabral cysts and femoral head coverage, extrusion index, LCEA, and Tonnis radiographic measurements. There were also statistically significant correlations seen between the number of labral tears and the Sharp angle. Table 5 shows all Spearman correlations between the variables studied.
Spearman correlations between 3D MRI measurements and AI-generated radiographic measurements for HD patients.
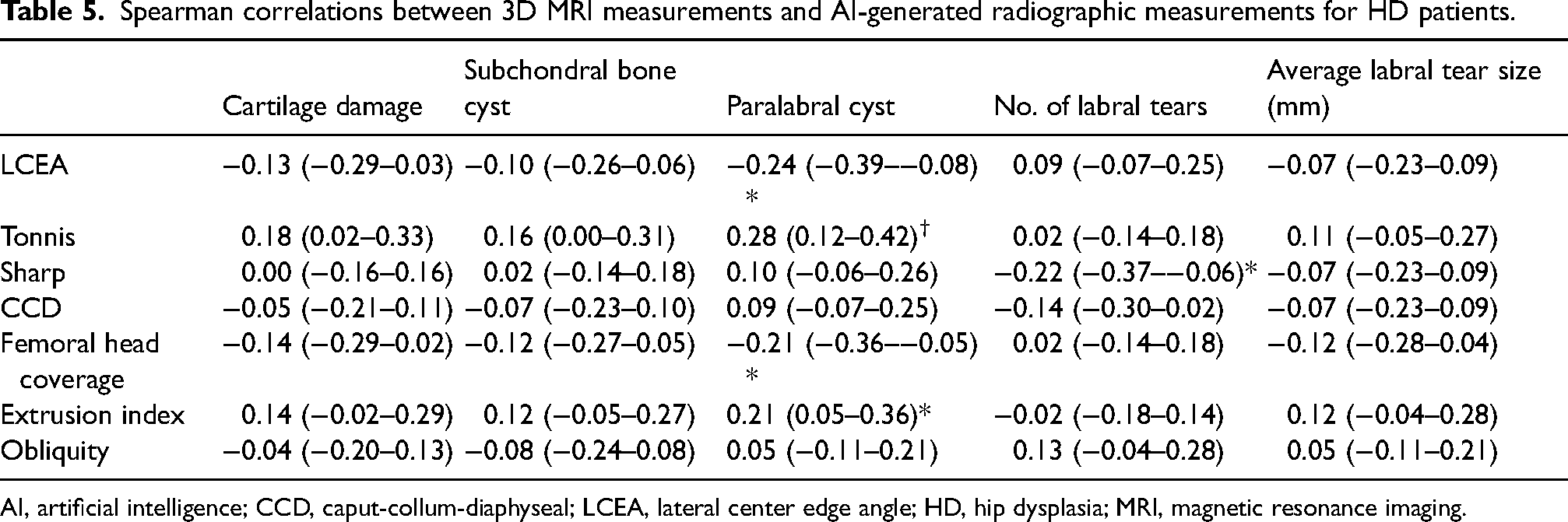
AI, artificial intelligence; CCD, caput-collum-diaphyseal; LCEA, lateral center edge angle; HD, hip dysplasia; MRI, magnetic resonance imaging.
Discussion
We attempted correlation of AI-generated radiographic measurements with internal derangement findings on advanced MRI in the setting of known HD. There were no statistically significant correlations seen between the length of labral tears and radiographic measurements. There were statistically significant, though weak, correlations seen between various AI-generated radiographic measurements and the presence of paralabral cysts and the number of labral tears. This suggests a role for AI-generated measurements to predict findings seen on 3D MRI based on radiographic findings for HD patients. There were negative correlations between LCEA and femoral head coverage with the presence of paralabral cysts (−0.24 and −0.21, respectively), as well as positive correlations between Tonnis angle and extrusion index with paralabral cysts (0.28 and 0.21, respectively). Furthermore, a negative correlation was also seen between the Sharp angle and the number of labral tears present (−0.22).
The positive and negative correlations seen between radiologic measurements and internal derangements seen through 3D MRI partially support our hypothesis that worsening parameters measured through advanced MRI would correlate with worsening radiographic parameters. Specifically, the negative correlation seen between the presence of paralabral cysts and the LCEA angle suggests that the formation of paralabral cysts is more with smaller LCEA angle, corresponding to HD disease progression. The positive correlation seen between the extrusion index and the presence of paralabral cysts suggests that suboptimal femoral head coverage is associated with paralabral cysts, as a larger extrusion index indicates worsening acetabular dysplasia (15).
Although there were some correlations seen between radiographic parameters measured through AI and internal derangements seen on 3D MRI, this study suggests that more work is needed to implement AI measurements into clinical scenarios.
The present study has some limitations. The study consists of predominantly female participants (97/139, 70%), which may affect the correlation patterns observed. However, HD is more prevalent in female populations, and the study precluded selection bias as a consecutive case series was included. Furthermore, the entire study population presented at a hip preservation clinic with symptoms, which means that the study cohort is more homogenous and more severe compared to the general HD population. This homogeneity may have resulted in some of the correlation trends seen. We did not correlate labral tear lengths observed in surgery due to the retrospective assessment and the fact that multiple tears in other hip locations are usually not repaired. This study is also limited by the lack of a control cohort since it was not possible to recruit participants without HD to undergo MRI and X-ray procedures. There are also a variety of factors that could influence the disease course of HD that were not recorded with the patient cohort, such as femoral version factors and laxity scores. Thus, these are possible confounding factors that could have influenced the findings in the study.
Despite its limitations, this study still presents a novel application of AI-generated measurements and 3D MRI in patients with HD. The potential of AI, which could complete standardized radiographic measurements in seconds that would otherwise take radiologists minutes, is immense in the clinical evaluation of patients. Furthermore, correlating AI-generated radiographic parameters with internal derangements measured through 3D MRI sheds light on the relationship between various imaging measurements between modalities, which adds to the body of knowledge for clinicians to better understand the disease progression of HD and offer more informed treatment plans.
Subsequent studies could examine the correlation between AI-generated radiographic measurements and other clinical (patient-reported outcome measures) and imaging parameters, and between AI generated radiographic measurements and postoperative findings. Further studies are necessary to develop a better understanding of the potential applications AI in musculoskeletal radiology, develop stronger correlations, and expand the breadth and depth of knowledge in this field.
In conclusion, this study produced some statistically significant correlations between various AI-generated radiographic measurements and assessments completed through 3D MRI for patients with HD. Lack of correlations with labral tear length may reflect complex pathophysiology of HD. This suggests a potential clinical role of AI in the treatment planning and prognostication of patients with HD.
Footnotes
Data availability
Data generated or analyzed during the study are available from the corresponding author by request.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AC is a consultant at ICON Medical and TREACE Medical Concepts Inc., receives book royalties from Jaypee and Wolters, is a medical advisor at Siemens, and has a research grant from Image Biopsy Lab Inc.; JW is a consultant at Ethicon.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.